Biopsychology
1/25
Earn XP
Description and Tags
This topic has no AO3 until about 1/3 of the way through at fight or flight. So you can't be asked 16 markers on anything before fight or flight.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
Divisions of the nervous system: CNS
The human nervous system is a complex network of nerve cells/neurons.
It has two main functions:
To collect, process and respond to information
To co-ordinate the working of different organs and cells
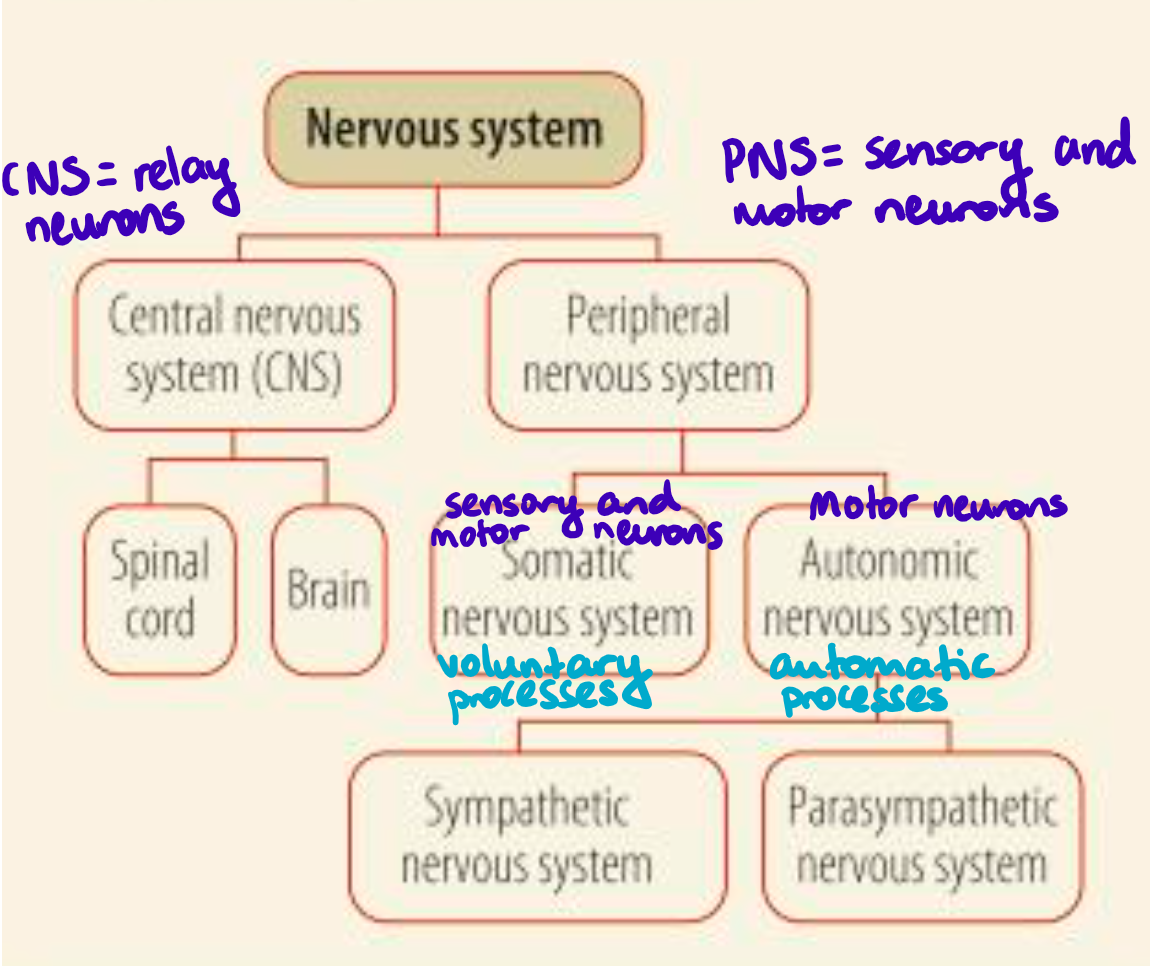
The human nervous system is divided into the central nervous system (CNS) and peripheral nervous system (PNS), with each of these further divided into different components, each with a different function but all working together.
SEE IMAGE ATTACHED
The CNS is made up of the brain and spinal cord, which are made up of RELAY NEURONS. The CNS passes messages to and from the brain and connects nerves to the PNS.
The spinal cord connects to different parts of the body through spinal nerves so its main function is to relay information between the brain and the rest of the body. This allows the brain to monitor and regulate bodily processes, such as digestion and breathing, and to coordinate voluntary movements. The spinal cord is also responsible for reflex actions, for example pulling your hand away from something that is hot. If the spinal cord is damaged, areas supplied by spinal nerves below the damaged site will be cut off from the brain and will stop functioning.
The brain can be divided into four main areas – the cerebrum, cerebellum, diencephalon and brain stem.
The cerebrum is the largest part of the brain, and is further divided into four different lobes, each of which has a different primary function:
Frontal lobe - thought and speech
Occipital lobe - has the visual cortex so deals with visual images
Temporal lobe - language, emotion, memory
Parietal lobe - integrates sensory information, language
The cerebellum sits beneath the back of the cerebrum. It is involved in controlling a person’s motor skills and balance, coordinating the muscles to allow precise movements.
The diencephalon lies beneath the cerebrum and on top of the brain stem. Within this area are two important structures, the thalamus and the hypothalamus.
The thalamus acts as a relay station for nerve impulses coming from the senses, routing them to the appropriate part of the brain where they can be processed. The hypothalamus has a number of important functions, including the regulation of body temperature, hunger and thirst. It also acts as the link between the endocrine system and the nervous system, controlling the release of hormones from the pituitary gland.
The brain stem is responsible for regulating the automatic functions that are essential for life. These include breathing, heartbeat and swallowing.
Divisions of the nervous system: PNS
All the nerves outside the CNS make up the peripheral nervous system. This function of this part of the nervous system is to send nerve impulses from the CNS (the brain and spinal cord) to the rest of the body and from the body back to the CNS.
The PNS involves SENSORY NEURONS and MOTOR NEURONS.
There are two main divisions of the peripheral nervous system, the somatic nervous system and the autonomic nervous system (ANS).
The somatic nervous system is responsible for carrying sensory and motor information to and from the spinal cord via sensory and motor neurons.
Sensory neurons relay messages to the CNS, and motor neurons relay information from the CNS to other areas of the body.
The somatic system is involved in causing voluntary processes to happen as it is also involved in reflex actions without the involvement of the CNS, which allows the reflex to occur very quickly.
The autonomic system is made of just motor neurons.
It controls internal glands and organs and it is responsible for involuntary/automatic actions which do not require conscious awareness, for example, the heart beating.
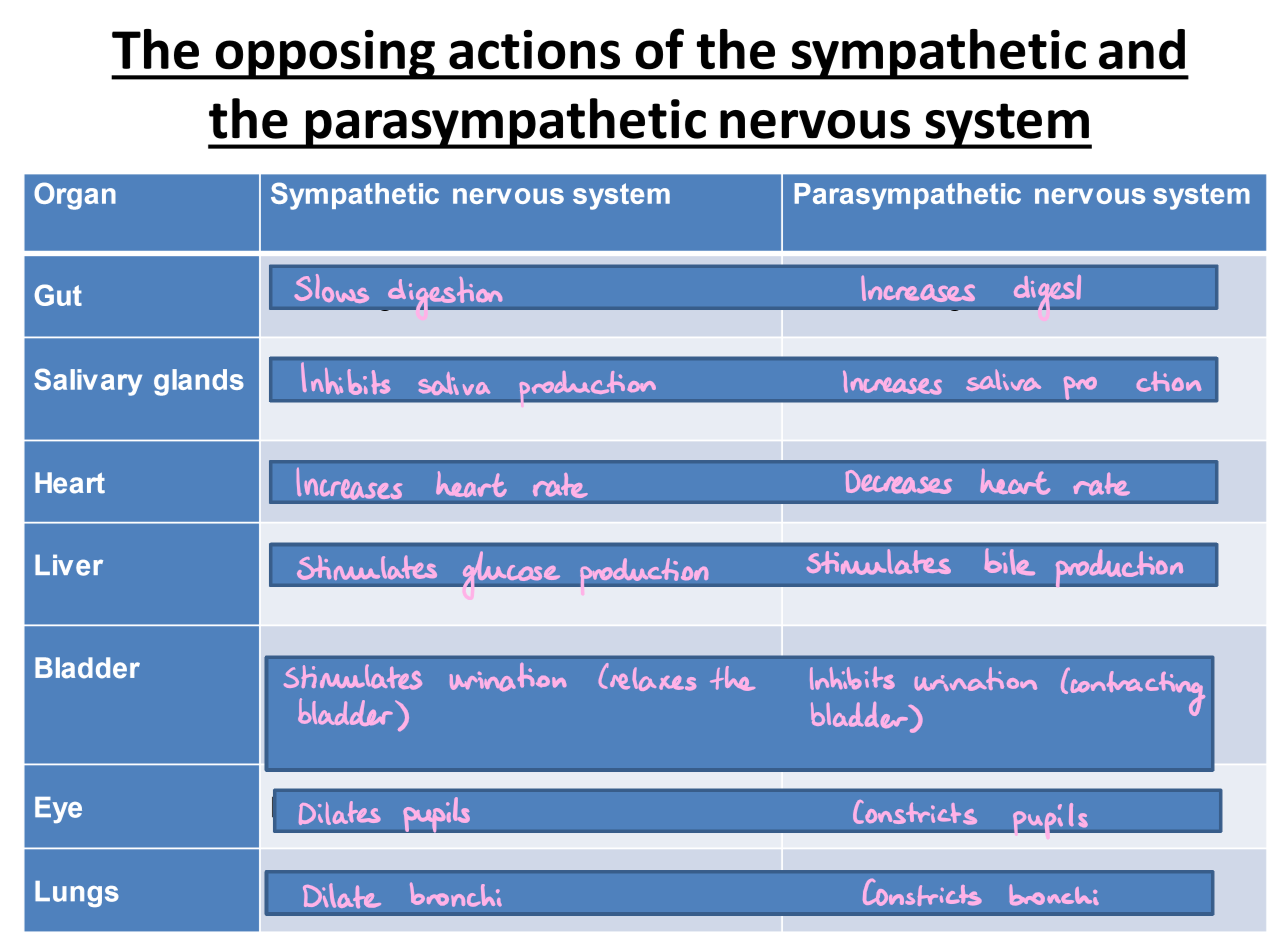
The ANS has two parts: the sympathetic and the parasympathetic. These two divisions actions are mostly antagonistic as they tend to regulate the same organs but have opposite effects.
The sympathetic systems tends to use noradrenaline, which has stimulating effects. It generally prepares the body to expend energy for fight or flight (so kicks in when you are stressed).
The parasympathetic tends to use acetylcholine, which has inhibiting effects. It generally maintains and conserved body energy and functions (so kicks in when you aren’t stressed i.e. after the “threat” has passed so your body can return everything to normal after fight or flight).
SEE IMAGE ATTACHED!!!
(So somatic nervous system has sensory and motor neurons whereas autonomic nervous system only has motor neurons.)
Neurons and synaptic transmission: The structure and function of neurons in general
Neurons/nerve cells are cells that conduct nerve impulses. They are specialised to carry neural information throughout the body.
Everything a person thinks and feels, says and does are caused by electrochemical events occurring within and between neurons.
Neurons can be one of three types: sensory neurons, relay neurons or motor neurons.
SEE IMAGE ATTACHED!!!
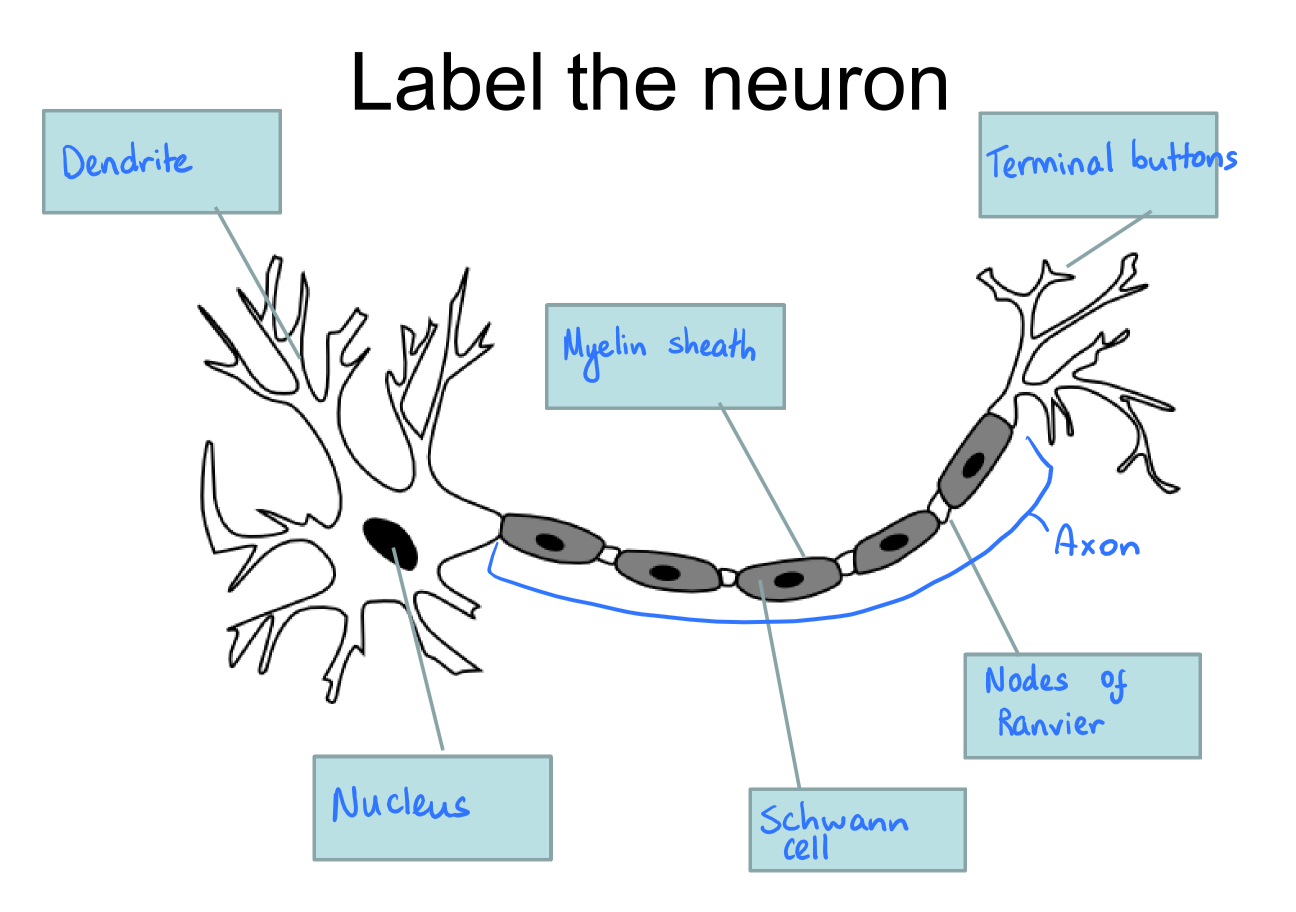
Neurons consist of:
Nucleus
The control centre – contains the cell's chromosomal DNA.
Dendrite
Receives the impulse from adjacent neurons.
Axon
Length which the electrical signals pass along.
Schwann cells
These are just the cells that make up the axon so they have the same function as the axon.
Myelin sheath
Insulates/protects the axon from external influences that might effect transmission.
Nodes of ranvier (gaps along the axon with no myelin sheath)
These speed up the transmission of the impulse by forcing it to ‘jump’.
Terminal buttons
Terminal buttons send signals to an adjacent neuron.
Neurons and synaptic transmission: Types of neuron
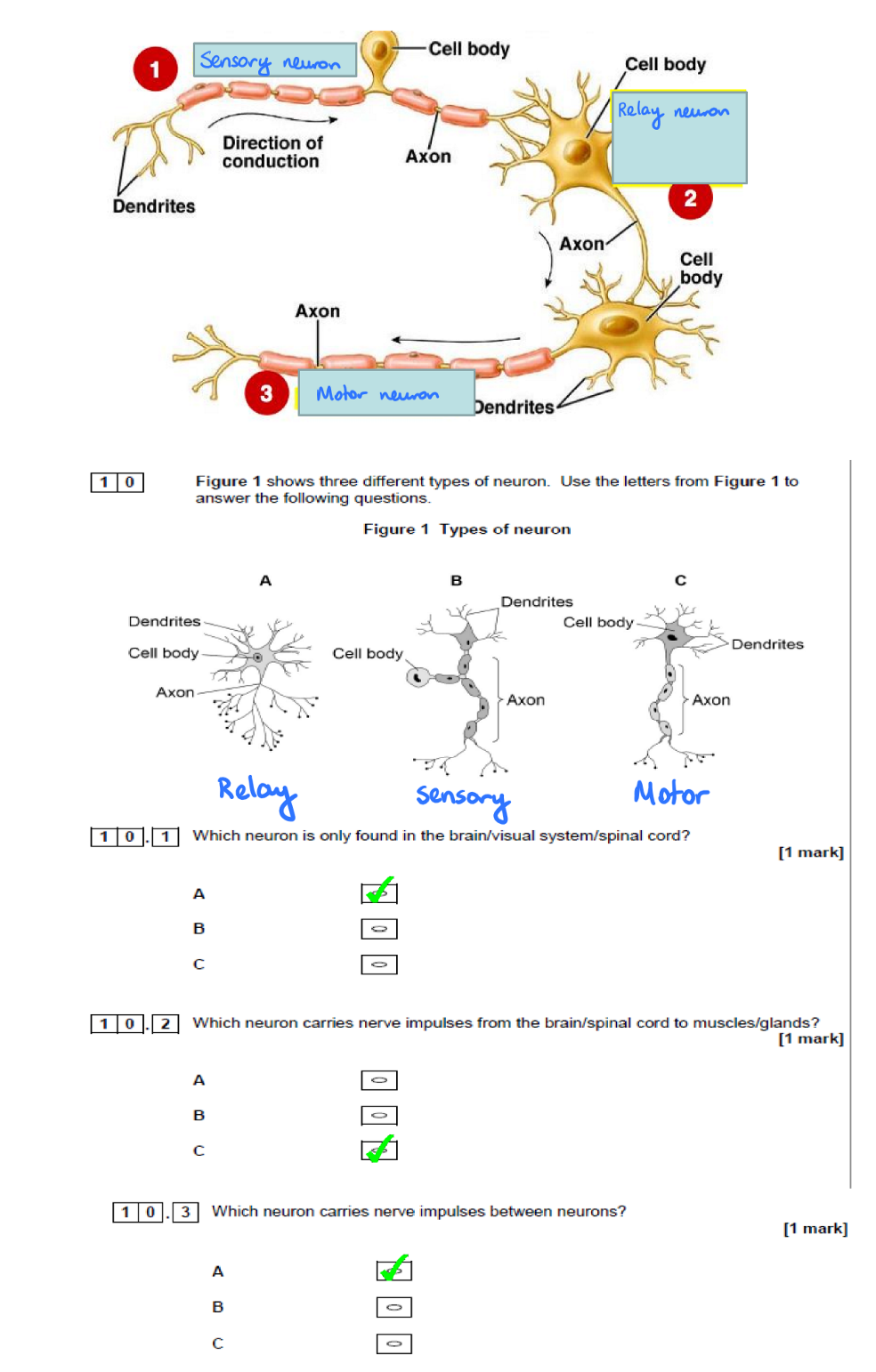
Neurons can be one of three types: sensory neurons, relay neurons or motor neurons.
The cellular structure of all neurons is the same. There are anatomical differences in size, depending on their function:
Motor neuron | Relay (Interconnecting) neuron | Sensory neuron |
|---|
Function | Carries messages from the CNS (i.e. brain and spinal cord) to effectors such as muscles and glands. | Transfers messages from sensory neurons to other relay neurons or motor neurons. | Carries messages from the senses to the brain and spinal cord. |
Structure | Short dendrites and long axons (the neuron you typically see in textbook diagrams) | Short dendrites and either short or long axons -but usually drawn with short axon. | Long dendrites and short axons and protruding cell body. |
SEE IMAGE ATTACHED - In diagrams…
Sensory neurons will be shown to have a protruding cell body.
Motor neurons just have the typical neuron shape.
Relay neurons will be drawn stumpier.
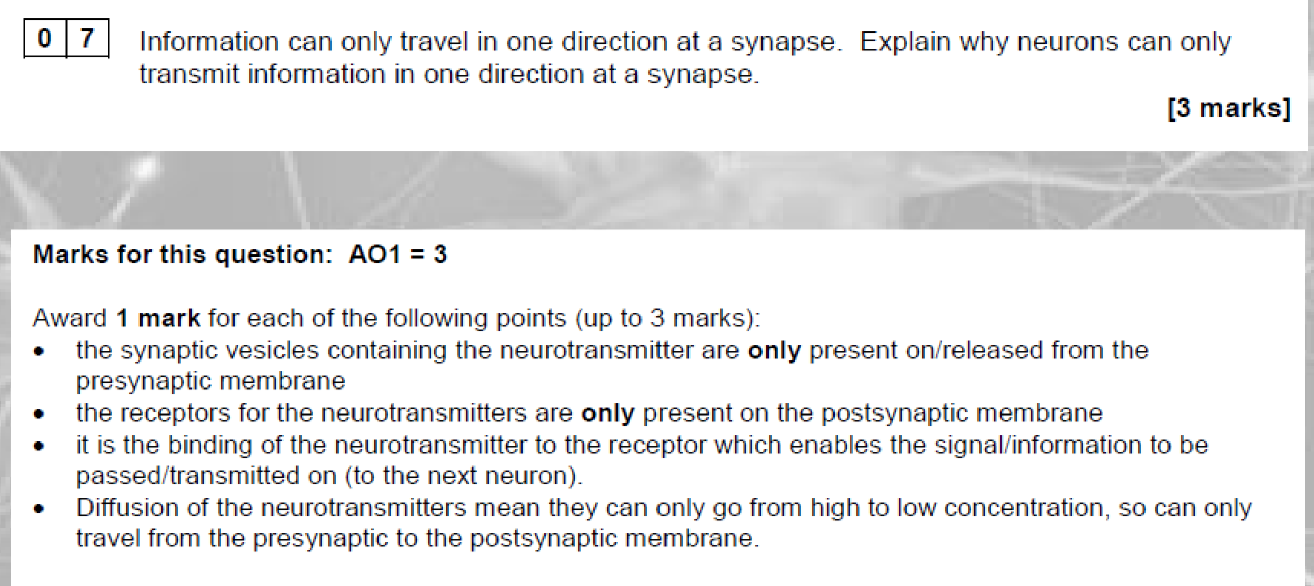
Neurons and synaptic transmission: Synaptic transmission
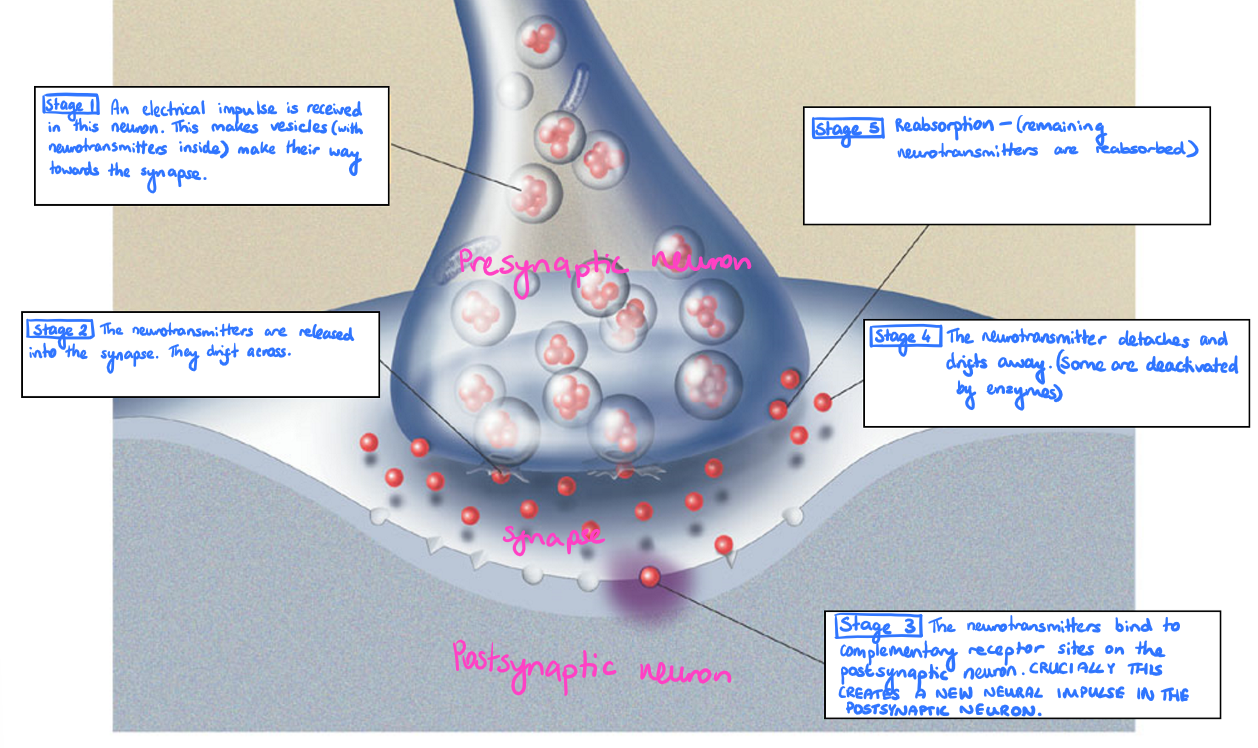
Synaptic transmission is the process by which a nerve impulse passes across the synaptic cleft/synapse from one neuron (the pre-synaptic neuron) to another (the post-synaptic neuron).
See image attached!!!
An electrical impulse is received in a neuron. This makes vesicles (with neurotransmitters inside) make their way towards the synapse.
The neurotransmitters are released into the synapse. They drift across, moving by diffusion from an area of high concentration to low concentration.
The neurotransmitters bind to complementary receptor sites on the postsynaptic neuron. CRUCIALLY THIS CREATES A NEW NEURAL IMPULSE IN THE POSTSYNAPTIC NEURON.
The neurotransmitter detaches and drifts away. (Some are deactivated by enzymes).
Reabsorption (remaining neurotransmitters are reabsorbed into the terminal button).
Excitation and Inhibition:
When neurotransmitters bind to receptors, they produce excitatory or inhibitory effects.
Excitatory neurotransmitters (e.g. acetylcholine) binding with a postsynaptic receptor causes an excitatory post-synaptic potential (EPSP), making the post-synaptic cell more likely to fire.
Inhibitory neurotransmitters (e.g. GABA) binding with a postsynaptic receptor causes an inhibitory post-synaptic potential (IPSP), making the post-synaptic cell less likely to fire.
A postsynaptic neuron can receive EPSPs and IPSPs at the same time. The likelihood of the cell firing is determined by adding up excitatory and inhibitory synaptic input. This net result is known as summation.
There is spatial summation when a large number of EPSPs are generated at many different synapses on the same post-synaptic neuron at a time.
Temporal summation is when large numbers of EPSPs are generated at the same synapse by a series of high frequency action potentials/impulses from the same pre-synaptic neuron.
A couple of definitions just for clarity:
Synapse = the conjunction at the end of the axon of one neuron and the dendrite of another.
Neurotransmitter = chemical substances that play an important part in the workings of the nervous system by transmitting nerve impulses across a synapse.
Tricky PPQ on neurons and synaptic transmission
SEE IMAGE ATTACHED!!!
The endocrine system
The endocrine system is a network of glands throughout the body that manufacture and secrete chemical messengers known as hormones.
Hormones are chemicals that regulate the activity of cells or organs in the body. They only have an effect on TARGET CELLS that have receptor sites for that hormone.
The endocrine system and nervous system work closely together to regulate the physiological processes of the human body, but they are different:
NERVOUS SYSTEM | ENDOCRINE SYSTEM |
Uses nerves to transmit information. | Uses blood vessels to transmit information. |
In charge of faster processes e.g. breathing and body movement. | In charge of body processes that are slow e.g. cell growth. |
Involves neurons and neurotransmitters (so electrical and chemical). | Uses hormones (so just chemical). |
Endocrine glands:
Endocrine glands are special groups of cells within the endocrine system whose function is to produce and secrete hormones.
The major glands of the endocrine system are: the pituitary gland, adrenal glands, and reproductive organs (ovaries and testes).
★ Pituitary gland - controls the release of hormones from all other endocrine glands (so its often called the master gland).
★ Adrenal glands - release adrenaline directly into the bloodstream which prepares the body for fight or flight by constricting blood vessels in the stomach. This inhibits digestion and increases heart rate.
★ Ovaries - facilitates the release of the female hormones, oestrogen and progesterone.
★ Testes - facilitates the release of the male hormone, testosterone.
THE PROCESS/HOW THE SYSTEM WORKS:
The hypothalamus (a region of the brain) receives information from many sources about the basic functions of the body and uses this information to help regulate these functions.
A signal is sent from the hypothalamus to the pituitary gland in the form of a ‘releasing hormone’.
This causes the pituitary to secrete a ‘stimulating hormone’ into the bloodstream.
This stimulating hormone then signals the target gland, e.g. adrenal glands, to secrete its hormone.
As levels of this hormone rises in the bloodstream, the hypothalamus shuts down secretion of the releasing hormone and the pituitary gland shuts down secretion of the stimulating hormone. This is negative feedback and it slows down secretion of the target gland’s hormone, resulting in stable concentrations of hormones circulating in the bloodstream (so prevents hormone levels from rising too high).
More on the major glands that you need to know too:
Pituitary gland -
It is controlled by the hypothalamus.
The pituitary gland controls the release of hormones from all other endocrine glands (so its often called the master gland).
It is the master gland
It has two main parts that release different hormones, which target different parts of the body: the anterior pituitary and the posterior pituitary.
The anterior pituitary -
Releases ACTH, as a response to stress, which stimulates the adrenal glands to produce cortisol.
Releases LH and FSH which stimulate the ovaries to produce oestrogen and progesterone and stimulate the testes to produce testosterone and sperm.
The posterior pituitary -
Releases oxytocin which stimulates the contraction of the uterus during childbirth and is also important for mother-infant bonding.
Adrenal glands -
The two adrenal glands sit on top of the kidneys.
Both are made up of two parts: the outer part is the adrenal cortex and the inner part is the adrenal medulla.
A key difference between the adrenal cortex and adrenal medulla is that the hormones released by the adrenal cortex are necessary for life whereas the hormones released by the adrenal medulla are not.
The adrenal cortex -
Produces cortisol, which regulates things like cardiovascular functions and anti-inflammatory functions.
Cortisol increases when stressed.
With low cortisol, we have low blood pressure, poor immune function, and inability to deal with stress. It is the opposite when high.
The adrenal cortex also produces aldosterone which is responsible for maintaining blood volume and pressure.
The adrenal medulla -
Releases adrenaline and noradrenaline, which prepare the body for fight or flight.
Adrenaline helps the body respond to a stressful situations, for example by increasing heart rate and blood flow to muscles and the brain.
Noradrenaline constricts the blood vessels, causing blood pressure to increase.
Ovaries -
Two ovaries are a part of the female reproductive system.
They are responsible for the production of eggs and for the hormones oestrogen and progesterone.
Progesterone, as well as being important in the menstrual cycle, has been found to be associated with heightened sensitivity to social cues.
Testes -
Testes are the male reproductive glands that produce the hormone testosterone.
Testosterone plays a role in sex drive, sperm production, and maintenance of muscle strength.
The fight or flight response AO1
The fight or flight response is a biological reaction that occurs during situations of extreme stress and it is designed to prepare the body for rapid action.
The amygdala and hypothalamus
When an individual is faced with a threat, an area of the brain called the amygdala is mobilised.
The amygdala associates sensory signals (what we see, hear or smell) with emotions associated with fight or flight, such as fear or anger.
The amygdala then sends a distress signal to the hypothalamus, which functions like a command centre in the brain, communicating with the rest of the body through the sympathetic nervous system.
The body’s response to stressors involves two major systems, one for acute stressors (i.e. short-term stressors) such as personal attack, and the second for chronic stressors (i.e. long-term stressors) such as a stressful job.
Response to acute stressors - this is associated with fight or flight.
The sympathetic nervous system
When the sympathetic nervous system (SNS) is triggered, it begins the process of preparing the body for the rapid action necessary for fight or flight.
The SNS sends a signal through to the adrenal medulla, which responds by releasing the hormone adrenaline into the bloodstream.
Adrenaline
As adrenaline circulates through the body, it causes a number of physiological changes…
The heart beats faster, pushing blood to the muscles, heart and other vital organs, and blood pressure increases.
Digestion is inhibited so that this energy is instead used for parts of the body needed for fight or flight.
Breathing becomes more rapid in order to take in as much oxygen as possible with each breath. Adrenaline also helps with the conversion of glycogen into glucose, supplying energy to parts of the body associated with the fight-or-flight response.
(Noradrenaline constricts blood vessels, causing blood pressure changes)
The parasympathetic nervous system
When the threat has passed, the parasympathetic branch of the autonomic nervous system (ANS) dampens down the stress response, returning the body to its resting state and promoting digestion (because it is inhibited when the SNS is aroused). The parasympathetic branch also slows down the heartbeat again and reduces blood pressure.
Response to chronic (ongoing) stressors:
Note that this is not fight or flight, so you don’t need to put it in a fight or flight 16 mark. You still need to know it though as it may be another question.
If the brain continues to perceive something as threatening, the second system kicks in. As the initial surge of adrenaline subsides, the hypothalamus activates a stress response system called the HPA axis. This consists of the hypothalamus, the pituitary gland and the adrenal glands.
‘H’ – The hypothalamus
The HPA axis relies on a series of hormonal signals to keep the SNS working. In response to continued threat, the hypothalamus releases a chemical messenger, corticotrophin-releasing hormone (CRH), which is released into the bloodstream in response to the stressor.
‘P’ – The pituitary gland
On arrival at the pituitary gland, CRH causes the pituitary to produce and release adrenocorticotrophic hormone (ACTH). From the pituitary, ACTH is transported in the bloodstream to its target site in the adrenal glands.
‘A’ – The adrenal glands
ACTH stimulates the adrenal cortex to release various stress-related hormones, including cortisol. Cortisol is responsible for several effects in the body and some of these are positive (e.g. a quick burst of energy and a lower sensitivity to pain) whereas others are negative (e.g. impaired cognitive performance and a lowered immune response).
Feedback
This system is also very efficient at regulating itself. Both the hypothalamus and pituitary gland have special receptors that monitor circulating cortisol levels. If these rise above normal, they initiate a reduction in CRH and ACTH levels, thus bringing cortisol levels back to normal.
The fight or flight response AO3
A limitation of the fight or flight response is that it is gender biased, as the original model was based on male behaviour. Taylor et al. (2000) found that females respond differently to stress as they are more likely to engage in a “tend and befriend” response, rather than fight or flight. This response involves tending to offspring and seeking social support (i.e. befriending), in order to protect themselves and those important to them. This aligns with females’ traditional evolutionary roles as the primary caregiver. Additionally, there are also biological explanations for these sex differences, for example the SRY gene, which is found on the Y chromosome (and therefore only present in males), is linked to increased aggression. This could explain why males are more likely to respond with fight behaviours when stressed. Therefore, these findings suggest that the fight or flight model is not fully generalisable to both sexes, reducing its explanatory power.
Another limitation of the fight or flight response is that it presents an overly simplistic view of human reactions to stress, and doesn’t account for other responses. Bray et al. has identified the existence of a third common response when under stress. This is the “freeze” response, in which individuals temporarily pause, becoming hyper-vigilant and immobile as they assess the threat before acting. This freeze response can be adaptive, as it allows time to gather information and make more appropriate decisions, which may be particularly beneficial in complex modern environments where immediate action could be risky. The inclusion of this additional response suggests that the original model lacks completeness and cannot provide a comprehensive explanation for the behaviour shown by humans in stressful situations.
A strength of the fight or flight response is that it is supported by real-life evidence. For example, during the 9/11 terrorist attacks, many individuals showed clear signs of fight or flight behaviour, such as fleeing the scene or attempting to intervene. This supports the idea that the fight or flight response can be an adaptive and functional mechanism in life-threatening situations, demonstrating its relevance in understanding human behaviour under extreme stress. Therefore, this increases the ecological validity of the model, as it shows that it can be applied to real-life situations.
A limitation of the fight or flight response is that it may have negative consequences when triggered inappropriately in modern life. This is because the high levels of adrenaline released during the stress response can strain the heart and increase the risk of cardiovascular issues. Additionally, this response may not be as useful in modern stressors, such as public speaking, where symptoms like a dry mouth (due to saliva production being inhibited) can be unhelpful. Therefore, these responses to stress, which were once useful for physical survival, now tend to be maladaptive for modern stressors. This shows that the fight or flight response may be less suited to modern-day stress, limiting its usefulness in explaining everyday behaviour.
A limitation of the fight-or-flight response explanation is that it may not fully account for gender differences in stress reactions. Research by Lee and Harley (2012) provides evidence of a genetic basis for these differences. They found that the SRY gene, found only on the male Y chromosome, promotes aggression and the fight-or-flight response by increasing the release of stress hormones like adrenaline. This suggests that the fight-or-flight model may be male-biased, as it is largely based on research using male participants and assumes a universal response to stress. Females, who lack the SRY gene, may be more likely to adopt a "tend-and-befriend" approach, focusing on social bonding and nurturing as a stress response. This undermines the generalisability of the traditional model, indicating that it may not apply equally to both sexes. Therefore, Lee and Harley’s findings highlight the need to consider biological sex differences in stress research, suggesting the fight-or-flight explanation is limited in its universality and may not reflect the full range of human responses to stress.
The brain: Localisation of function AO1
Localisation of function is the principle that specific functions (language, memory, hearing etc…) have specific locations within the brain.
(Gall’s theory of phrenology in the early 19th century was influential - believed bumps on the head in certain areas are indicative of certain traits being prominent in that person.
But this was soon discredited as Flourens demonstrated that major divisions of the brain had different functions by removing/damaging areas of the brain in animals.)
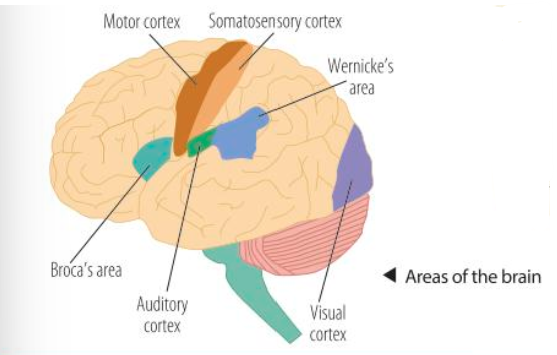
Localisation of function in the brain:
Motor and somatosensory areas
Visual and auditory centres
Language centres: Broca’s and Wernicke’s areas
YOU NEED TO KNOW WHERE THESE AREAS ARE AND WHAT THEY DO!!!
See image attached.
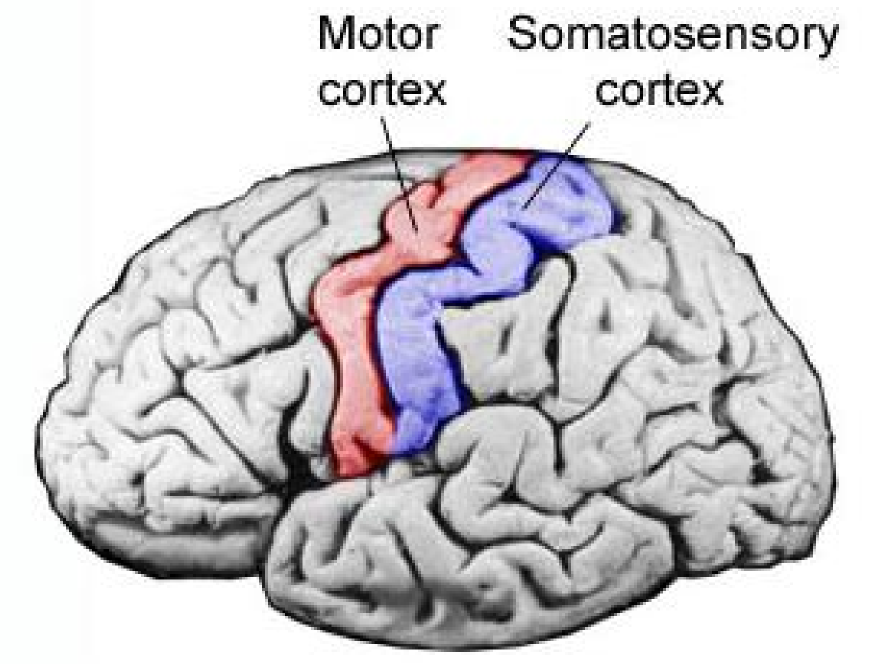
The brain: Localisation of function: Motor and somatosensory areas AO1
SEE IMAGE ATTACHED.
The motor cortex
The motor cortex is located in the frontal lobe of the brain, along a bumpy region known as the precentral gyrus.
The motor cortex is responsible for the generation of voluntary motor movements on one side of the brain, controlling the muscles on the opposite side of the body.
It is present in both the hemispheres of the brain. Different parts of the motor cortex exert control over different parts of the body. These regions are arranged logically next to one another, e.g. the region that controls the actions of the foot is next to the region that controls the leg and so on.
The somatosensory cortex
The somatosensory cortex is located in the parietal lobe of the brain, along a region known as the postcentral gyrus. The postcentral gyrus is the area of the cortex dedicated to the processing of sensory information related to touch.
The somatosensory cortex detects sensory events arising from different regions of the body. Using sensory information from the skin, the somatosensory cortex produces sensations of touch, pressure, pain and temperature, which it then localises to specific body regions.
As with the motor cortex, both hemispheres have a somatosensory cortex, with the cortex on one side of the brain receiving sensory information from the opposite side of the body.
The brain: Localisation of function: Visual and auditory centres AO1
Visual centre
The primary visual centre in the brain is located in the VISUAL CORTEX, in the occipital lobe of the brain.
However, visual processing actually begins in the retina, at the back of the eye, where light enters and strikes the photoreceptors (rods and cones). Nerve impulses from the retina are then transmitted to the brain via the optic nerve. Some nerve impulses from the retina travel to areas of the brain involved in the coordination of circadian rhythms, but the majority terminate in an area of the brain called the thalamus, which acts as a relay station, passing this information on to the visual cortex.
The visual cortex spans both hemispheres, with the right hemisphere receiving its input from the left-hand side of the visual field, while the visual cortex in the left hemisphere receives its input from the right-hand side of the visual field.
The visual cortex contains several different areas, with each of these areas processing different types of visual information, such as colour, shape or movement.
Auditory centre
The auditory centre in the brain is concerned with hearing. Most of this area lies within the temporal lobes on both sides of the brain, where we find the AUDITORY CORTEX. The auditory pathways begin in the cochlea in the inner ear, where sound waves are converted to nerve impulses, which travel via the auditory nerve to the auditory cortex in the brain.
On the journey from the cochlea to the brain, the first stop is the brain stem. Within the brain stem a basic decoding takes place, to evaluate the duration and intensity of a sound. The next stop is in the thalamus, which acts as a relay station and also carries out further processing of the auditory stimulus.
The last stop in this journey is the auditory cortex. Although the sound has already been largely decoded by this stage, in the auditory cortex it is recognised and may result in an appropriate response.
SEE IMAGE ATTACHED ON FIRST LOCALISATION OF FUNCTION FLASHCARD FOR THE LOCATIONS OF VISUAL AND AUDITORY!!!
The brain: Localisation of function: Language centres AO1
Broca’s area
This area is named after Paul Broca, the French neurosurgeon who treated a patient who offered the term ‘Tan’ because that was the only syllable this particular patient could express. Tan had an unusual disorder. Although he had been able to understand spoken language, he was unable to speak, nor express his thoughts in writing.
Subsequently, Broca studied eight other patients, all of whom had similar language deficits, along with lesions in their left frontal hemisphere. Patients with damage to areas in the right hemisphere often did not have the same language problems.
This led him to identify the existence of a ‘language centre’ in the left posterior portion of the frontal lobe of the left hemisphere (Broca, 1865). This area is believed to be critical for speech production.
Someone with damage here is said to have expressive/broca’s aphasia.
Wernicke’s area
Carl Wernicke discovered another area of the brain that was involved in understanding language. This area, named Wernicke’s area, was in the posterior portion of the left temporal lobe.
Whereas Broca’s patients could understand language but not speak, patients with a lesion in Wernicke’s area could speak but were unable to understand language.
Someone with damage to their Wernicke’s area is said to have receptive/wernicke’s aphasia.
Wernicke proposed that language involves separate motor and sensory regions located in different cortical regions.
The sensory region, located in Broca’s area, is close to the area that controls the mouth, tongue and vocal cords.
The sensory region, located in Wernicke’s area, is close to regions of the brain responsible for auditory and visual input.
The brain: Localisation of function AO3
A limitation of localisation of function is that it can be challenged by case studies where patients were able to rewire their brains after trauma. For example, Sarah Scott suffered a stroke that damaged Broca’s area, which initially left her unable to speak fluently. However, over the course of three years, her speech significantly improved. This suggests that other areas of her brain adapted and took over the function of language production. If Broca’s area was solely responsible for speech, such recovery wouldn’t be possible. This demonstrates the brain’s ability to reorganise itself after damage, which undermines the idea that specific functions are rigidly fixed to particular areas. Therefore, this suggests that while certain brain regions may be specialised, the brain is dynamic and capable of redistributing functions, suggesting localisation is not as fixed or absolute as once believed.
The belief that language is localised in the left hemisphere is not universally applicable. This is because case studies like that of JW, who was born without a left hemisphere yet was still able to develop speech, refute this. JW’s ability to speak despite lacking the hemisphere traditionally associated with language function suggests that the right hemisphere can compensate for this loss. This challenges the notion that language must be localised in the left hemisphere of the brain. Hence, this evidence undermines a core assumption of localisation theory and suggests a more flexible, distributed model of brain function.
A limitation of the localisation of function (LoF) theory is that it assumes all individuals have the same localised areas of function. Research by Braverlier et al. (1997) using a silent reading task found significant variation in the patterns of brain activation among participants. Additionally, Harasty et al. found gender differences in brain anatomy, reporting that females tend to have larger Broca’s and Wernicke’s areas than males. These findings suggest that localisation is not consistent across individuals and may vary based on factors such as gender or other biological differences. This undermines the idea that specific cognitive functions are always confined to the same regions of the brain for all people. Therefore, the theory of localisation may be overly simplistic and fails to account for the complex and variable nature of human brain organisation.
There is strong evidence supporting the localisation of language functions to specific areas of the brain, particularly from studies on aphasia. Aphasia is a language disorder that impairs the ability to communicate. Expressive aphasia, also known as Broca’s aphasia, involves difficulty in producing language and has been observed in patients like “Tan”. In contrast, receptive aphasia, linked to Wernicke’s area, results in difficulty understanding language, as shown in Wernicke’s case studies. These distinct patterns of impairment correspond closely with damage to specific brain areas as Broca’s aphasia is associated with lesions in the left frontal lobe (Broca’s area), while Wernicke’s aphasia relates to damage in the left temporal lobe (Wernicke’s area). The clear link between specific types of language deficit and particular brain regions supports the theory that language functions are localised. Thus, findings from aphasia studies provide support for the localisation of language processing in the brain, reinforcing the validity of the localisation of function theory.
A strength of the localisation of function theory is that it is supported by evidence from modern brain scanning techniques. For example, Peterson et al. (1988) used positron emission tomography (PET) scans to demonstrate that different brain areas are activated when participants perform different tasks. Listening to words activated Wernicke’s area, whereas speaking words activated Broca’s area. This supports the idea that specific areas of the brain are responsible for particular functions, in this case, different aspects of language. Brain imaging provides direct, real-time evidence of brain activity in living individuals, making the findings more objective and reliable. Therefore, the use of scientific brain imaging techniques strengthens the localisation theory by providing empirical support for the idea that cognitive functions are tied to specific brain regions.
The brain: Lateralisation and split brain research AO1
Lateralisation
Lateralisation refers to the fact that the two halves of the brain have different functional specialisations. E.g. language is lateralised to the left hemisphere.
However this raises an important question: if language is located in the left hemisphere, how can we talk about things that are experiences in the right hemisphere, for example face recognition.
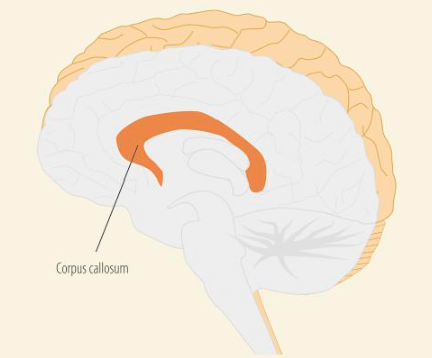
⤷ This is because the two hemispheres are connected by the corpus callosum which allows information received by one hemisphere to be sent to the other hemisphere.
We are able to study the different abilities of the two hemispheres because there was a treatment for severe epilepsy where surgeons cut the corpus callosum. These patients are referred to as split-brain patients.
See image attached.
Split-brain research, Sperry and Gazzaniga (1967)
(Btw, split-brain research is the same as research into lateralisation of the brain).
The aim was to test the capabilities of the two hemispheres.
Information from the left visual field goes to the right hemisphere and information from the right visual field goes to the left hemisphere. But, in split-brain patients, the information presented in one hemisphere has no was of travelling to the other hemisphere.
Therefore, they had split-brain patients fixate on a dot in the centre of a screen, or they would split their vision with a tachistoscope, while information was presented to either the left or right visual field.
They did a “describe what you see” test where the patient was flashed a picture, e.g. of a dog, to the right visual field and asked what they had seen. They would answer ‘dog’. However, if a picture of a cat was flashed to the left visual field the patient would say that he or she sees nothing. This is because information from the left visual field is processed by the right hemisphere (as can be seen in the picture), but as it has no language centre, cannot respond verbally. The left hemisphere, which does have a language centre, does not receive information about seeing the picture of a cat, therefore cannot say that it has seen it.
They also did a tactile test where an object was placed in the patient’s left hand. The findings showed that the patient could not describe what they felt. This is because it was processed in the right hemisphere which has no language centre.
They did a drawing task where the left-hand (controlled by the right hemisphere) would consistently draw clearer and better pictures than the right hand, even with right-handed patients. This demonstrated the superiority of the right hemisphere when it comes to visual motor tasks.
Split-brain research has taught us that:
There are differences between the two hemispheres
Left-hemisphere is responsible for speech and language
Right-hemisphere is responsible for visual-spatial processing and facial recognition.
However, it hasn’t shown us that the brain is organised into discrete regions with specific sections responsible for specific tasks.
The brain: Lateralisation and split brain research AO3
Remember that in the exam you could be asked to evaluate 'lateralisation' (the idea that the different hemispheres of the brain have different functions) generally speaking OR you may have to evaluate split brain research specifically (research that explores the notion of lateralisation).
So, you could get separate 16 markers on them.
Lateralisation
A strength of hemispheric lateralisation is that it may enhance neural processing capacity. By using only one hemisphere for a specific task, such as language, the other hemisphere is freed to perform other functions. This idea was supported by Rogers et al. (2004), who found that lateralised chickens could perform two tasks at once—finding food and watching for predators. This suggests that lateralisation improves cognitive efficiency by allowing both hemispheres to carry out different processes simultaneously, which could be adaptive in complex or demanding environments. Therefore, lateralisation may provide an evolutionary advantage by improving multitasking and overall brain efficiency.
A strength of hemispheric lateralisation is that it has been linked to immune system functioning, allowing predictions to be made. Tonnessen et al. found that individuals with strong right-hemispheric skills, such as architects and those who are mathematically gifted, were more likely to be left-handed and suffer from allergies or immune system issues. This suggests that the same genetic mechanisms involved in brain lateralisation may also influence immune development, showing a biological link that extends beyond brain function alone. As a result, researchers can make predictions about other biological traits, such as immune health, on the basis of lateralisation.
A weakness of the theory of hemispheric lateralisation is that it may not apply consistently across all individuals, as lateralisation changes with age. Szaflarski et al. found that language functions are largely lateralised to the left hemisphere in children and young adults, but after the age of 25, this lateralisation begins to decrease. This suggests that older adults start to rely on both hemispheres more equally, possibly to compensate for age-related cognitive decline. This challenges the idea that lateralisation is a fixed, universal feature of brain organisation. Therefore, the theory may lack generalisability, as it doesn’t fully account for individual or age-related differences in brain function.
A strength of hemispheric lateralisation is that it is supported by research using brain imaging techniques, which provide objective and reliable data. For example, fMRI studies have shown that certain functions consistently activate one hemisphere more than the other - for instance, language tasks tend to activate the left hemisphere, while spatial and emotional tasks often activate the right. This scientific evidence supports the idea that lateralisation is a real and measurable phenomenon. The use of modern neuroimaging adds credibility because it allows researchers to observe brain activity in real time, offering strong empirical support for the theory. Therefore, the validity of hemispheric lateralisation is strengthened by the use of objective methods.
Split-brain research
A strength of split-brain research is that it has useful real-world implications for understanding and supporting individuals with brain damage. Findings from these studies have increased our understanding of how the two hemispheres function independently and how certain functions, like language or visual processing, are lateralised in the brain. This knowledge can inform rehabilitation strategies for patients who have suffered strokes or undergone brain surgery, by identifying which hemisphere is affected and targeting therapy accordingly. Therefore, split-brain research goes beyond theory, offering practical value in clinical settings to improve patient care and recovery outcomes.
A limitation of early split-brain research is that it may have overestimated the role of the left hemisphere in language. Gazzaniga (1998) pointed out that some split-brain findings were challenged by later case studies, such as patient J.W., who developed the ability to speak using the right hemisphere (Turk et al., 2002). This shows that language function is not strictly lateralised to the left hemisphere, and that the brain may have more plasticity and compensatory mechanisms than originally thought. Such findings undermine the rigid view of lateralisation and highlight the brain’s adaptability.
A limitation of split-brain research is the small and unrepresentative sample sizes used. Andrews (2001) noted that many studies involved just one or a few participants, some of whom had other medical issues or incomplete split-brain procedures. This reduces the generalisability of the findings, as the unique circumstances of these individuals may not reflect how a fully functioning split-brain operates in the general population. Consequently, conclusions about hemispheric lateralisation drawn from such studies may lack population validity.
A limitation of split-brain research is that not all patients have their brains split in exactly the same way. Some individuals may have had only partial sectioning of the corpus callosum or other variations in the procedure, which affects the extent to which information can be transferred between hemispheres. This lack of consistency means that the findings from split-brain studies may not be reliable or generalisable, as the brain functioning of each patient could differ significantly. Therefore, conclusions drawn from split-brain research may be based on unrepresentative cases, weakening the validity of the findings.
The brain: Plasticity and functional recovery AO1
Plasticity
Plasticity refers to the brain’s ability to modify its own structure and function as a result of either brain trauma or through experience/learning.
As people gain new experiences, neuron pathways that are used frequently develop stronger connections, whereas neurons that are rarely or never used eventually die.
By developing new connections and pruning away weak ones, the brain is able to constantly adapt to a changing environment.
Therefore neuronal organisation changes with experience. We have example of this occurring….
Playing video games:
Playing video games makes many different complex cognitive and motor demands. Kühn et al. (2014) compared a control group with a video game training group that was trained for two months for at least 30 minutes per day on the game Super Mario. They found a significant increase in grey matter in various brain areas including the cortex, hippocampus and cerebellum whereas no such increase was found with the control group, who played no videogames. This means those areas were more densely packed with neurons following sustained video game training. The researchers concluded that video game training had resulted in new synaptic connections in brain areas involved in spatial navigation, strategic planning, working memory and motor performance – skills that were important in playing the game successfully.
Maguire’s taxi driver study:
Maguire used MRI scans to compare the brains of London taxi drivers with those of non-taxi drivers. London taxi drivers undergo extensive training which involves memorising the layout of over 25,000 streets and thousands of landmarks.
The findings showed that taxi drivers had hippocampi that were more densely packed with neurons compared to the control group. Also, the volume of the posterior hippocampus correlated positively with the amount of time spent as a taxi driver. This is evidence for plasticity, specifically how the brain rewires via learning.
Functional recovery
Functional recovery is a type of plasticity, describing how the brain rewires after brain damage/trauma e.g. through neuronal unmasking.
There are three ways in which functional recovery can occur…
Neuronal unmasking:
There are ‘dormant synapses’ in the brain. These are synaptic connections that exist anatomically but their function is blocked.
Under normal conditions these synapses may be ineffective because the rate of neural input to them is too low for them to be activated. However, increasing the rate of input to these synapses, as would happen when a surrounding brain area becomes damaged, can then open (or ‘unmask’) these dormant synapses.
The unmasking of dormant synapses can open connections to regions of the brain that are not normally activated, creating a lateral spread of activation which, in time, gives way to the development of new structures.
Axonal sprouting:
This is the growth of new nerve endings which connect with other undamaged neurons to form new neuronal pathways.
This can also involve neuronal/axonal regeneration whereby, if just partially damaged, the axon can regenerate and form a new connection in order to recover function.
Homologous recruitment:
This is when a similar area in the opposite (undamaged) hemisphere of the brain takes over the function of a damaged area. This helps maintain or restore abilities lost due to brain injury.
(Stem cells:
Stem cells are unspecialised cells that have the potential to give rise to different cell types that carry out different functions, including taking on the characteristics of nerve cells. One way this could work in functional recovery is stem cells could be implanted into the brain and would directly replace dead or dying cells. There have been clinical trials involving stem cells being used to help stroke victims but it is not yet a widely approved treatment for stroke victims)
Note: if you get a STEM questions don’t mention stem cells as a way we can recover because with the stem cell method, the brain isn’t recovering on its own and is instead recovering due to human intervention.
The brain: Plasticity and functional recovery AO3
Note: you could get a 16 marker on just plasticity or a 16 marker on just functional recovery.
If you get one on plasticity, you can talk about how the brain rewires through learning/experience and also after trauma. BUT if you get one on functional recovery, just talk about rewiring after trauma.
Plasticity:
Could use the video game study or the taxi driver study used in the AO1.
Brain plasticity tends to decrease with age, becoming less efficient. Boyke et al. (2008) found that 60-year-olds trained to juggle showed increased grey matter in the visual cortex, though it reversed after stopping practice. This shows that while plasticity is still possible in older adults, it may be more temporary and reliant on continued stimulation. This suggests that plasticity is not entirely age-dependent, but age does influence how long-lasting and adaptable brain changes can be.
Animal research provides strong evidence for experience-dependent plasticity. Kempermann et al. (1998) found that rats in enriched environments (rat circus) developed more neurons in the hippocampus than those in standard cages. This indicates that a stimulating environment can physically change the brain’s structure, enhancing its learning and memory capacity. Although generalising to humans has limitations, this supports the biological basis of plasticity.
Research into plasticity has real-word application. This is because it has influenced stroke and brain injury rehabilitation, encouraging therapies that help patients form new neural connections. For example, therapy that stimulates brain regions can aid recovery by enhancing plastic responses. This shows that plasticity research has practical, real-world benefits in healthcare.
There is support for plasticity from case studies. For example, at 18, Sarah Scott experienced a major stroke that left her with aphasia and motor impairments. Initially, she struggled with speech, understanding, and movement. However, over the years, she made remarkable progress through intensive therapy, developing new ways to communicate and regaining physical ability. Her brain was able to reorganise functions, with undamaged areas compensating for those affected by the stroke. This was facilitated by consistent rehabilitation, showing how plasticity can be activated through targeted stimulation and effort over time. Sarah's case highlights the real-world impact of brain plasticity, demonstrating how recovery is possible even after severe damage, especially when supported by therapy and environmental stimulation.
Functional recovery:
There is strong fMRI-based evidence supporting the role of neuronal unmasking in recovery. Ward et al. (2003) found that after a stroke, patients attempting hand movements showed brain activity in areas outside the primary motor cortex. This suggests that regions not normally involved in that function were being recruited to compensate, showing real-time neural adaptation during recovery. The use of fMRI gives this evidence high internal validity, as it directly measures changes in brain activity during attempted movement.
Case studies can provide support for functional recovery. For example, JW, who developed with only a right hemisphere due to early brain damage, demonstrated the ability to use language, which is typically managed by the left hemisphere. This shows that the right hemisphere can fully take over complex cognitive functions, like language, which are normally lateralised. It reflects the brain’s capacity for functional reorganisation, particularly during early developmental stages. JW’s case strongly supports the idea that homologous recruitment is not just a compensatory process, but a mechanism capable of sustaining high-level cognitive functioning after significant structural loss.
Controlled animal research provides robust support for axonal sprouting as a biological mechanism in recovery. Carmichael et al. (2015) induced strokes in the motor cortex of mice and treated them with GDF10, a growth-promoting compound. Within four weeks, the mice showed both axonal growth and full restoration of motor performance. This study offers clear causal evidence that stimulating axonal growth can directly lead to functional recovery, with performance levels matching those of non-injured mice. The findings provide strong scientific support for axonal sprouting and suggest potential for future therapeutic applications targeting biological repair pathways.
A limitation of functional recovery is that research into it often faces ethical and practical constraints, particularly when it comes to experimental studies in humans. This is because it is ethically not possible to deliberately induce brain damage, meaning researchers must rely on naturally occurring injuries or use animal models. While animal studies, like those involving induced strokes in mice, offer experimental control, they raise concerns about applicability to humans due to differences in brain structure, complexity, and cognitive function. As a result, the most rigorous evidence often comes from non-human subjects, which limits how confidently the findings can be translated into human clinical practice.
Ways of studying the brain AO1
A variety of methods are used by research scientists in order to study the brain:
Scanning techniques: fMRI, EEG, ERP
Post-mortem examinations
Functional Magnetic Resonance Imaging (fMRI)
This is a technique for measuring changes in brain activity while a person does a task.
It does this by using magnets to track oxygenated blood flow. Oxygenated blood and deoxygenated blood have different magnetic properties, and if a particular area of the brain becomes more active, it requires more oxygen, therefore oxygenated blood there will be higher.
The fMRI detects these changes in blood flow and the receiver coils in the scanner and researchers are able to produce maps showing which areas of the brain are involved in particular mental activity.
Electroencephalogram (EEG)
This technique measures electrical activity in the brain.
Electrodes placed on the scalp detect small electrical charges that occur due to activity of brain cells/neurons. This is because neurons communicate using tiny electrical impulse, so when lots of neurons fire together, they create brain waves.
When electrical signals from the different electrodes are graphed over a period of time, the resulting representation is called an EEG.
Different types of brain activity produce different wave shapes.
EEG focuses on the general brain wave activity (not elicited by a specific stimuli because that would be ERP)
Event-related potentials (ERPs)
ERPs use the same electrode headsets that are used in the case of EEGs, but ERPs measure small voltage changes in the brain that are triggered by specific events or stimuli.
Event-related potentials (ERPs) are very small voltage changes in the brain that are triggered by specific events or stimuli, such as cognitive processing of a specific stimulus. ERPs are difficult to pick out from all the other electrical activity being generated within the brain at a given time.
To establish a specific response to a target stimulus requires many presentations of the stimulus and these responses are then averaged together. Any extraneous neural activity that is not related to the specific stimulus will not occur consistently, whereas activity linked to the stimulus will. This has the effect of cancelling out the background neural ‘noise’, making the specific response to the stimulus in question stand out more clearly.
ERPs can be divided into two categories. Waves occurring within the first 100 milliseconds after presentation of the stimulus are termed ‘sensory’ ERPs as they reflect an initial response to the physical characteristics of the stimulus.
ERPs generated after the first 100 milliseconds reflect the manner in which the subject evaluates the stimulus and are termed ‘cognitive’ ERPs as they demonstrate information processing.
Post-mortem examinations
After death, the brain is carefully removed and preserved. Its structure is examined.
Researchers compare what they find in the brain to the person’s known behaviours or symptoms when they were alive e.g., if someone had speech problems, scientists might look for damage in Broca’s area.
Ways of studying the brain AO3
fMRI
A strength of fMRI is that it provides a more objective and reliable measure of mental processes than relying on self-report methods. Verbal reports can be biased, inaccurate, or incomplete, especially when individuals are unaware of or unable to describe their experiences. fMRI captures brain activity directly through imaging, offering insight into mental functions like memory, emotion, or decision-making that might be difficult to articulate. This enables researchers to study things such as unconscious processing or disorders affecting communication. As a result, fMRI enhances the understanding of complex psychological processes by providing data that verbal methods alone cannot capture.
A limitation of fMRI is that it does not directly measure neural activity. Instead, fMRI detects changes in blood oxygenation levels that occur in response to increased brain activity. This indirect measurement means that the technique only infers brain activity based on blood flow, which may not accurately reflect the timing or intensity of neural processes. As such, fMRI may not provide a fully precise or quantitative understanding of mental functioning. Therefore, while fMRI offers useful insights, its reliance on blood flow limits its ability to capture the true complexity of brain activity.
EEG
A strength of EEG is its ability to record brain activity in real time. EEG measures electrical activity through electrodes placed on the scalp, capturing rapid changes as they occur in milliseconds. This high temporal resolution allows researchers to pinpoint the exact moment certain brain processes happen in response to specific tasks or stimuli. It’s particularly valuable when studying time-sensitive cognitive functions like attention and perception. Therefore, EEG is highly effective for investigating the timing of brain activity and how it relates to behaviour.
A limitation of EEG is its inability to measure activity in deeper brain structures. EEG electrodes placed on the scalp can only record electrical activity from the outer layers of the brain, such as the cerebral cortex. This means important regions like the hypothalamus or hippocampus -which are involved in functions like memory, emotion, and hormonal regulation - remain inaccessible with standard EEG. As a result, researchers may miss critical data when studying complex cognitive processes. Therefore, EEG provides an incomplete picture of brain activity, particularly when deeper brain areas are involved.
ERGs
A strength of ERPs is that they provide a continuous and time-locked measure of brain activity in response to specific stimuli. ERPs are derived from EEG recordings and isolate brain responses triggered by particular events, such as a visual or auditory stimulus. This allows researchers to observe how mental processing unfolds over time and how it's influenced by experimental changes - such as variations in stimulus type or attention level. It’s especially useful in cognitive psychology for tracking perception, attention, and decision-making. As a result, ERPs are valuable for exploring how the brain responds to external events and how this processing changes under different conditions.
A limitation of ERP is that the signals are very small and difficult to isolate. The brain produces a lot of electrical activity unrelated to the stimulus, which can mask the specific ERP signal researchers are trying to detect. To overcome this, researchers must repeat the stimulus many times and average the results to cancel out background noise. This process is time-consuming and can be tiring for participants, especially in clinical or developmental settings. Therefore, while ERPs weak signal strength makes the data collection process lengthy and more demanding.
Post-mortem examinations
A strength of post-mortem examinations is their ability to explore aspects of the brain that non-invasive methods cannot reach. Post-mortem studies allow direct access to brain tissue, enabling researchers to study microscopic structures and biochemical details such as neurotransmitter levels or cellular abnormalities. This is especially valuable for investigating deeper brain regions - like the hypothalamus or hippocampus - which are difficult to study with techniques like EEG or fMRI due to depth or resolution limits. Therefore, post-mortem studies provide a unique and detailed understanding of the brain's internal structure and chemistry, particularly for complex disorders.
A limitation of post-mortem studies is that the brain can be affected by many uncontrolled variables. Factors such as the stage of illness, how the person died, how long after death the brain was examined, and any medications they were taking can all alter brain structure or chemistry. These confounding factors make it difficult to determine whether observed abnormalities are genuinely related to the condition being studied or are simply artifacts caused by other influences. Therefore, post-mortem findings may lack reliability and should be interpreted cautiously, especially when forming conclusions about brain-behaviour relationships.
Circadian rhythms AO1
Biological rhythms are cyclical changes in the way that biological systems behave. Biological rhythms vary in length…
Circadian rhythms are a pattern of behaviour that generally occur once every 24 hours i.e. the sleep–wake cycle once every day.
Infradian rhythms and Ultradian rhythms will be covered next.
The nature of circadian rhythms:
Our circadian rhythms are driven by our body clocks (found in all of the cells of the body) and synchronised by the endogenous pacemaker, the suprachiasmatic nuclei (SCN), found in the hypothalamus.
This pacemaker must constantly be reset so that our bodies are in synchrony with the outside world. (e.g. if you move to Australia from UK, it wouldn’t make sense to have your biggest sleep drive at 10pm UK time because that’s 9am in Australia)
Light provides the primary input to this system, setting the body clock to the correct time. Light is an exogenous zeitgeber (i.e. an external cue of time) so our circadian rhythm/SCN responds to it as a means to re-set.
The SCN then uses this information to coordinate the activity of the entire circadian system.
The sleep-wake cycle:
The main example of a circadian rhythm subject is the sleep–wake cycle. This is our psychological perception of feeling tired and fatigued versus feeling alert and awake. Our sleep-wake cycle is circadian because it describes the biological ‘peaks and troughs’ of different chemicals in the body that make us feel strong sleep drives and period of alertness that work roughly to a 24 hour rhythm.
Sleep and wakefulness are not determined by the circadian rhythm alone, but are also under homeostatic control. When we have been awake for a long period of time, our bodies are using up lots of energy so homeostasis tells us that we must sleep.
Other circadian rhythms:
Core Body Temperature
Sleep occurs when core temperature begins to drop.
In the last hours of sleep, body temperature rises again.
This rise helps promote alertness in the morning.
Hormone Production
Hormone release follows a circadian rhythm.
Example: Melatonin peaks during the hours of darkness.
Melatonin regulates sleepiness, dropping again when it becomes light.
Circadian rhythms AO3
Michel Siffre’s temporal isolation study provides research support for both the existence of an endogenous pacemaker (SCN) and the importance of light in regulating circadian rhythms. This is because when Siffre lived underground with no external cues such as daylight, clocks, or radio, his sleep–wake cycle continued, showing the presence of a free-running circadian rhythm controlled by the SCN. However, his rhythm drifted beyond 24 hours, sometimes stretching to 48 hours, and he lost track of real time. This shows that the SCN is responsible for generating circadian rhythms internally, but without the external zeitgeber of light, the rhythms become de-synchronised and misaligned with the environment. Light is therefore necessary to entrain the SCN and keep the circadian rhythm on a 24-hour cycle. Therefore, Siffre’s findings support the role of the SCN as the master clock and that light is an exogenous zeitgeber that synchronises our circadian rhythms with the outside world.
However, a limitation of early circadian rhythm studies is that participants were not fully isolated from artificial light. For example, in Michel Siffre’s temporal isolation studies, participants were shielded from natural light but still exposed to artificial light. Czeisler et al. (1999) demonstrated that even dim artificial light can significantly alter circadian rhythms, shifting cycles to as short as 22 hours or as long as 28 hours. This suggests that early studies may have produced inaccurate estimates of the “free-running” circadian rhythm because artificial light could have acted as an unintended extraneous variable, skewing the results. Therefore, research into circadian rhythms must account for the confounding effects of artificial light to ensure valid conclusions about the natural timing of human biological rhythms.
A strength of circadian rhythm research is its practical application in real-world settings. Research into circadian rhythms has helped us understand the negative effects of shift work and jet lag. For example, night-shift workers often experience disrupted biological clocks when working without natural light and trying to sleep during daylight hours. By applying research findings, workers can use specially designed lights that mimic daylight to stay alert during shifts and use blackout blinds or eye masks to improve sleep quality during the day. Similarly, travellers can use “light box therapy” to reduce jet lag by promoting alertness in line with their new time zone. This shows how circadian rhythm research not only improves scientific understanding but also provides practical solutions that enhance wellbeing and productivity in everyday life.
There is research support for the importance of light as an exogenous zeitgeber in regulating circadian rhythms. Hughes (1977) studied participants stationed at the British Antarctic Station and found that in February, cortisol levels followed the expected daily cycle, peaking in the morning as participants awoke. However, after three months of continuous darkness, cortisol release patterns shifted, with peak levels occurring at noon instead of morning. This demonstrates that extreme changes in light exposure, such as those in polar regions, can disrupt the regulation of circadian rhythms. Therefore this supports the idea that light/exogenous zeitgebers are responsible for variations in circadian hormone release.
A limitation of circadian rhythm research is that there are significant individual differences between people. For example, Czeisler et al. (1999) found that circadian cycles can range widely from 13 to 65 hours. Similarly, Duffy et al. (2001) showed that some individuals are naturally “morning people” (preferring to rise early and sleep early), while others are “night owls” (preferring to wake and sleep later). This suggests that circadian rhythms are not universal and that biological clocks vary considerably between individuals. As a result, findings from research may not apply equally to everyone, limiting the generalisability of conclusions about circadian rhythms. Therefore, while circadian rhythm research provides valuable insights, recognising individual differences is crucial to avoid oversimplifying how biological clocks function across the population.
Ultradian and Infradian rhythms AO1
Two other important biological rhythms are ultradian and infradian.
Ultradian rhythms:
Cycles that last less than 24 hours.
Example: light and deep sleep
So, the sleep-wake cycle is a circadian rhythm, but within the sleep cycle, the ultradian rhythm exists. This is the 5 stages that make up a typical night’s sleep.
Sleep stages:
The ultradian rhythm follows a pattern of alternating REM (rapid eye movement) and NREM (non-rapid eye movement) sleep, which consists of stages one through to four.
This cycle repeats itself about every 90–100 minutes throughout the night, with different stages having different durations.
A complete cycle consists of a progression through the four stages of NREM sleep before entering a final stage of REM sleep, then the whole cycle starts all over again.
Most of what we know about sleep stages comes from EEGs (the sleep stages cause change in brain waves).
Stage 1
4–5%: Light sleep. Muscle activity slows down. Occasional muscle twitching.
Stage 2
45–55%: Breathing pattern and heart rate slows. Slight decrease in body temperature.
Stage 3
4–6%: Deep sleep begins. Brain begins to generate slow delta waves.
Stage 4
12–15%: Very deep sleep. Rhythmic breathing. Limited muscle activity. Brain produces delta waves.
Stage 5
20–25%: Rapid eye movement. Brainwaves speed up and dreaming occurs. Muscles relax and heart rate increases. Breathing is rapid and shallow.
The Basic Rest Activity Cycle:
Kleitman (1969) referred to the 90-minute cycle found during sleep as the Basic Rest Activity Cycle, or BRAC.
He argues that this 90-minute ultradian rhythm continues during the day, even when we are awake.
But in the day, rather than moving through sleep stages, we move through states of alertness and physiological fatigue approximately every 90 mins (so still an ultradian rhythm.. just not asleep).
An everyday observation for the existence of a BRAC is 10.30 am coffee breaks (because it divides the 9am-12pm morning into 90 min phases).
Infradian rhythms:
Rhythms that have a duration of over 24 hours (longer than a day). So, they can last days, months or maybe even a year.
Example: the menstrual cycle.
Weekly rhythms:
There are differences in human behaviour that conform to a weekly cycle.
For example, male testosterone levels are elevated at weekends and young couples report more sexual activity at weekends than on weekdays.
The frequency of births at weekends is lower than on weekdays.
Halberg et al. (2002) reported seven-day rhythms of blood pressure and heart rate in humans.
Underlying biological cycles could dictate these differences, hence infradian rhythms, but it could also be the environment causing these changes i.e. the rhythms are influenced by external cues.
Monthly rhythms: the human menstrual cycle:
A woman’s menstrual cycle lasts about one month and there are considerable variations in the length of this cycle, with some women experiencing a relatively short 23-day cycle whereas others have a cycle as long as 36 days (Refinetti, 2006).
The average appears to be around 28 days.
The menstrual cycle is regulated by hormones, which either promote ovulation or stimulate the uterus for fertilisation.
Ovulation occurs roughly halfway through the menstrual cycle, when oestrogen levels peak, and usually lasts for 16 to 32 hours. After the ovulatory phase, progesterone levels increase in preparation for the possible implantation of an embryo in the uterus.
Most women experience a peak in LH on day 14. And, provided their menstrual cycle is regular, they will always experience their peak LH on day 14 of each newly started cycle!
Annual rhythms:
In most animals, annual rhythms are related to the seasons (e.g. migration), but in humans the calendar year appears to influence behaviour regardless of changes in temperature.
Research suggests a seasonal variation in mood in humans, especially in women (Magnusson, 2000), with some people becoming severely depressed during the winter months. This is seasonal affective disorder (SAD).
The winter is also associated with an increase in heart attacks, which varies seasonally and peaks in winter. In fact, there is a annual rhythm in human deaths, with most deaths occurring in January (Trudeau, 1997).
NOTE: If asked for an example of infradian rhythms, go for the menstrual cycle (monthly) or the SAD (annual) rather than the weekly ones because they have more objective research about them and there is also more to say about them.
Ultradian and Infradian rhythms AO3
Ultradian rhythms:
A strength of the ultradian rhythms is that the basic rest activity cycle (BRAC) is supported by research from a real-world performance. Ericsson et al. (2006) studied elite violinists and found that their practice sessions typically lasted no longer than 90 minutes before they took a break, consistent with the 90-minute BRAC cycle. The best violinists also napped more frequently than their teachers to recover from practice. This supports Kleitman’s claim that fatigue is a natural characteristic of the BRAC cycle and shows how the rhythm applies beyond sleep, extending into patterns of alertness and productivity during the day. Ericsson also found similar patterns in other high-performing groups such as musicians, athletes, and writers, strengthening the reliability of the findings. Therefore, the BRAC is not only a theoretical model but also has strong ecological validity, as it is reflected in the behaviour of elite performers in real-life contexts.
There is research support for the existence of ultradian rhythms in sleep. Dement and Kleitman (1957) monitored participants’ EEG recordings while they slept and woke them during different stages of sleep. They found that brainwave changes could clearly distinguish each stage of sleep. Moreover, when participants were awakened during REM sleep, they reported dreaming 80–90% of the time. This demonstrates that sleep consists of distinct stages that follow a 90-minute ultradian rhythm, with REM sleep strongly linked to dreaming. The use of EEG recordings provides objective, scientific evidence to support these findings, increasing the reliability of conclusions about sleep patterns. Therefore, Dement and Kleitman’s study provides strong empirical support for the ultradian rhythm of sleep stages.
A strength of ultradian rhythm research is that it is supported by evidence from controlled sleep lab studies. For example, Tucker et al. studied participants over 11 days and nights using EEG headsets and found evidence for ultradian sleep stages. He also observed individual differences in cycle length, with some participants’ stages lasting slightly longer or shorter than the typical 90 minutes. This suggests that while ultradian rhythms are a consistent biological process, individual variation plays a role in their expression. Therefore, this research not only supports the existence of ultradian rhythms but also highlights their biological basis, since differences could not be explained by environmental factors.
NOTE: You could always use some of the earlier EEG AO3 points since most of what we know about sleep stages comes from EEGs!!
Infradian rhythms:
There is research support for the role of infradian rhythms in Seasonal Affective Disorder (SAD). Studies show that individuals with SAD have higher melatonin levels during winter, which can be treated using light box therapy to lower melatonin and reduce depressive symptoms. This demonstrates that SAD is linked to infradian cycles, as seasonal changes in melatonin levels occur on an annual basis and directly influence mood Therefore, infradian rhythms are not only observable in biological cycles like menstruation but also in seasonal mood disorders, showing their broader impact on human functioning.
Research suggests that infradian rhythms such as the menstrual cycle may be influenced by exogenous cues. For example, studies have shown that women who live together often experience synchronised menstrual cycles, and one experiment found that rubbing women’s sweat on the upper lips of other women could bring their cycles into alignment. This indicates that infradian rhythms are not solely controlled by internal biological processes but can also be shaped by external factors. So, a strength of infradian rhythm research is that it has led to insight as to how such infradian rhythms (like the menstrual cycle) are perhaps altered by exogenous cues.
A strength of infradian menstrual cycle research is that it has highlighted the complexities of infradian rhythms. Penton-Voak found that women’s mate preferences vary across the menstrual cycle, with females preferring masculine faces during the fertile phase and more feminine faces during the non-fertile phase. This makes evolutionary sense, as masculine traits are associated with good genes and reproductive success, while feminine traits are linked with nurturing qualities important for long-term parenting. This shows how the menstrual cycle not only regulates fertility but also influences behaviour in ways that may have adaptive value. Therefore, menstrual cycle research has deepened our understanding of infradian rhythms by revealing their influence on complex behaviours such as mate choice, not just hormonal regulation.
Research into infradian rhythms has linked them to the phases of the moon, but this belief is widely disputed. For example, midwives often believe more babies are born during a full moon, but statistical studies (Arliss et al., 2005) show this is purely subjective. Similarly, some mental health professionals think the moon alters behaviour, but consistent scientific evidence is lacking (Vance, 1995).This highlights that while correlations have been reported between the lunar cycle and aspects of human behaviour, there is no evidence of causation (Foster & Roenneberg, 2008). Therefore, although lunar rhythm research is popular, it demonstrates the danger of relying on correlations without scientific backing, limiting its credibility as an explanation for infradian rhythms.
Endogenous pacemakers and Exogenous zeitgebers AO1
NOTE: A 16 marker on ‘endogenous pacemakers and exogenous zeitgebers’ is very similar to a 16 marker on ‘circadian rhythms’.
Endogenous pacemakers:
Endogenous pacemakers refers to anything whose origins are within the organism (INTERNAL), and which act like a clock, keeping us to a rhythm (pacemaker).
So endogenous pacemakers are internal body clocks.
The most important endogenous pacemaker in mammals is the suprachiasmatic nucleus (SCN).
The SCN:
The SCN is a tiny cluster of nerve cells which lies in the hypothalamus.
The SCN plays an important role in generating the body’s circadian rhythm. It acts as the ‘master clock’, controlling other brain regions that control sleep and arousal, and has control over other biological clocks throughout the body.
Neurons within the SCN spontaneously synchronise with each other, so that their target neurons in sites elsewhere in the body receive correctly time-coordinated signals.
These peripheral clocks can maintain a circadian rhythm, but not for very long, which is why they must be controlled by the SCN.
The SCN receives information about light levels via the optic nerve. This happens even when our eyes are shut, because light penetrates the eyelids.
The pineal gland:
The SCN then sends signals to the pineal gland to increase levels of melatonin at night and to decrease melatonin levels in the morning.
Melatonin induces sleep by inhibiting the brain mechanisms that promote wakefulness.
Despite the endogenous nature of our body clocks, they are still quite sensitive to exogenous zeitgebers (e.g. light).
Exogenous zeitgebers:
Exogenous zeitgebers are environmental events that are responsible for entraining the biological clock of an organism.
The most important exogenous zeitgeber for animals is light.
Light:
Receptors in the SCN are sensitive to changes in light levels during the day and use this information to synchronise the activity of the body’s organs and glands.
Light resets the internal biological clock each day, keeping it on a 24-hour cycle.
Rod and cones in the retina detect light to form images.
However, there is a third type of light-detecting cell called which gauges overall brightness to help reset the biological clock. The protein called melanopsin is critical in this system as it is sensitive to natural light and melanopsin cells send signals to the SCN to set the daily body clock.
Social cues:
Social stimuli, such as mealtimes and social activities, may also have a role as zeitgebers.
Endogenous pacemakers and Exogenous zeitgebers AO3
NOTE: These are just the same AO3 points that I’m using for circadian rhythms, just slightly tweaked.
Michel Siffre’s temporal isolation study provides research support for both the existence of an endogenous pacemaker (the SCN) and the importance of exogenous zeitgebers (specifically light). This is because when Siffre lived underground with no external cues such as daylight, clocks, or radio, his sleep–wake cycle continued, showing the presence of a free-running rhythm controlled by the SCN. However, his rhythm drifted beyond 24 hours, sometimes stretching to 48 hours, and he lost track of real time. This shows that the SCN, as an endogenous pacemaker, is responsible for generating rhythms internally, but without the exogenous zeitgeber of light, these rhythms become de-synchronised and misaligned with the environment. Light is therefore necessary to entrain the SCN and keep biological rhythms on a 24-hour cycle. Therefore, Siffre’s findings support the role of the SCN as the master endogenous pacemaker and highlight that light is a crucial exogenous zeitgeber for maintaining synchrony with the external world.
However, a limitation of early research into endogenous pacemakers and exogenous zeitgebers is that participants were not fully isolated from artificial light. For example, in Michel Siffre’s temporal isolation studies, participants were shielded from natural light but still exposed to artificial light. Czeisler et al. (1999) demonstrated that even dim artificial light can significantly alter biological rhythms, shifting cycles to as short as 22 hours or as long as 28 hours. This suggests that early studies may have produced inaccurate estimates of the role of the SCN as an endogenous pacemaker, because artificial light could have acted as an unintended exogenous zeitgeber, skewing the results. Therefore, research into pacemakers and zeitgebers must account for the confounding effects of artificial light to ensure valid conclusions.
A strength of research into endogenous pacemakers and exogenous zeitgebers is its practical application in real-world settings. For instance, research has helped us understand the negative effects of disrupted biological clocks in shift work and jet lag. Night-shift workers often experience misalignment between their SCN-driven rhythms and the external environment when working without natural light and attempting to sleep during the day. By applying research findings, workers can use specially designed lights that mimic daylight to stay alert, and blackout blinds or eye masks to improve sleep. Similarly, travellers can use “light box therapy” to entrain their SCN to a new time zone more quickly. This shows how understanding pacemakers and zeitgebers not only advances science but also provides practical solutions that enhance wellbeing and productivity.
There is research support for the importance of exogenous zeitgebers, particularly light, in regulating the SCN. Hughes (1977) studied participants stationed at the British Antarctic Station and found that in February, cortisol levels followed the expected daily cycle, peaking in the morning as participants awoke. However, after three months of continuous darkness, cortisol release patterns shifted, with peak levels occurring at noon instead of morning. This demonstrates that extreme changes in light exposure can disrupt the regulation of rhythms, highlighting that the SCN alone (as an endogenous pacemaker) is not sufficient to maintain synchrony. Therefore, this supports the idea that light acts as a crucial exogenous zeitgeber that interacts with the SCN to regulate biological processes such as hormone release.