Laryngopharynx / Hypopharynx
1/6
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
7 Terms
Overview
Anatomy and Boundaries of the Laryngopharynx:
The laryngopharynx connects the oropharynx to the larynx and ultimately the esophagus.
The region is bordered by structures such as the epiglottis and the surrounding pharyngeal muscles.
Epiglottis – The Key Flat Valve:
The epiglottis plays a crucial role in protecting the airway during swallowing, preventing food or liquid from entering the larynx and trachea.
Pharyngeal Muscles:
These muscles are responsible for the movement of the food bolus during swallowing. Their coordination is vital for effective swallowing and ensuring that food is directed into the esophagus and not the airway.
Innervation:
The vagus nerve provides the motor innervation to the pharyngeal muscles, while sensory innervation is supplied by branches of the glossopharyngeal nerve.
Impact of Interventions for Head and Neck Cancer:
Treatments such as surgery, radiation, and chemotherapy can have significant implications for swallowing function in the laryngopharynx.
Complications from these interventions can lead to dysphagia (difficulty swallowing), which needs to be managed by a multidisciplinary team, including speech pathologists.
Implications for Practice:
Understanding the anatomy, function, and potential complications in this region is crucial for managing patients undergoing treatment for head and neck cancer. Interventions may cause both structural and functional changes, and speech pathologists play a critical role in assessing and rehabilitating swallowing disorders related to these treatments.
Boundaries
The laryngopharynx or hypopharynx has the following boundaries:
Lateral and Posterior Boundaries:
Formed by the inferior pharyngeal constrictor muscles.
Lower End:
The laryngopharynx ends at the level of the C6 vertebra, where it connects to the esophagus.
Implications of Soft Tissue Boundaries
The boundaries of the laryngopharynx are soft tissue structures, which means they are movable and can change shape or position based on muscular contraction.
These boundaries are also under control by neural innervation, which regulates movement and coordination during processes such as swallowing.
The ability of these soft tissue boundaries to move and adapt plays a critical role in swallowing dynamics and in managing the passage of food from the pharynx into the esophagus, preventing aspiration into the airway.
Openings
Superior Opening:
This is an unnamed opening that connects the laryngopharynx to the oropharynx.
Anterior Opening:
This is the laryngeal inlet (or aditus), which is the opening to the larynx.
It is guarded by the epiglottis, a flat valve made of elastic cartilage, which plays a key role in protecting the airway during swallowing.
The laryngeal inlet connects the laryngopharynx with the larynx.
Inferior Opening:
The cricopharyngeus muscle, which is the circular part of the inferior pharyngeal constrictor, marks the junction where the laryngopharynx transitions into the esophagus.
Key Considerations
Epiglottis: The epiglottis serves as a critical protective mechanism to seal off the airway during swallowing, preventing food from entering the larynx and trachea.
Cricopharyngeus: Acts as a sphincter to regulate the flow of food from the laryngopharynx into the esophagus, ensuring a controlled and coordinated transition during swallowing.
Epiglottis
Anatomical Position
Inferior to the oropharynx and superior to the larynx.
Anterior to the hypopharynx and posterior to the hyoid bone.
Medial to the piriform sinus (or piriform recess), through which food or fluid travels into the laryngopharynxand then to the esophagus.
Structure and Composition
The epiglottis is composed of elastic cartilage, which provides the necessary flexibility for its function.
Functional Role in Swallowing
During swallowing, the larynx is elevated, which causes the epiglottis to passively close, effectively sealing the laryngeal inlet to prevent food or fluid from entering the airway.
After swallowing, as the larynx descends, the epiglottis returns to its normal, upright position.
Importance in Swallowing
The epiglottis acts as a protective valve during swallowing, ensuring that food or fluid is directed into the esophagus and not the trachea, preventing aspiration and potential respiratory complications
Epiglottis and Its Attachments
Epiglottis Attachments
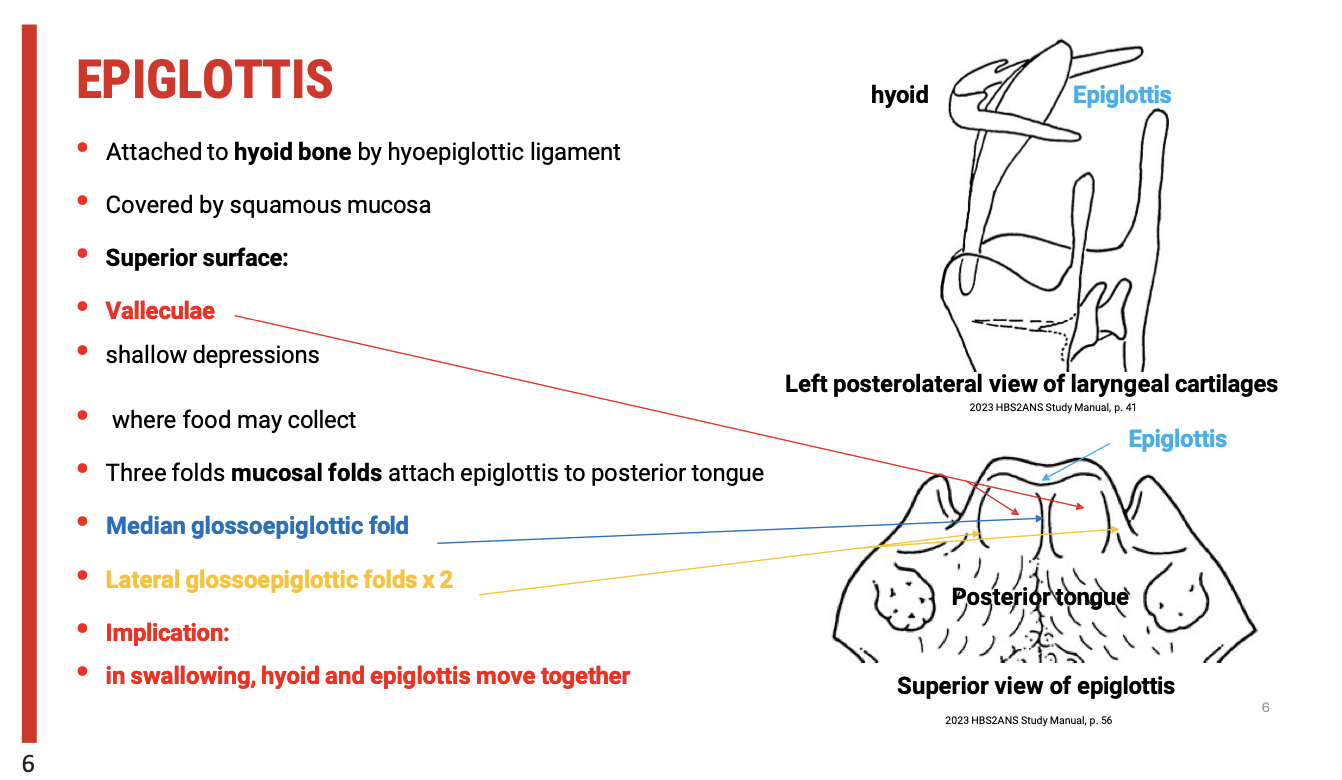
Hyoepiglottic Ligament
The epiglottis is attached to the hyoid bone via the hyoepiglottic ligament.
This ligament provides a connection between the epiglottis and the hyoid bone, which plays a crucial role in the movement of both structures during swallowing.
Mucosal Covering
The hyoepiglottic ligament is typically covered by squamous mucosa, which provides a smooth surface for movement and function during swallowing.
Glossopharyngeal Attachments
Mucosal Folds: Three mucosal folds attach the epiglottis to the posterior surface of the tongue:
Median glossoepiglottic fold (middle fold).
Two lateral glossoepiglottic folds (on either side).
These folds help anchor the epiglottis and contribute to its movement and positioning during swallowing.
Functional Implications for Swallowing
Volvulae (Shallow Depressions)
The superior surface of the epiglottis contains volvulae, which are shallow depressions where food may collect during swallowing.
Volvulae are important to examine, as food can accumulate in these areas, potentially increasing the risk of aspiration if not effectively cleared.
Hyoid and Epiglottis Movement
The hyoid bone and epiglottis move together during swallowing, which is critical for protecting the airwayby ensuring that the epiglottis covers the laryngeal inlet.
Dysfunction in the movement of these structures can lead to swallowing difficulties and aspiration risk.
Clinical Implications
When assessing patients for swallowing disorders, it is important to evaluate the function of these attachments to determine whether the epiglottis is effectively protecting the airway.
Areas where food can collect, such as the volvulae and between the glossoepiglottic folds, should be carefully examined to identify any issues with swallowing efficiency or the risk of aspiration.
Function of the Epiglottis in Swallowing
The epiglottis plays a crucial role in protecting the airway during swallowing by ensuring food and liquids are directed into the oesophagus rather than the larynx. Here's a breakdown of its function:
Key Functions
Protection of the Airway
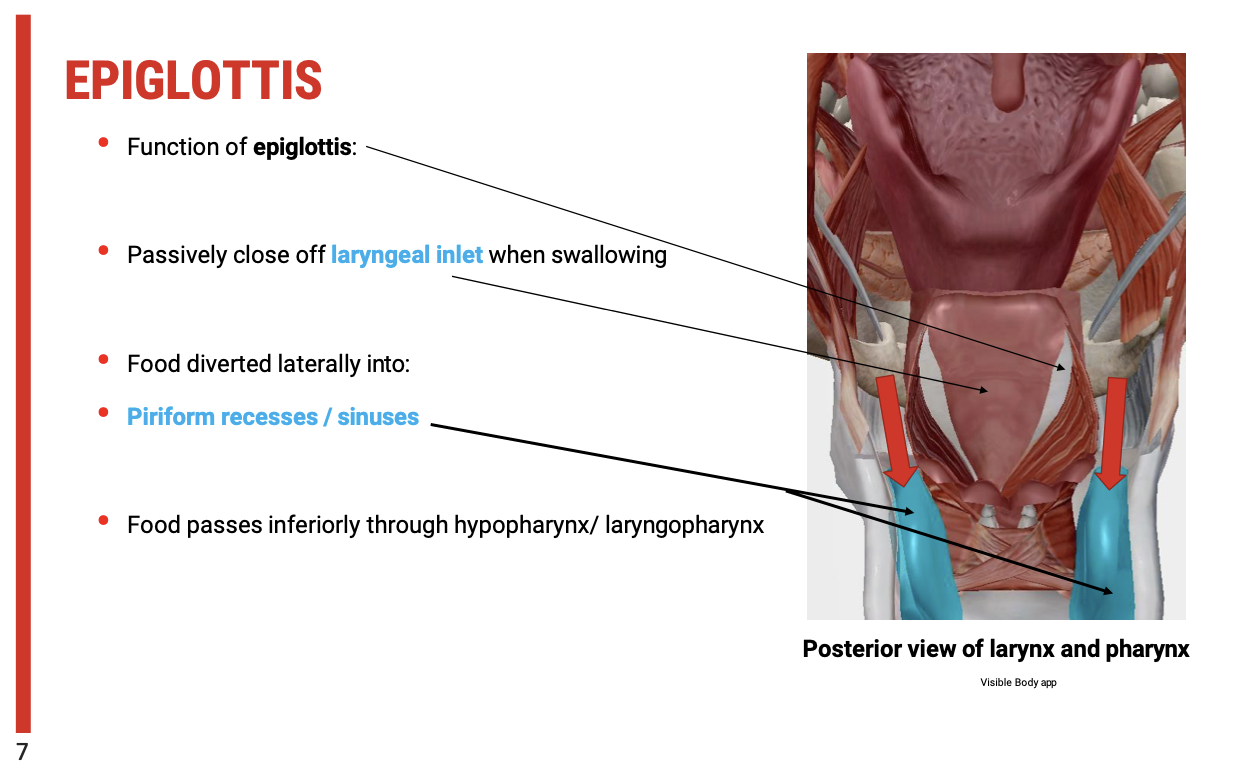
As the larynx rises during swallowing, the epiglottis passively closes off the laryngeal inlet. This prevents food or liquid from entering the airway and directs it away from the vocal cords and trachea.
This closure is critical for avoiding aspiration and ensuring that food or liquids are directed into the digestive tract rather than the respiratory tract.
Food Diversion
When the laryngeal inlet is closed by the epiglottis, food is diverted into the piriform recesses (or piriform sinuses), which are located on either side of the larynx.
The piriform recesses act as channels, guiding the food inferiorly through the hypopharynx and laryngopharynx toward the oesophagus.
Coordination of Swallowing
Proper coordination of the epiglottis, larynx, and pharyngeal muscles is essential for safe and effective swallowing.
A failure in this coordination can result in food entering the airway, increasing the risk of aspiration or choking.
Clinical Implications
Dysfunction in the movement of the epiglottis, such as failure to close the laryngeal inlet properly, can lead to swallowing difficulties and aspiration, especially in patients with neurological disorders, head and neck cancers, or conditions affecting the muscles involved in swallowing.
Assessment of the epiglottis and laryngeal closure is an important part of evaluating swallowing function, particularly for patients at risk of aspiration pneumonia or dysphagia.
Function and Muscles of the Pharynx in Swallowing
Epiglottis Function
The epiglottis plays a key role in protecting the airway during swallowing:
Closure of the Laryngeal Inlet: When the larynx rises, the epiglottis passively closes off the laryngeal inlet, preventing food or liquid from entering the airway.
Food Diversion: As the epiglottis closes, food is diverted into the piriform recesses (sinuses), then passes inferiorly through the hypopharynx and laryngopharynx toward the oesophagus.
Coordinated Swallowing: Effective swallowing relies on coordination between the epiglottis, larynx, and pharyngeal muscles to ensure safe passage of food into the oesophagus.
Muscles of the Pharynx
The pharyngeal muscles are primarily involved in swallowing and protecting the airway during swallowing. These muscles include:
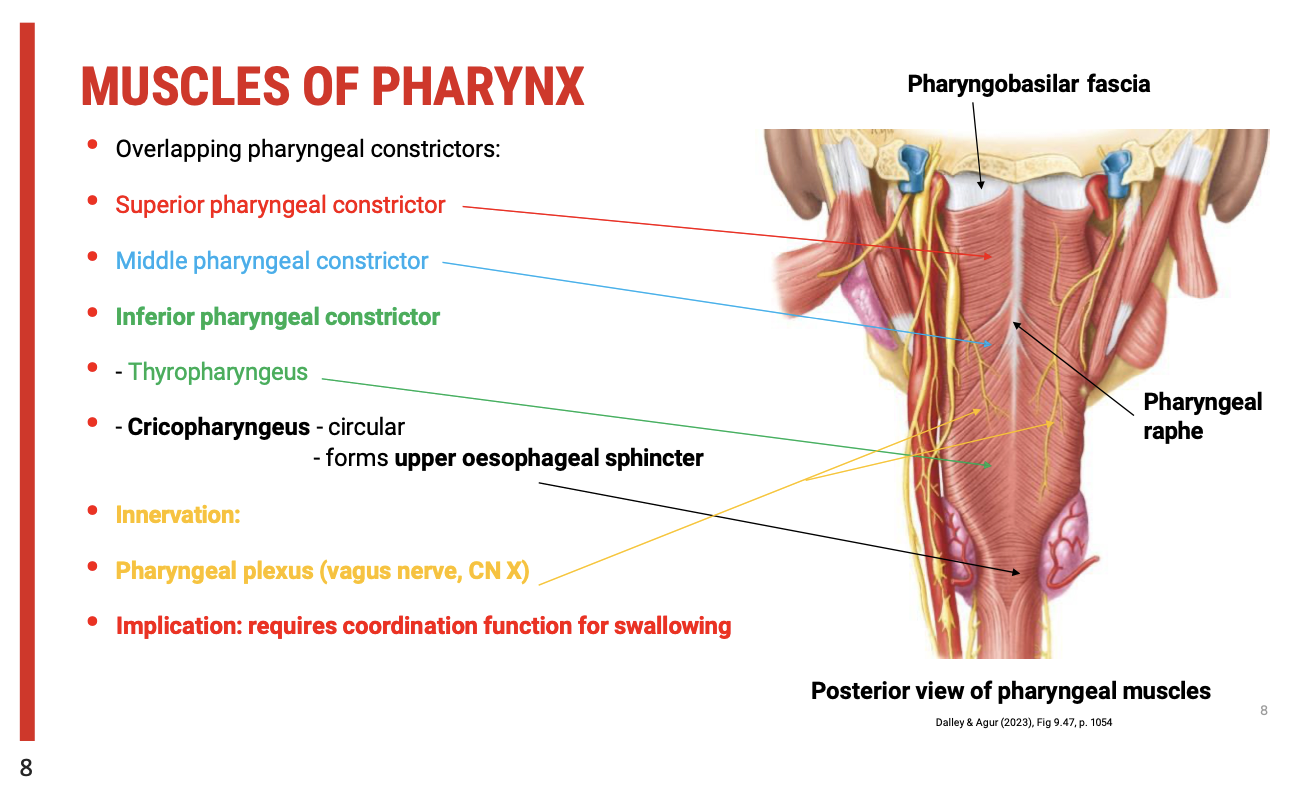
Pharyngeal Constrictors (Overlapping Muscles):
Superior Pharyngeal Constrictor: Surrounds the nasopharynx.
Middle Pharyngeal Constrictor: Surrounds the oropharynx.
Inferior Pharyngeal Constrictor: Surrounds the laryngopharynx. This muscle has two components:
Thyropharyngeus: An oblique muscle.
Cricopharyngeus: A circular muscle that forms the upper oesophageal sphincter.
Role of the Muscles in Swallowing:
These muscles work sequentially to propel food through the pharynx and into the oesophagus.
The upper oesophageal sphincter (Cricopharyngeus) must dilate when the bolus reaches it, allowing food or liquid to pass into the oesophagus.
Innervation
The pharyngeal muscles are innervated by the pharyngeal plexus, a branch of the vagus nerve.
The vagus nerve plays a vital role in coordinating the muscular contractions necessary for normal swallowing.
Clinical Implications
Effective coordination of these muscles, particularly those innervated by the vagus nerve, is crucial for safe swallowing.
Dysfunction in these muscles or their innervation (e.g., due to neurological conditions) can lead to dysphagia, or difficulty swallowing, which may increase the risk of aspiration and related complications.