Master Combined Written Review Deck
1/896
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
897 Terms
When to use an Ilfeld vs Rhino vs Pavlic orthosis?
Pavlic is the 1st line of defense - usually 0-3 months old and is the most commonly used
Ilfeld is second line treatment. Is great at maintaining abduction but not as good at holding as much hip flexion
Rhino orthosis is also second line treatment is improvement has not been found after 3-4 weeks of pavlik treatment - it is also an alternative to using spica cast
Congenital deformity
Presents as ankle PF, subtalar inversion, and forefoot adduction
Clubfoot
Serial casting
Achilles Tenotomy
Ponsetti or Denis Brown bar
AFO
Treatments for clubfoot
Maintain external rotation, abduction, and DF
Involved feet are externally rotated 60-70 degrees
Non-involved feet are externally rotated 30-40 degrees
Some use Markell shoes and Denis Browne bar
Ponseti AFO and Abduction Bar
treatment for clubfoot

When is an AFO used for kids with clubfoot? How does it work?
Used in older kids with persistent deformity
Extended medial trim lines to reduce forefoot adduction
Internal straps for varus correction

Why are their holes in the back of AFOs for clubfoot?
Holes are in the back of the heel to see if fully seated and posterior material to discourage plantarflexion

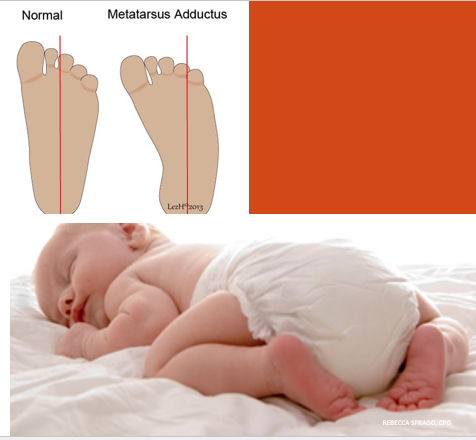
At birth there is a normal slight adduction of the forefoot
Usually disappears within 3-6 months of age - persistent adduction is treated if beyond that time
Metatarsus adductus

How do you differentiate clubfoot and metatarsus adductus?
Rule out clubfoot if able to plantarflex and dorsiflex ankle. If they can’t DF, it is probably clubfoot
Treatment options for metatarsus adductus
Wheaton AFO
Reverse last shoes - or shoes on the opposite feet
Bebax shoes
SMOs for older kids

No neurological reason for toe walking
Sometimes parents can link a sensory issue (only do it barefoot, only on carpet, etc)
Idiopathic toe walking
If the child has full ROM - what are some possible treatment options?
Carbon fiber footplate
PF restricting SMOs/AFOs

If the child is losing DF ROM, what treatment options are there?
Night-time stretching AFOs
Serial casting
Patella neutral but feet point inward
Normal at birth
Usually self-corrects by age 3
Tibial torsion
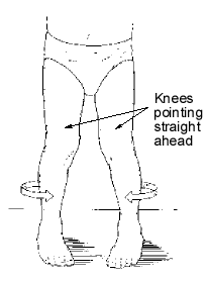
What is the difference between tibial torsion and metatarsus adductus?
Metatarsus adductus is just the foot while tibial torsion is the foot AND the shank/tibia
What is tibial torsion associated with?
Sitting on the feet
When is tibial torsion treated?
If it persists through childhood
Treatment option for tibial torsion
Wheaton KAFO

Wheaton style AFO
Solid trough style KAFO with bent knee
Wheaton style has detachable knee and AFO sections that can progressively be rotated out

What does any treatment for tibial torsion have to accomplish?
Need to go above the knee to de-rotate the tibia
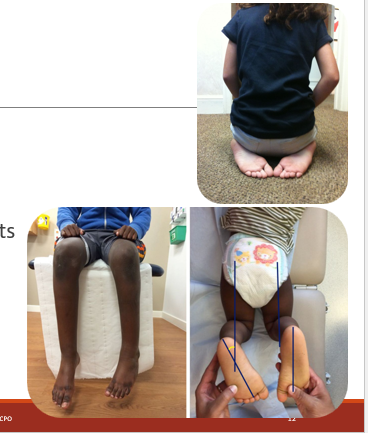
Normal at birth
Patella and feet both point in
Associated with W-sitting
Femoral torsion
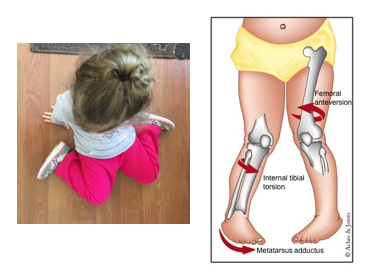
How will a patient present with femoral torsion?
Exam will show increased hip internal rotation ROM and decreased external rotation ROM
Treatment and when for femoral torsion
Possible treatment is with osteotomy if persistent past age 8
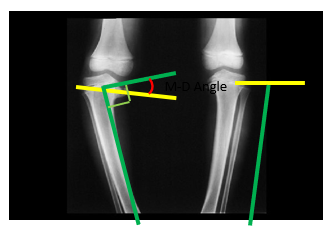
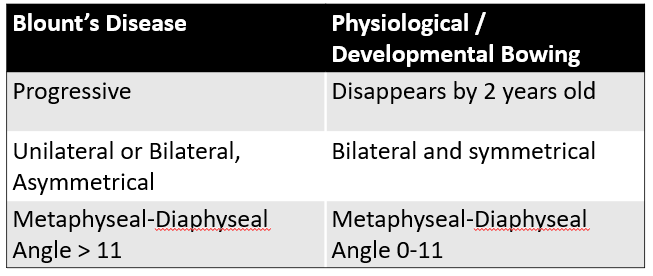
Blount’s disease is AKA
Tibia Vara
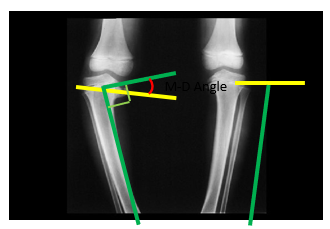
Reduced growth on the medial side of the epiphyseal plate resulting in increasing varus of the tibia
Blount’s disease
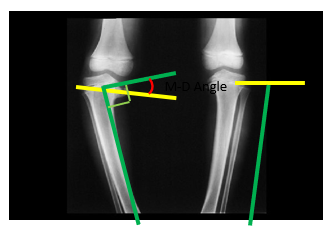
What metaphyseal-diaphyseal angle does it need to be to be blount’s?
Angle greater than 11
Goal of treatment for blount’s disease
Prevent progression of deformity
Treatment options for Blount’s disease
KAFO
Surgical tibial osteotomy
KAFO characteristics for treating Blount’s
Single upright KAFO (can do double uprights in heavier kids)
Adjustable uprights for growth with valgus pressure at knee center with pressure medially
Trimlines below perineum and proximal to the ankle
Knee locked in extension
Strap/band to pull tibia medially

Wear schedule and how long do they use the KAFO for blount’s?
Worn 22-23 hours a day
Usually for 1.5-2 years
Compare and contrast Blount’s disease to normal physiological/developmental bowing
_________ is the most commonly fractured bone in children
Femur
Infantile femur fracture
60% of femur fractures in children under age 1 are due to….
Non-accidental trauma
Suspect abuse especially if non-ambulatory, however one study showed fractures resulting from use of exersaucers

Treatment for infantile femur fracture
Age < 6 months - Pavlik harness
Which direction(s) does the hip have more/greater ROM?
Flexion
Abduction
External Rotation
The anatomical hip joint is usually estimated to be ______ and ______ to the greater trochanter
anterior and proximal
T/F: Excessive anteversion of the femur will result in in-toeing when the femoral head is centered in the acetabulum.
TRUE
Which of the following could be a clinical presentation of hip flexion contracture?
Decreased lumbar lordosis
Crouch stance
Anterior pelvic tilt
Forward trunk lean
Posterior pelvic tilt
Crouch stance
Anterior pelvic tilt
Forward trunk lean
T/F: If the right gluteus medius is weak, it will cause the right pelvis to drop during swing phase (when the left leg is the stance leg).
FALSE
The angle of the pubic arch is usually larger in a _______ pelvis, compared to a _____ pelvis
female; male
The Ryder's Test / Craig Test is used to assess a patient's _________________.
Femoral torsion angle (anteversion/retroversion)
Knee extension
L3
Ankle Dorsiflexion
L4
Ankle plantarflexion
S1
A patient with femoral retroversion will likely present ________.
A. knock kneed
B. toed out
C. toed in
D. with greater internal rotation range
B. toed out

This image shows the proper position for testing what level of hip extension MMT?
4/5
You note that your patient externally rotates their thigh while attempting to demonstrate at least a 3/5 MMT for hip flexion. This is most likely the result of _______.
A. excessive tightness of the hip abductors
B. slack iliofemoral ligament
C. substituting hip adductors to assist with hip flexion
D. partial paralysis at the S1 level
C. substituting hip adductors to assist with hip flexion
Hip flexion
L2
Ankle dorsiflexion
L4
Toe extension
L5
Which of the following orthoses would not be used to treat DDH?
A. SWASH orthosis
B. Pavlik harness
C. Scottish Rite Orthosis
D. Ilfeld orthosis
A. SWASH orthosis
Which of the following would not be considered a benefit of using a standing frame?
A. Improves bone integrity
B. Stretches muscles to prevent contractures
C. Improves bowel and bladder function
D. Easier to move between activities
D. Easier to move between activities
T/F: It is always possible to have hands-free ambulation with a standard HKAFO.
FALSE
Which of the following would be most appropriate for a 6 year old patient with scissor gait and inability to sit unassisted?
A. Rhino abduction orthosis
B. Ilfeld orthosis
C. Newport unilateral orthosis
D. SWASH orthosis
D. SWASH orthosis
Which of the following knee joints would be most appropriate to use on an HKAFO for a patient with knee flexion contractures, whose goal is standing stability?
A. Dial adjustable with drop lock
B. Posterior offset with drop lock
C. Dial adjustable without drop lock
D. Single axis with drop lock
A. Dial adjustable with drop lock
Which of the following would be appropriate for a patient with spinal cord injury with L3 as the last intact level?
As a reminder - a patient must exhibit at least a 3/5 for the myotome to be considered intact at that level.
A. Articulated AFO with PF stop at 90 degrees
B. Unilateral Newport
C. Twister cables
D. Floor reaction AFO
D. Floor reaction AFO
Which of the following would be appropriate to treat Legg-Calve-Perthes?
A. Swivel walker
B. Ilfeld orthosis
C. Scottish Rite Orthosis
D. Derotation straps
C. Scottish Rite Orthosis
You get a call to fit a hip orthosis following total hip arthroplasty, the resident on call asked you how you usually set up the hip joint? What would be your suggestion?
Flexion 0-90 degrees, abduction 10 degrees
What position should the hips be in to treat developmental dysplasia of the hip in a 2 month old infant?
Flexion and abduction
Which orthosis controls all three degrees of freedom of the hip joint?
A. Twister cables
B. Newport Jr. Orthosis
C. Pavlik harness
D. Scottish Rite Abduction orthosis
C. Pavlik harness
In order to score a 5/5 when performing MMT for the plantar flexor group, the patient should be able to complete ____ heel rises at a consistent rate of one rise every 2 seconds using correct form in all repetitions.
25
When are patients first screened for DDH?
A. Week 2-4
B. Only if there is a family history of skeletal dysplasia
C. 3 month check up
D. Birth - 7 days
D. Birth - 7 days
When an infant is wearing a pavlik harness, the onesie should be placed
under the harness to protect the babies skin from the harness and to keep the harness clean.
What is the first line of treatment for DDH?
Pavlik harness
One way to differentiate between Club foot and Metatarsus adductus is
A. The amount of forefoot adduction
B. the amount of DF range
C. The presence of forefoot valgus
D. whether the position is present at birth
B. the amount of DF range
Tibial Torsion can be effectiviely treated with
A. Bebax shoe
B. Wheaton AFO
C. Twister cables
D. Wheaton KAFO
D. Wheaton KAFO
T/F: A burr is required when riveting a metal upright to an afo.
FALSE
The dacron straps on your patients KAFO keep breaking the speedy rivets. How should you address this issue?
A. switch to copper rivets with a burr
B. switch to nylon speedy rivets
C. switch to speedy rivets with a shorter stem
D. switch to copper rivets without a burr
A. switch to copper rivets with a burr
The corrective force on a blounts orthosis should ideally be
A. posteriorly directed, applied to the anterior of the knee
B. laterally directed, applied to the medial side of the knee
C. medially directed, applied to the lateral side of the knee
D. anteriorly directed, applied to the posterior of the knee
C. medially directed, applied to the lateral side of the knee
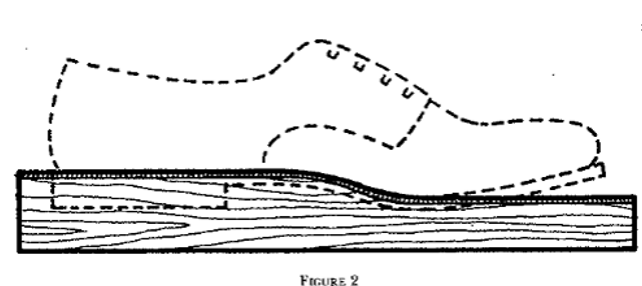
What is a “Last Board” and why do we use it?
Mimics the shoe to get the correct SVA in the coronal and sagittal planes
What is the Carlson modification and when is it used?
Sustentaculum tali groove correction that helps with pronation control and corrects hindfoot valgus
What orthotic design was the Carlson modification first introduced?
In the UCBL
What is the 3-point pressure system to correct flexible forefoot aDduction deformity

A forefoot adduction presentation would be most likely present in which pathology?
A.Pronation
B.Leg Calf Perthes
C.Charcot Arthropathy
D. Club foot
Club foot
What is a “Sabolich Trimline?”
Controls pronation and supination by controlling tibial internal + external rotation - extending onto the shank and increasing surface area for the corrective force
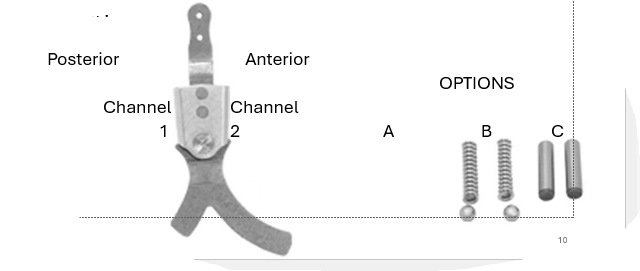
Which combination would simulate an eccentric contraction of the Tibialis Anterior?
Anterior channel = nothing
Posterior channel = spring
Want a combo that RESISTS PF - NOT stopping it

What is this strap called and what is used to correct it?
Corrects the hindfoot valgus deformity
Called a valgus t-strap
Your patient has a severe tibial nerve injury. What phase of gait would you likely notice a deviation? What feature would you add to your orthotic design to compensate for this injury?
Tibial nerve effects the plantar flexes
Late stance/push off - patient loses 3rd rocker
DF stop (anterior channel pin, foam piece anteriorly, check strap posteriorly - all valid options), pushing off plastic, forcing into PF and preventing tibial progression
Describe the toe plate trimline that would provide the greatest external knee extension moment. What part of gait will the patient notice the moment the most?
Full length foot plate
Notice the moment more during 3rd rocker
Trimlines for a Semi-rigid AFO
Through the malleoli

What features would you add to an orthosis to provide the greatest amount of Pronation control?
Medial Sabolich trimline
Valgus control - 3 point pressure system
Intrinsic medial heel wedge
ST modification
Increase the medial longitudinal arch
Forefoot aBduction control (distal to the 5th met head and proximal to the 1st met head)
Cast in Windlass position
When would a Lateral buttress / flange be added to an orthosis or shoe?
To provide additional lateral support, probably to control a varus or varum deformity
Supination control

What is the name of the toe plate trimline C? When is it used?
¾ length
Often the length of the rigid support in an FO, can be an AFO (leaves more room in the toe box of the shoe but less forefoot control and no effect on 3rd rocker)
Basically not controlling forefoot and decreasing knee hyperextension
Why might you add a heel lift to an FO or AFO?
Accommodate PF contracture, bringing the floor to the foot, meeting SVA
Define SVA - how is it measured? What is the desired SVA position for an AFO shoe combination?
Shank to vertical angle
Measured along the tibial crest
11 degrees
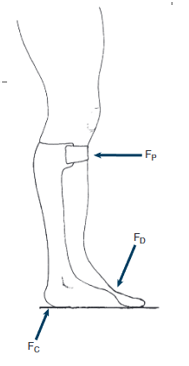
What moment is this 3-point pressure system creating at the ankle? What influence will this have on the knee?
PF ankle moment
Increases knee stability
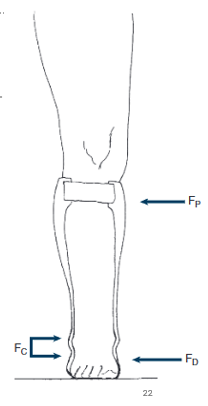
What moment is this 3-point pressure system creating at the ankle?
Valgus moment to correct varus position

What are indications for this knee joint?
Polycentric knee joint
Self-suspending
Reduce bunching in popliteal area
Reduce vertical displacement during knee flexion
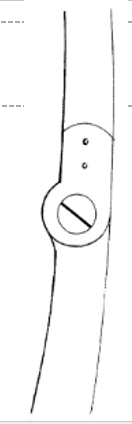
What are indications for this knee joint?
Single-axis knee joint
Mild-moderate genu varum/valgum
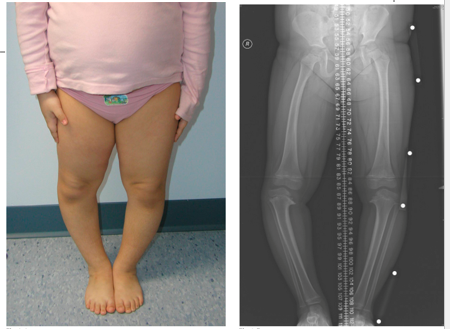
What is the pathology present in the patient’s right leg?
How would you design an orthosis to treat this condition?
Blount’s
Create a valgus pressure system to lessen the load on the medial growth plates and allow straightening of the tibia
What is an indication for a “conventional” orthosis?
What is a contraindication?
When changes in limb size are anticipated, such as seen with edema (peripheral or deep, lymphedema, PVD), cardiovascular disease, kidney disease, long term
Conventional orthosis wearers who are unwilling to change to a new system - if it isn’t broken, don’t fix it! Also if they have upper extremity limitations
Contraindications include spasticity and excessive deformity
Hip flexion
L2
Knee extension
L3
Ankle dorsiflexion
L4
Toe extension
L5
Ankle PF/eversion/hip extension
S1
Knee flexion
S2
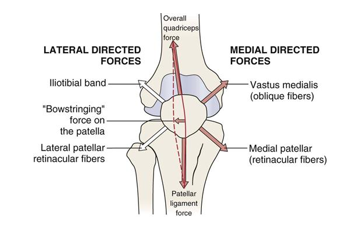
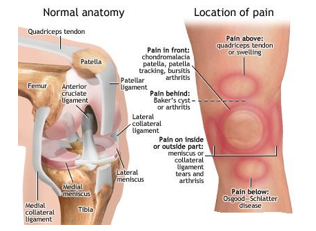
Name the different patellofemoral pathologies
Patellar subluxation/dislocation
Chondromalacia patella
Patellar tendonitis - AKA Osgood-Schlatter Disease
Fracture
_______ ______ from muscle attachments and connective tissues maintain the appropriate alignment
Balanced forces
What can unbalanced forces cause?
Lateral tracking disorder
Medial tracking disorder
What does the Q-angle affect?
Patellar tracking
The higher the Q-angle → lateral subluxation