Week 6/7 Trauma ABCS III
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Our bodies change over time
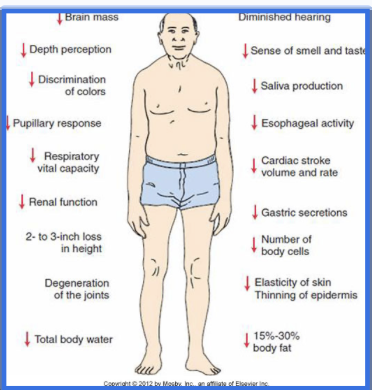
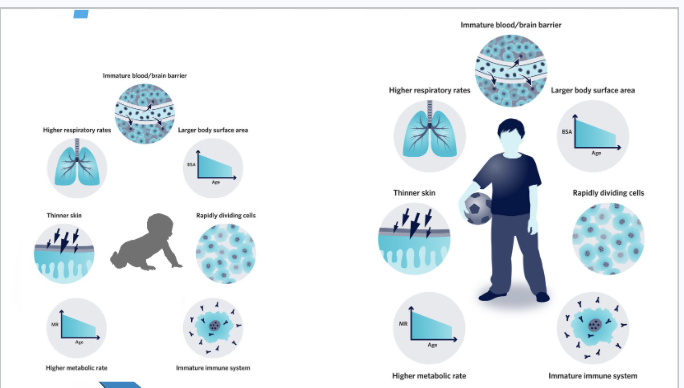
As infants develop, their vital sign ranges change, their anatomy changes, and their response to injury changes. Older patients will begin to show signs of changing and failing body systems and their musculoskeletal anatomy may change shape and become less flexible. Medications that older patients may be on can change their response to injury.
Body systems continue to develop and mature in the young.
Aging body systems show signs of dysfunction.
There are anatomical differences.
Photo
Photo
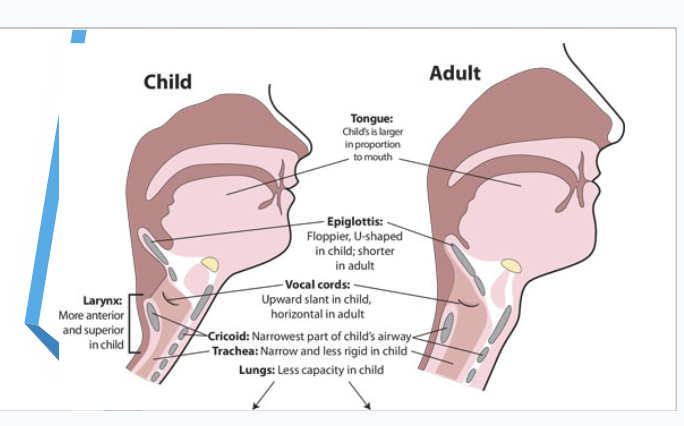
Respiratory issues in Children
Hypoventilation and hypoxia are more likely than hypovolemia and hypotension.
Injured children can rapidly deteriorate from labored breathing to tachypnea and on to exhaustion and apnea.
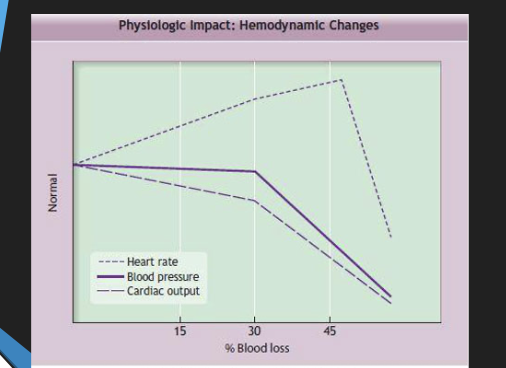
Shock
Most pediatric injuries do not cause immediate exsanguination.
Blood pressure is a poor indicator of blood loss and peripheral perfusion.
Children remain in compensated shock longer than adults, but decline very rapidly.
physiologic Impact
Burns
All burns are serious, regardless of size.
Burns are not just a skin injury.
Large burns involve multiple organ systems.
Smoke inhalation can be life-threatening.
It is often more dangerous than the burn itself.
Carbon monoxide
Cyanide
Children account for 20% of all burn victims
Consider the possibility of intentional injury (abuse).
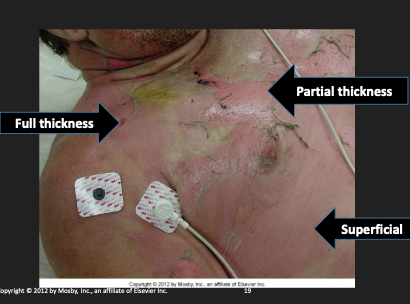
Burn Assessment
Depth of injury
Superficial (1st degree)
Partial thickness (2nd degree)
Superficial
Deep
Full thickness (3rd and 4th degree)
Burn depth may evolve over time.
Burn Management
Conduct primary survey–ABCDE. Airway breathing circulation disability, exposure
Airway occlusion may occur as swelling progresses.
Breathing may become compromised from chest wall eschar or toxic pulmonary injury.
Monitor respiratory rate, SaO2
Circulatory status may be compromised as fluid leaks into damaged tissue, which causes swelling and hypotension.
ALS/transport
Specific burn therapy
Stop any ongoing burning.
Cover with dry, sterile non adherent dressing (sheet).
Do not use any ointments or other topical antibiotic.
Multiple Patient Situations
A multiple patient scenario occurs each time there is more than one patient.
Are there sufficient resources available on-scene to manage all patients?
Triage is used primarily when the number of patients exceeds the immediate treatment and/or transport capacity.
If number of patient exceeds resources- MASS CASUALTY INCIDENT
Transport only one critical patient per ambulance.
Patients who require spinal motion restriction require stretcher for transport
When possible, distribute patients to all available hospitals.
Green - person can walk, regardless of broken arm.
black - deceased
tags
Trauma Resuscitation Issues
In certain situations, it may be allowable to withhold or terminate resuscitation efforts in:
Injuries not compatible with life
Pulseless and non breathing blunt trauma victims
Trauma patients with EMS- witnessed cardiopulmonary arrest and 15 minutes of unsuccessful resuscitation and CPR--recommendations may be revised--
Special consideration in trauma resuscitation must be given to patients who may have greater likelihood of survival:
hypothermia
immersion incidents
lightning strike
Follow protocols, system guideline, Online medical control consult
Multisystem Trauma
Multiple-trauma patient
More than one serious injury
Multisystem-trauma patient
One or more injuries serious enough to affect more than one body system
Teamwork, timing, and transport decision are key to proper management.
Determining Patient Severity
Most critical decisions
Patient priority/severity
Whether to limit scene time or not
Which hospital or transport method is best for your patient
Determining Severity:
Physiologic Criteria
Altered mental status (GCS < 14)
Head injury
Hypotension (systolic < 90 mm Hg)
Shock, internal bleeding
Abnormally slow respiratory rate
Head injury, later stages of shock
Determining Severity:
Anatomic Criteria
Penetrating injuries to head, neck, torso, and extremities proximal to elbow and knee
Chest wall instability or deformity - crepidis everywhere. Flailed chest
Two or more proximal long-bone fractures
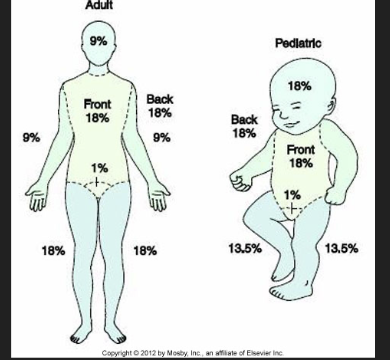
Determining burn area adult vs pediatric.Rule of 9
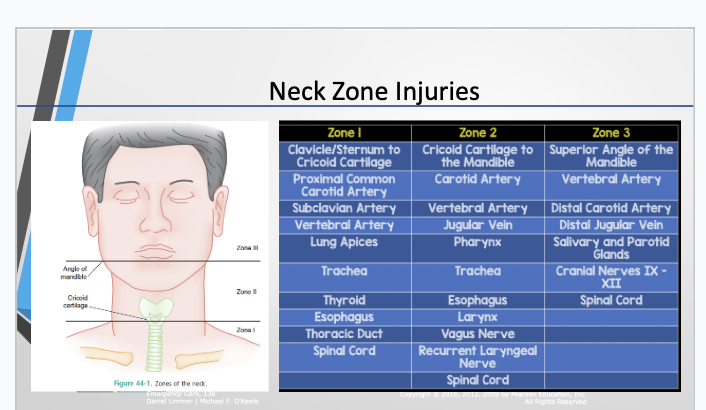
Neck Zone Injuries
Determining Severity:
Anatomic Criteria
Crushed, degloved, mangled, or pulseless extremity
Amputation proximal to wrist or ankle
Pelvic fractures - blood loss. Bind it.
Open or depressed skull fracture
Paralysis
Determining Severity:
Mechanism of Injury
In absence of anatomic or physiologic signs, MOI is considered if severe.
Falls
Intrusion
Ejection from automobile
Death in same passenger compartment
Vehicle telemetry data consistent with high risk of injury
Determining Severity: Special Patients and Considerations
Older adults do not efficiently compensate for shock.
Children may benefit by transport to a pediatric specialty facility.
Patients with certain conditions
Taking anticoagulants
Pregnant
Managing the Multisystem-Trauma Patient
A Typical Call
Practice with crew.
Determine roles.
En route to call, review roles each member of the crew will have.
Ensure scene safety.
Auto crash will have passing traffic.
Penetrating trauma - we want police. Stabs, gunshot wounds.
Assailant may still be on the scene.
Perform the primary assessment.
Ensure an open airway.
Perform urgent or emergency moves.
Transport.
Give a report to the trauma team at the emergency department during handover.
Analysis of the Call
In a scenario with critical injuries
Follow priorities determined by assessments.
Do not delay transport by performing treatments that would waste time.
Show good judgment.
Postpone taking vital signs until en route when appropriate.
Give the hospital staff time to prepare.
General Principles of Multisystem-Trauma Management
Follow priorities determined by primary assessment.
Attend to immediate threats to life.
Reassess what to treat on scene and what needs definitive care.
Call hospital so they can prepare.
General Principles of Multisystem-Trauma Management
Depending on your primary assessment, you may postpone taking vital signs until you are en route to the hospital.
As you reassess your patient in the vehicle, call the hospital as necessary to update the vital signs.
General Principles of Trauma Management
Limit scene treatment
Stabilize cervical spine.
Suction airway.
Insert oral or nasal airway.
Restore patent airway.
Ventilate with bag-valve mask.
Administer high-concentration oxygen.
Control bleeding.
Immobilize patient on cot
General Principles of Multisystem-Trauma Management
Scene safety is paramount.
Ensure an open airway.
Perform urgent or emergency moves as necessary.
Adapt to the situation.
Remember
Your primary assessment should determine whether your patient is seriously injured or potentially seriously injured.
Limit scene treatment to life-threatening conditions.
Your patient will tell you how severe their injuries are! (physiologic criteria, anatomic criteria, MOI)