BioSci D170: Applied Human Anatomy Midterm 2
1/452
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
453 Terms
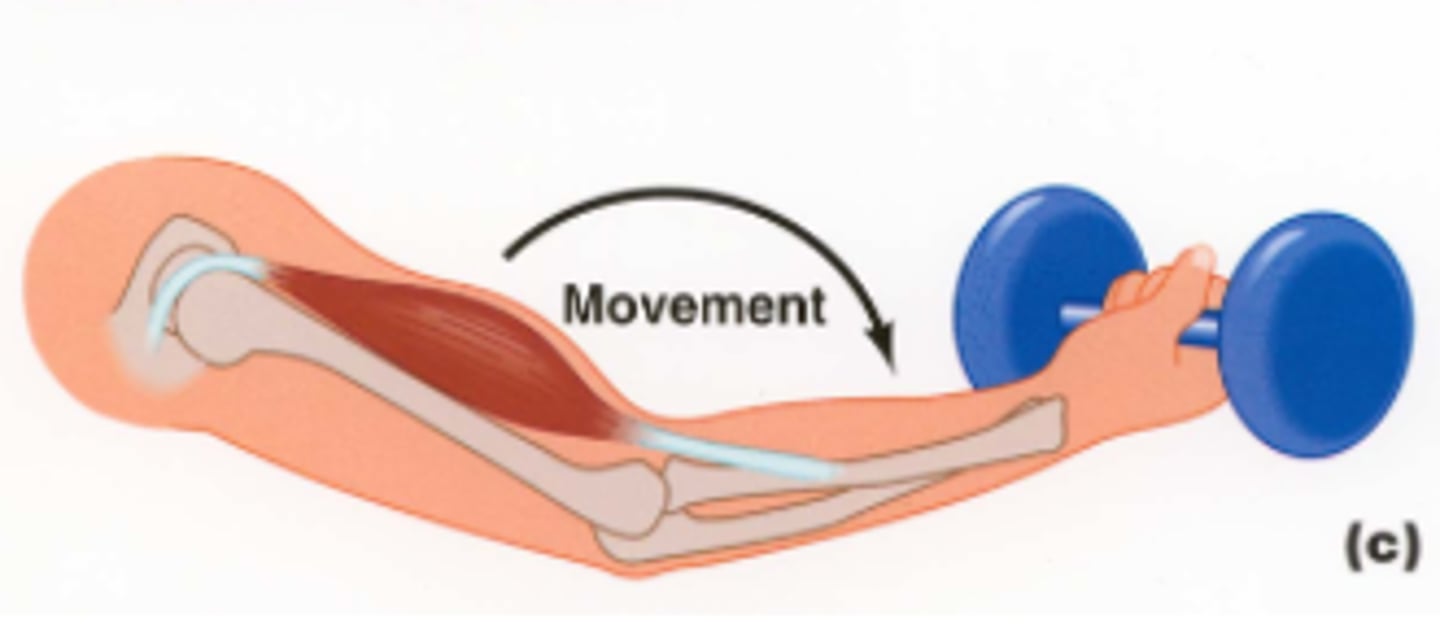
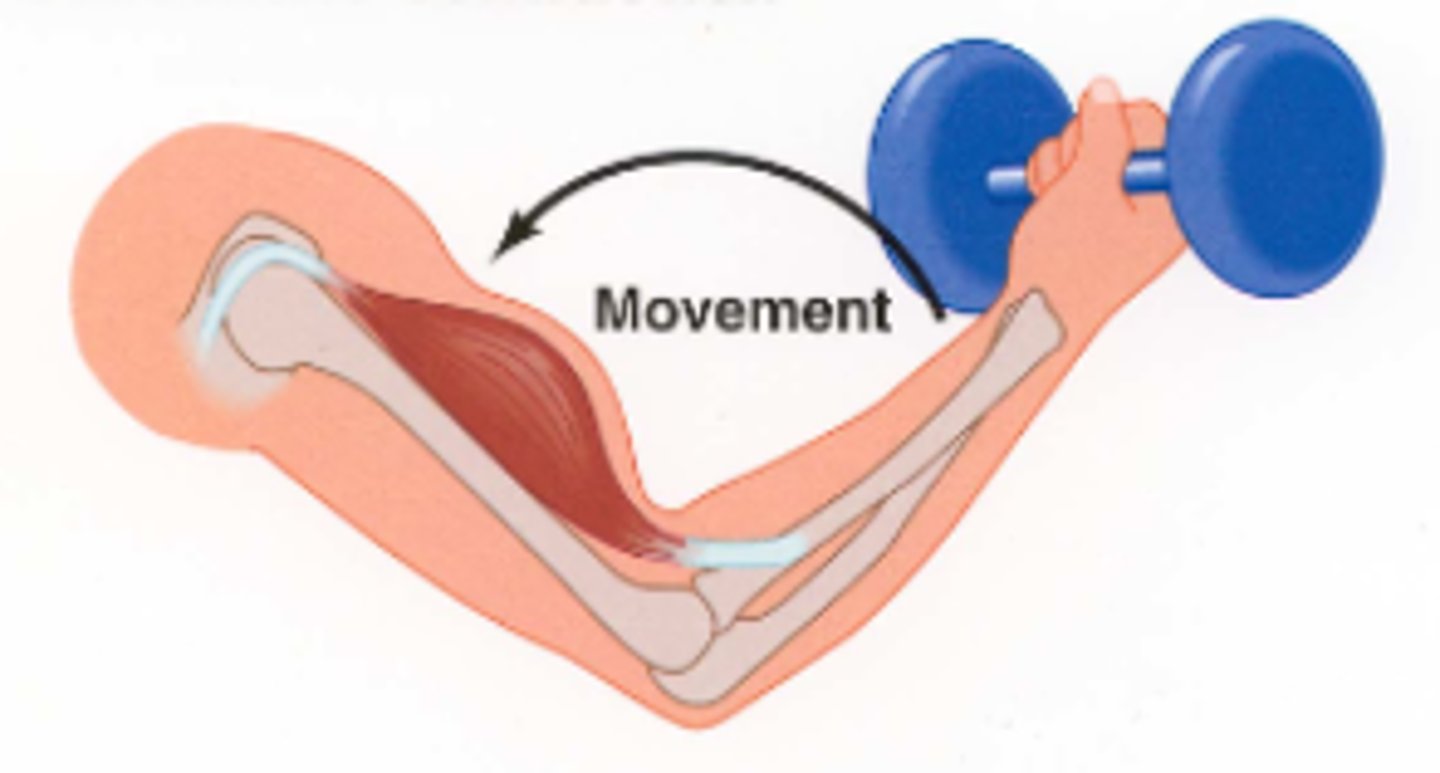
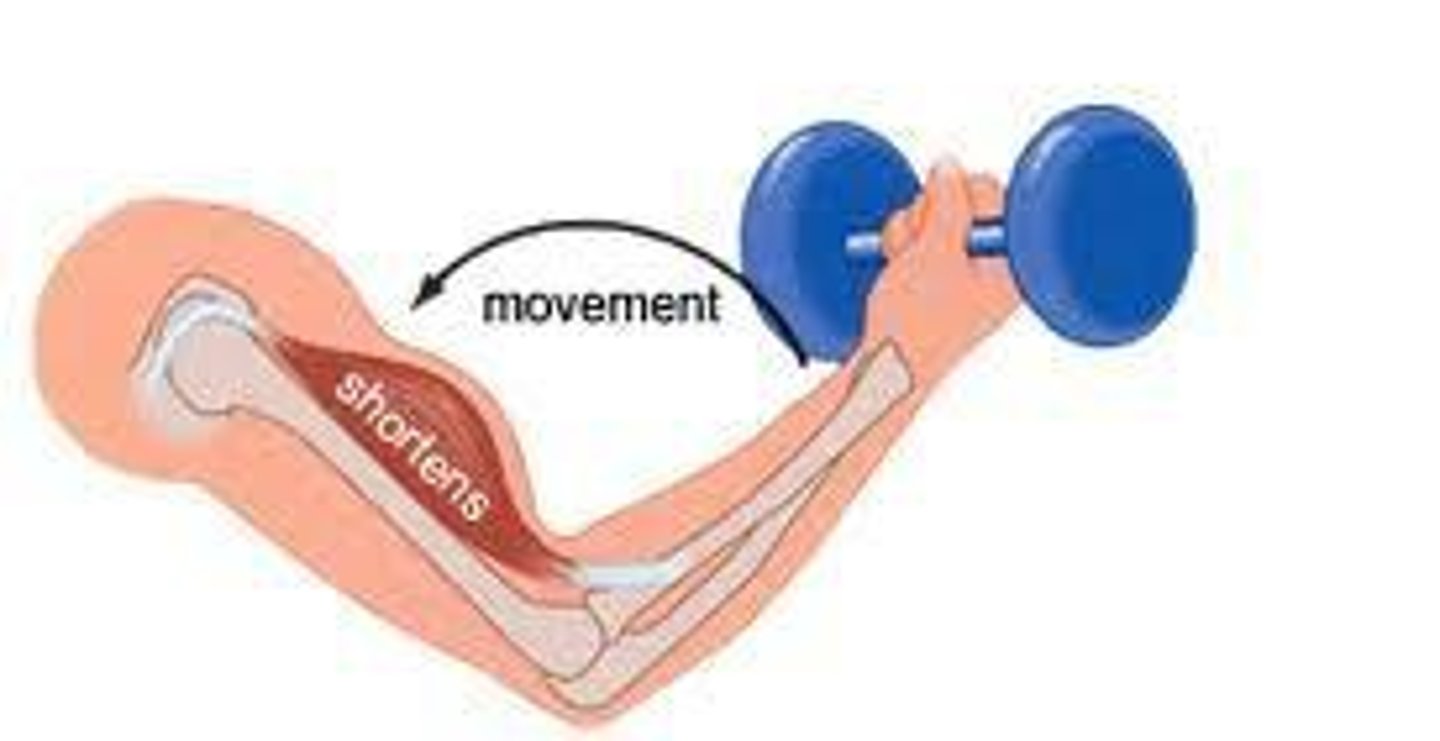
Flexion
A movement that decreases the angle between two bones (or body parts) within a connecting joint.
Example: flexion of the arm (bending the arm) as the angle between the humerus and the radius (or ulna) gets smaller.
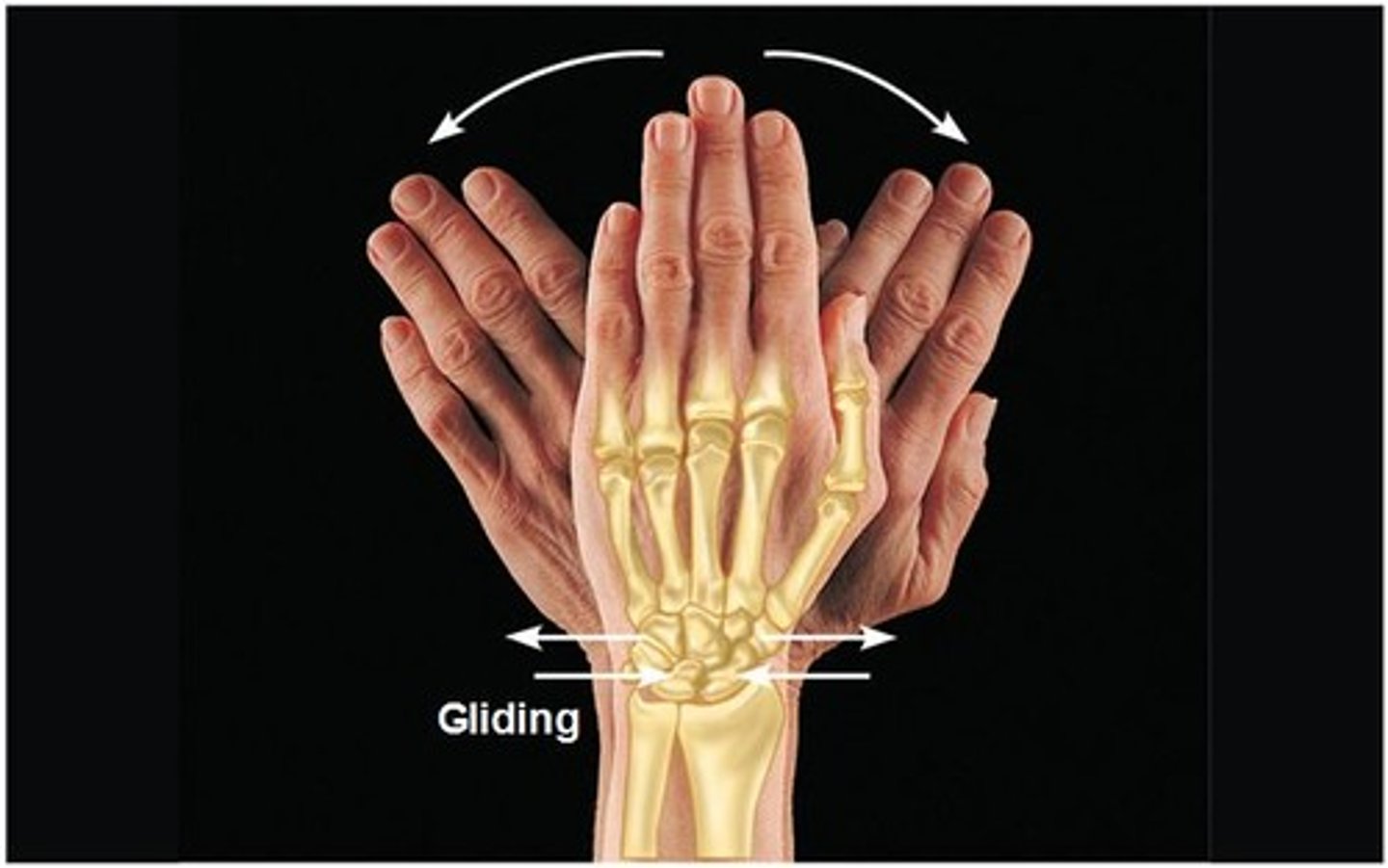
Gliding
The nearly flat surfaces of two bones slip across each other.
Example: Occurs at the joints between the carpals and tarsals and between the flat articular processes of the vertebrae.
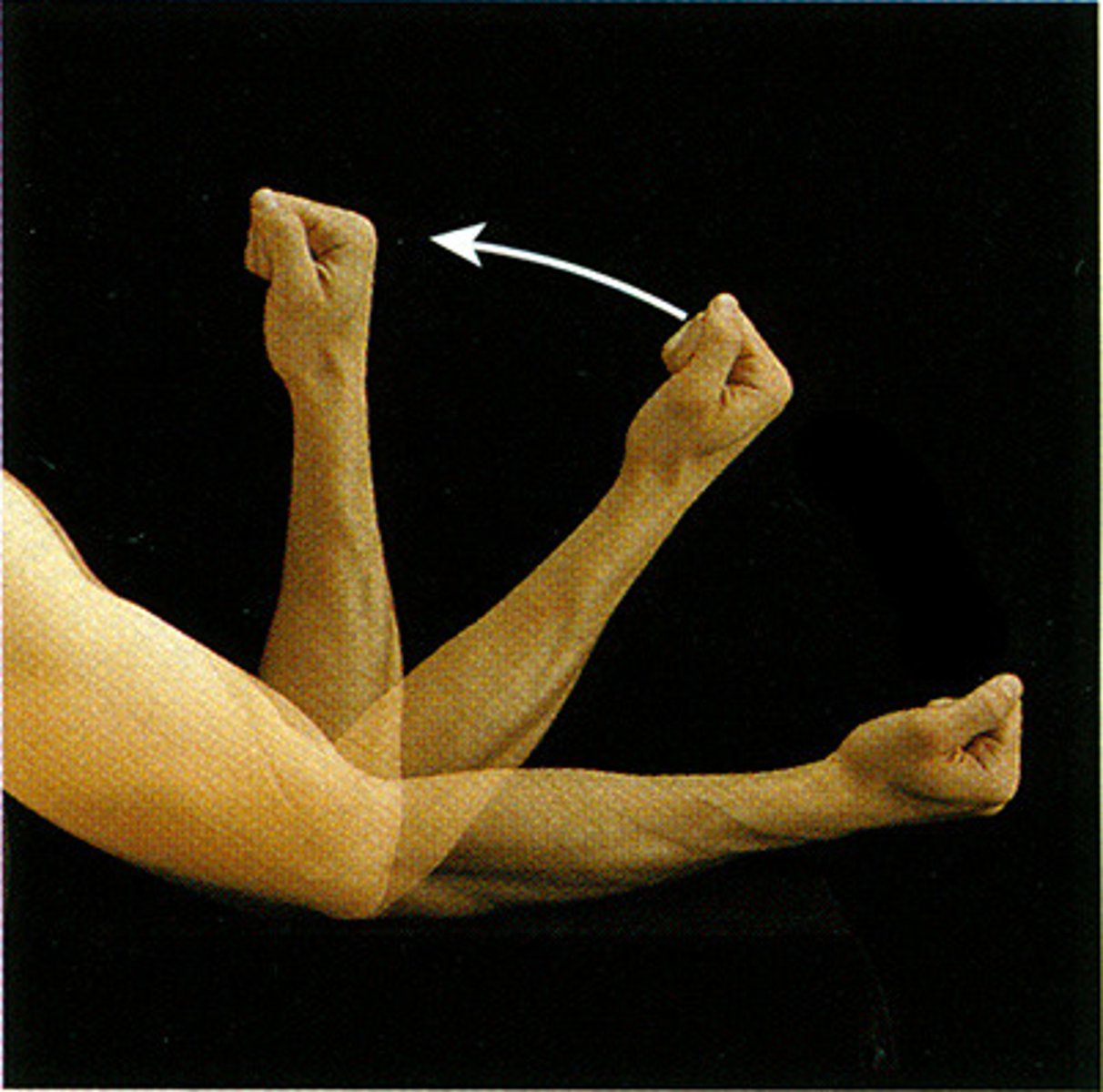
Extension
Increasing the angle between bones, usually in the sagittal plane
Example: Straightening the fingers after making a fist
Hyperextension
Bending a joint back beyond its normal range of motion.
Example: Individuals who have loose ligaments that allow a greater range of motion can be capable of hyperextending the joints.

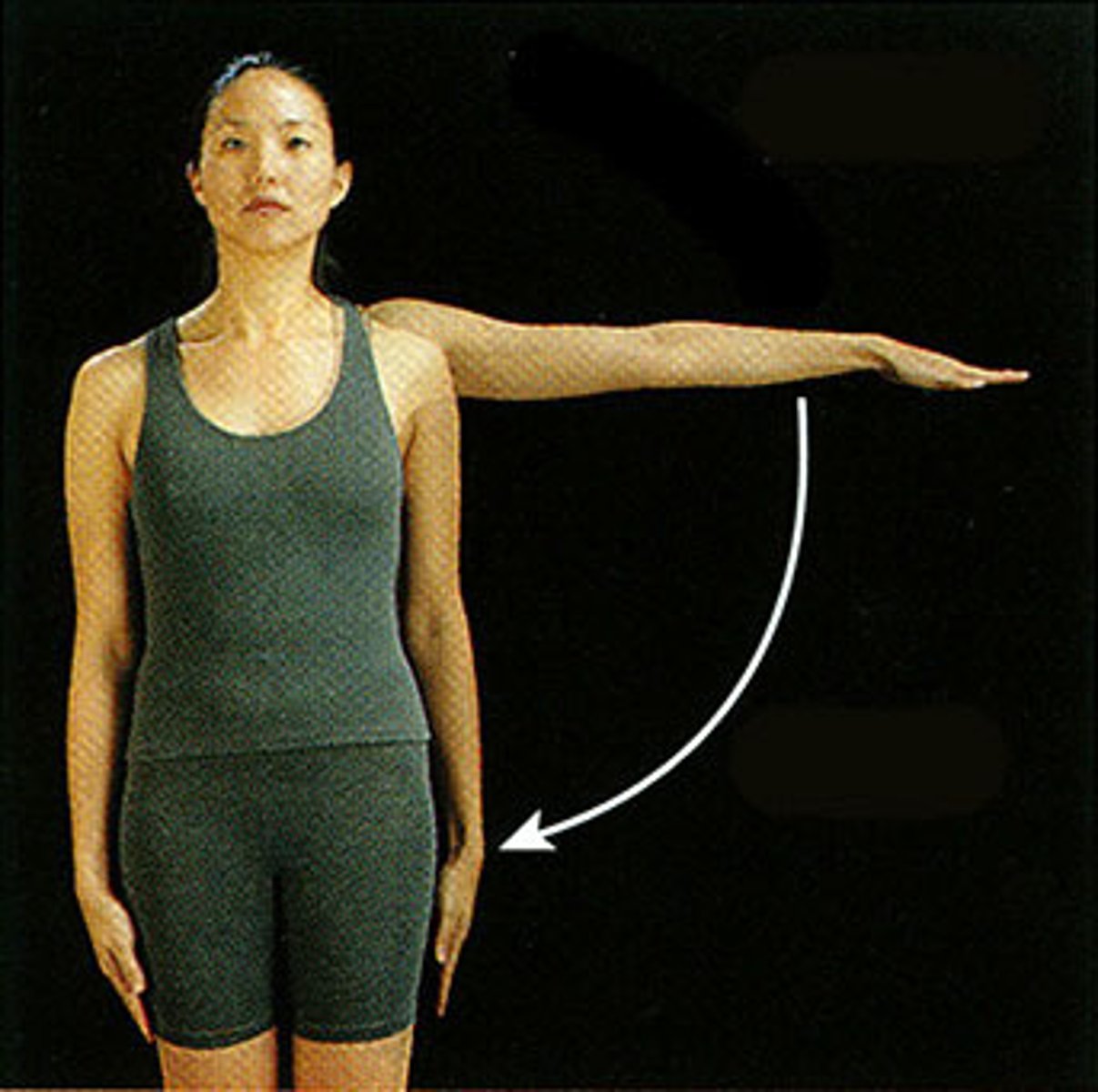
Abduction
Moving a limb away from the body midline in the frontal plane.
Example: Raising the arm or thigh laterally

Adduction
Moving a limb toward the body midline in the frontal plane.
Example: Moving digits toward the midline of the hand or foot
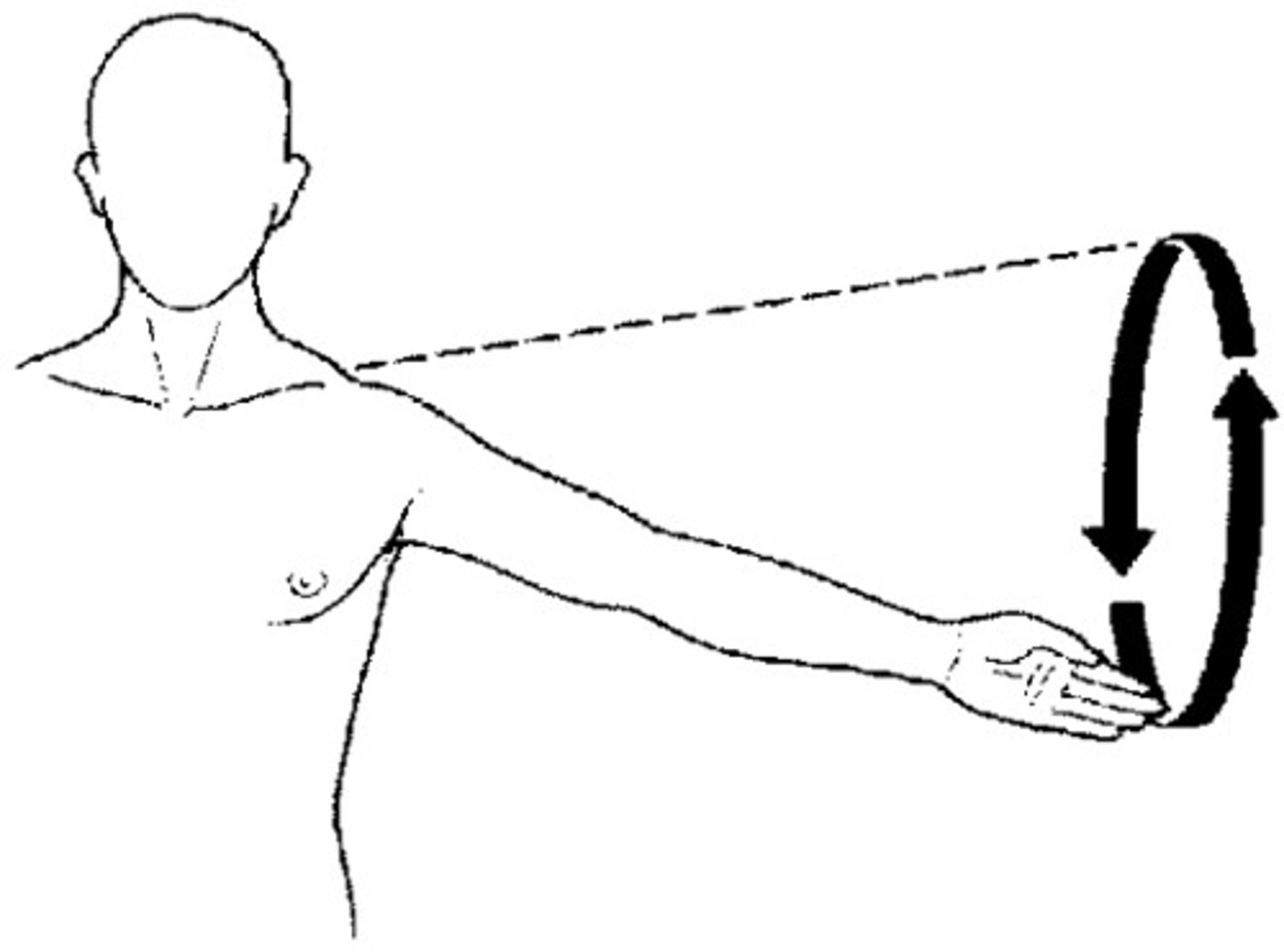
Circumduction
Moving a limb or finger so that it describes a cone in space. This is a complex movement that combines flexion, abduction, extension, and adduction in succession.
Example: The movement of the arm at the shoulder joint in a circular motion
Rotation
Turning a bone around the longitudinal axis. This motion occurs along the transverse plane. The only movement allowed between the first two cervical vertebrae.
Example: The entire vertebral column also rotates, twisting the whole trunk to the right or left.

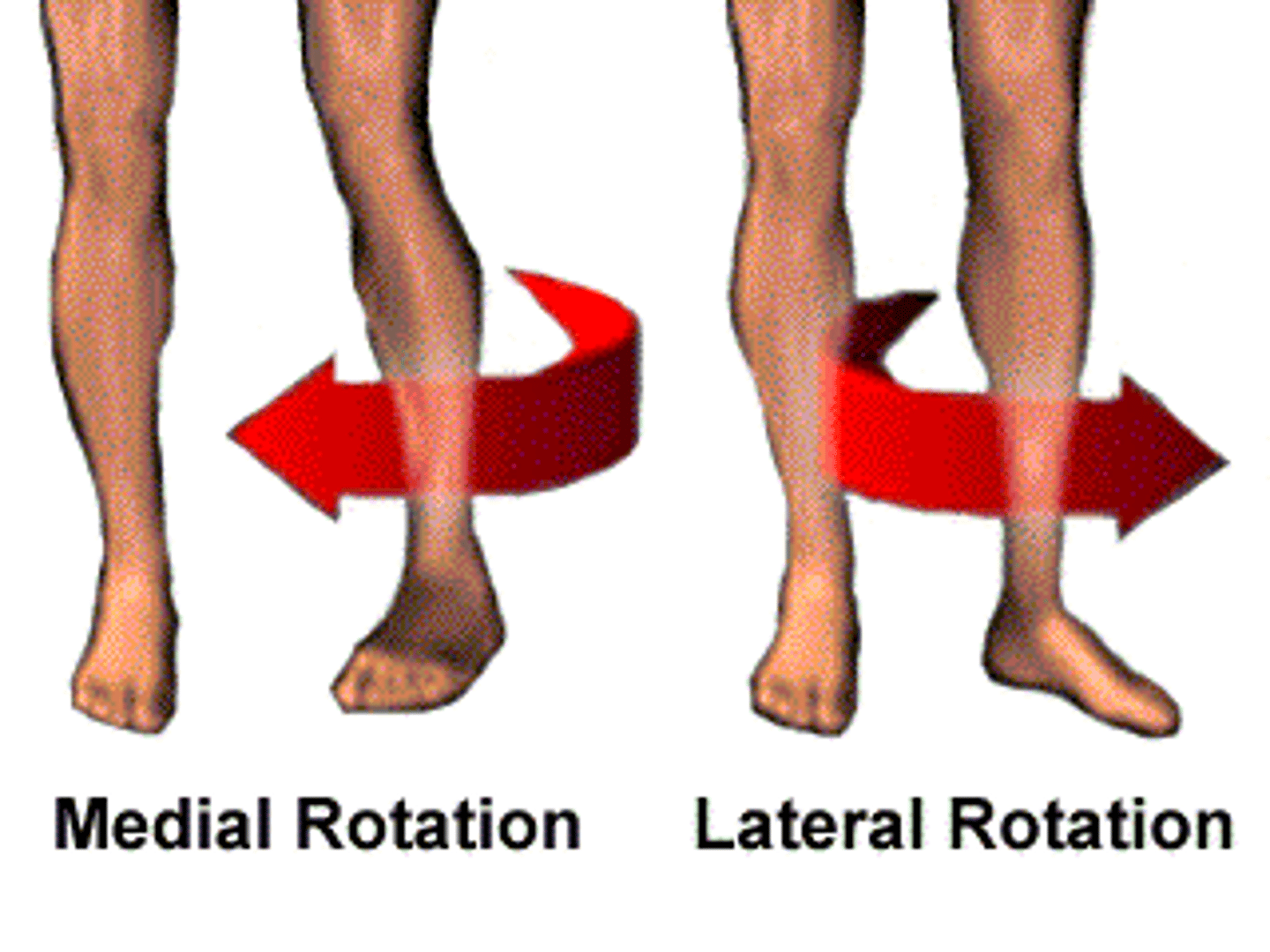
Medial Rotation
also known as internal rotation is a rotational movement of a bone or a body part towards the midline of the body. Medial rotation Rotating toward the median plane
Example: Medial rotation of the arm at the shoulder joint found in the swinging motion after hitting the ball in tennis or golf.
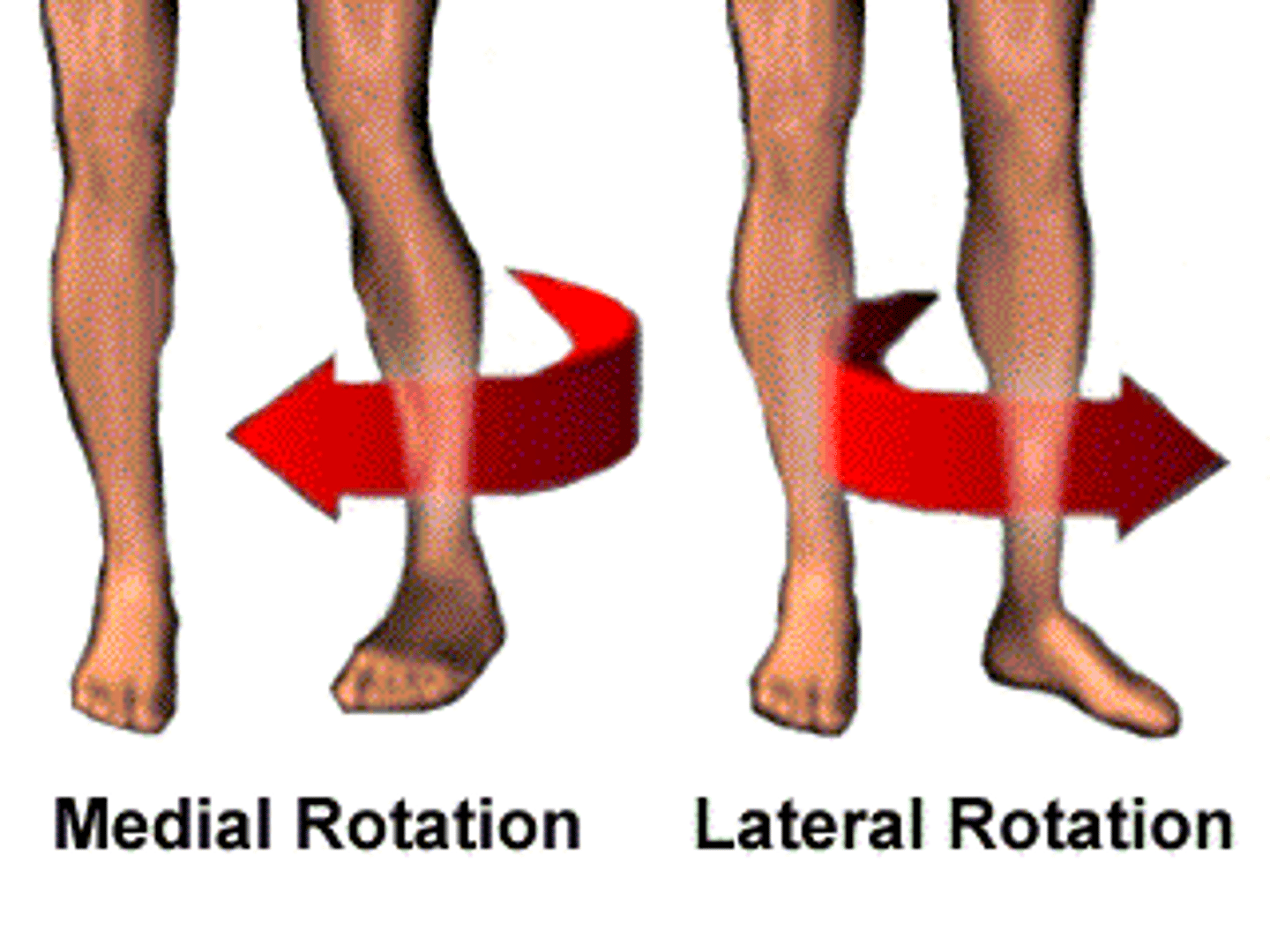
Lateral Rotation
Rotating away from the median plane
Example: When the shoulder joint rotates laterally as you move your arm away from your body
Elevation
Lifting a body part superiorly
Example: Elevation of a mandible during chewing
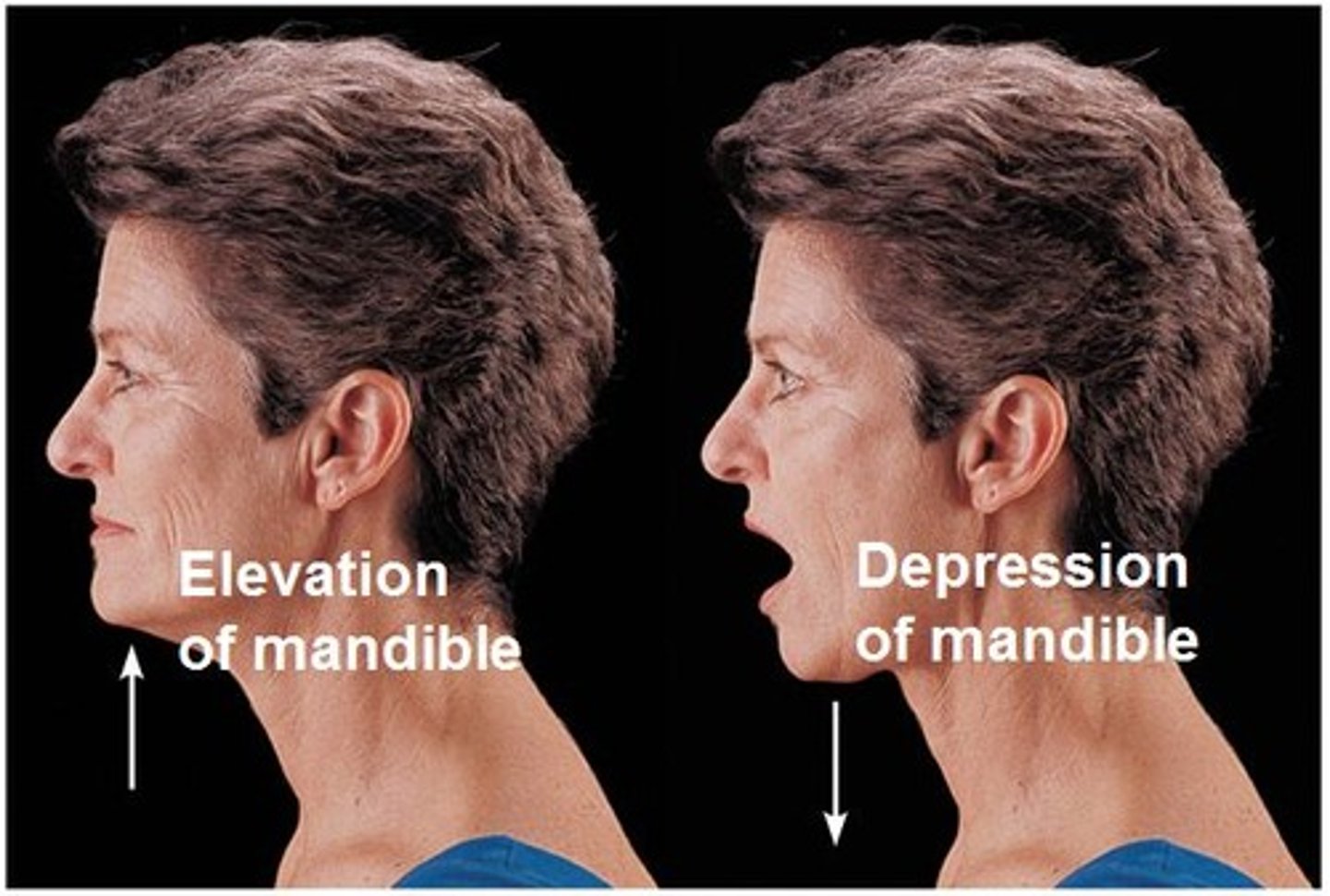
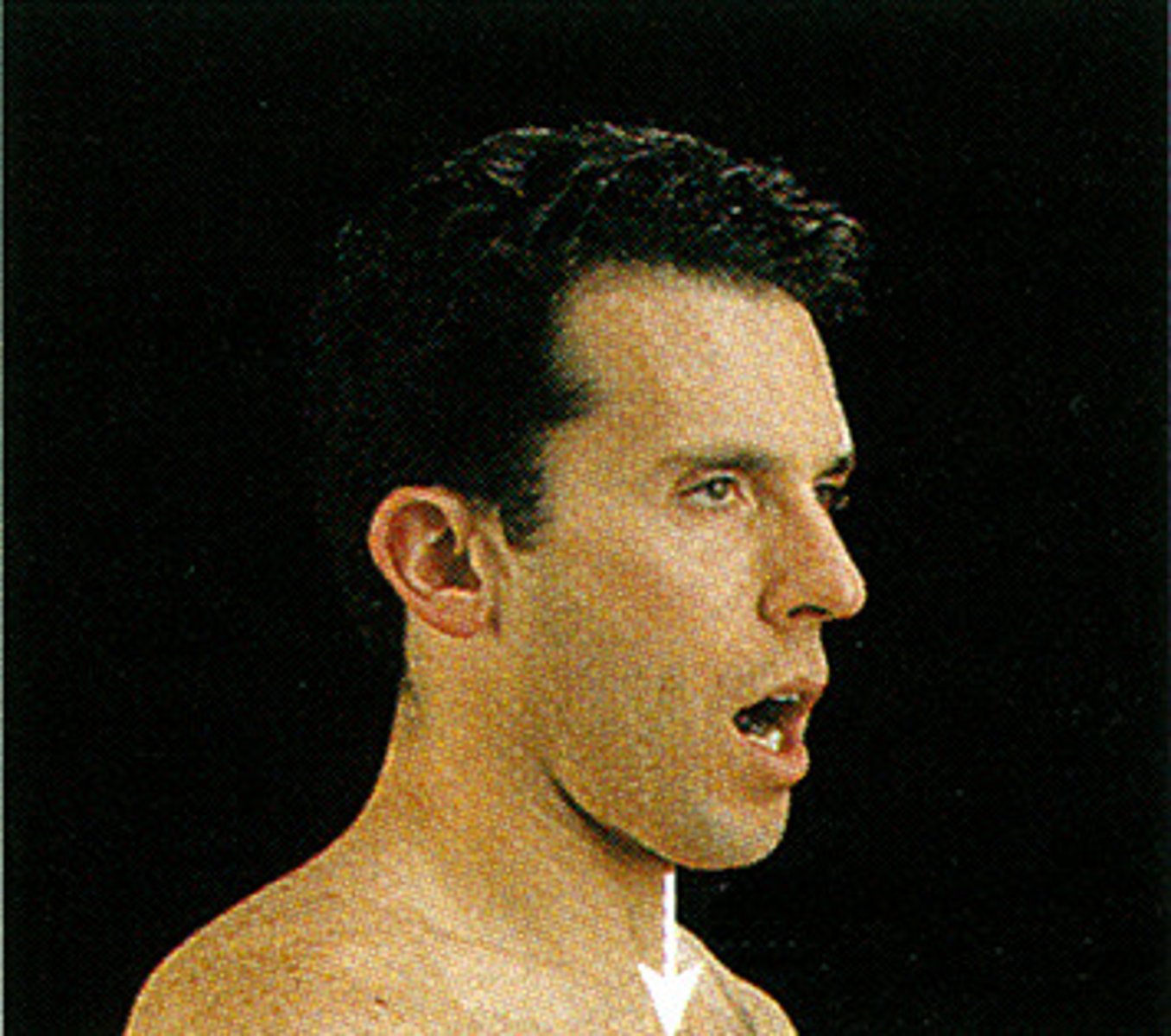
Depression
Moving a body part inferiorly.
Example: Depression of a mandible during chewing
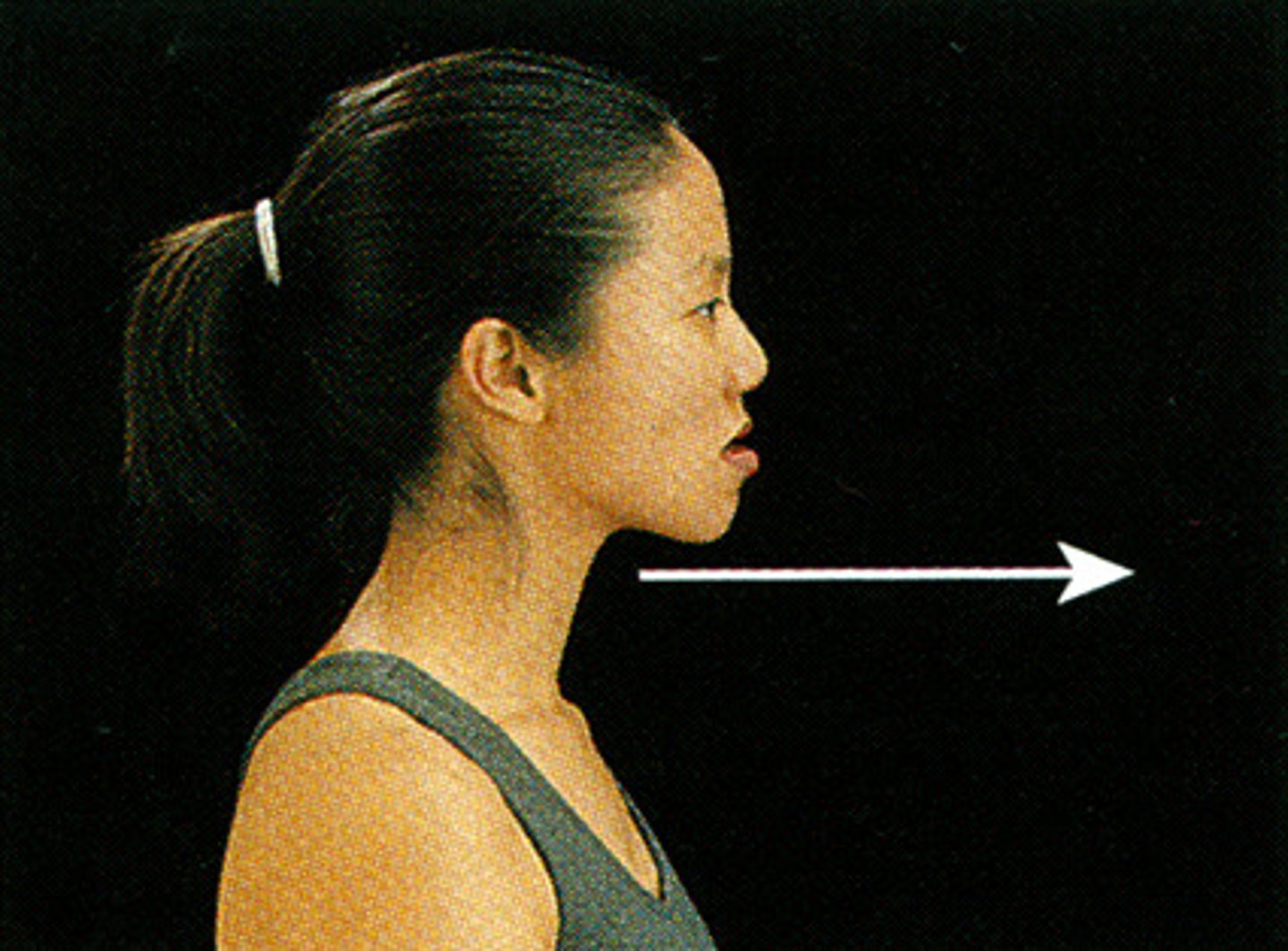
Protraction
Moving a body part in the anterior direction.
Example: When you move your mandible (lower jaw) forward to stick out your chin.
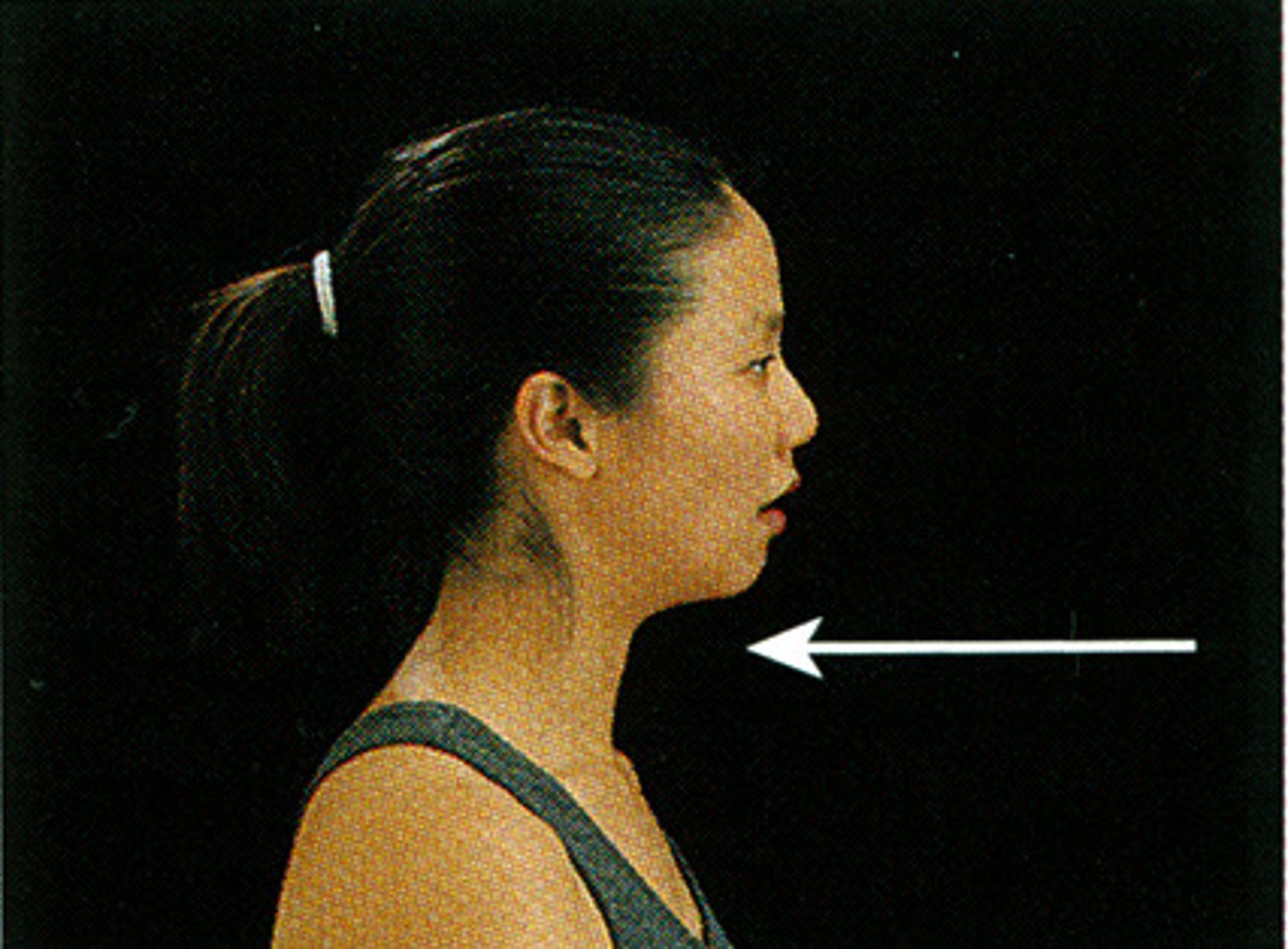
Retraction
Moving a body part in the posterior direction.
Example: When the scapulae (shoulder blades) move closer to the midline of the back, as when pulling the shoulders back.
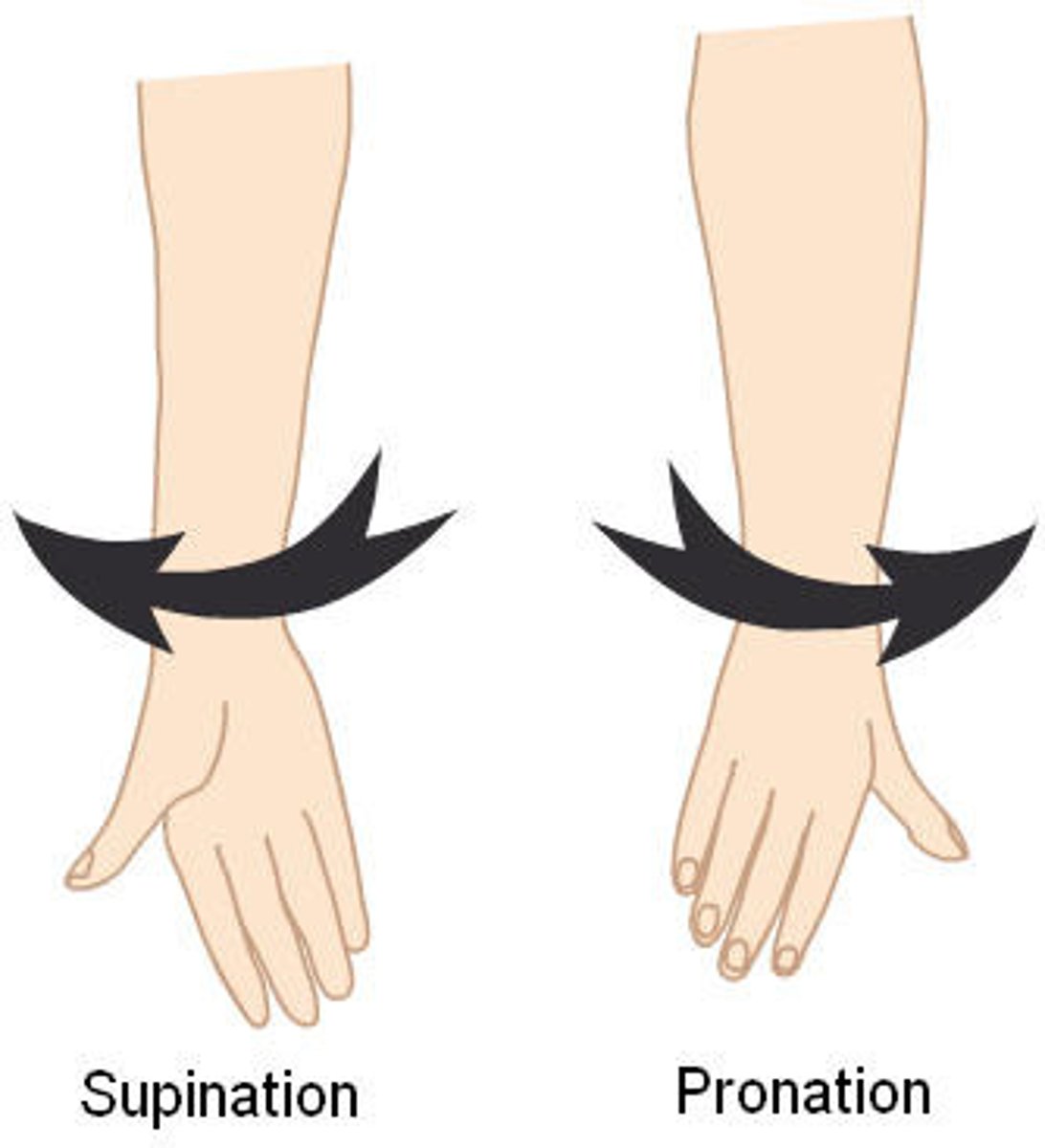
Supination
Rotating the forearm so the palm faces anteriorly.
Example: Occurs when the forearm, specifically the radius, rotates laterally so that the palm faces anteriorly.
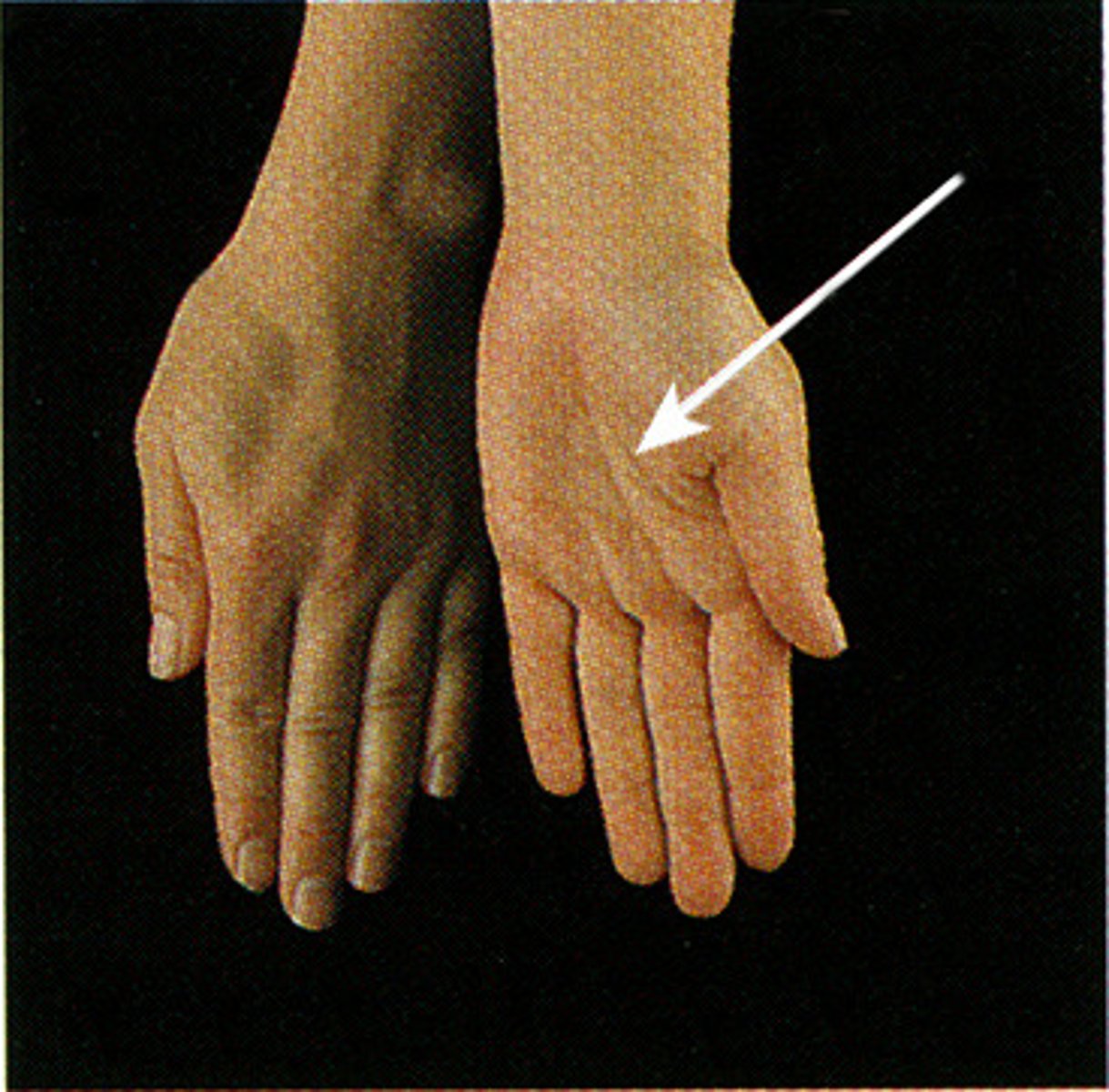
Pronation
Rotating the forearm so the palm faces posteriorly. Pronation brings the radius across the ulna so that the two bones form an X.
Example: Occurs when the radius rotates medially so that the palm faces posteriorly
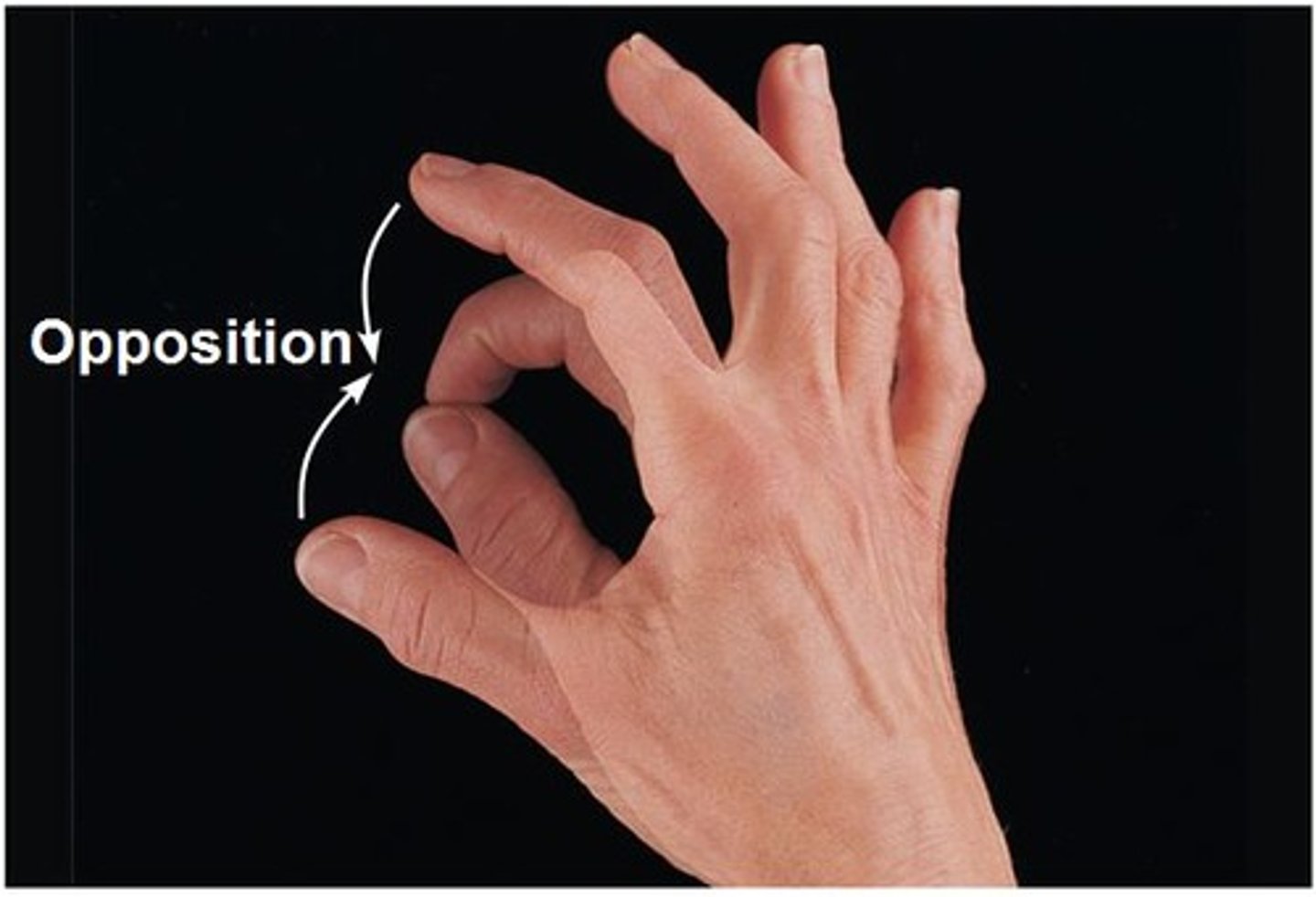
Opposition
Moving the thumb to touch the tips of the other fingers. In the palm, the saddle joint between metacarpal I and the trapezium allows a movement called opposition of the thumb.
Example: you move your thumb across the palm enabling it to touch the tips of the other fingers on the same hand
Inversion
Turning the sole of the foot medially.
Example: To invert the foot, turn the sole medially
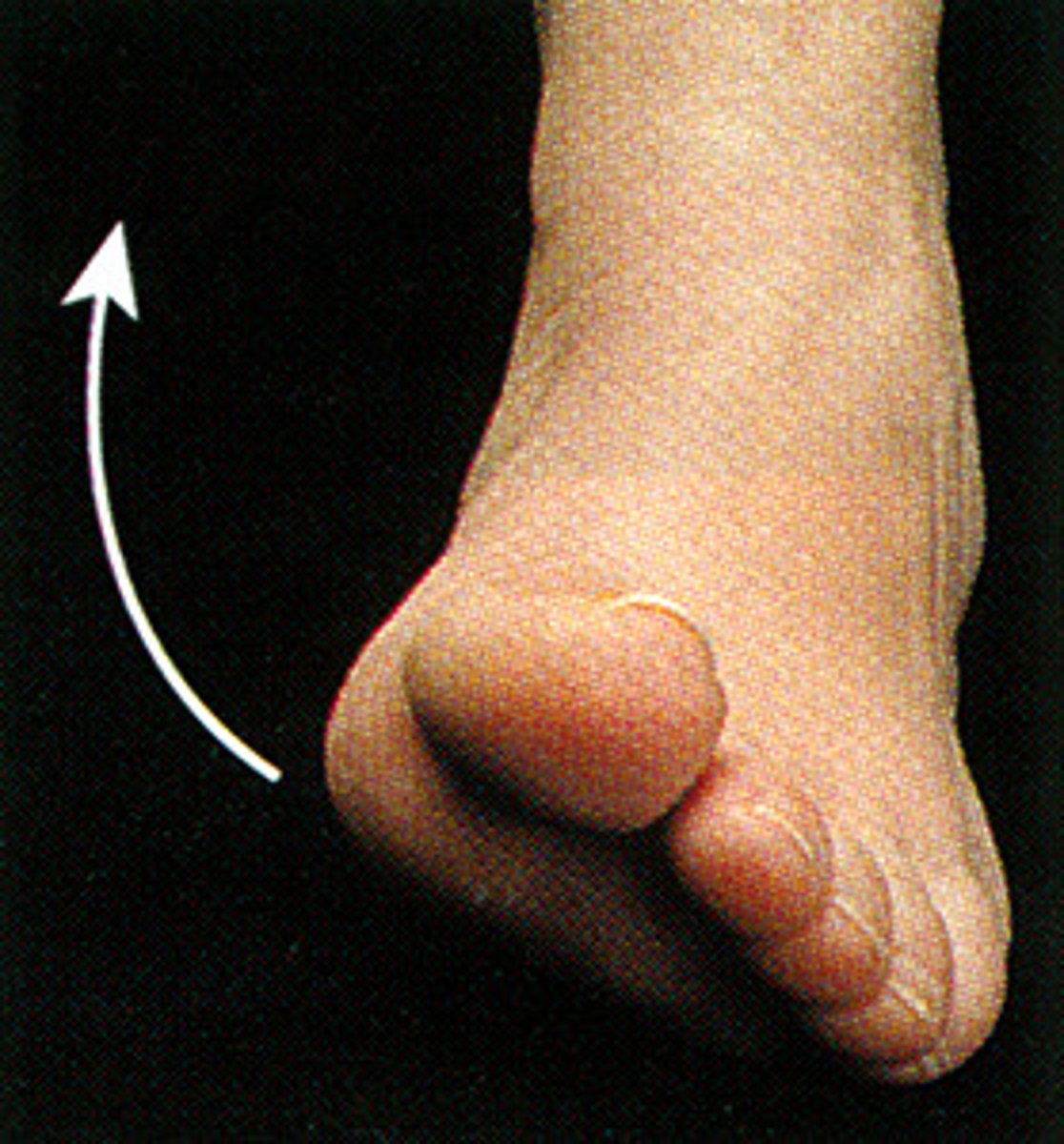
Eversion
Turning the sole of the foot laterally.
Example: To evert the foot, turn the sole laterally
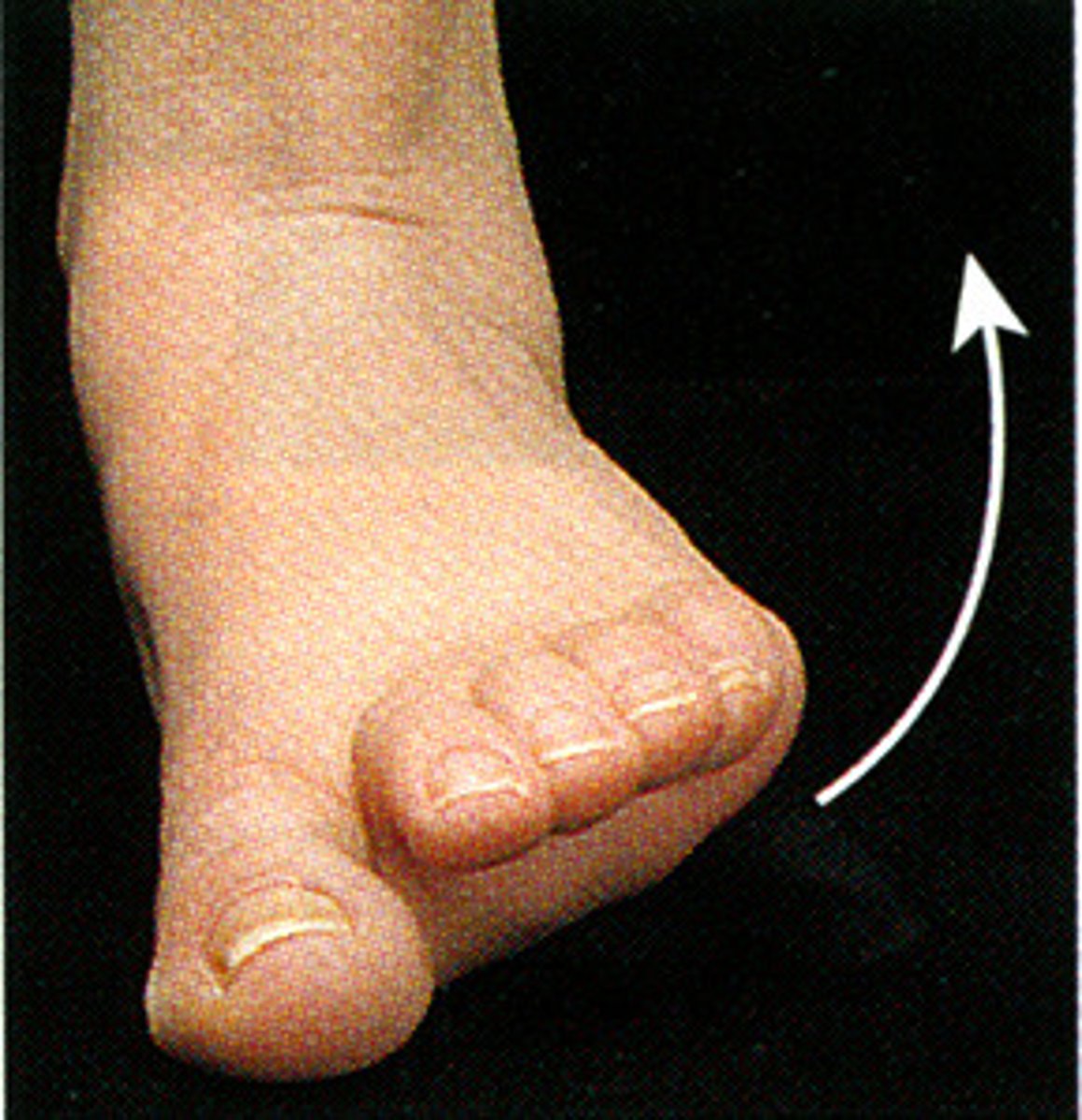
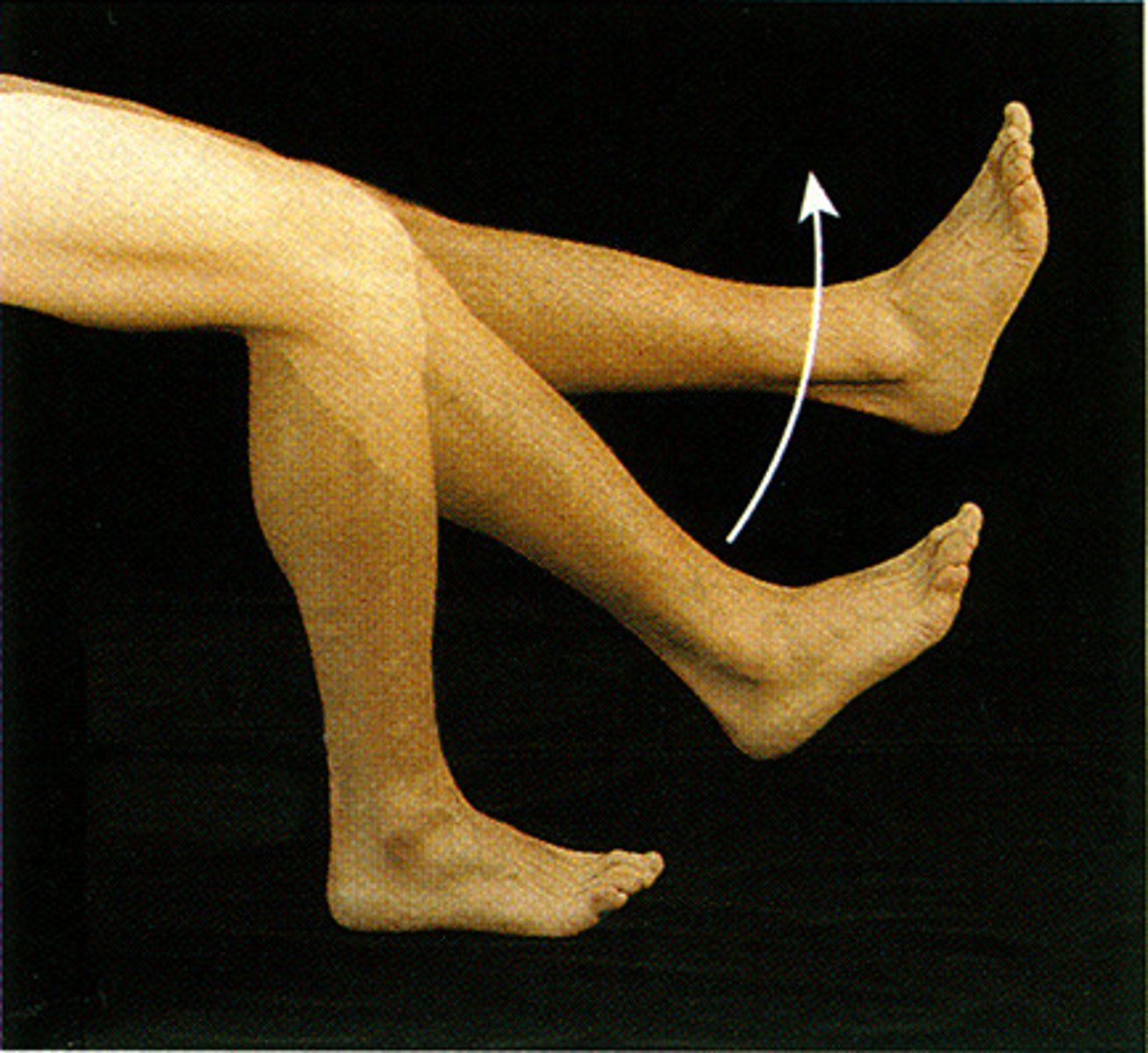
Dorsiflexion
Lifting the foot so its superior surface approaches the shin.
Example: Standing with your heels

Plantar Flexion
a depression movement of the feet and elevation of the heel.
Example: tip-toeing motion of the feet in ballerina when they dance.

Nonaxial
Adjoining bones move but not in any specific axis.
Example: plane joint of intercarpal.
Uniaxial
Movement occurs around a single axis.
Example: the elbow joint
Biaxial
Movement can occur around two axes; thus, the joint enables motion along both the frontal and sagittal planes.
Example: the wrist joint, flexion-extension and abduction-adduction.
Multiaxial
Movement can occur around all three axes and along all three body planes: frontal, sagittal, and transverse.
Example: The shoulder joint, flexion/extension, abduction/adduction, and medial/lateral rotation.
Plane
Flat articular surface allowing non-axial movement such as gliding.
Example: intercarpal & intertarsal joints, joints between vertebral articular surfaces.
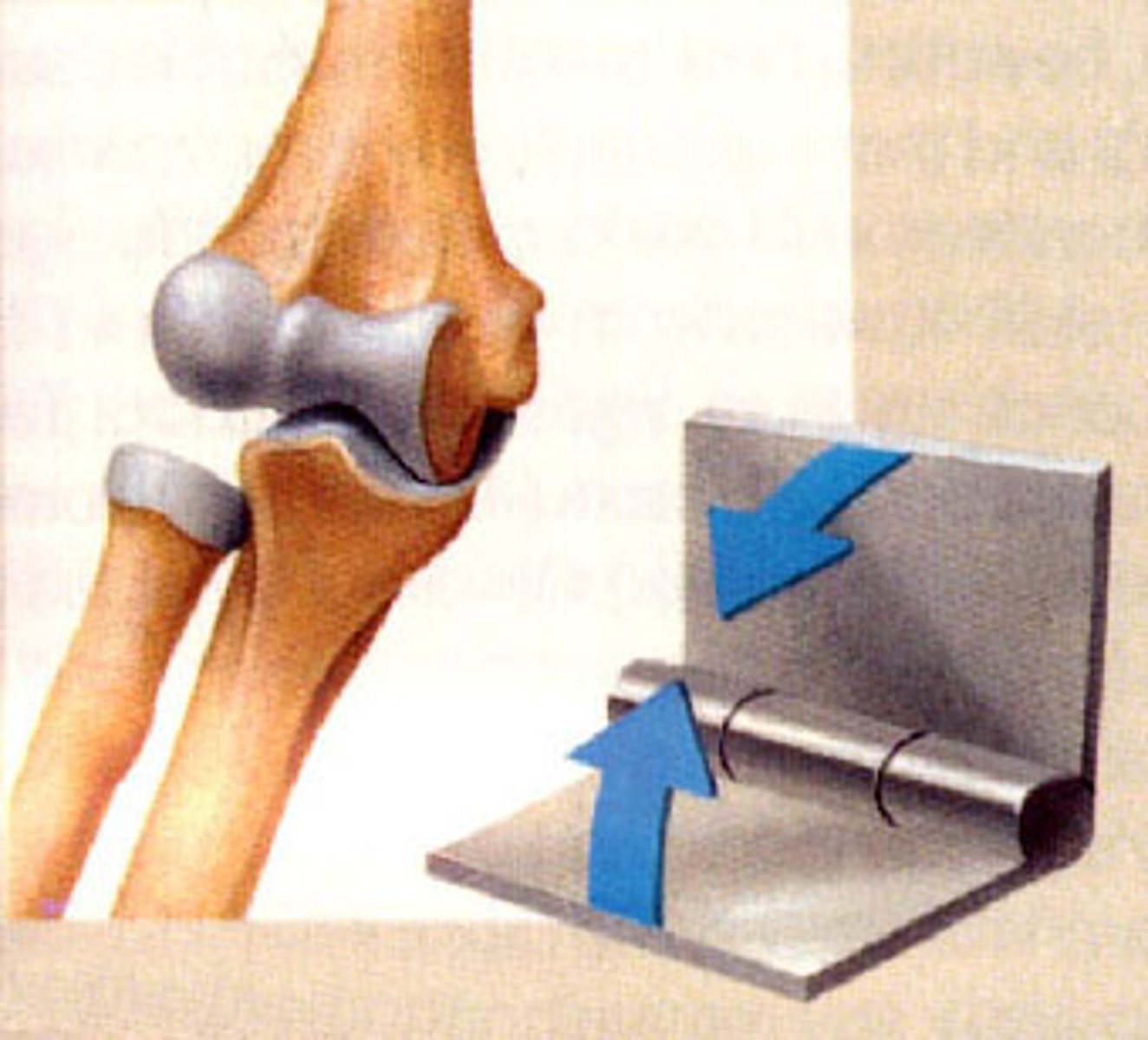
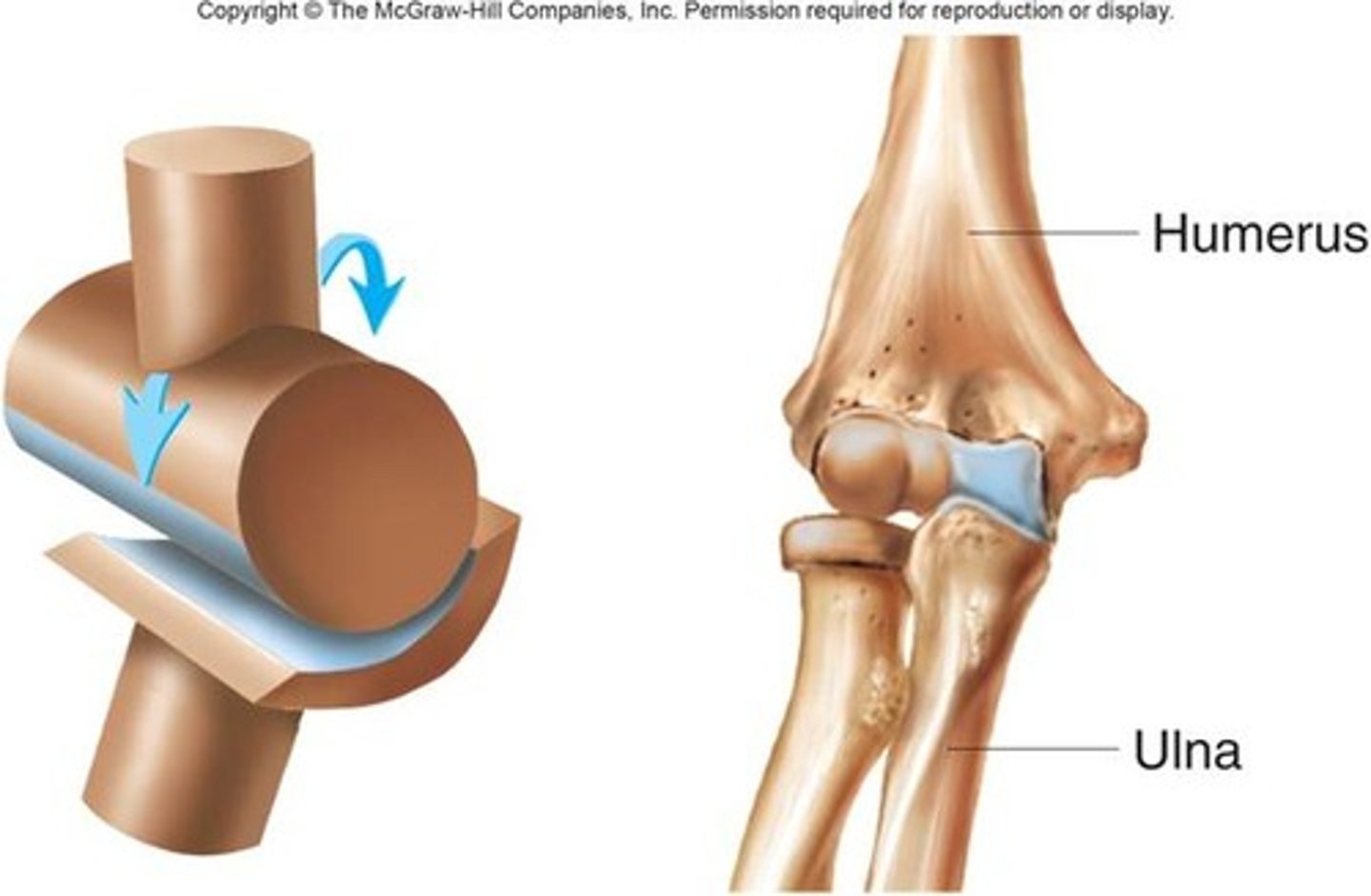
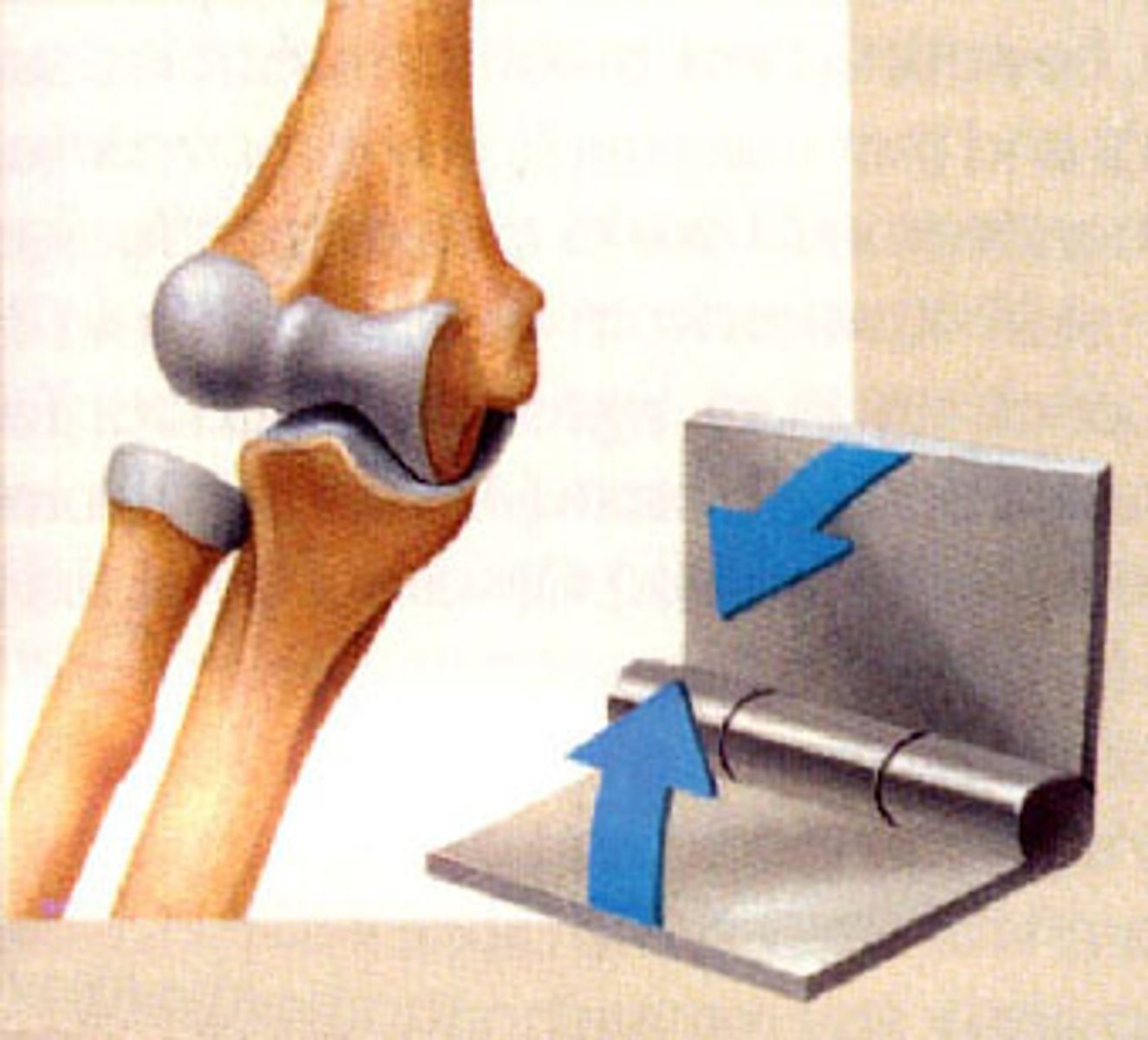
Hinge
The convex surface of one bone fits into the concave surface of another bone, allowing for angular motion along one plane.
Example: Elbow joints, interphalangeal joints
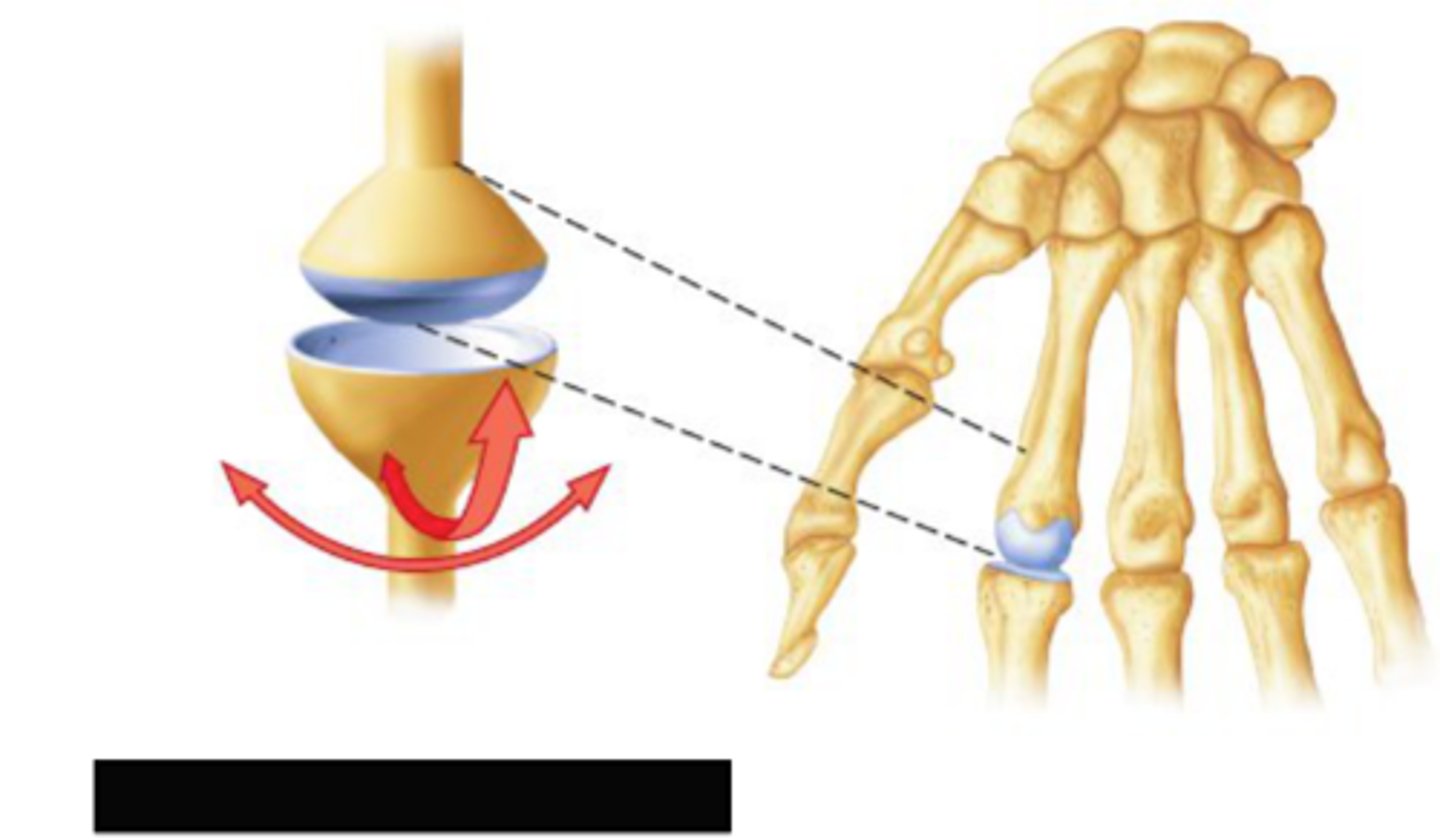
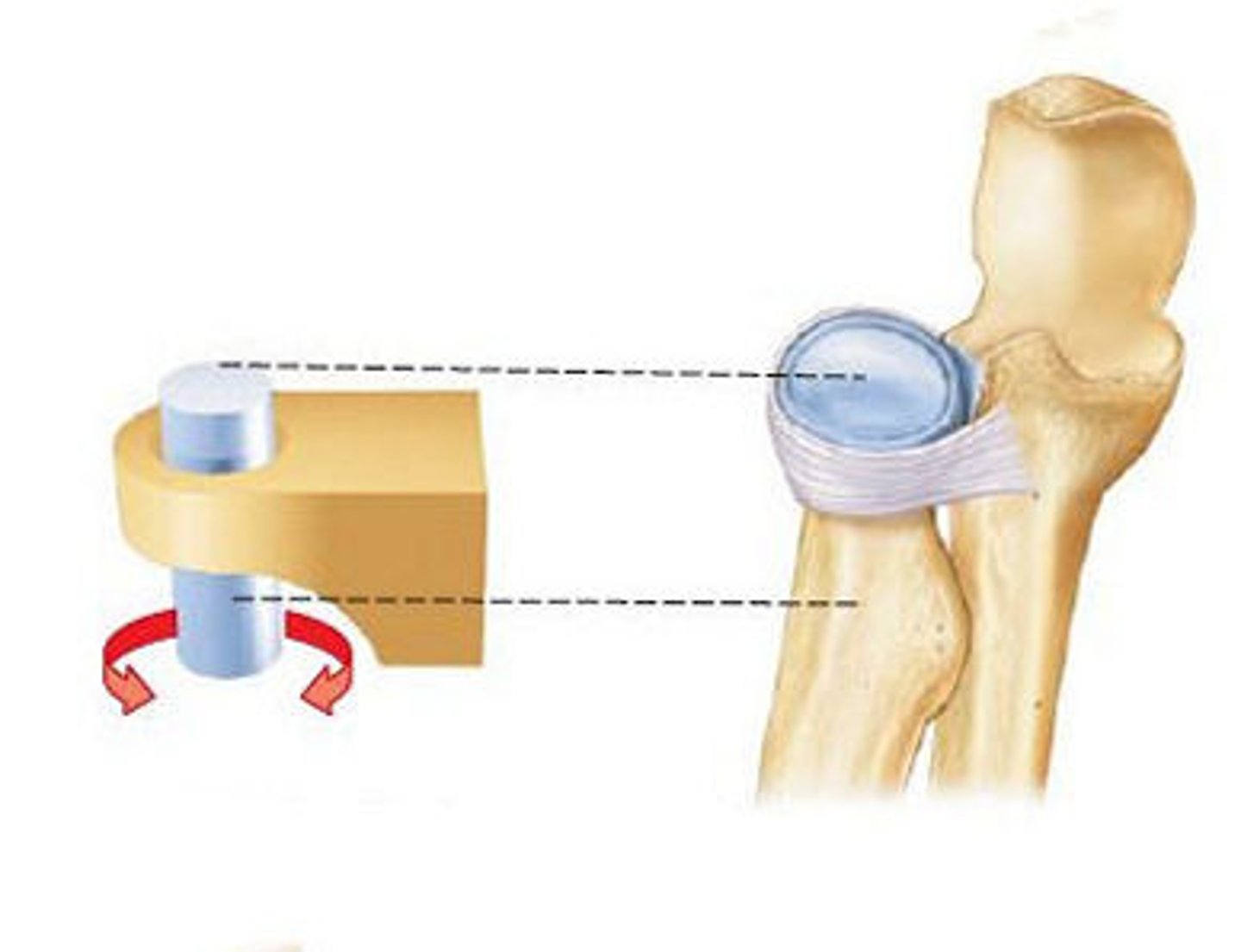
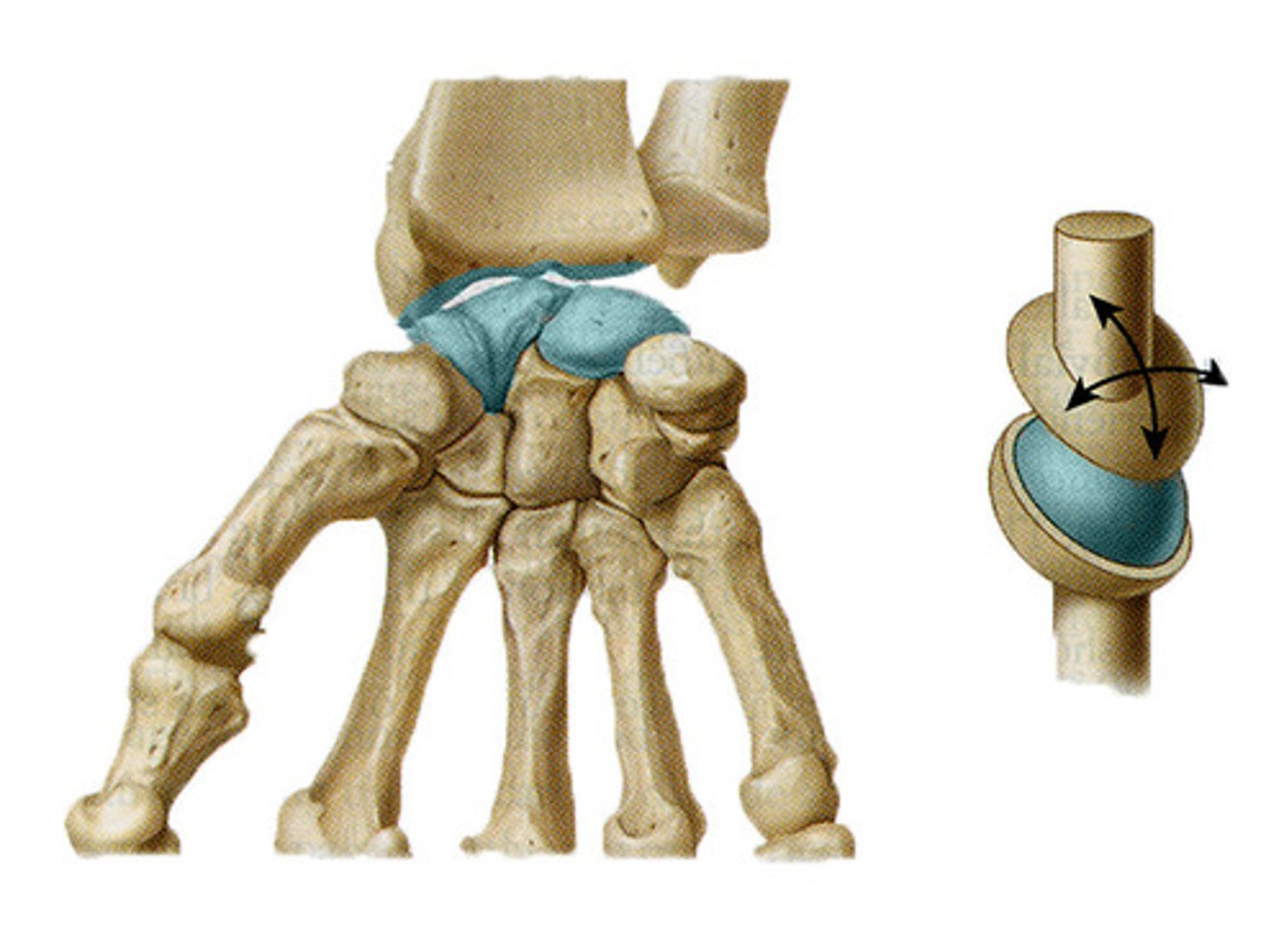
Pivot
A rounded or pointed surface of one bone articulates with a ring formed by another bone and a ligament, allowing for rotational movement around a central axis.
Example: Proximal radioulnar joints, atlantoaxial joint
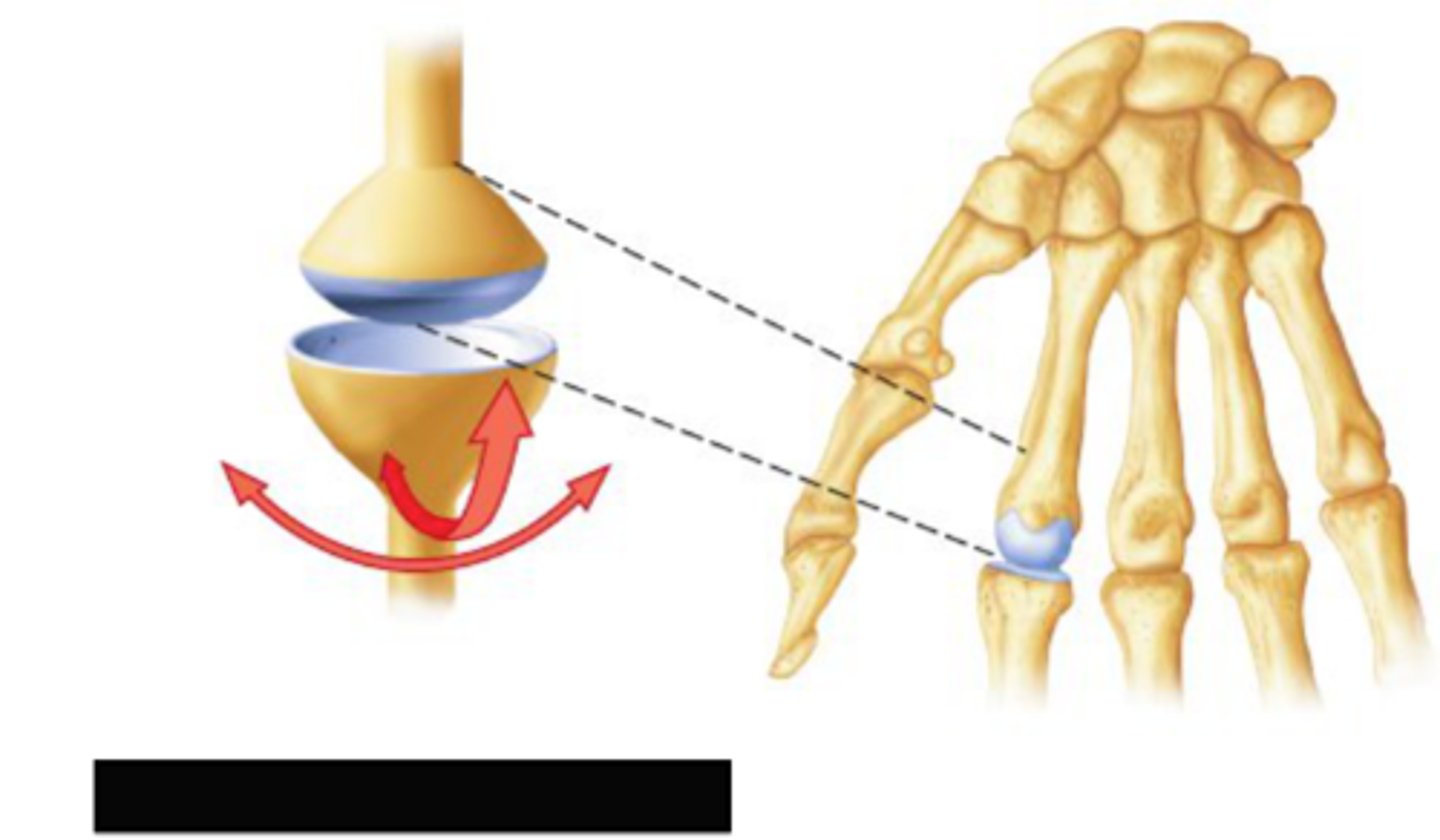
Condylar
The oval-shaped condyle of one bone fits into the elliptical-shaped cavity of another bone, allowing for angular motion along two planes.
Example: Metacarpophalangeal (knuckle) joints, wrist joints
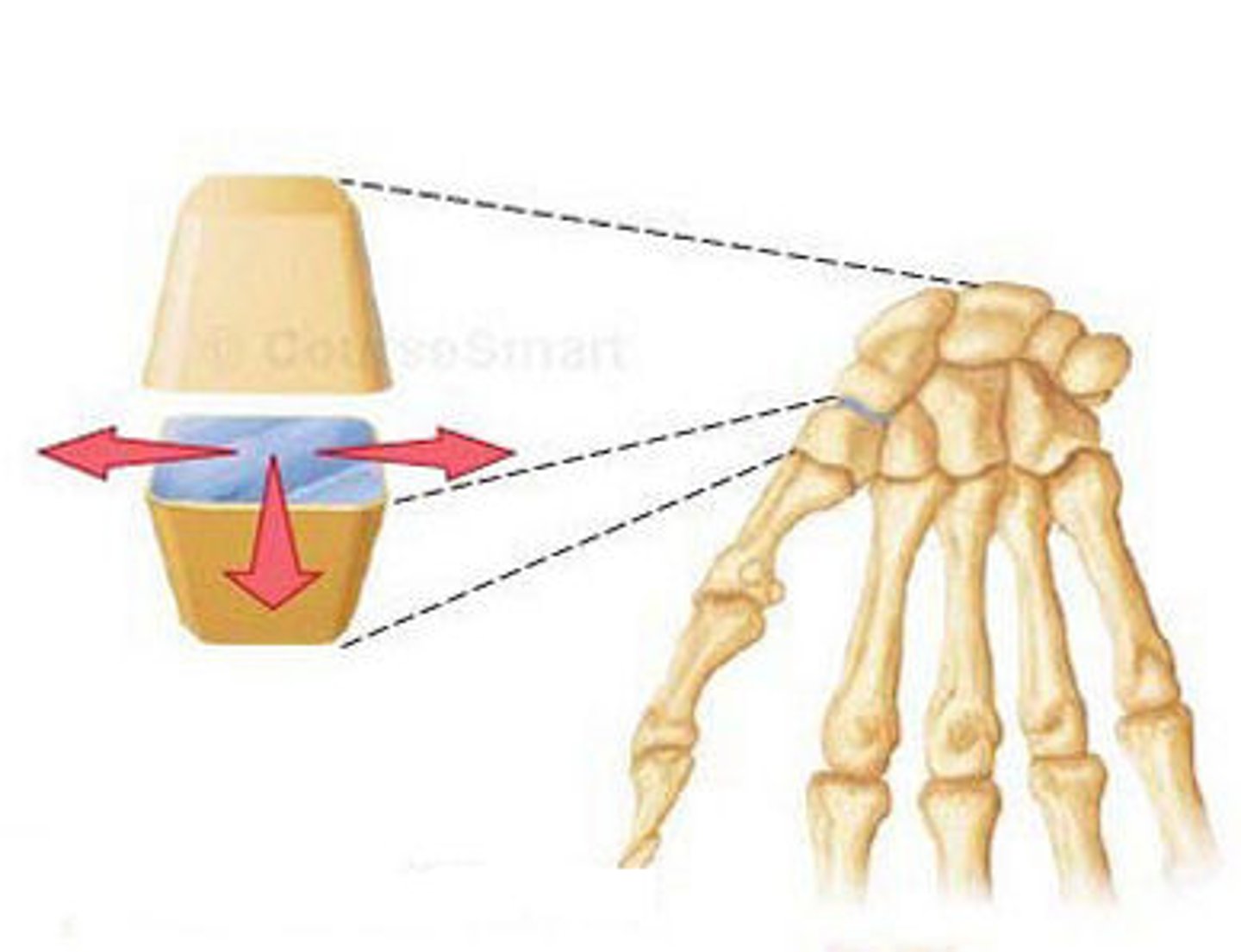
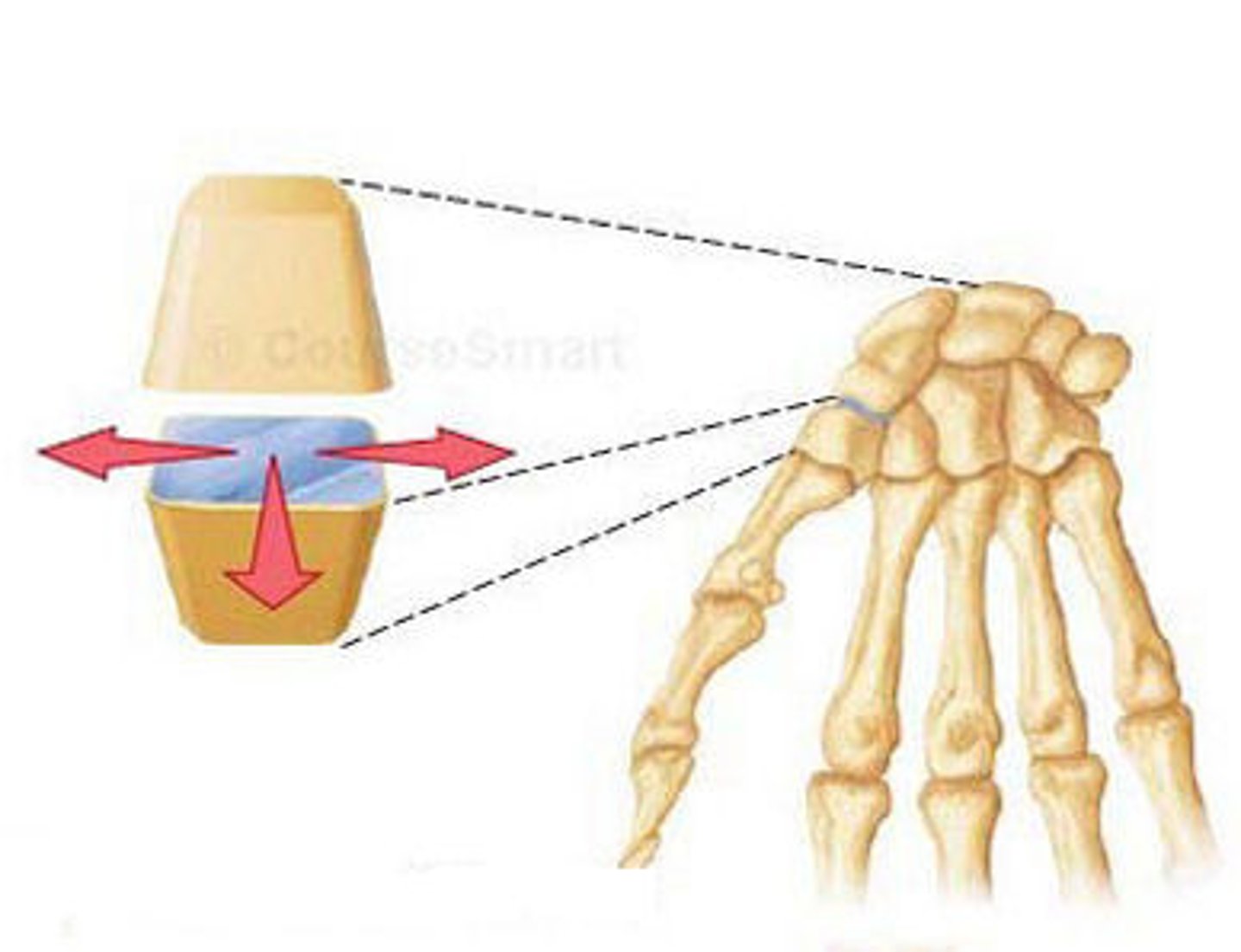
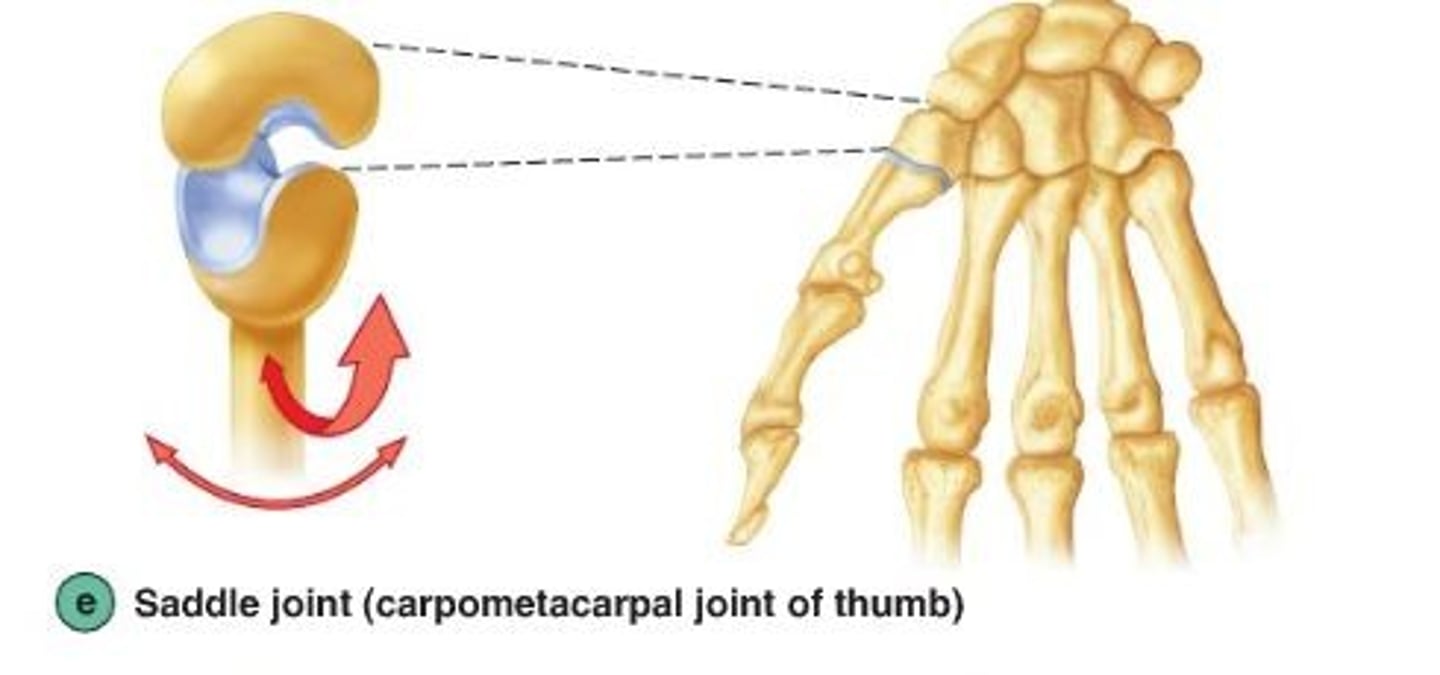
Saddle
The articular surfaces of both bones have a saddle shape, allowing for angular motion along two planes with increased range of motion compared to a condyloid joint.
Example: Carpometacarpal joints of the thumbs
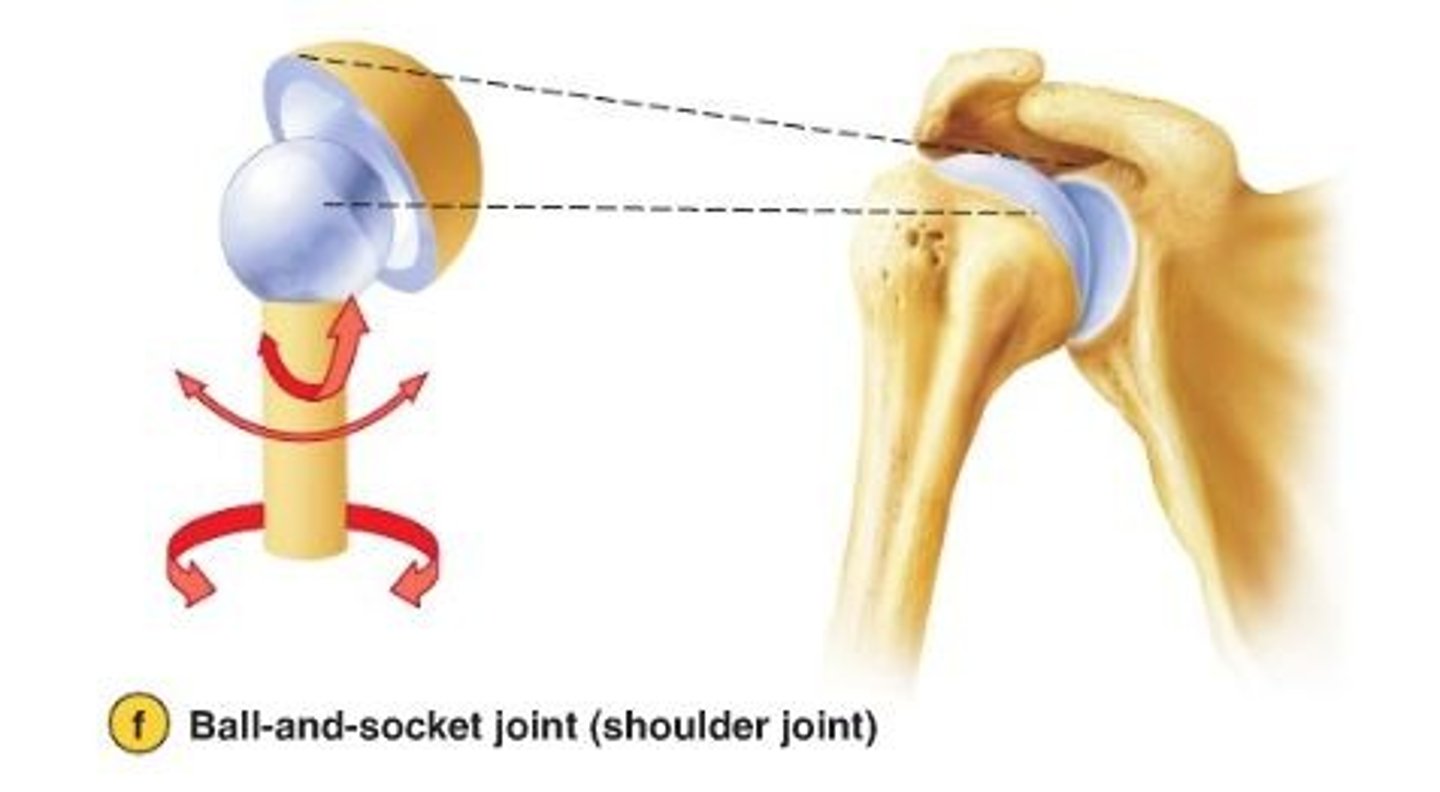
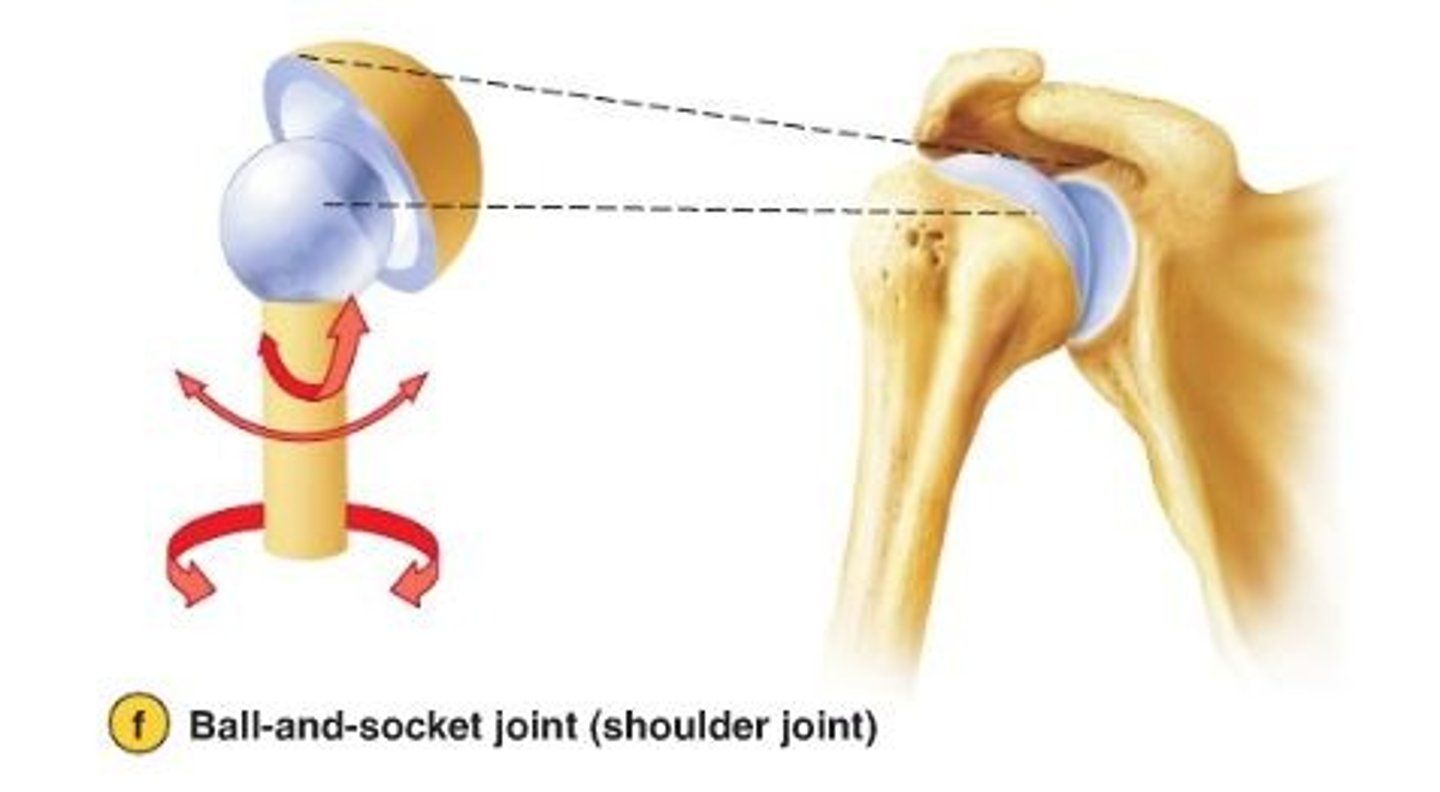
Ball-and-Socket
The spherical head of one bone articulates with the cup-like depression of another bone, allowing for motion along multiple axes.
Example: Shoulder joints and hip joints
Number and Position of Stabilizing Ligaments
The capsules and ligaments of synovial joints help hold the bones together and prevent excessive or undesirable motions. Ligaments located on the medial or inferior side of a joint resist excessive abduction; lateral and superiorly located ligaments resist adduction. Anterior ligaments resist excessive extension and lateral rotation; posterior ligaments resist excessive flexion and medial rotation. The more ligaments a joint has, the stronger it is. Once stretched, ligaments stay stretched but they stretch that much.
Muscle Tone
A constant, low level of contractile force generated by a muscle even when it is not causing movement. Muscle tone helps stabilize joints by keeping tension on the muscle tendons that cross over joints just external to the joint capsule. In this manner the muscle functions like a ligament holding the adjoining bone surfaces together. The muscles that surround a joint help to support and stabilize it. When the muscles are contracted, they create tension that helps to hold the joint in place. This is known as muscle tone.

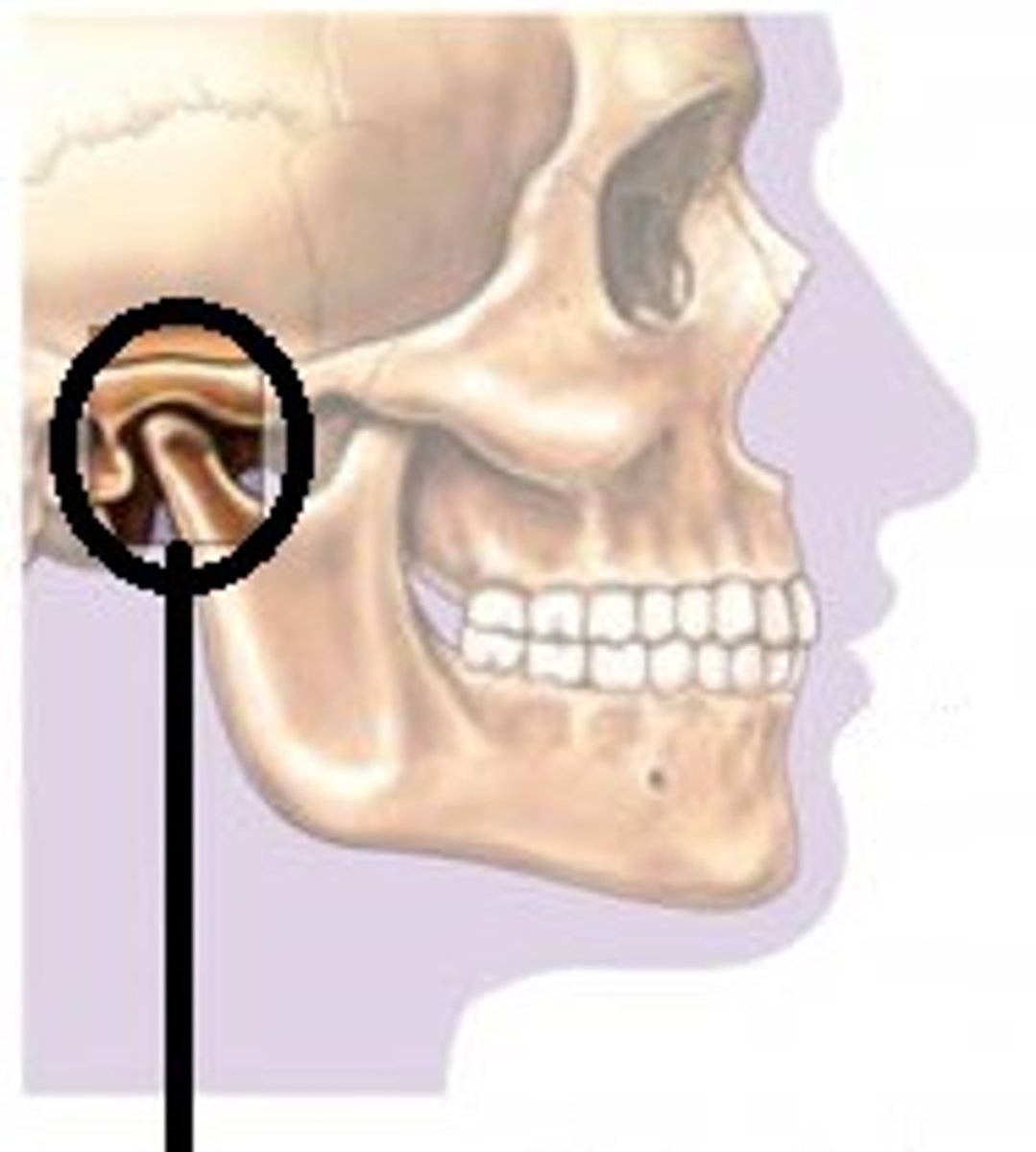
Temporomandibular Joint (TMJ)
Bones:
- condylar process of the mandible and inferior surface of temporal bone
Structural Type:
- Synovial, modified hinge joint.
- Contains articular disc.
Functional Type:
- Diathrotic, gliding and uniaxial
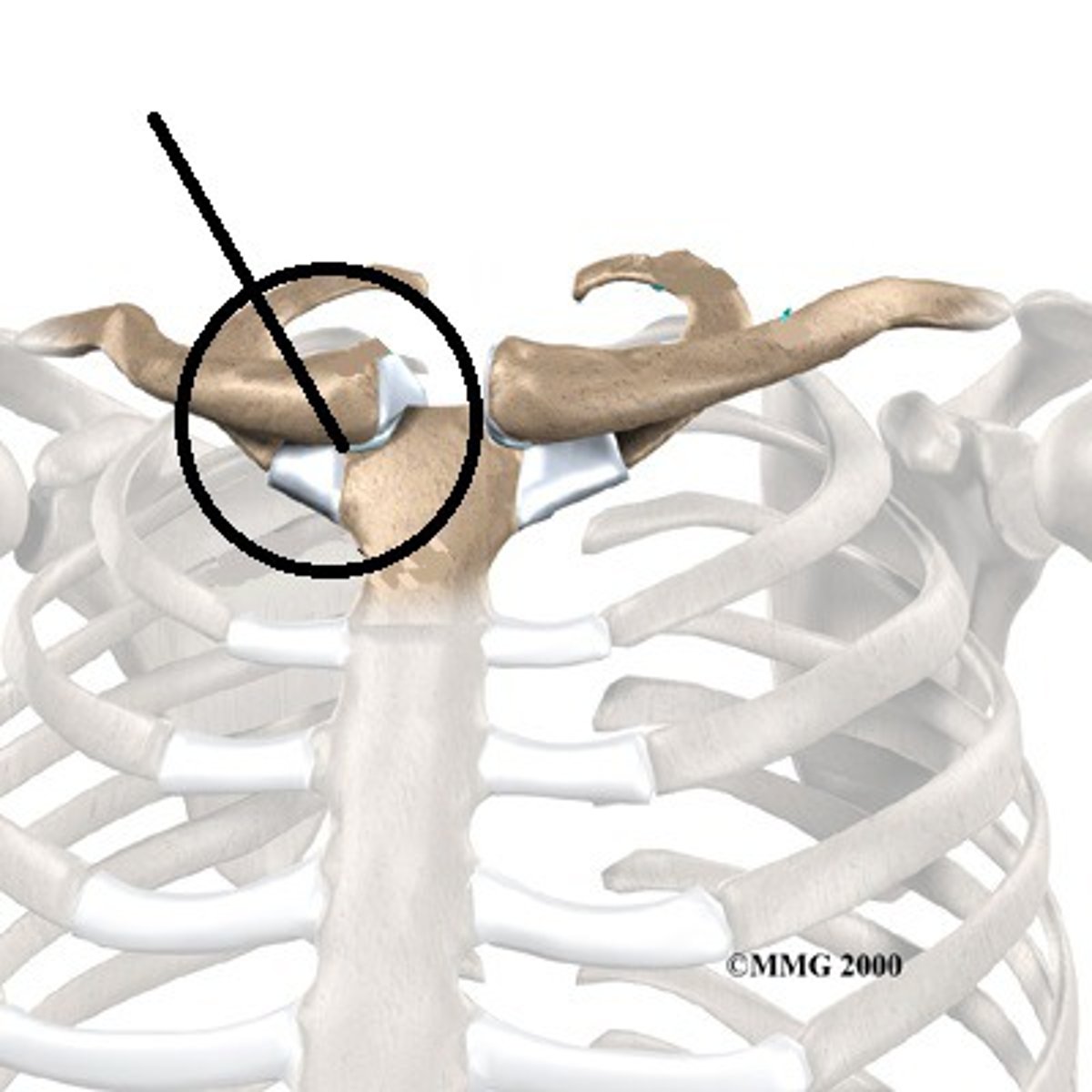
Sternoclavicular Joint
Bones:
- Sternum and clavicle
Structural Type:
- Synovial; shallow saddle (contains articular disc)
Functional Type:
- Diarthrotic; multiaxial (allows clavicle to move in all axes)
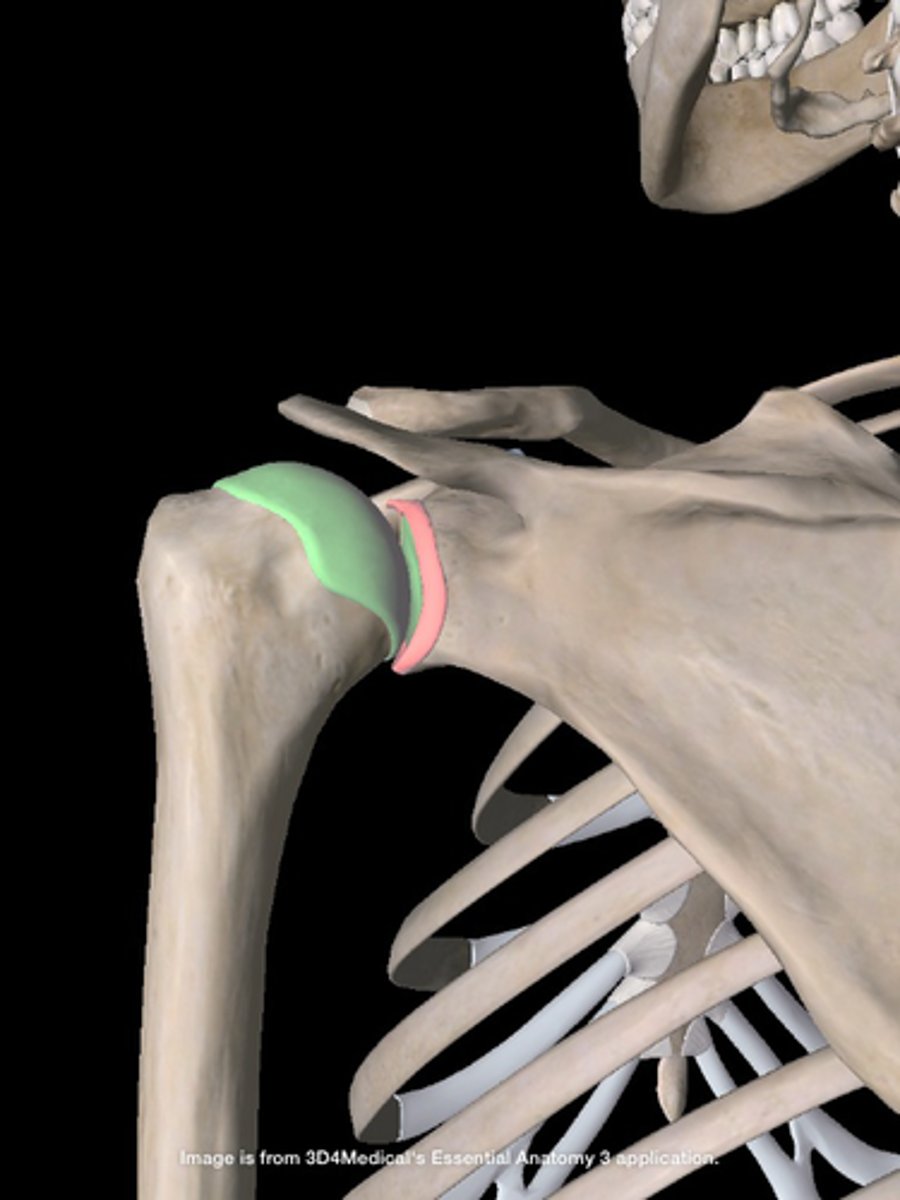
Shoulder (Glenohumeral) Joint
Bones:
- Scapula and humerus
Structural Type:
- Synovial; balland-socket
Functional Type:
- Diarthrotic; multiaxial; flexion, extension, abduction, adduction, circumduction, rotation of humerus
Elbow Joint
Bones:
- Ulna (and radius) with humerus
Structural Type:
- Synovial; hinge
Functional Type:
- Diarthrotic; uniaxial; flexion, extension of forearm
Wrist Joint
Bones:
- Radius and proximal carpals
Structural Type:
- Synovial; condylar
Functional Type:
- Diarthrotic; biaxial; flexion, extension, abduction, adduction, circumduction of hand
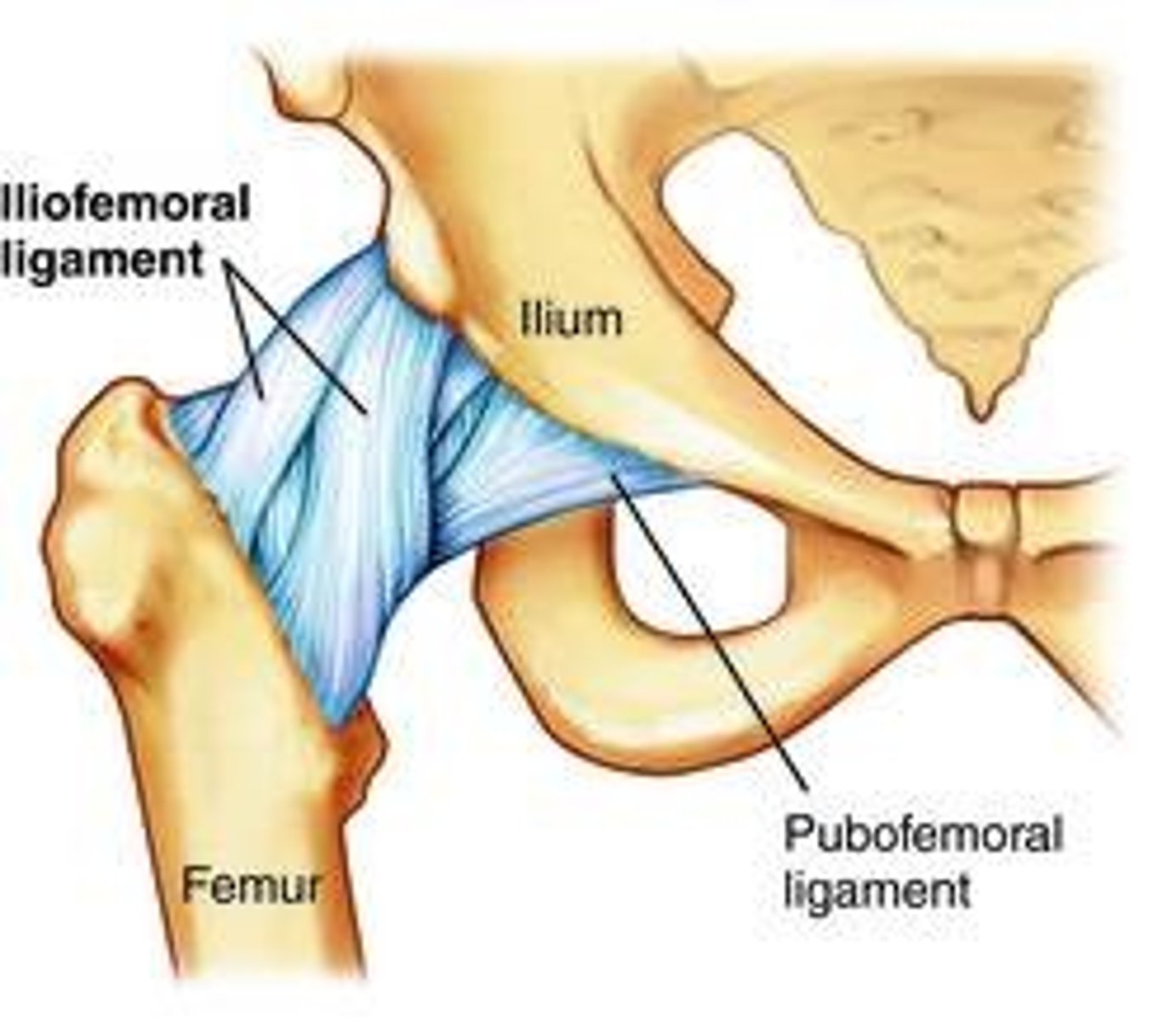
Hip Joint
Bones:
- Hip bone and femur
Structural Type:
- Synovial; ball and socket
Functional Type:
- Diarthrotic; multiaxial; flexion, extension, abduction, adduction, rotation, circumduction of femur
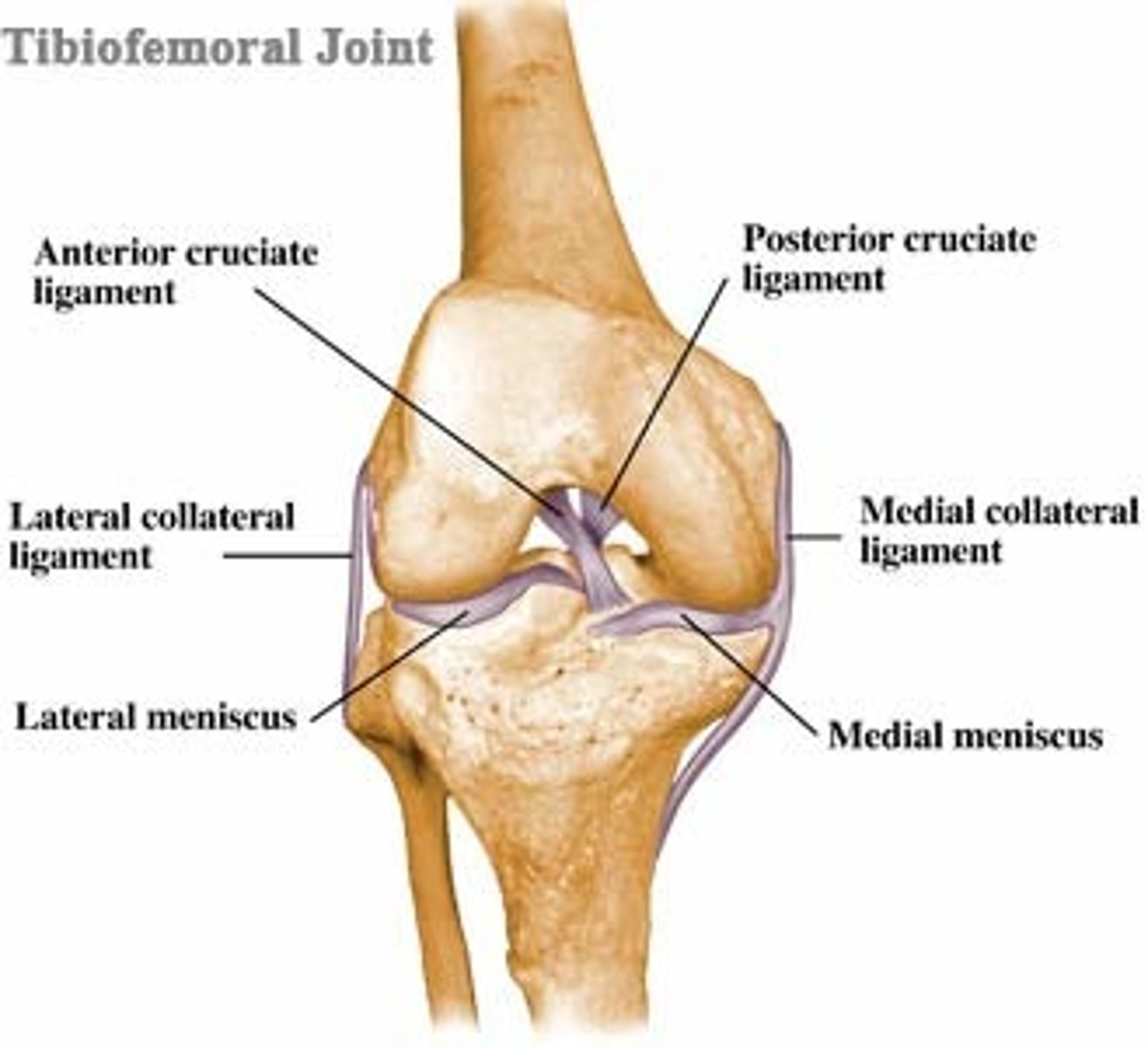
Knee (Tibiofemoral) Joint
Bones:
- Femur and tibia
Structural Type:
- Synovial; modified hinge, structurally bicondylar (contains articular discs)
Functional Type:
- Diarthrotic; biaxial; flexion, extension of leg, some rotation allowed
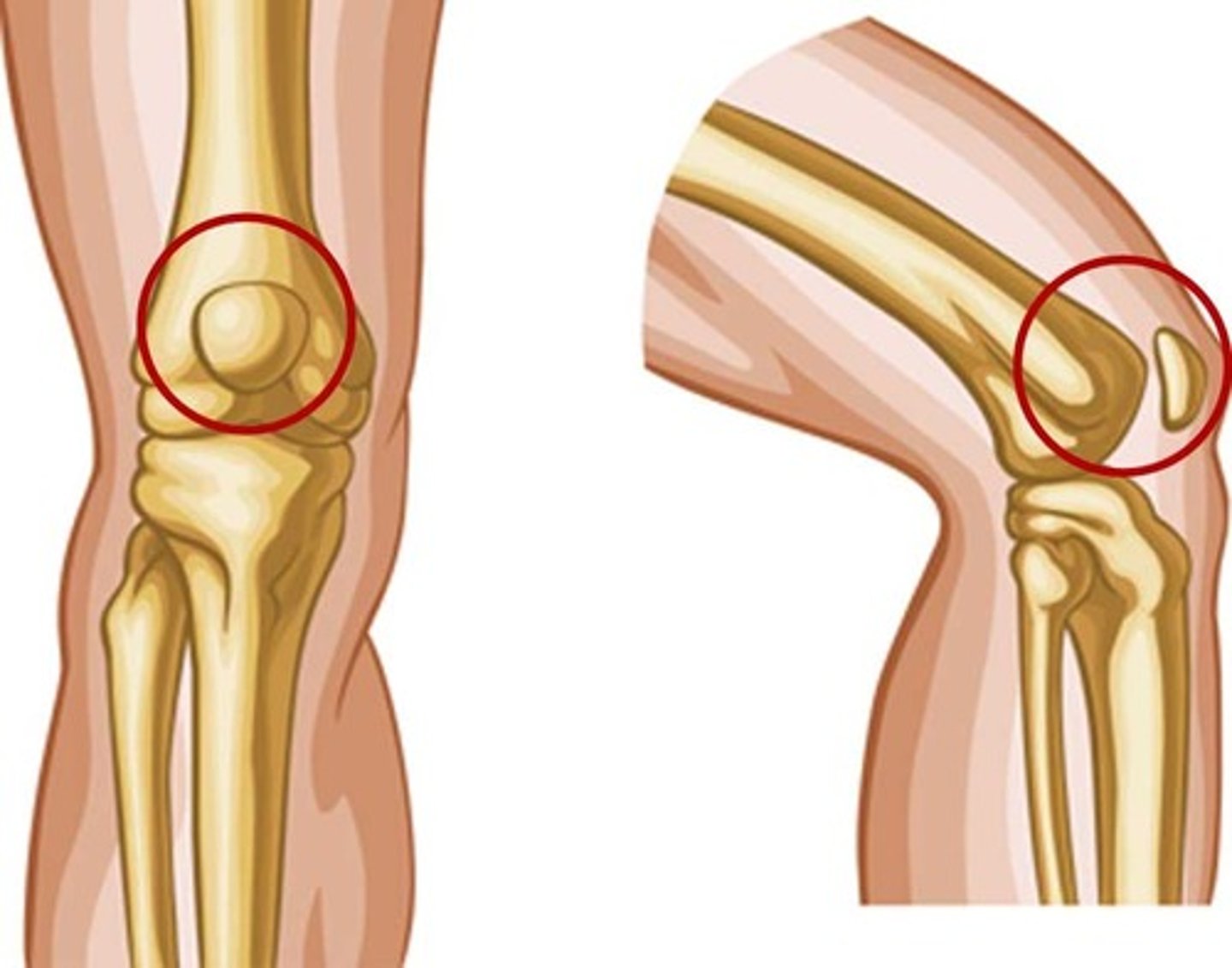
Knee (Femoropatellar) Joint
Bones:
- Femur and patella
Structural Type:
- Synovial; plane
Functional Type:
- Diarthrotic; gliding of patella
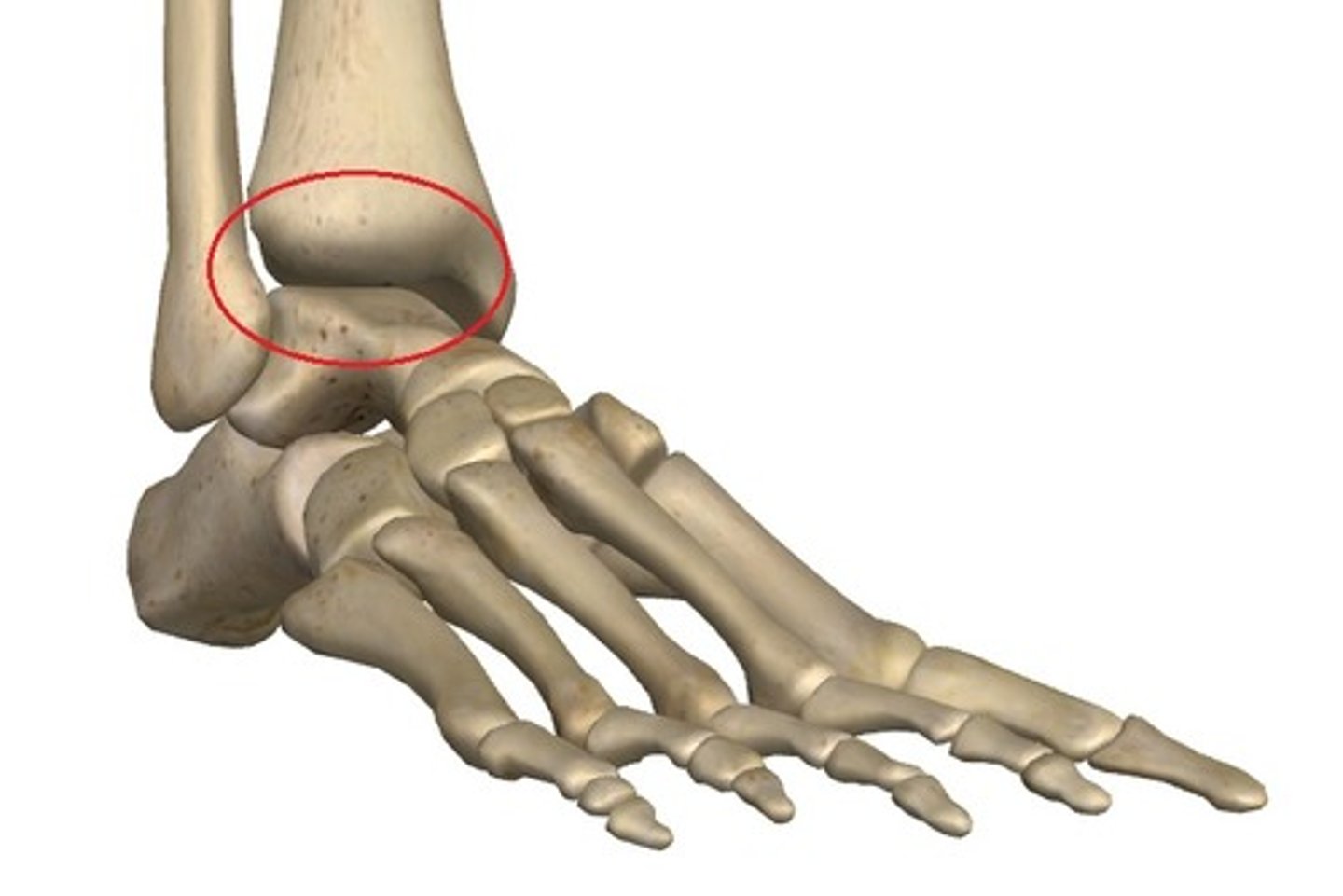
Ankle Joint
Bones:
- Tibia and fibula with the talus
Structural Type:
- Synovial; hinge
Functional Type:
- Diarthrotic; uniaxial; dorsiflexion and plantar flexion of foot
Shoulder (Glenohumeral) Joint Description
In the shoulder joint, stability has been sacrificed to provide the most freely moving joint of the body. This ball-and-socket joint is formed by the head of the humerus and the shallow glenoid cavity of the scapula.
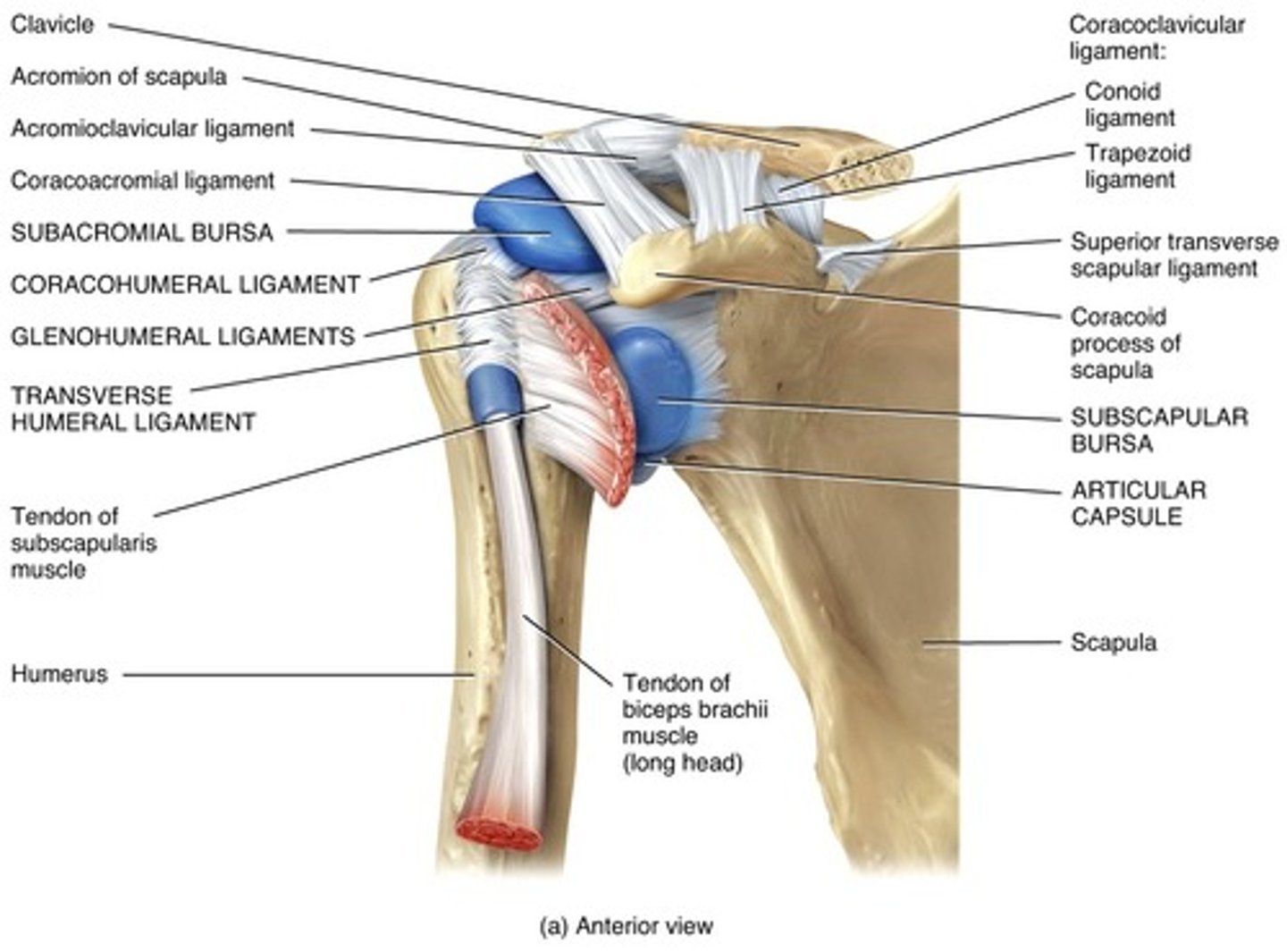
Glenoid Labrum
A rim of fibrocartilage that slightly deepened the glenoid cavity. A shallow cavity contributes little to joint stability

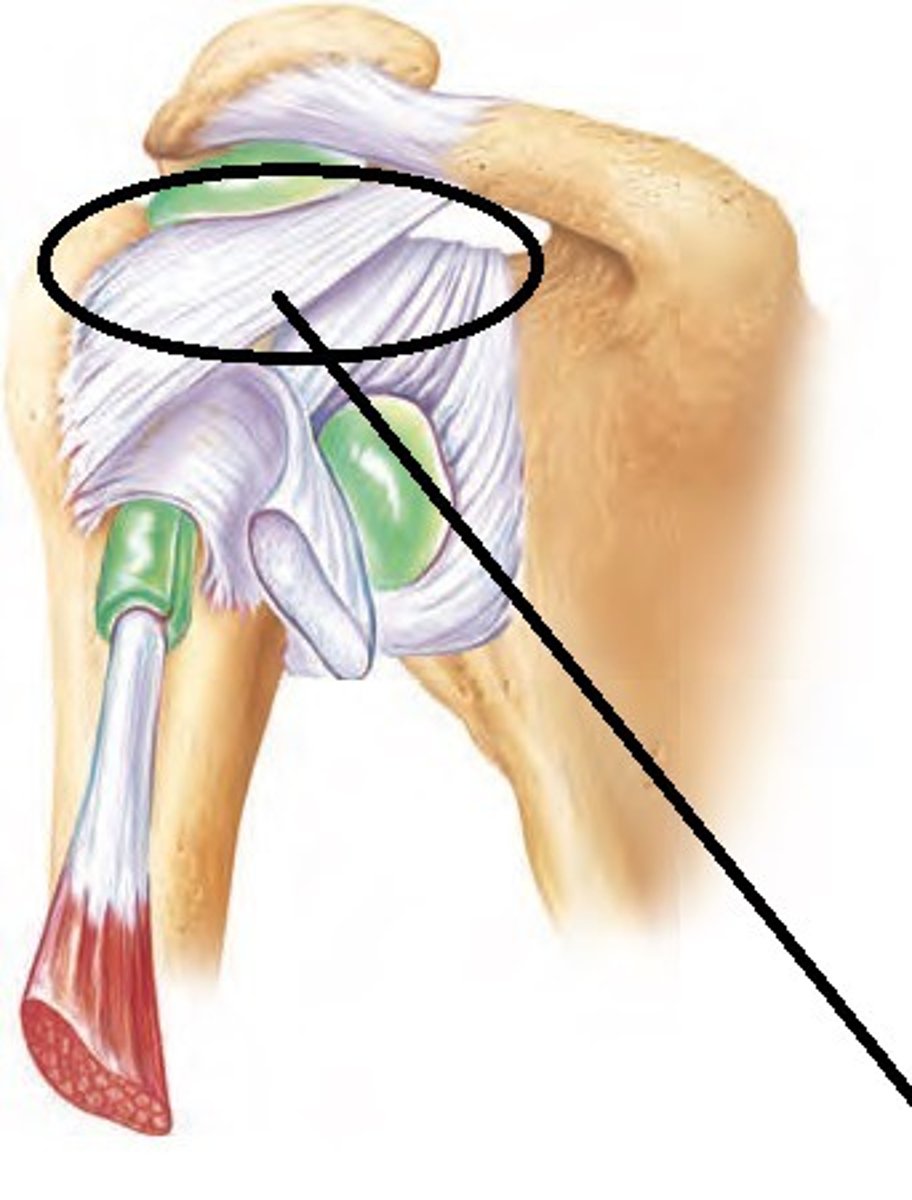
Coracohumeral Ligament
The superior part of the capsule that is the only strong thickening of it. Helps support the weight of the upper limb. Reinforces the upper part of the joint capsule.
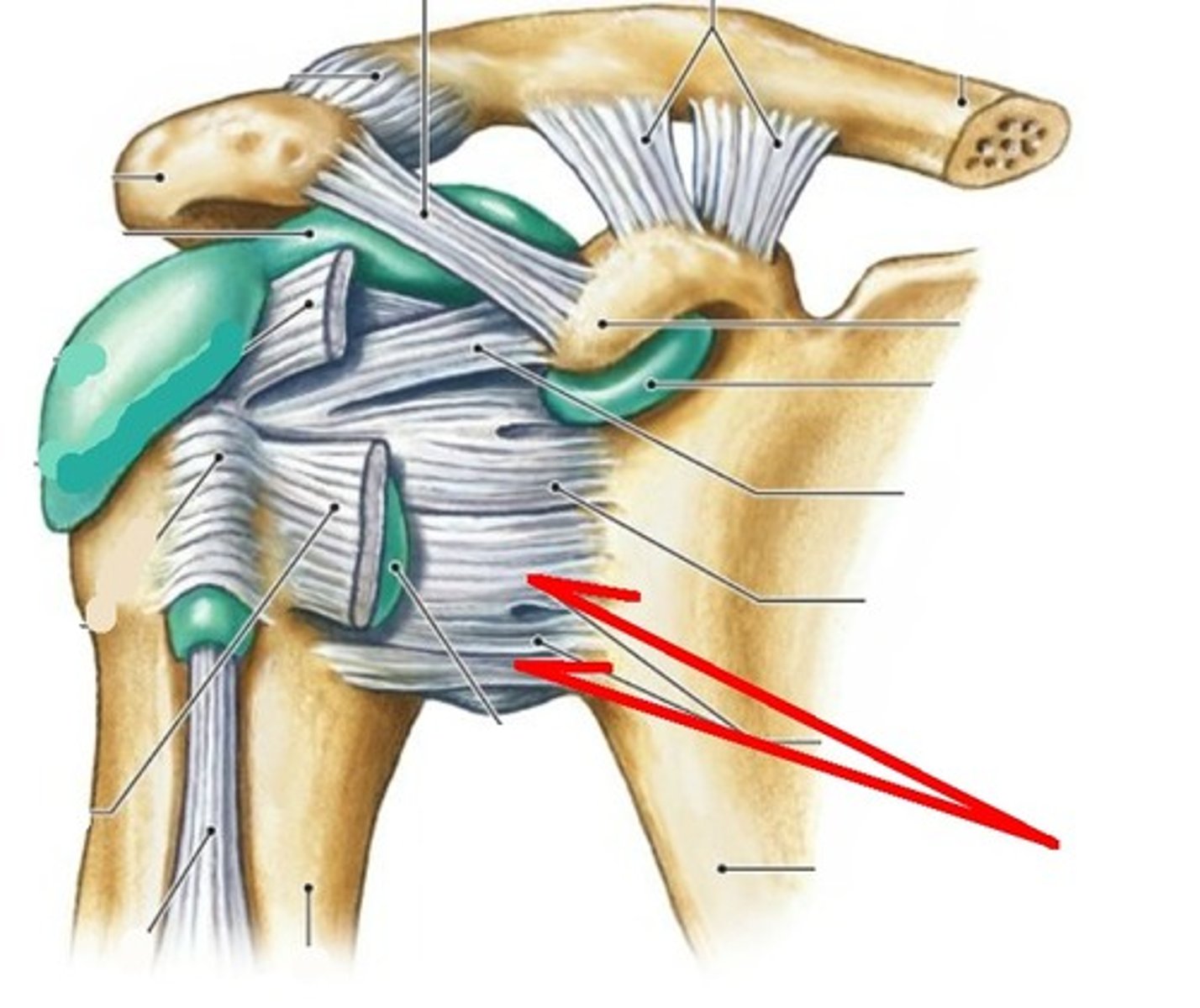
Glenohumeral Ligament
The anterior part of the capsule thickens slightly into three rather weak. A group of three ligaments that also help stabilize the joint.
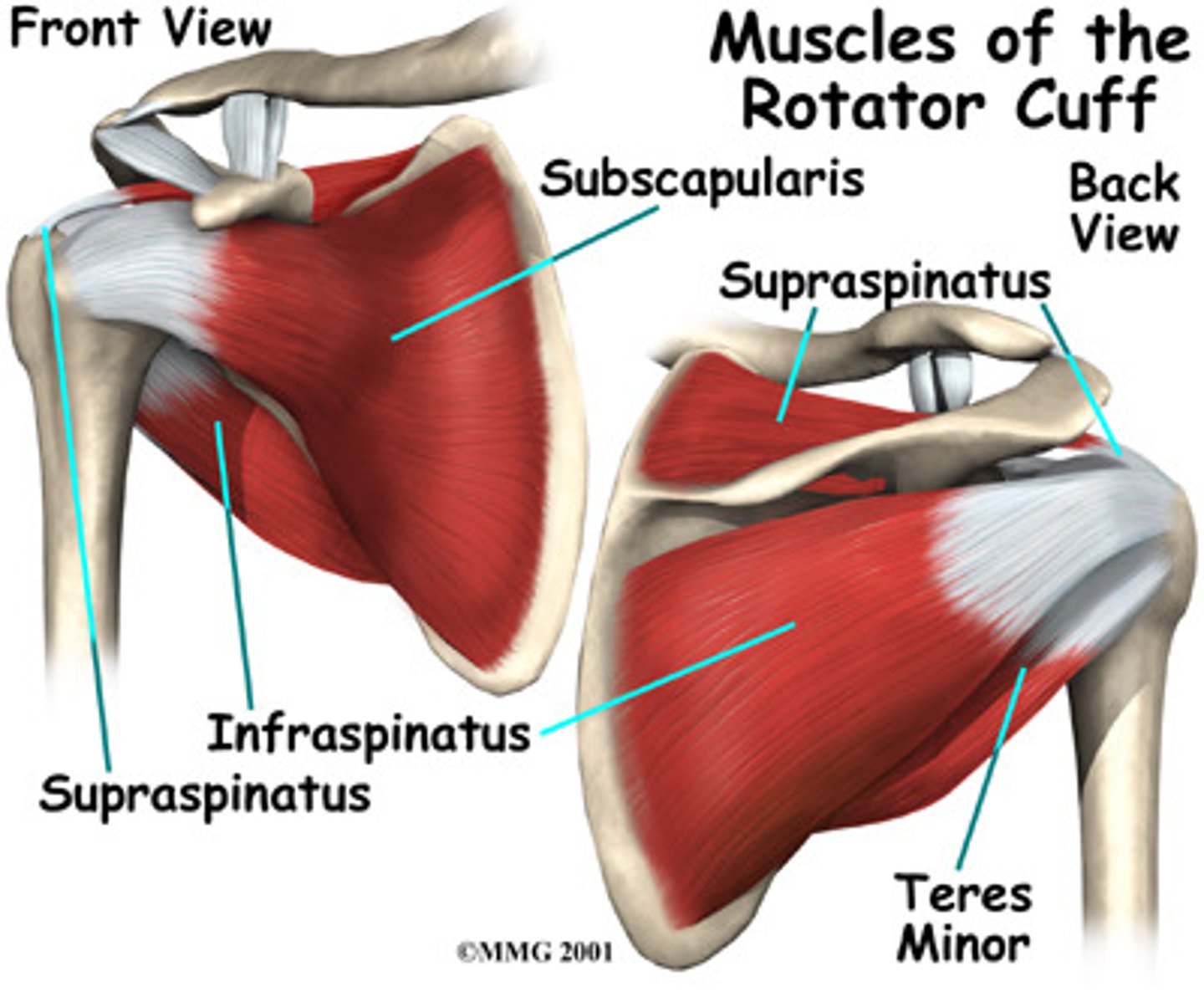
Rotator Cuff
Group of four tendons and the associated muscles which encircle the shoulder joint and merge with the joint capsule. The rotator cuff muscles include the subscapularis, supraspinatus, infraspinatus, and teres minor. Moving the arm vigorously can severely stretch or tear the rotator cuff. Attaches to the scapula and surrounds the head of the humerus. These muscles and tendons work together to provide stability to the shoulder joint, as well as to lift and rotate the arm.
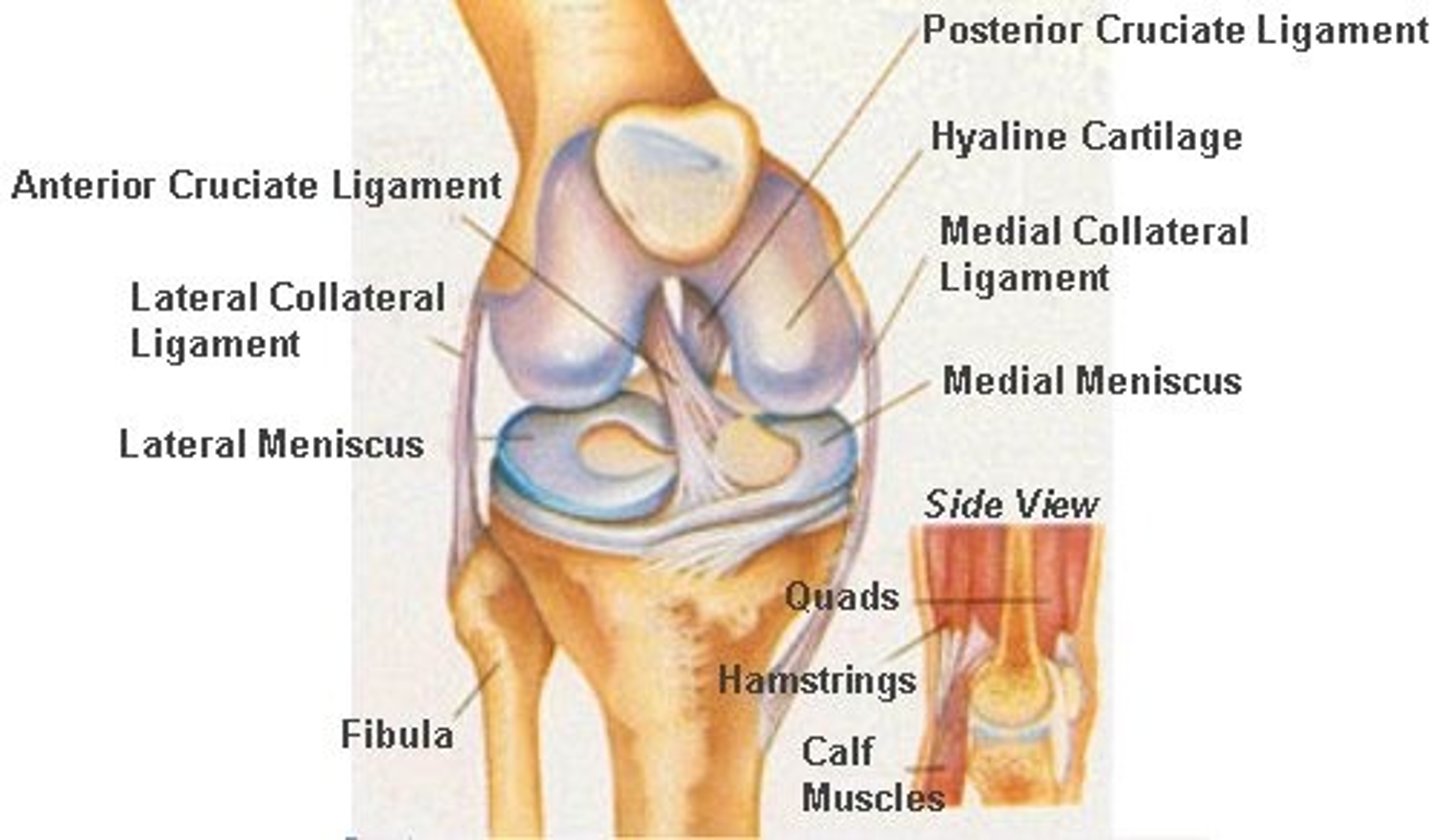
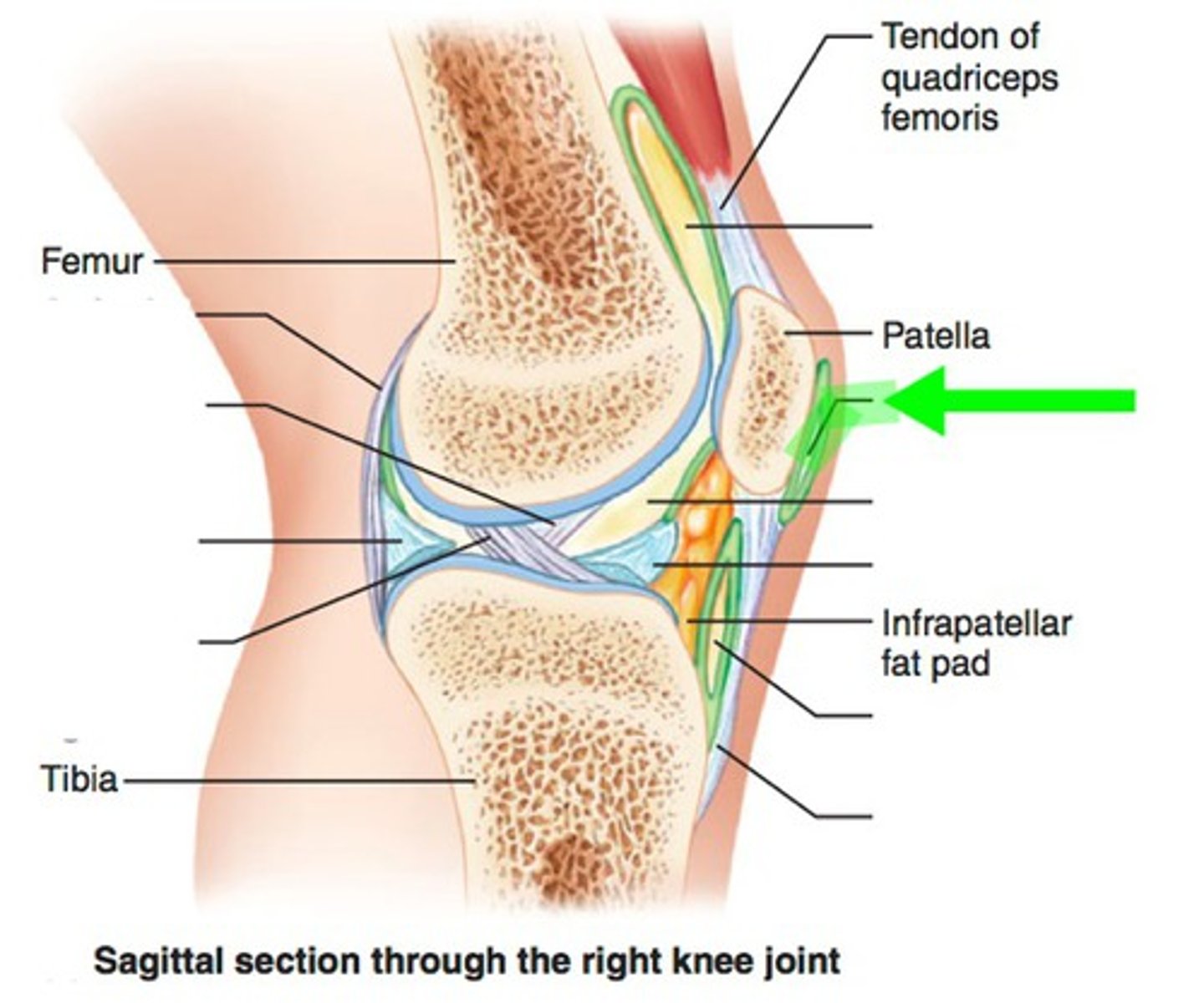
Knee Joint
The knee joint, the largest and most complex joint in the body, primarily acts as a hinge. However, it also permits some medial and lateral rotation when in the flexed position and during the act of leg extension. Structurally, it is compound and bicondyloid, because both the femur and tibia have two condylar surfaces. In this joint, the wheel-shaped condyles of the femur roll along the almost-flat condyles of the tibia like tires on a road. Sharing the knee cavity is an articulation between the patella and the inferior end of the femur; this femoropatellar joint is a plane joint that allows the patella to glide across the distal femur as the knee bends.
Subcutaneous Prepatellar Bursa
A small fluid-filled sac located in front of the patella. The bursa helps to reduce friction between the skin and the patella during movements.
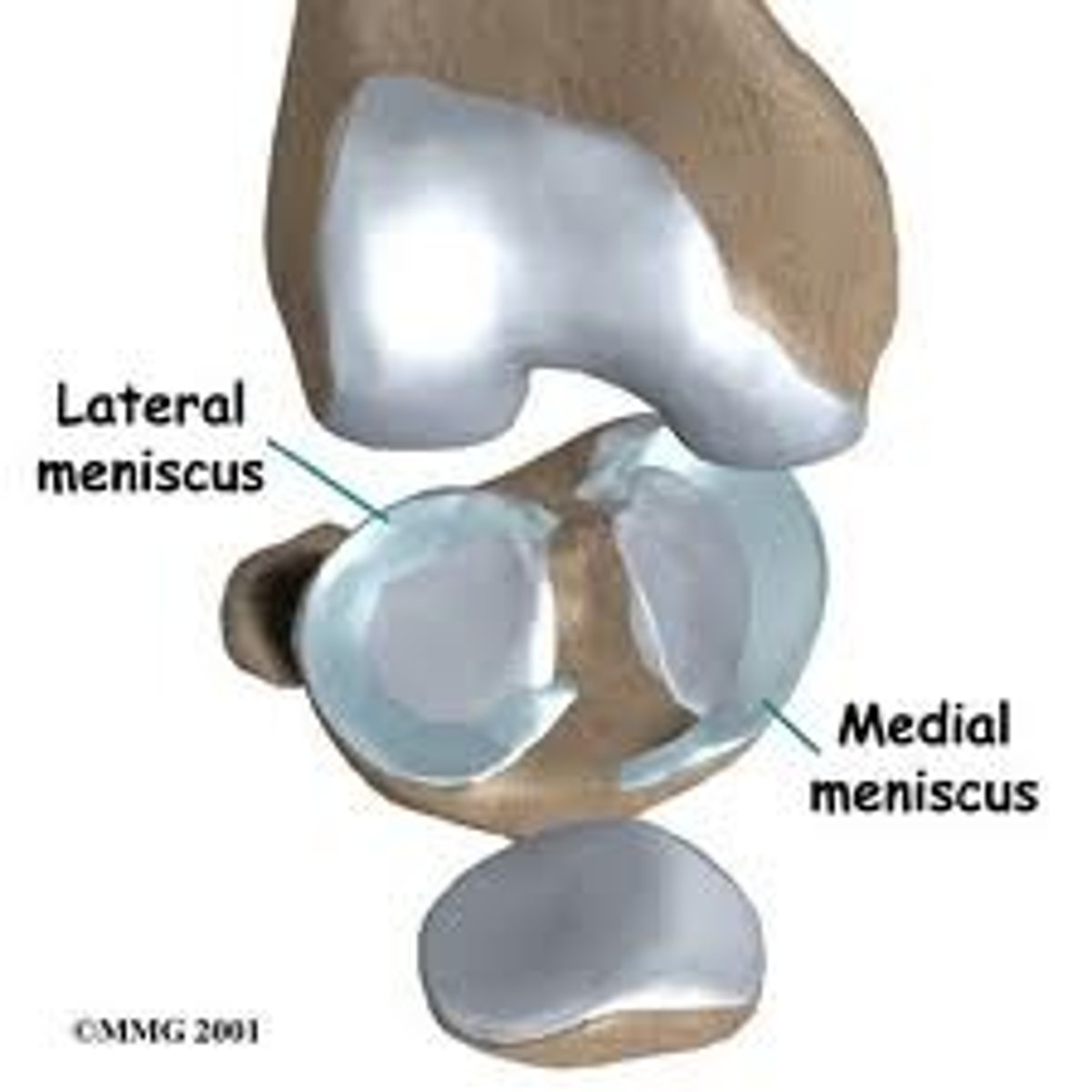
Lateral and Medial Menisci
Crescent-shaped pieces of fibrocartilage located on the tibial plateau. The menisci help to distribute the forces across the knee joint and provide stability to the joint. The medial meniscus is larger and more C-shaped, while the lateral meniscus is more circular. The menisci help to stabilize the joint by guiding the condyles during flexion, extension, and rotation movements and preventing side-to-side rocking of the femur on the tibia.
Patellar Ligament
A continuation of the tendon of the main muscles on the anterior thigh, the quadriceps femoris. The patella ligament connects the patella to the tibia and helps to stabilize the joint during movements.
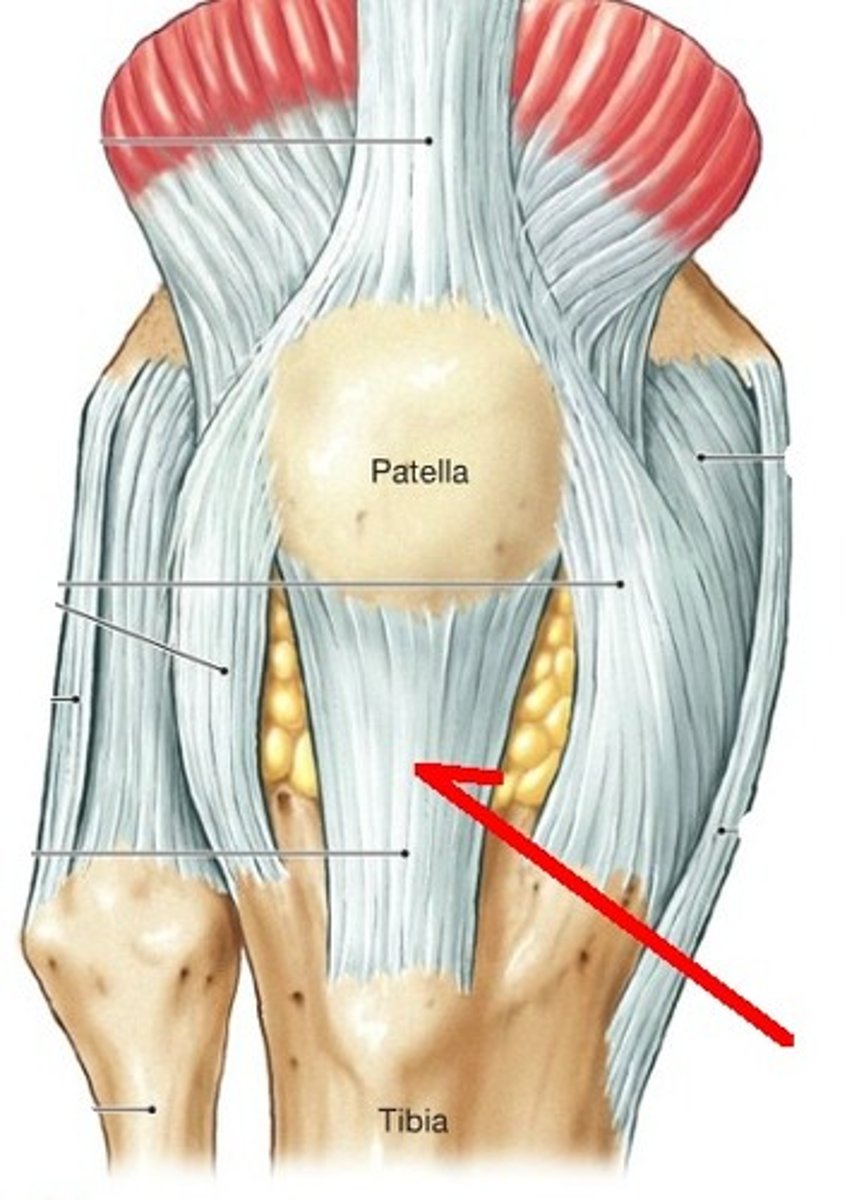
Medial and Lateral Patellar Retinaculum
Bands of connective tissue that anchor the patella (kneecap) to the femur and tibia. The retinaculum on the medial side of the knee is thicker and stronger than the one on the lateral side. Together, they form a sort of "track" for the patella to slide up and down during movements of the knee joint. This helps to ensure proper tracking and stability of the patella during activities such as walking, running, and jumping.
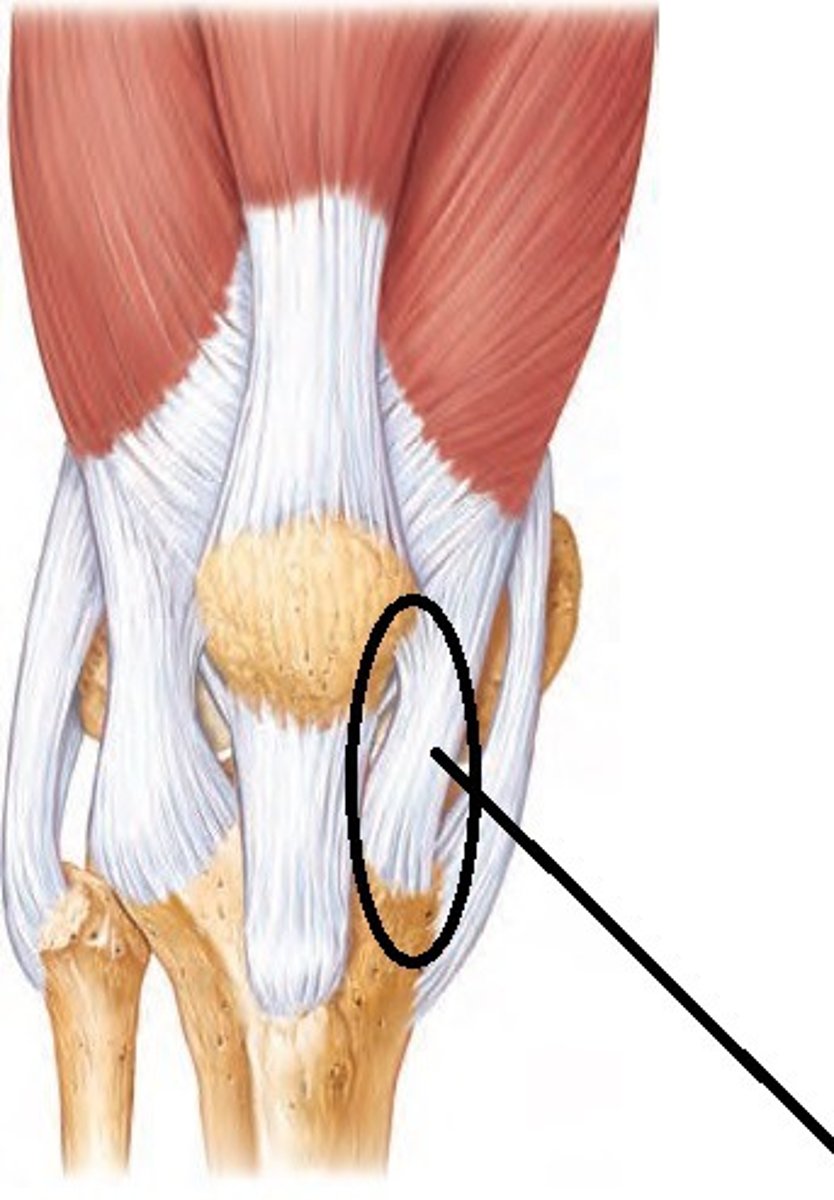
Fibular Collateral Ligament
Extracapsular ligaments located on the lateral side of the joint capsule of the knee, prevents the knee joint from sliding off to the outer side of the body axis. Halts leg extension, prevent hyperextension, and prevents the leg from moving laterally and medially at the knee.

Tibial Collateral Ligament
Extracapsular ligaments located on the medial side of the joint capsule of the knee. The tibial collateral ligament runs from the medial epicondyle of the femur to the medial condyle of the tibia. Halts leg extension, prevent hyperextension, and prevents the leg from moving laterally and medially at the knee.

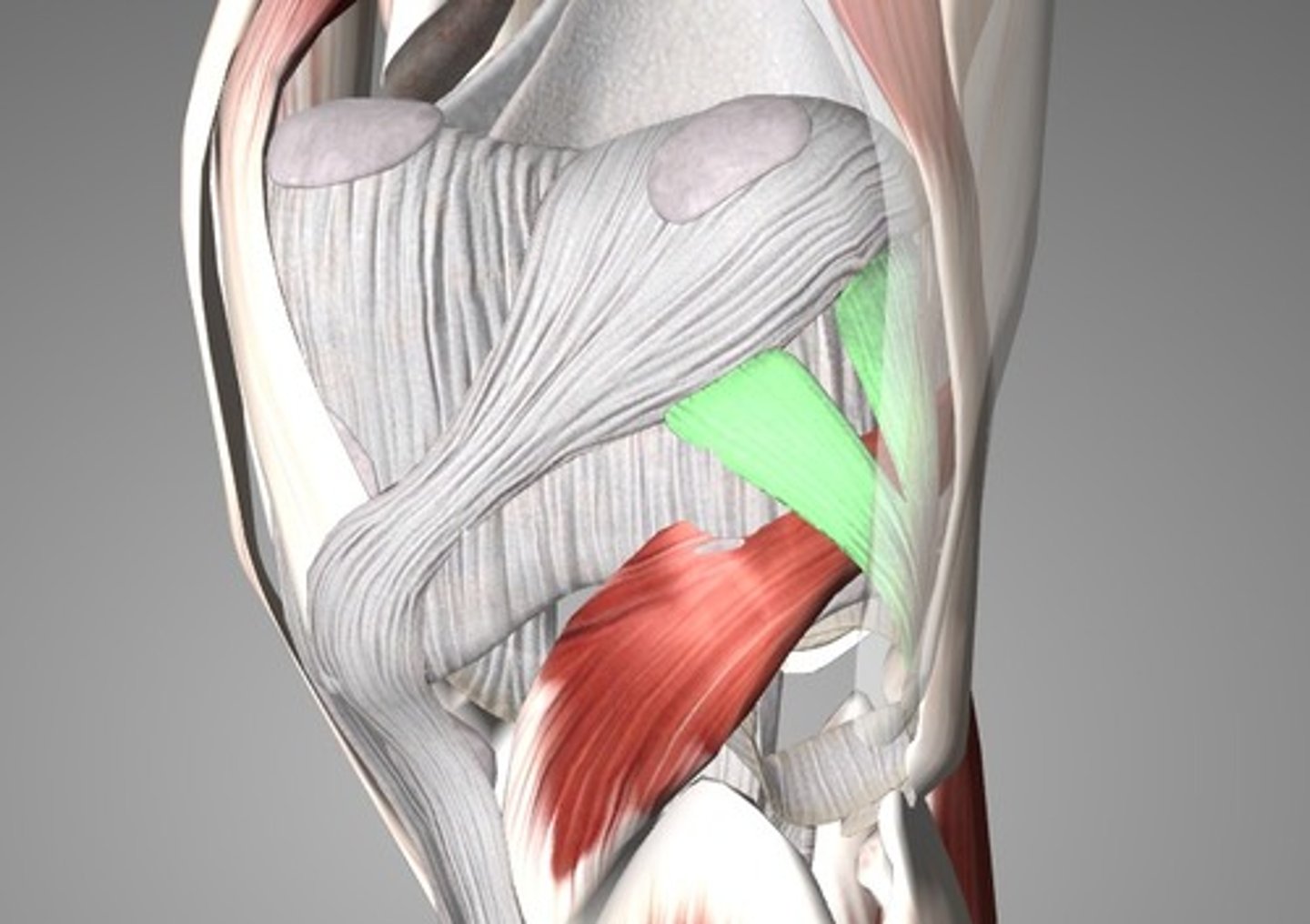
Oblique Popliteal Ligament
Crosses the posterior aspect of the capsule. It is a part of the tendon of the semimembranosus muscle that fuses with the joint capsule and helps stabilize the joint. Provide additional stability to the posterior aspect of the knee joint
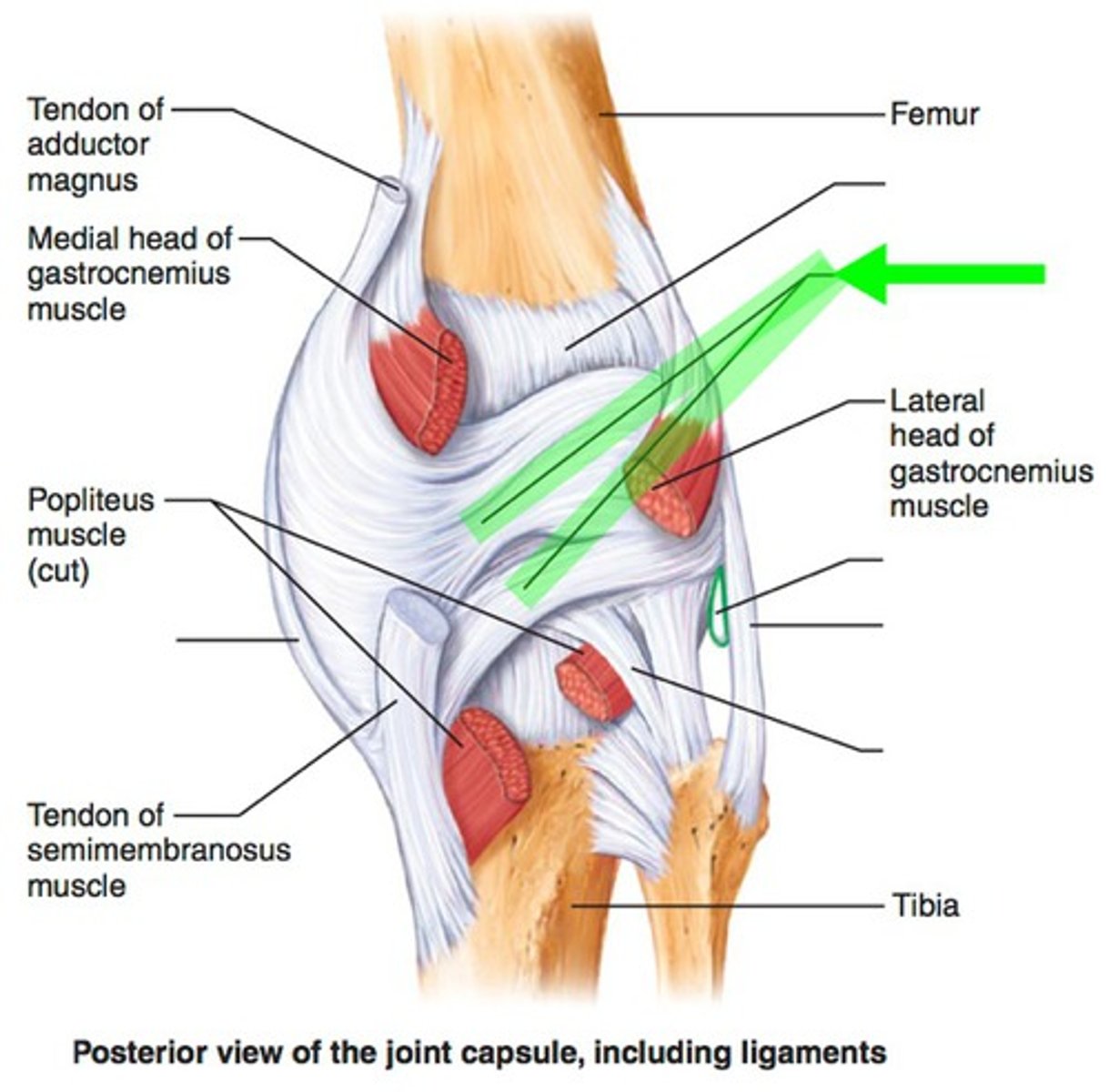
Arcuate Popliteal Ligament
Arcs superiorly from the head of the fibula over the popliteus muscle to the posterior aspect of the joint capsule. Provide additional stability to the posterior aspect of the knee joint
Anterior Cruciate Ligament
Attaches to the anterior part of the tibia, in the intercondylar area. From there, it passes posteriorly to attach to the femur on the medial side of the lateral condyle. The ACL prevents anterior displacement of the tibia on the femur and provides rotational stability to the joint.

Posterior Cruciate Ligament
Arises from the posterior intercondylar area of the tibia and passes anteriorly to attach to the femur on the lateral side of the medial condyle. The PCL prevents posterior displacement of the tibia on the femur and provides stability during flexion of the knee joint.

Contractility
Muscle tissue contracts forcefully. Muscle cells contain myofilaments, specific types of microfilaments that are responsible for the shortening of muscle cells. There are two kinds of myofilaments, one containing the protein actin and the other containing the protein myosin. These two proteins generate contractile force in every cell in the body. This contractile property is most highly developed in muscle cells.
Excitability
Nerve signals or other stimuli excite muscle cells, causing electrical impulses to travel along the cells' plasma membrane. These impulses initiate contraction in muscle cells.
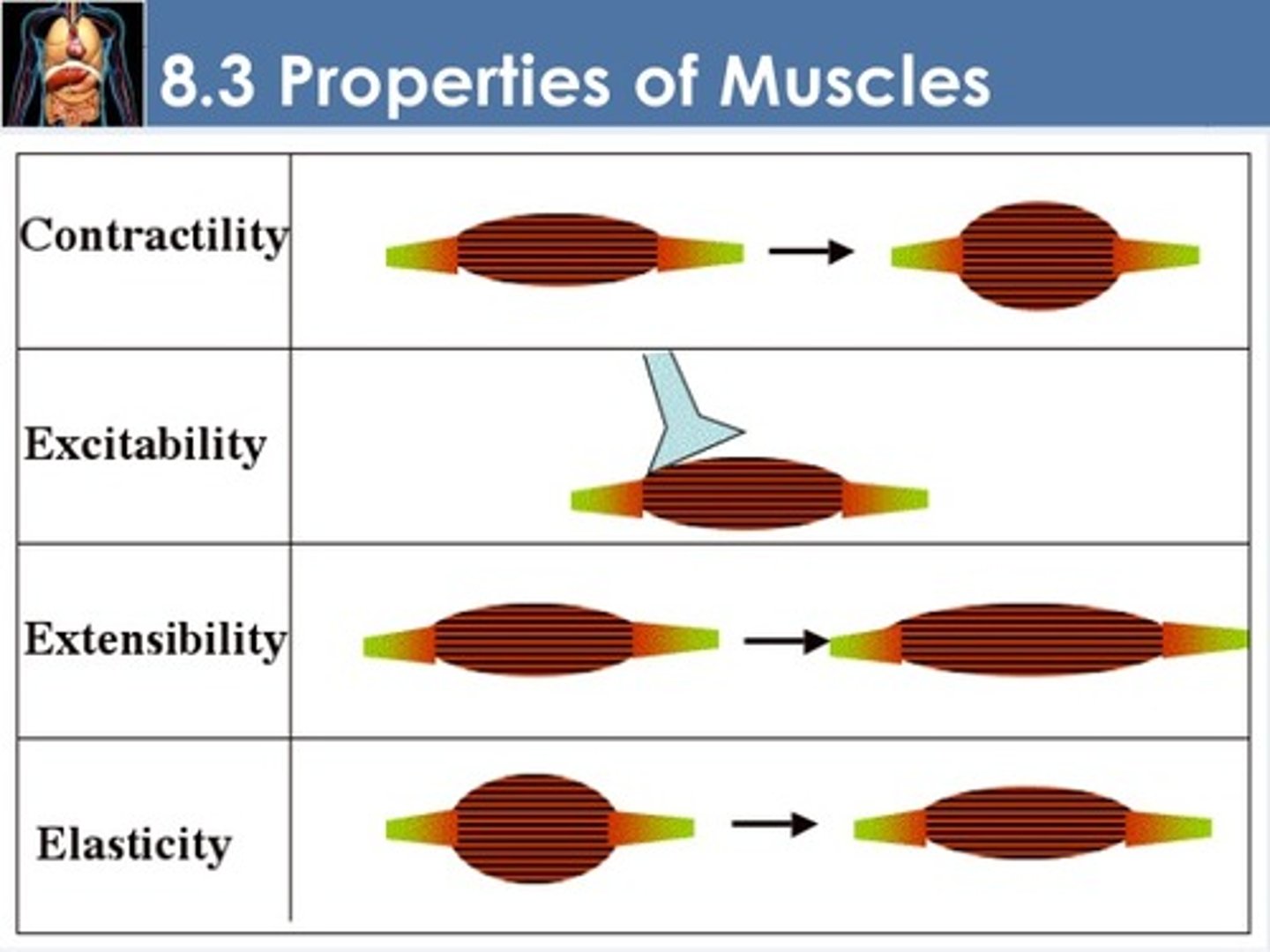
Extensibility
Muscle tissue can be stretched. Contraction of one skeletal muscle will stretch an opposing muscle. The muscular wall of a hollow organ is stretched by the substances contained within that organ—a bolus of food in the digestive tract or urine in the urinary bladder, for example.
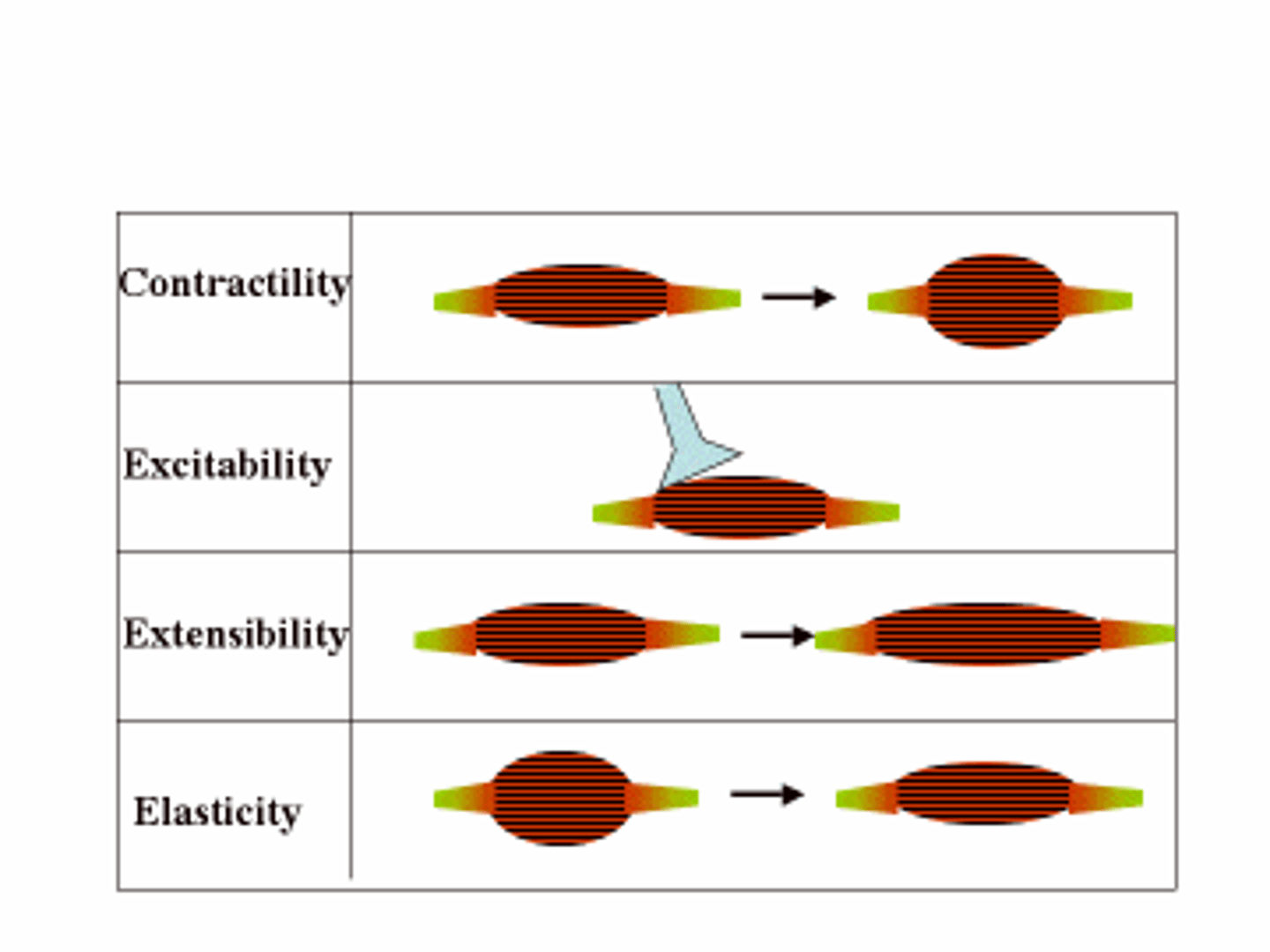
Elasticity
After being stretched, muscle tissue recoils passively and resumes its resting length.
Four Functions of Muscle Tissue
Produce Movement
- contraction of multiple muscles in the legs helps you raise the feet and thrust the hip to move the body forward.
Open and Close Body Passageways
- Muscle fibers in the iris of the eye constrict and relax to change pupil diameter
Maintain Posture and Stabilize Joints
- Muscle tone, the constant low-level contraction of muscles, helps stabilize and strengthen many synovial joints.
Generate Heat
- Excess heat generated during exercise stimulates sweating to cool us down
Two Characteristics of Different Muscle Types
(1) the presence or absence of light and dark stripes, called striations, in the muscle cells
(2) whether control of contraction is voluntary or involuntary
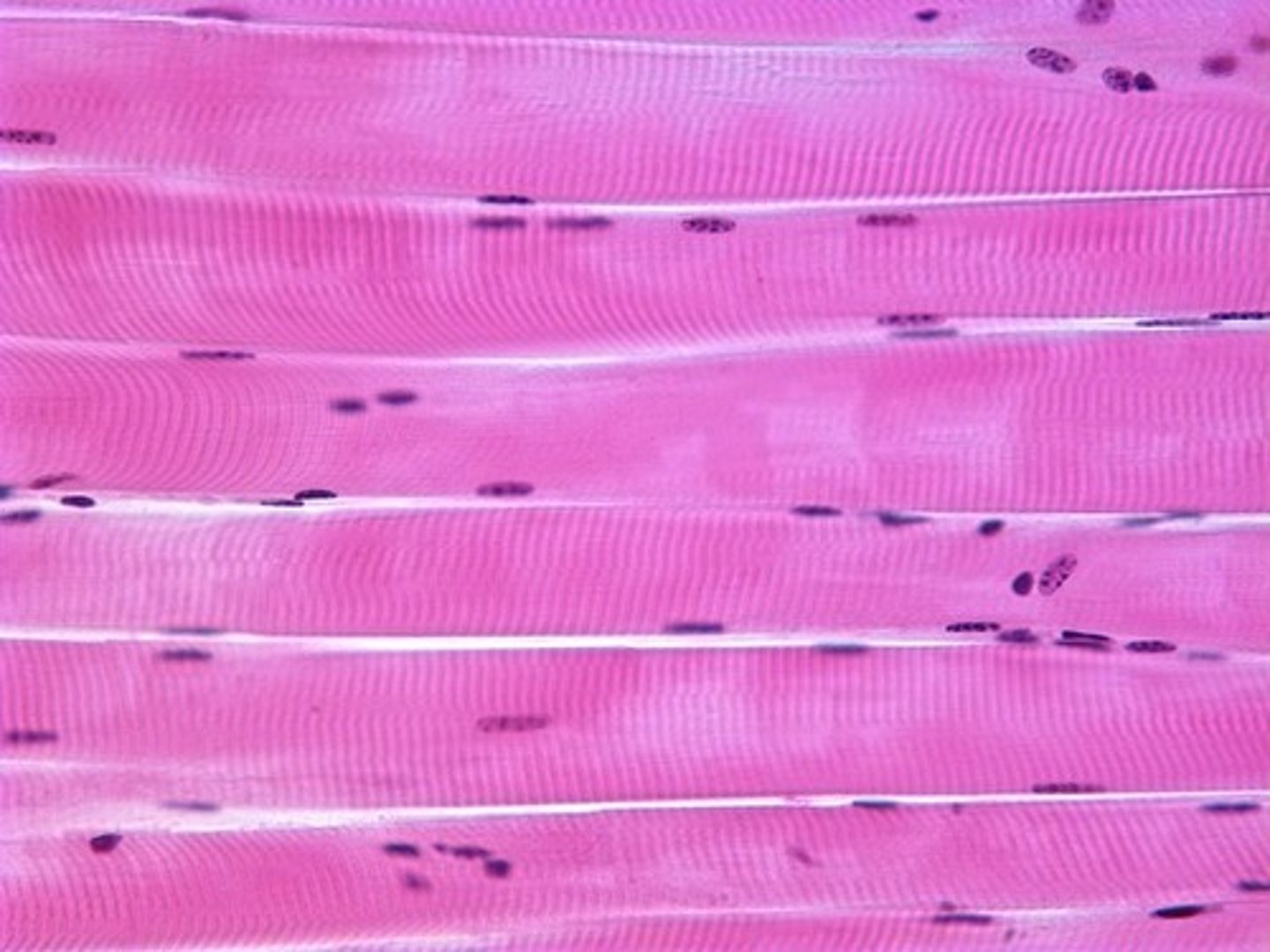
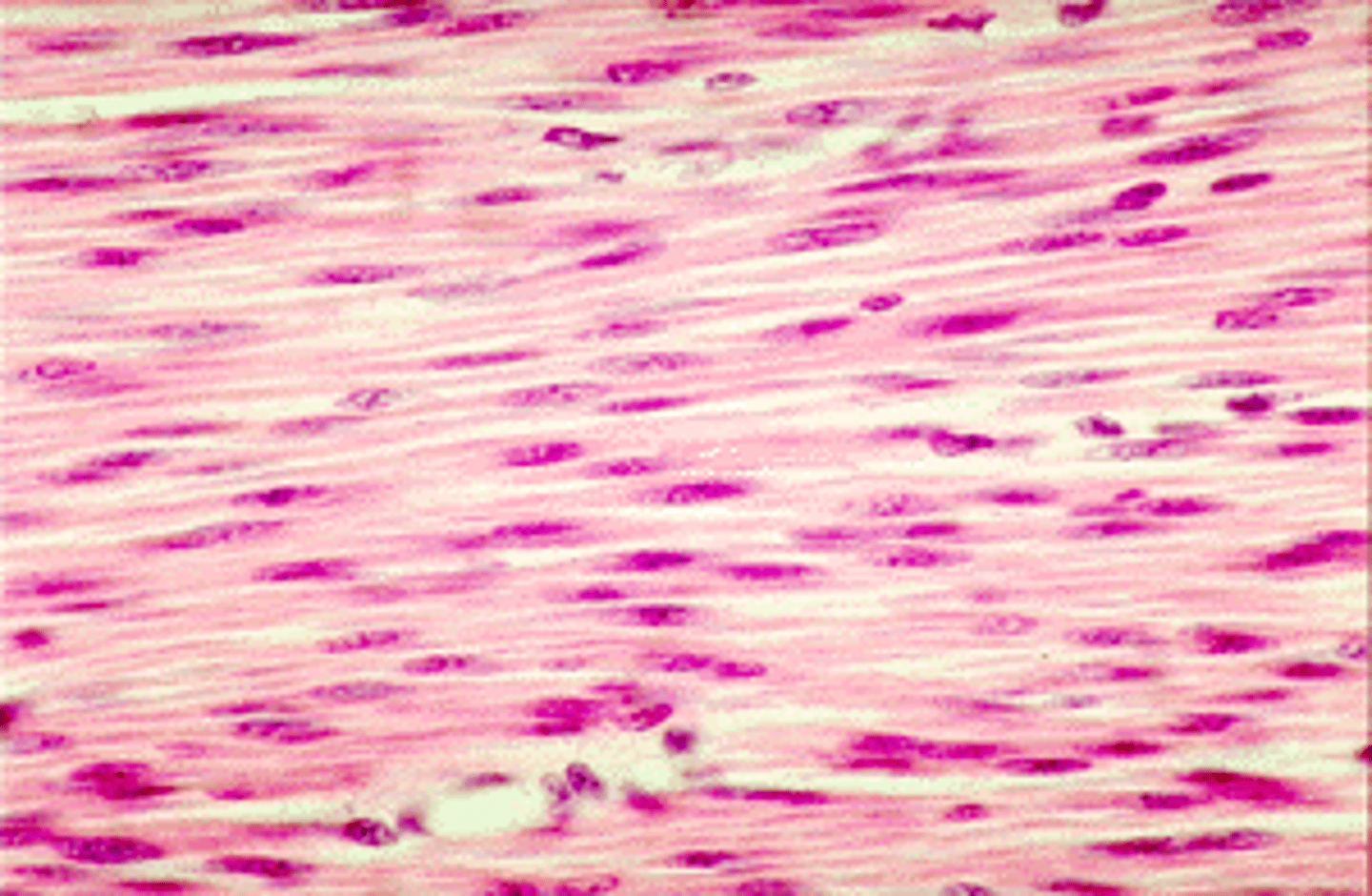
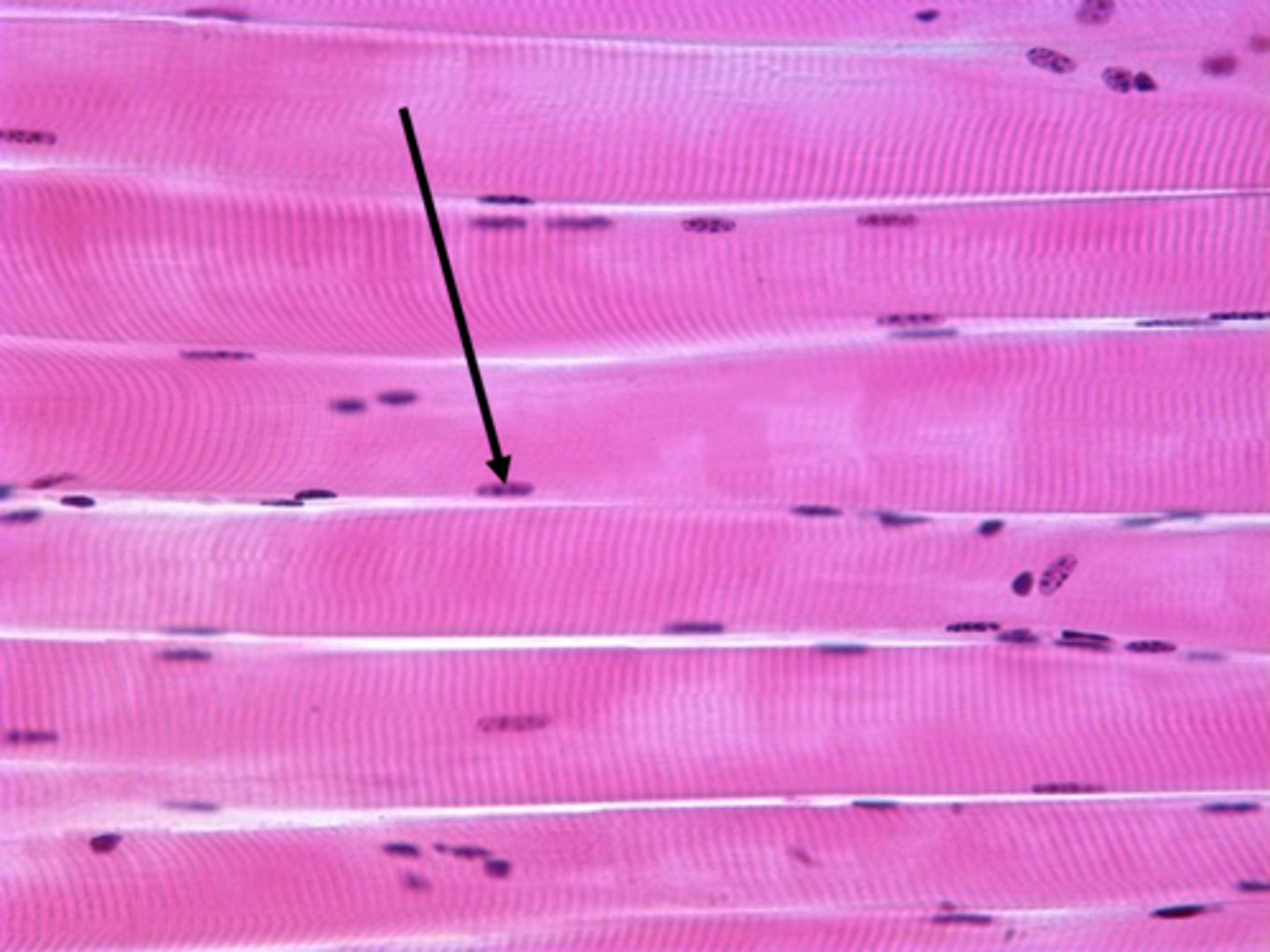
Skeletal Muscle
The muscle cells of skeletal muscle tissue are striated muscle. Discrete organs that attach to and move the skeleton. The elongated, cylindrical skeletal muscle cells are called muscle fibers. Skeletal muscle is innervated by the voluntary division of the nervous system and is subject to conscious control; you can control this muscle tissue at will.
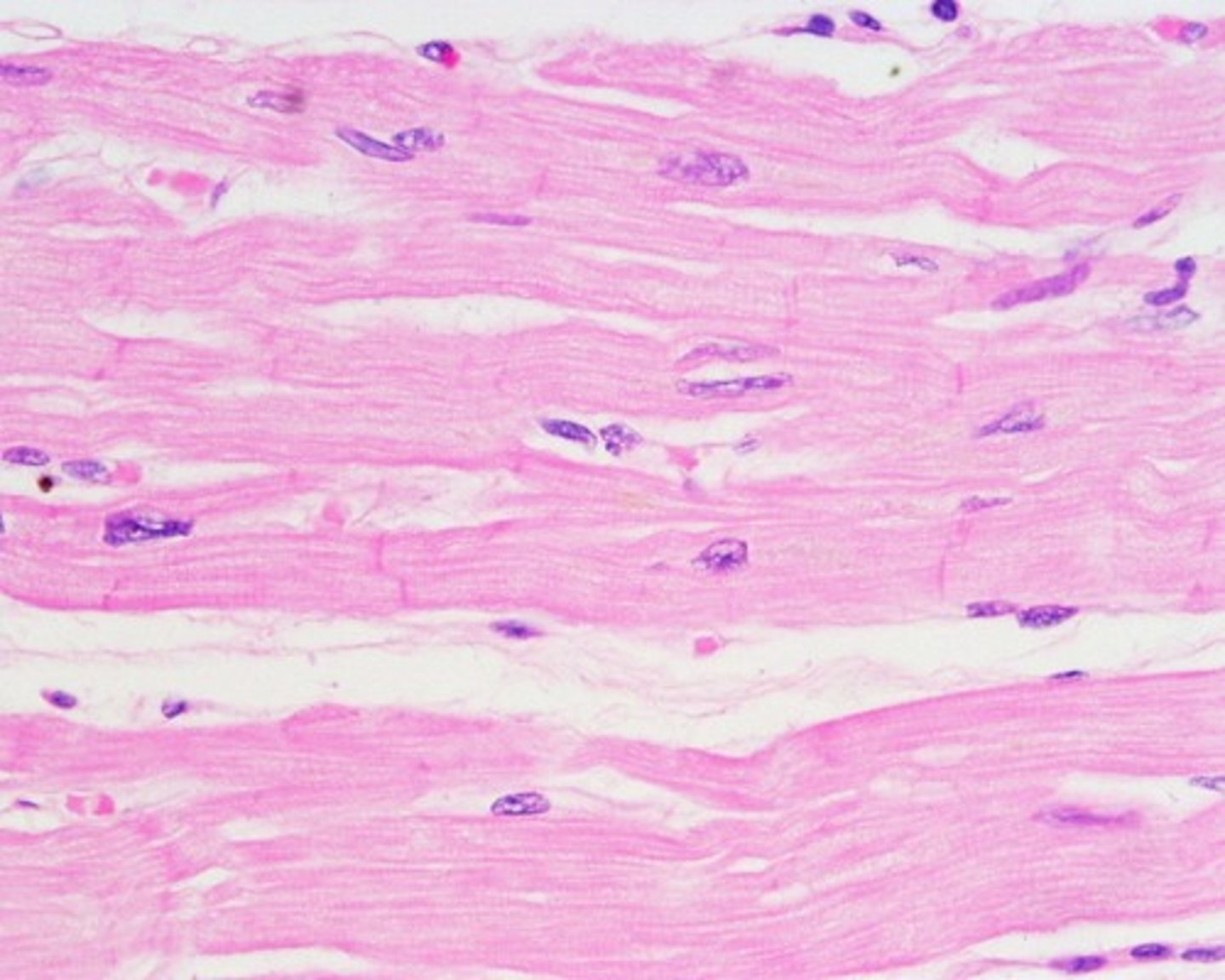
Cardiac Muscle
Cardiac muscle tissue occurs only in the wall of the heart. The muscle cells of cardiac muscle are striated muscle, but its contraction is involuntary. Cardiac muscle can contract with no nervous stimulation. The involuntary division of the nervous system regulates contraction of cardiac muscle tissue; we have no direct, conscious control over how fast our heart beats. visceral muscle, a term reflecting the fact that both occur in the visceral organs and are innervated by the involuntary division of the nervous system.
Smooth Muscle
Most smooth muscle tissue in the body is found in the walls of hollow internal organs other than the heart, such as the stomach, urinary bladder, blood vessels, and respiratory tubes. The muscle cells of smooth muscle lack striations. Like skeletal muscle, these cells are elongated and referred to as muscle fibers. As with cardiac muscle, the involuntary division of the nervous system innervates smooth muscle. visceral muscle, a term reflecting the fact that both occur in the visceral organs and are innervated by the involuntary division of the nervous system.
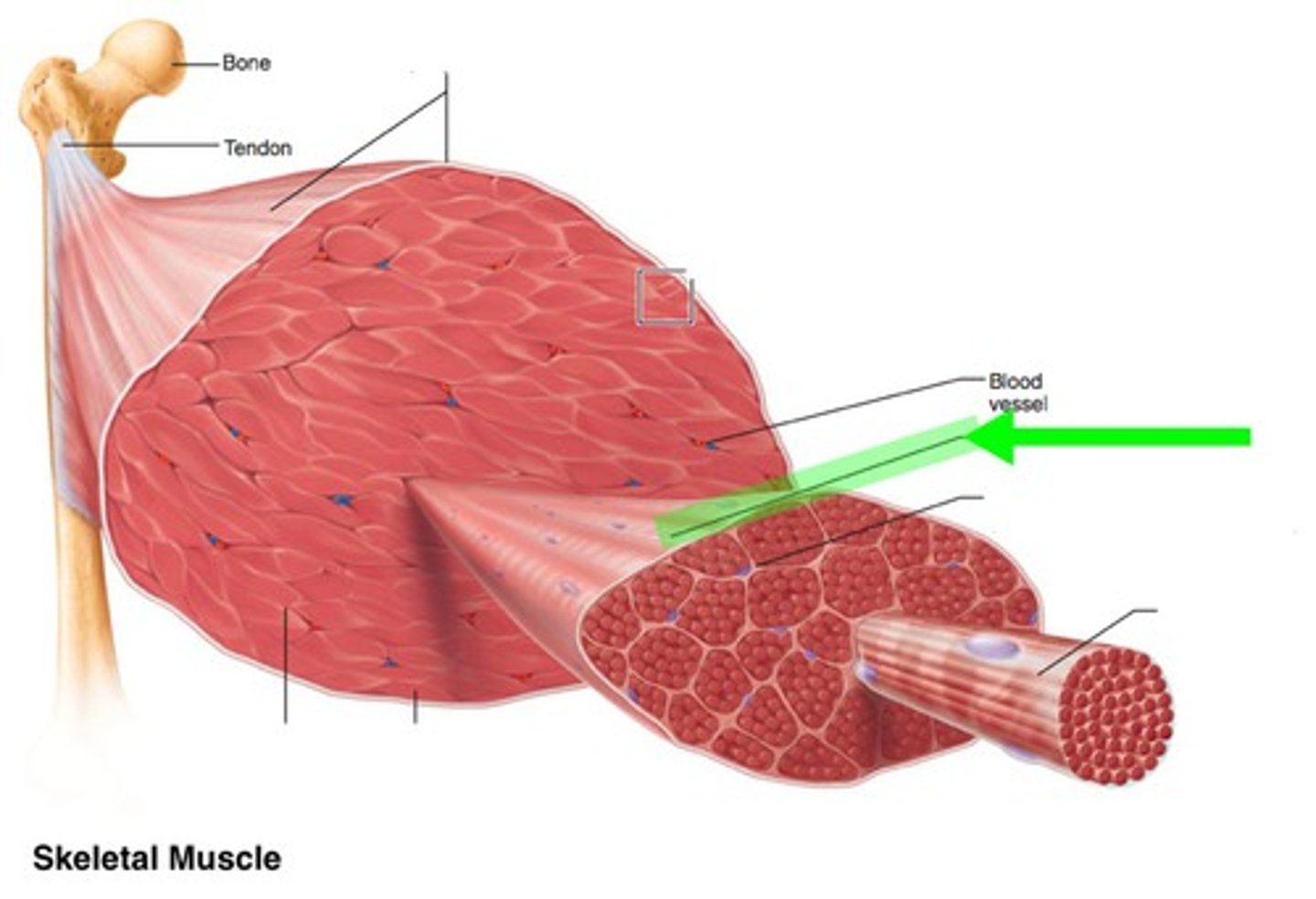
Tissues That Make Up Skeletal Muscles
Skeletal muscle tissue, connective tissue, blood vessels, and nerves.
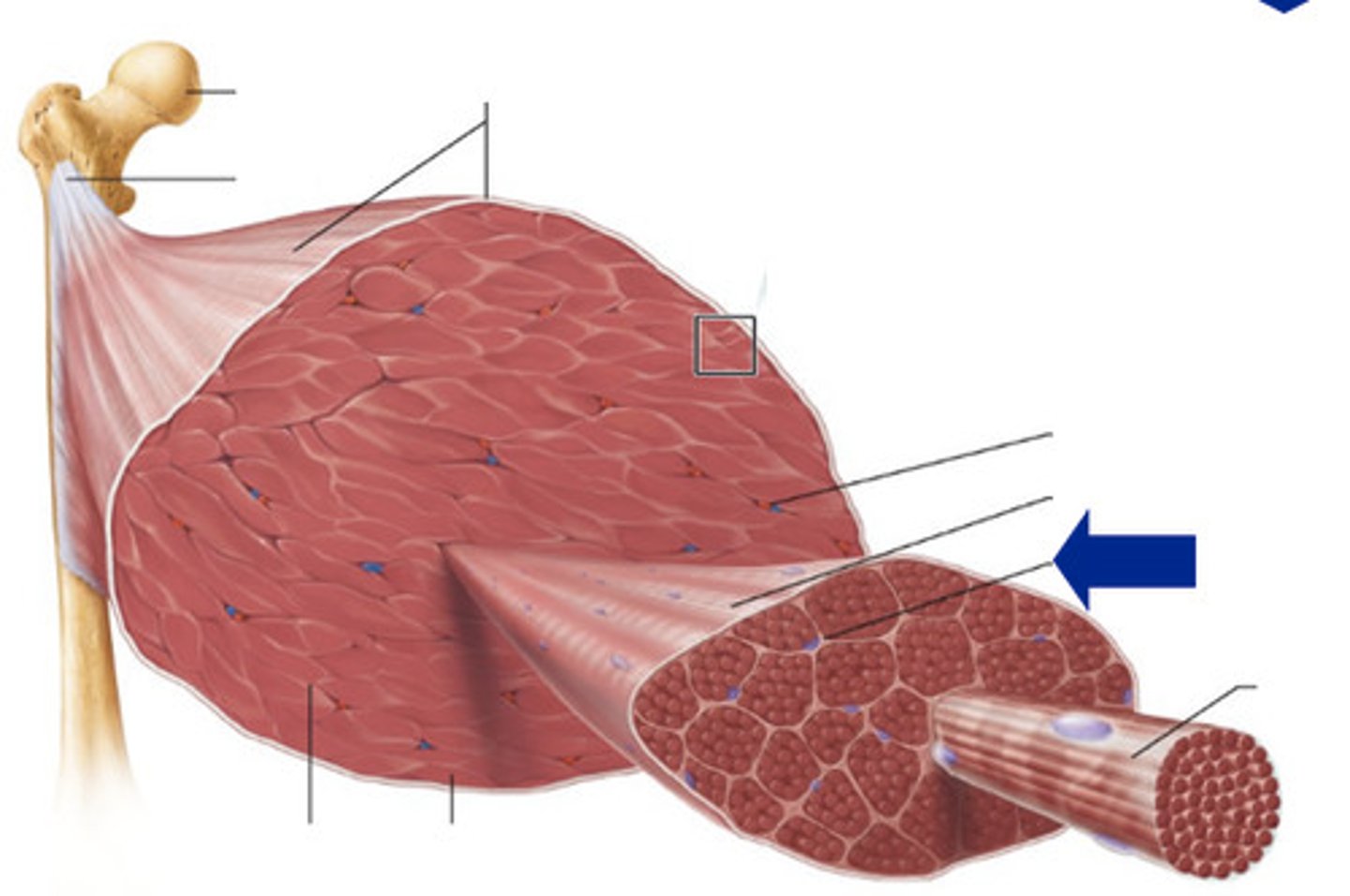
Connective Tissue Sheaths of Skeletal Muscles
These fibrous connective tissues bind muscle fibers together and hold them in parallel alignment so they can work together to produce force. These sheaths are continuous with each other: The endomysium merges with the perimysium, which in turn is continuous with the epimysium.
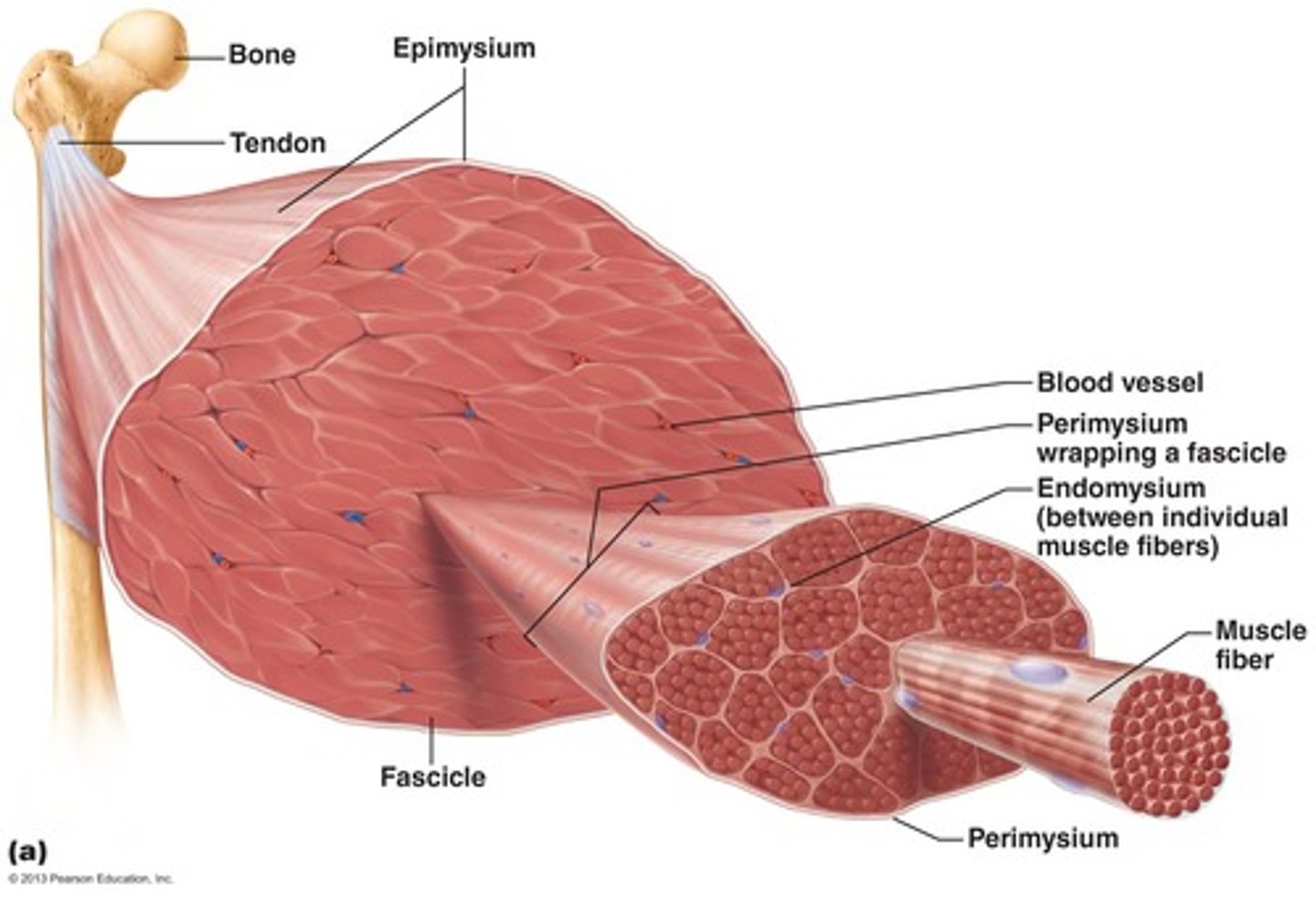
Epimysium
Outer layer of dense, irregular connective tissue
Surrounds the whole skeletal muscle.
Sometimes the epimysium blends with the deep fascia that lies between neighboring muscles
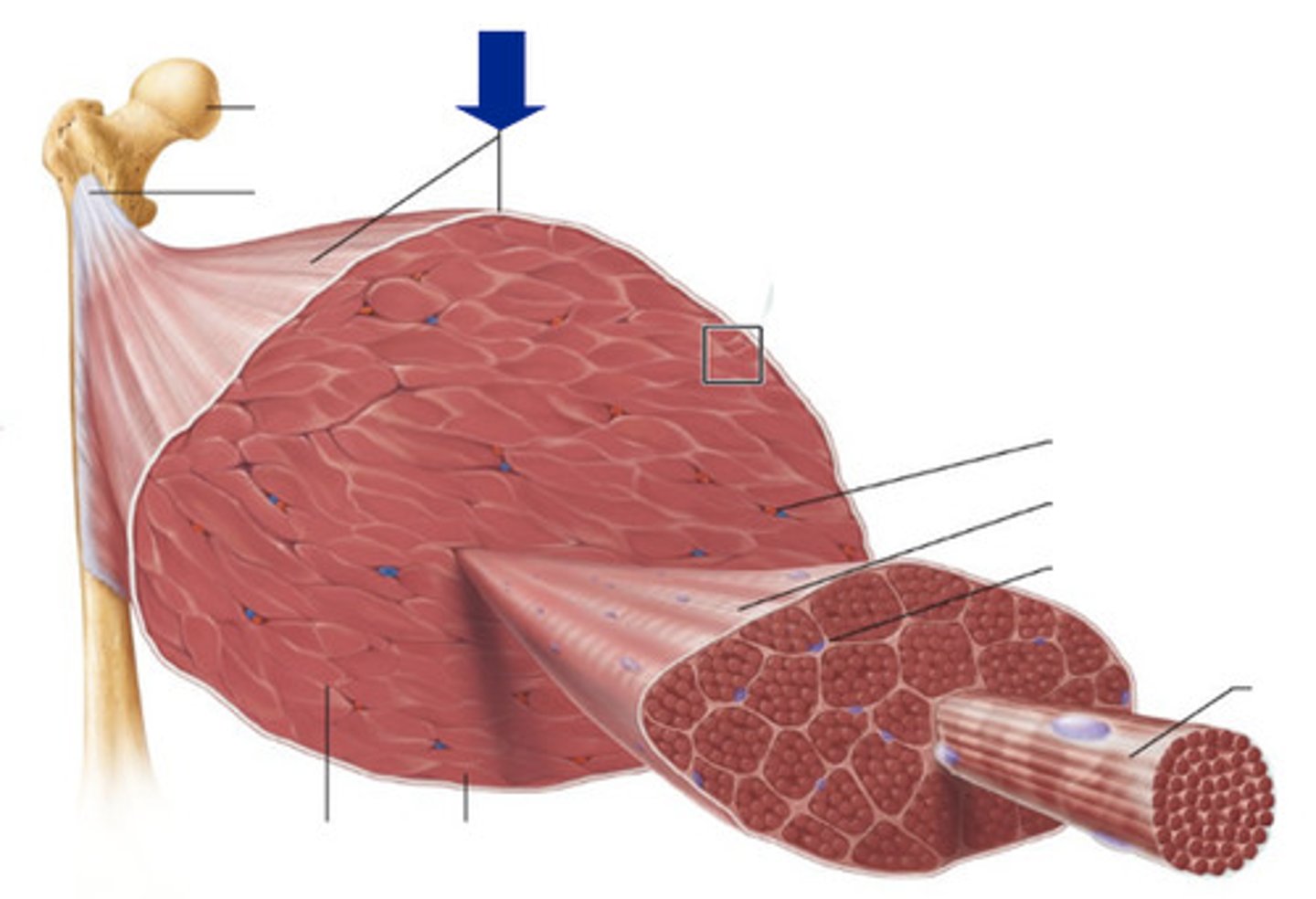
Perimysium
A layer of fibrous connective tissue surrounding each fascicle
Fasicles are groups of separated muscle fibers that resemble a bundle of sticks
Endomysium
Within a fascicle, each muscle fiber is surrounded by a fine sheath of loose connective tissue consisting mostly of reticular fibers
Tendon
All three sheaths (epimysium, perimysium, and endomysium) converge to form a tendon, the connective tissue structure that joins skeletal muscles to bones. When muscle fibers contract, they pull on the surrounding endomysium. Because of the continuity between sheaths, this pull is then exerted on the perimysium, epimysium, and tendon, a sequence that transmits the force of contraction to the bone being moved. The sheaths also provide a muscle with much of its natural elasticity and carry the blood vessels and nerves that serve the muscle fibers.
How does a muscle attach to a bone?
A muscle attaches to a bone through tendons. The tendons attach muscle to bone by fusing the collagen fibers of the tendon with the periosteum, the tough outer layer of the bone. A muscle attachment is the location on a bone where a muscle connects to the bone. Each skeletal muscle extends from one bone to another, crossing at least one movable joint. When the muscle contracts, it causes one of the bones to move while the other bone usually remains fixed.
What is the difference between an origin and an insertion?
The attachment of the muscle on the less movable bone is called the origin of the muscle, whereas the attachment on the more movable bone is called the muscle's insertion. Thus, when the muscle contracts, its insertion is pulled toward its origin. In the muscles of the limbs, the origin is by convention the more proximal attachment of the muscle, and the insertion is the more distal attachment. The functions of the origin and the insertion may switch, depending on body position and the movement produced when the muscle contracts.
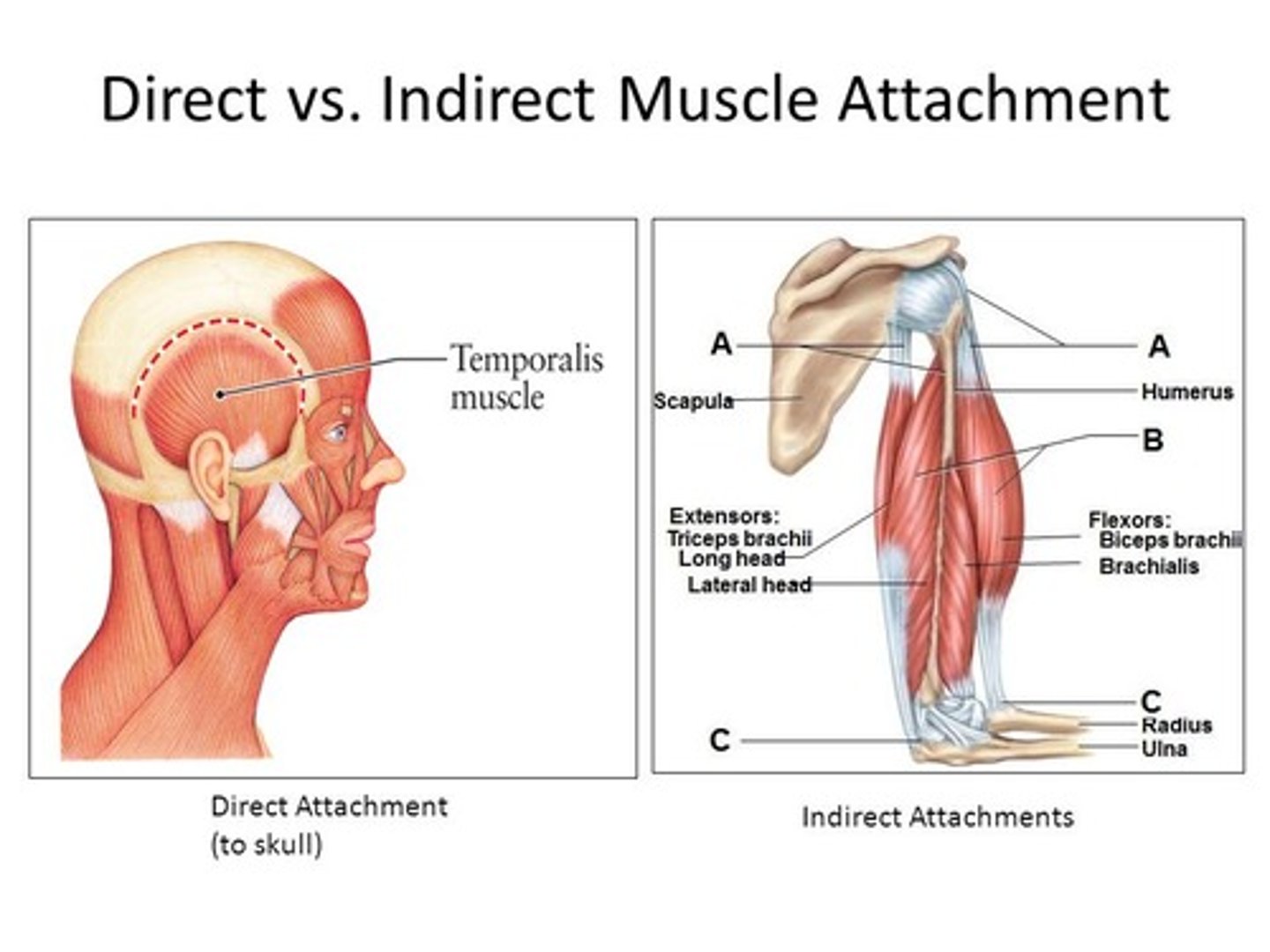
Indirect vs Direct Attachment
Muscles attach to their origins and insertions via strong fibrous connective tissues that extend into the fibrous periosteum of the bone. In direct, or fleshy, attachments, the attaching strands of connective tissue are so short that the muscle fascicles themselves appear to attach directly to the bone. In indirect attachments, the connective tissue extends well beyond the end of the muscle fibers to form either a cordlike tendon or a flat sheet called an aponeurosis.
Indirect attachments are more common than direct attachments, and most muscles have tendons. Raised bone markings are often present where tendons meet bones. These markings include tubercles, trochanters, and crests. Although most tendons and aponeuroses attach to bones, a few attach to skin, to cartilage, or to a raphe.
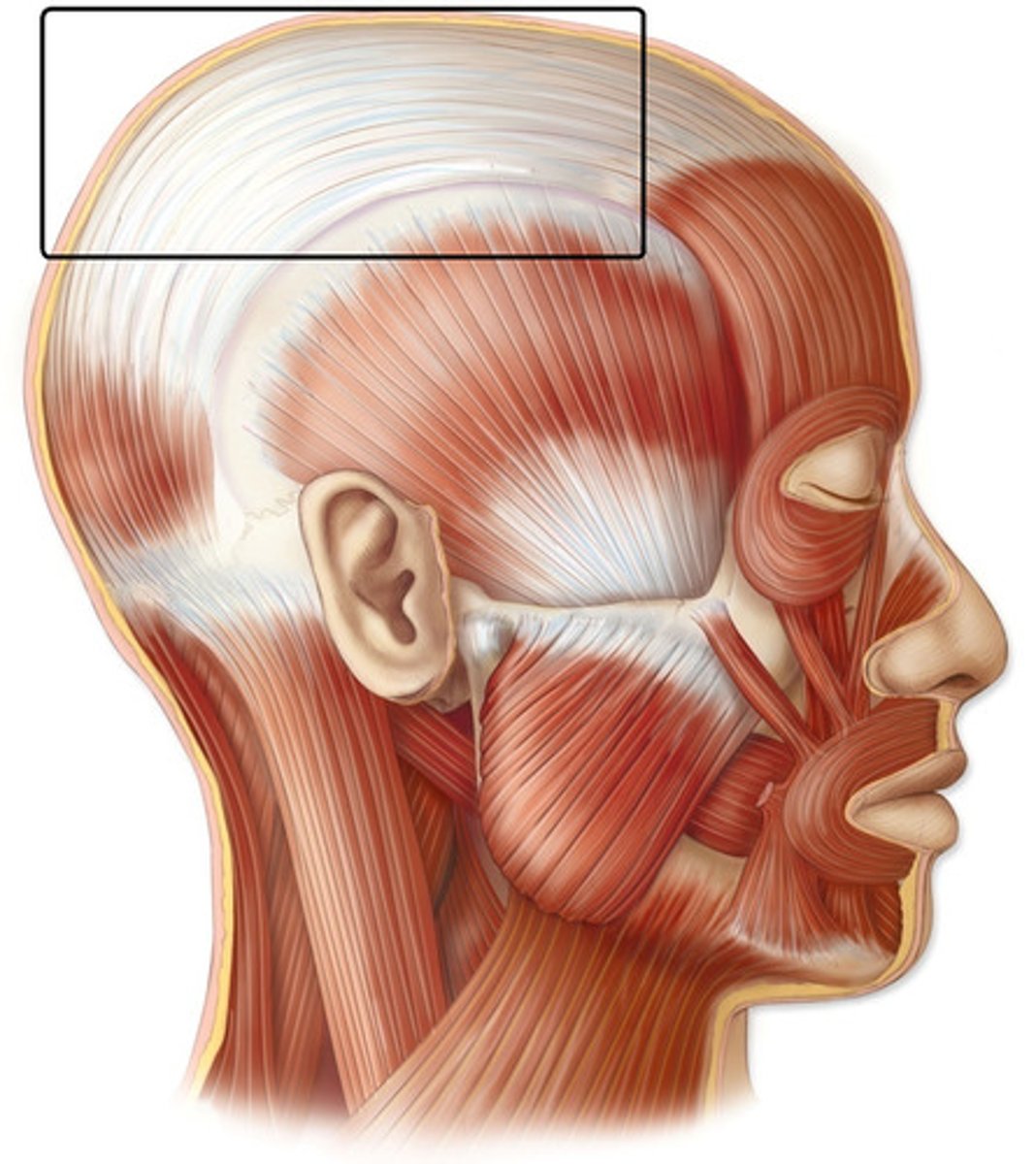
Aponeurosis
A cordlike tendon or a flat sheet.
Raphe
A seam of fibrous tissue.
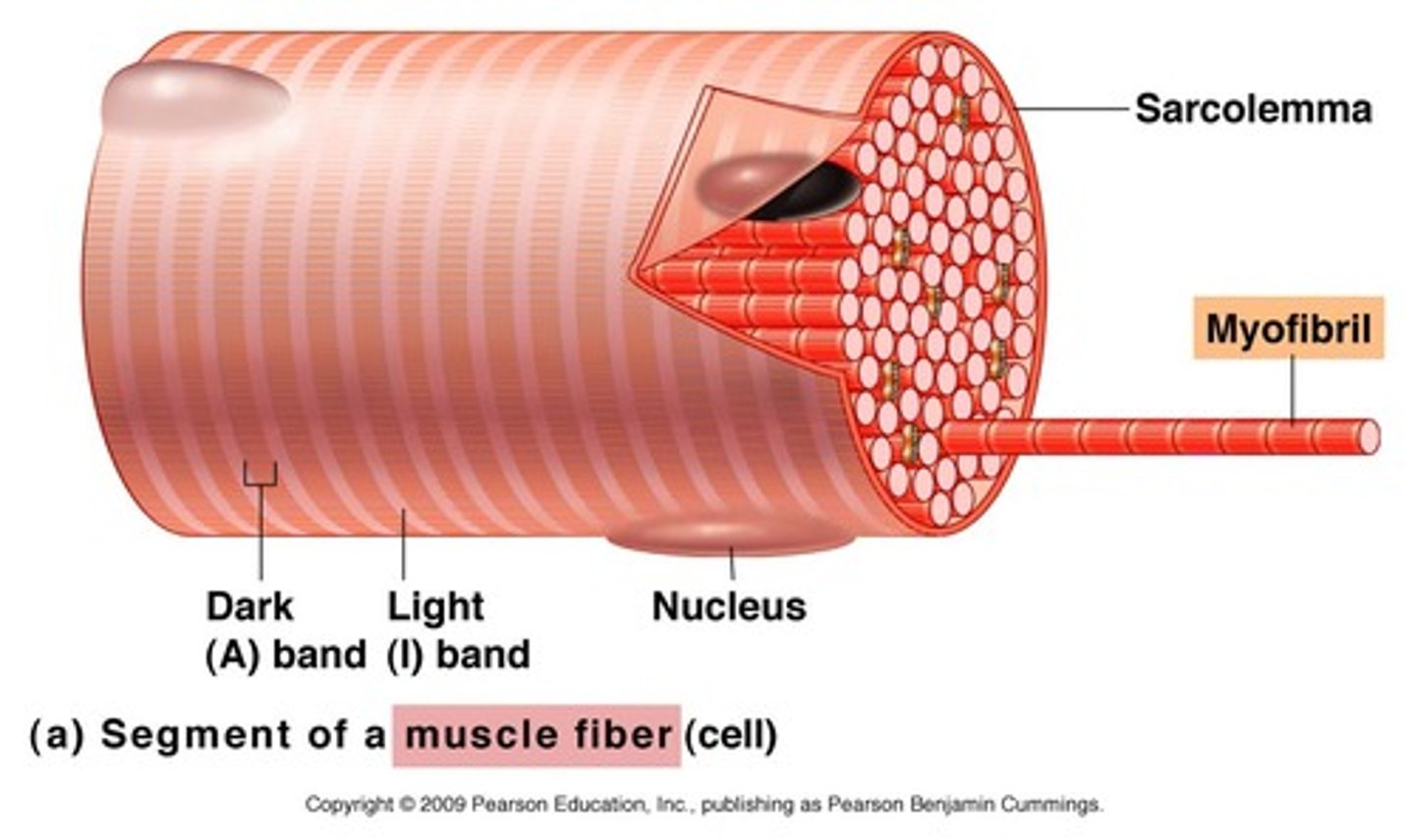
Skeletal Muscle Fiber
Striated appearance: Skeletal muscle fibers have a banded or striped appearance due to the arrangement of contractile proteins called actin and myosin within the sarcomeres of the muscle fiber.
Multiple nuclei: Unlike most cells in the body, skeletal muscle fibers are multinucleated, meaning they contain multiple nuclei within a single cell.
Sarcoplasmic reticulum: Skeletal muscle fibers have a specialized endoplasmic reticulum called the sarcoplasmic reticulum, which stores and releases calcium ions required for muscle contraction.
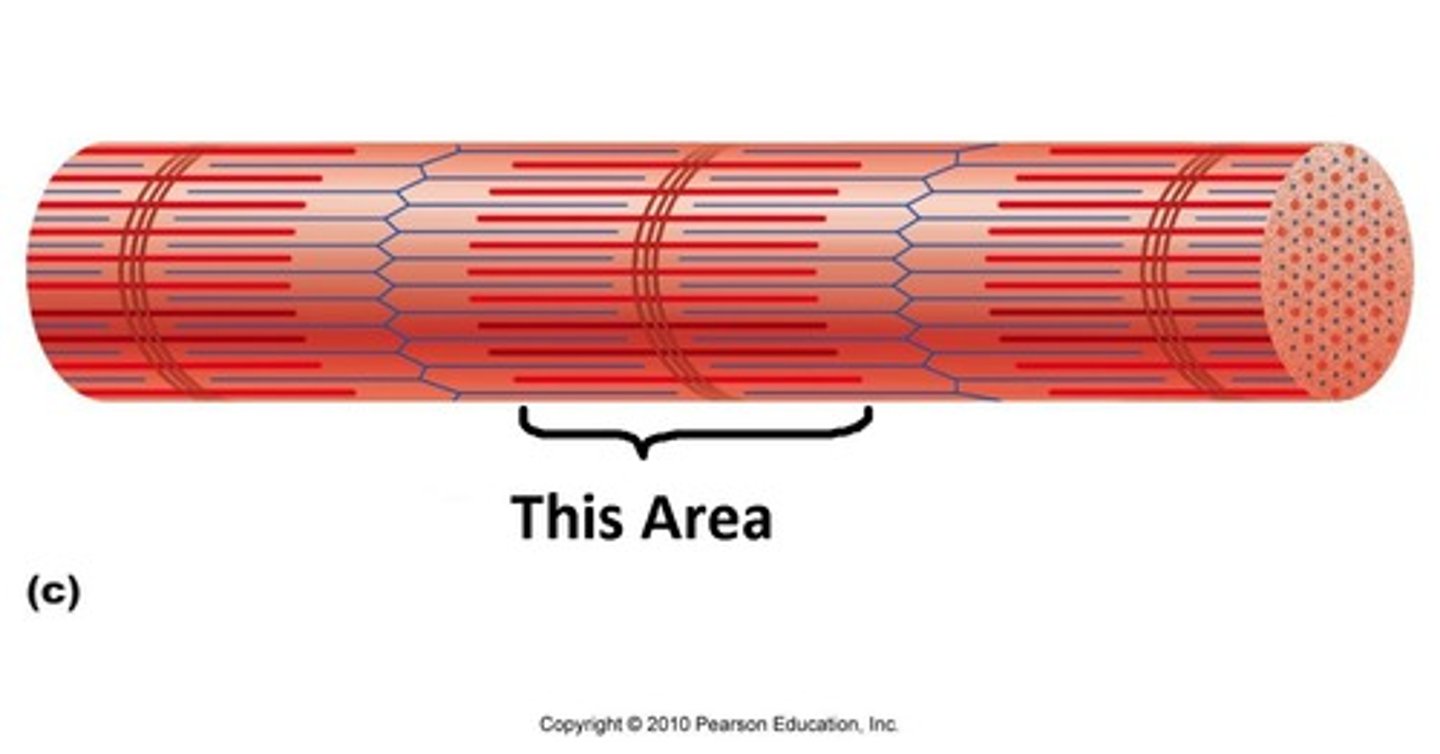
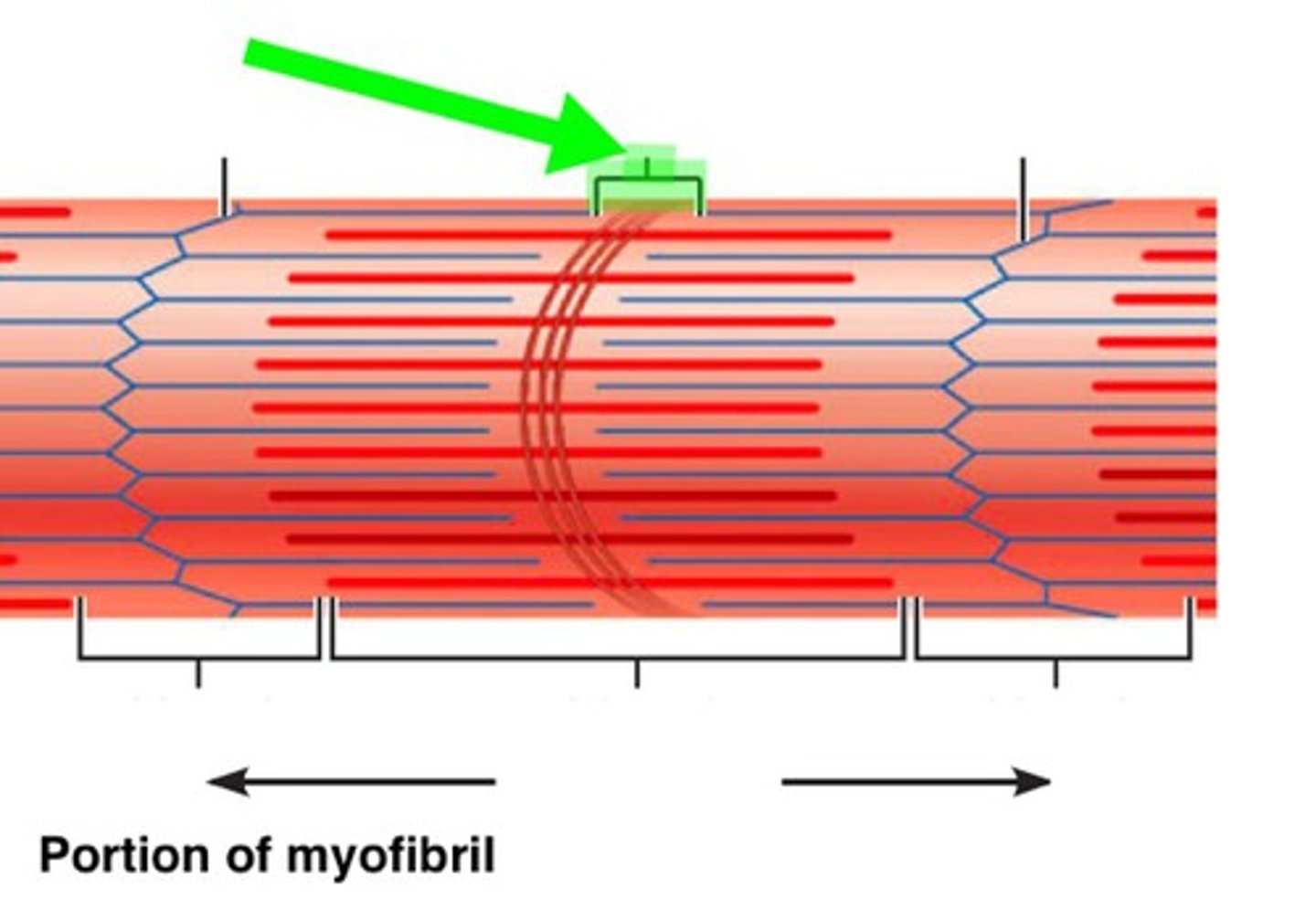
Myofibrils
Internal structure of long, rod-shaped organelles. Unbranched cylinders that are present in large numbers, making up more than 80% of the sarcoplasm. They are specialized contractile organelles unique to muscle tissue. Myofibrils contain myofilaments. The myofibrils in a fiber are separated from one another by other components of the sarcoplasm. Among those components are mitochondria and glycosomes, both of which supply energy for muscle contraction.
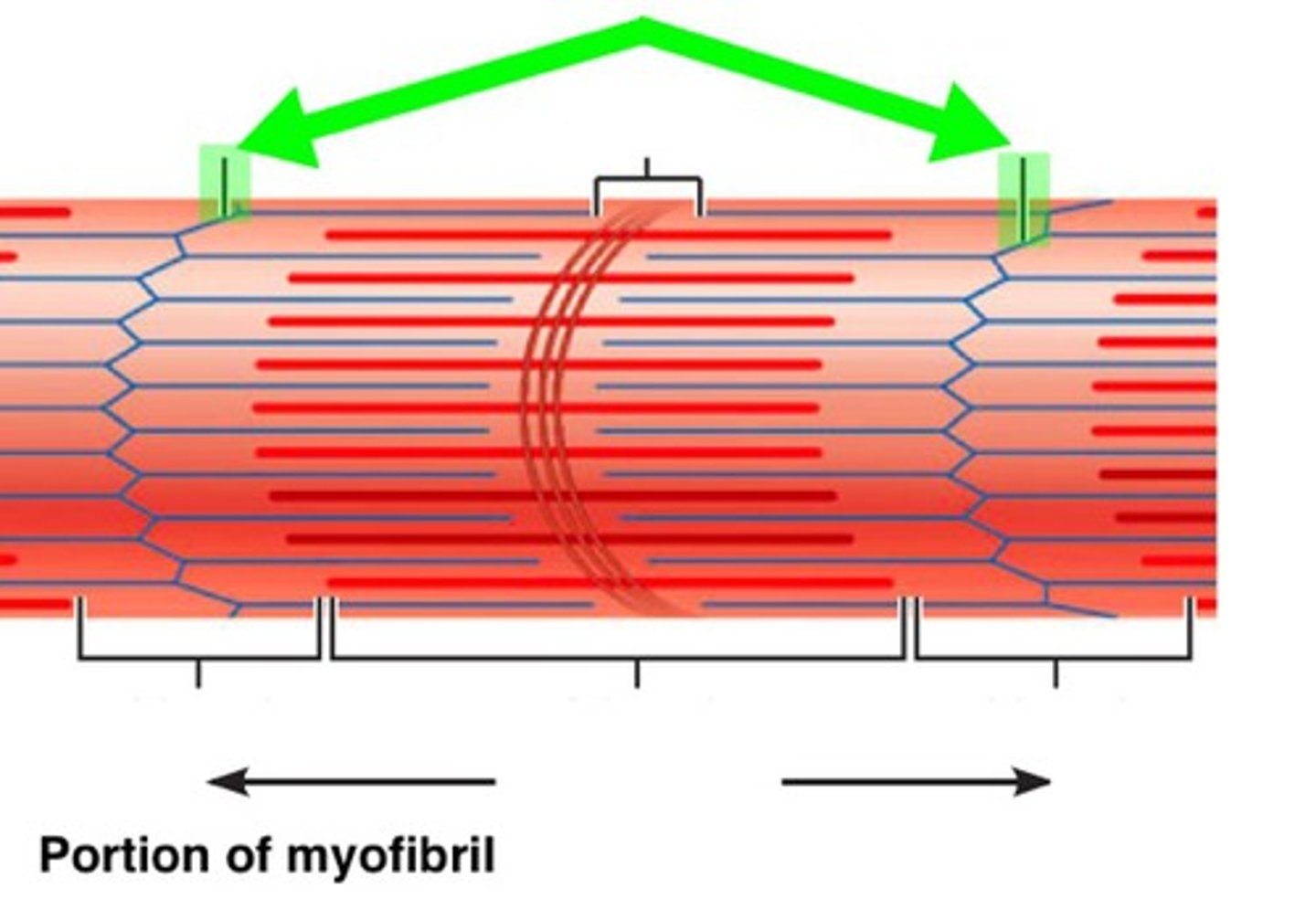
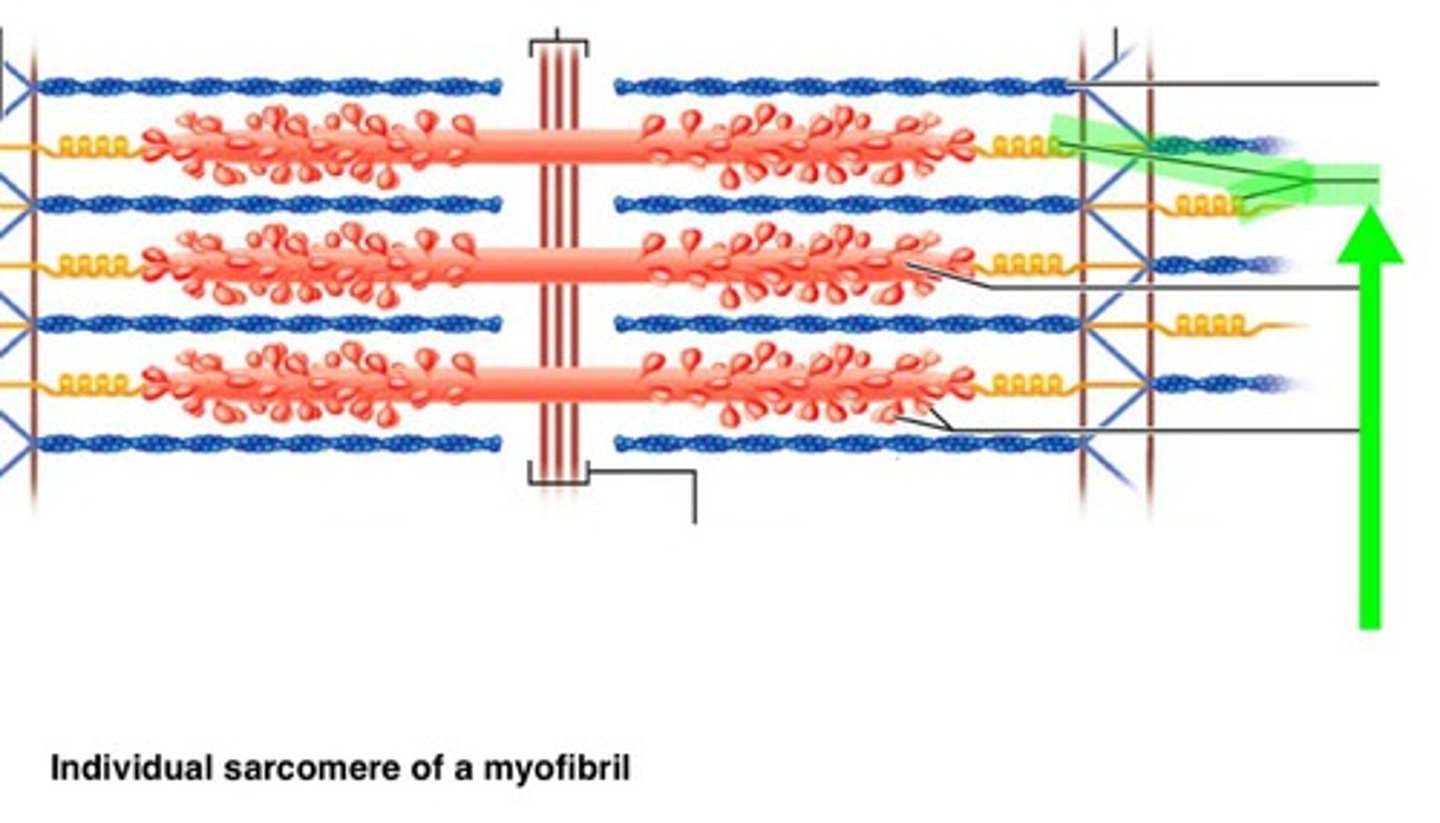
Sarcomere
Repeating segments that makeup a myofibril (many myofibrils in a muscle cell myofiber). Acts as a basic unit of contraction in skeletal muscle. Bounded by Z disks.
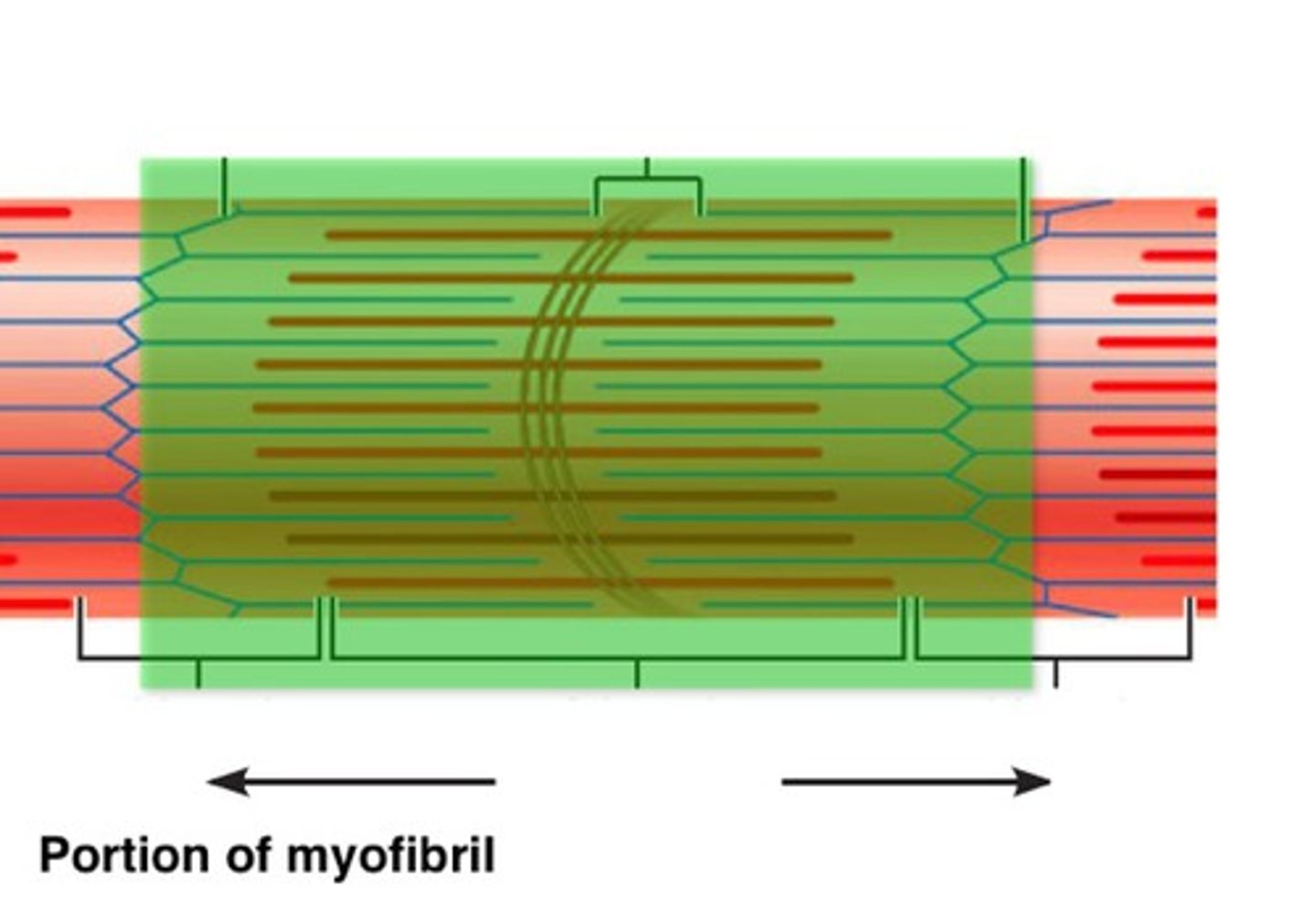
Z disc (Z line)
The boundaries at the two ends of each sarcomere.
Thin Filament
Attached to each Z disc and extending toward the center of the sarcomere are many fine myofilaments. The thin filaments are composed primarily of the contractile protein actin and two regulatory proteins, troponin and tropomyosin.
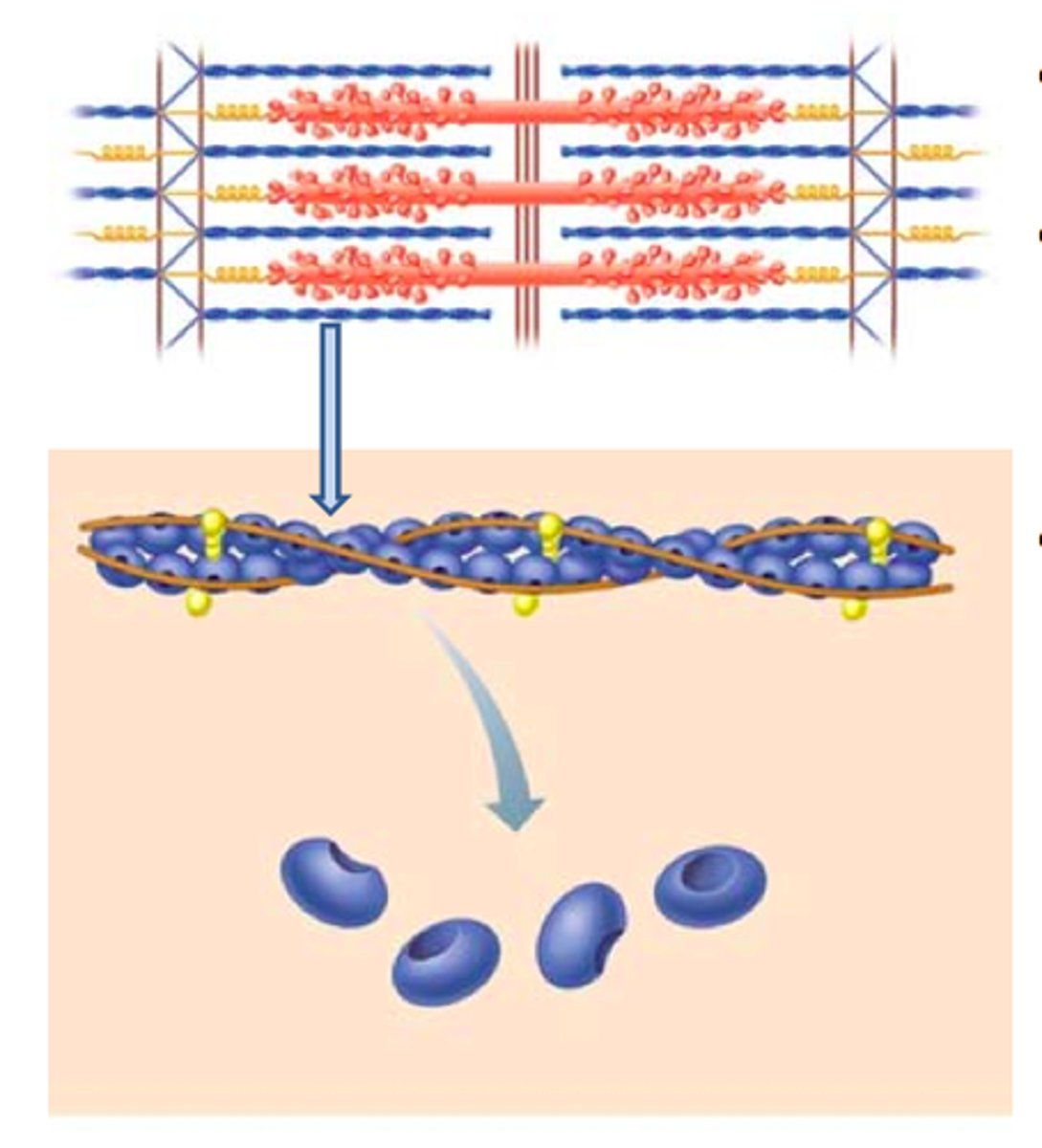
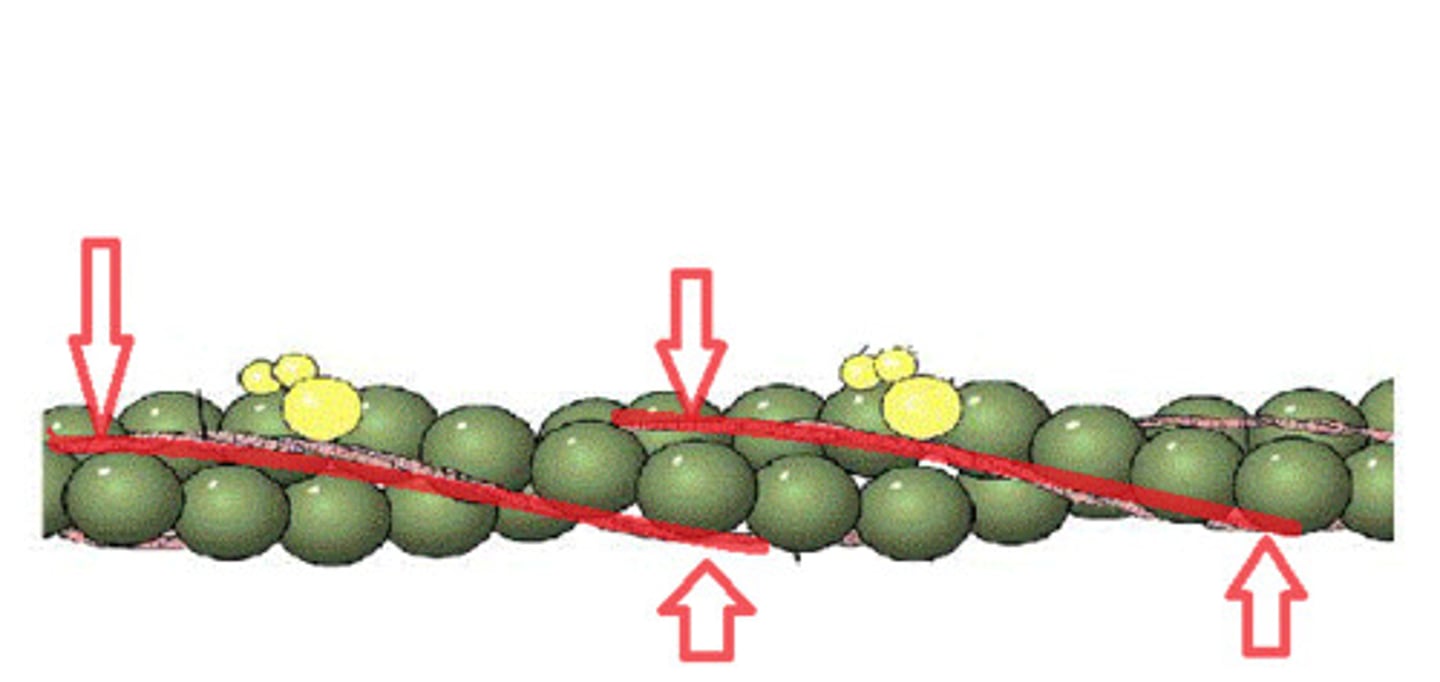
Troponin
Globular protein with three binding sites: one for actin, one for tropomyosin, and one for calcium. Troponin attaches the tropomyosin strand to the actin molecule.
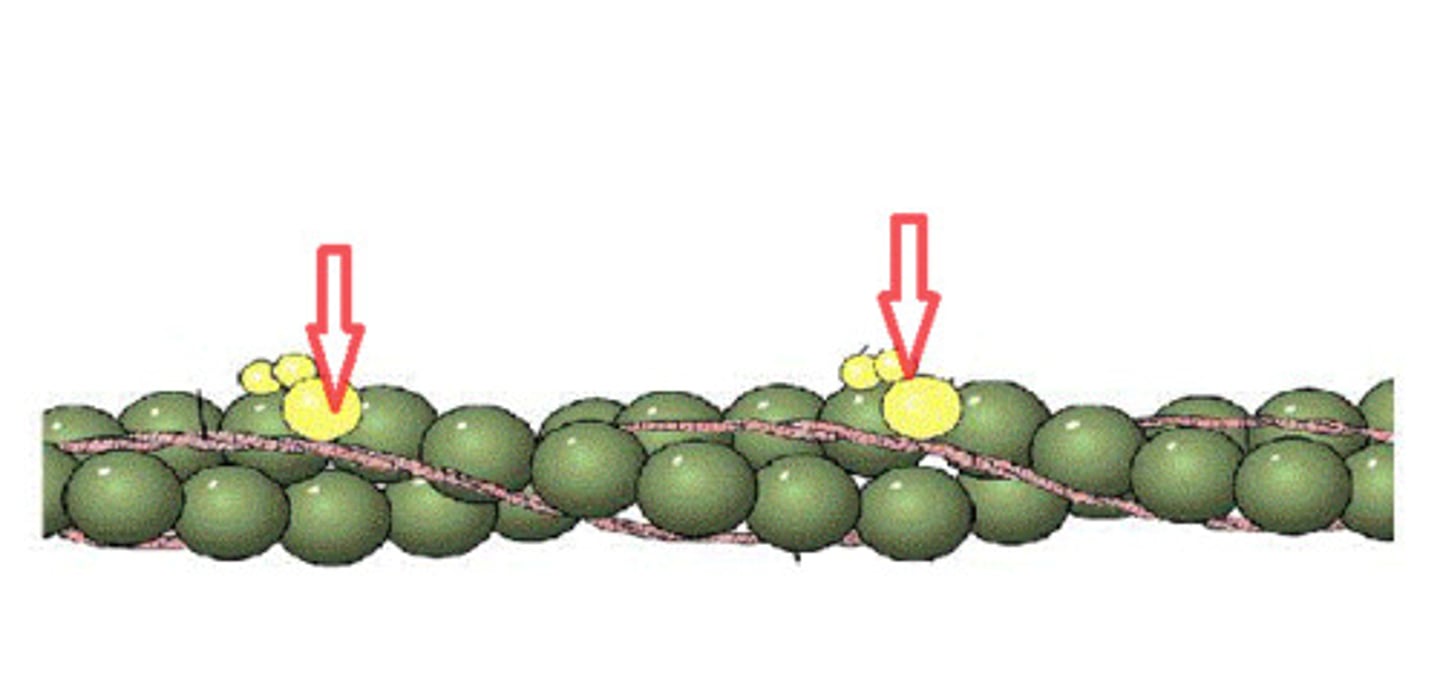
Tropomyosin
Forms a thin strand that spirals around the actin molecule.
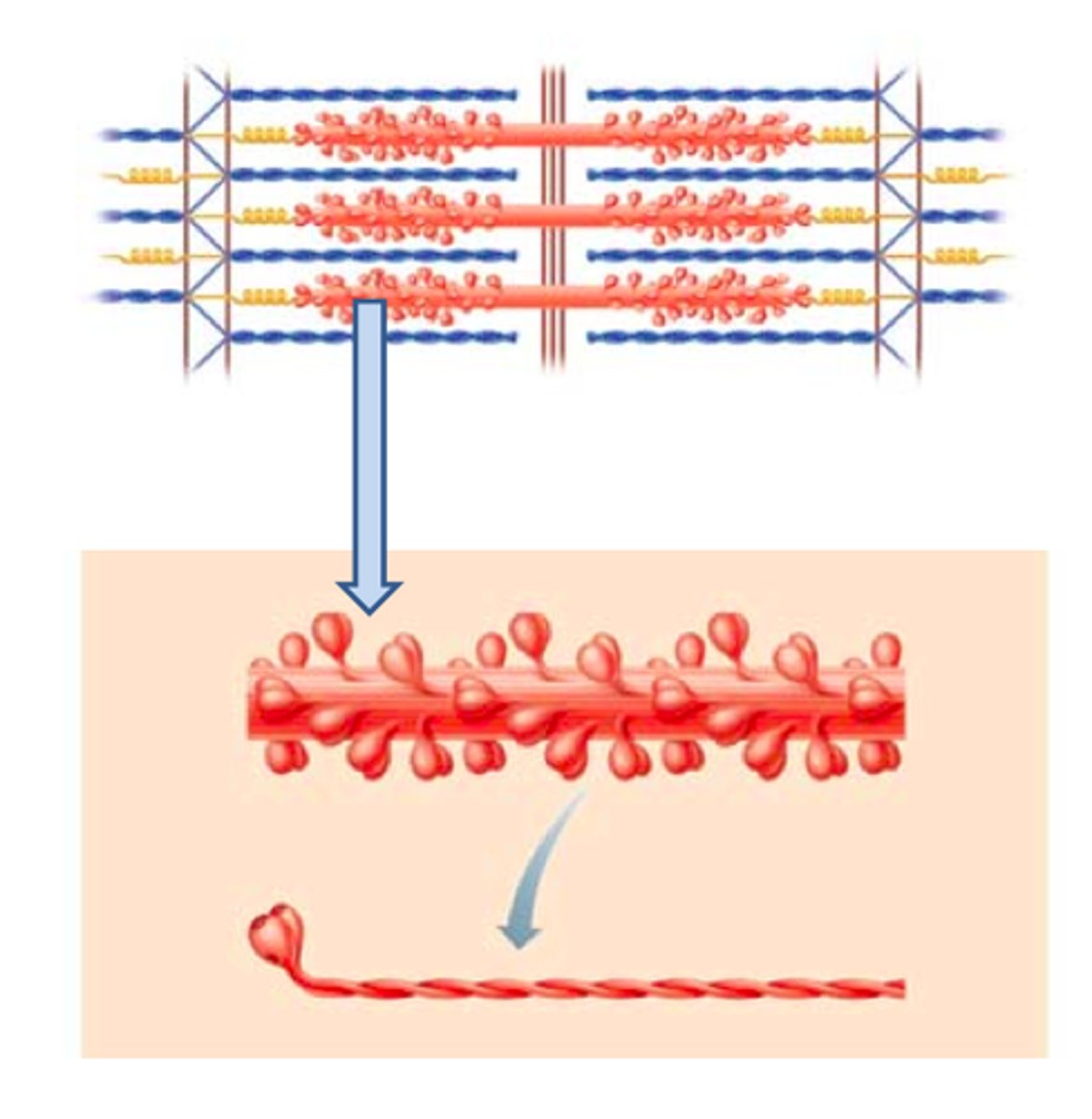
Thick Filament
In the center of the sarcomere and overlapping the inner ends of the thin filaments is a cylindrical bundle of thick (myosin) filaments. Thick filaments consist largely of myosin molecules. They also contain ATPase enzymes that split ATP (energy-storing molecules) to release the energy required for muscle contraction. Both ends of a thick filament are studded with knobs called myosin heads.
A Band
The dark bands are created by the full length of the thick filaments in the sarcomeres, along with the inner ends of the thin filaments, which overlap the thick filaments
H Zone
The central part of an A band, where no thin filaments reach
I Band
The two regions on either side of the A band. Contains only thin filaments. Each I band is part of two adjacent sarcomeres and has a Z disc running through its center. The I band shrinks as the muscle contracts.
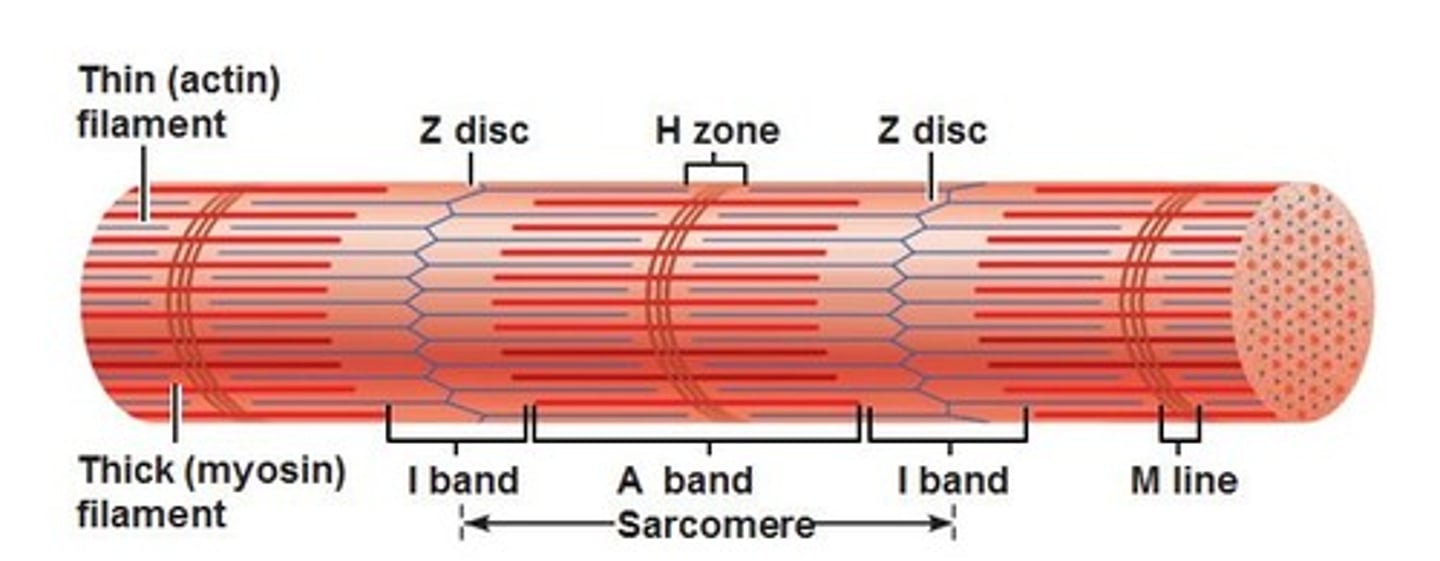
M Line
In the center of the H zone that contains tiny rods that hold the thick filaments together.
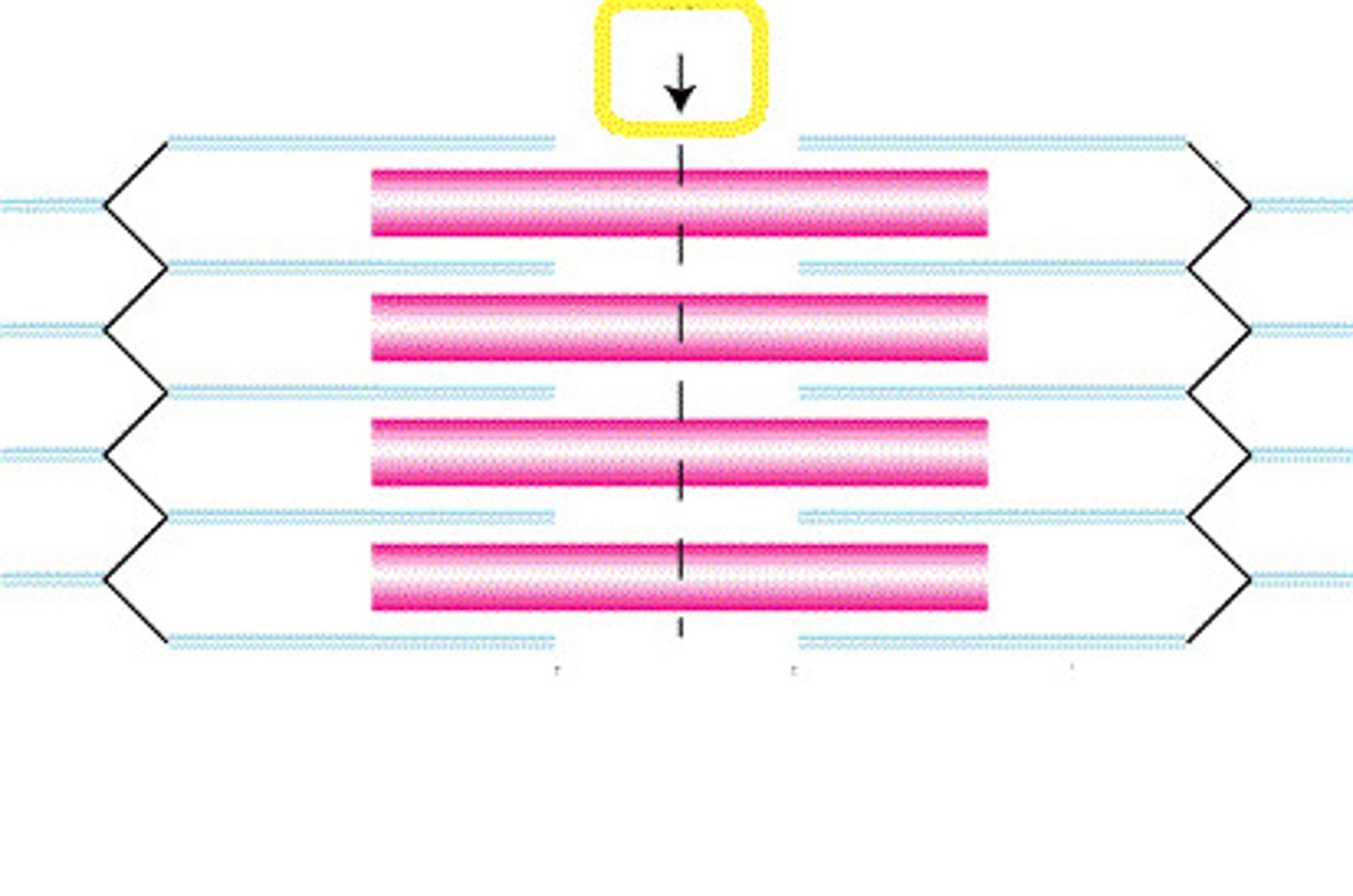
Titin
Springlike molecule in sarcomeres that resists overstretching. The titin molecules in a sarcomere are found in the elastic filaments. They extend from the Z disc to the thick filament and run within the thick filament to attach to the M line. It holds the thick filaments in place in the sarcomere, thereby maintaining the organization of the A band and it unfolds when the muscle is stretched and then refolds when the stretching force is released, thereby contributing to muscle elasticity. Titin does not resist stretching in the ordinary range of extension, but it becomes stiffer the more it uncoils; therefore, it strongly resists excessive stretching that tries to pull the sarcomere apart.
Sarcolemma
The plasma membrane of muscle cells.
Synaptic Cleft
The terminal boutons are separated from the sarcolemma of the muscle fiber by a space called the synaptic cleft
At the synapse, the plasma membranes of the two neurons are separated by a synaptic cleft
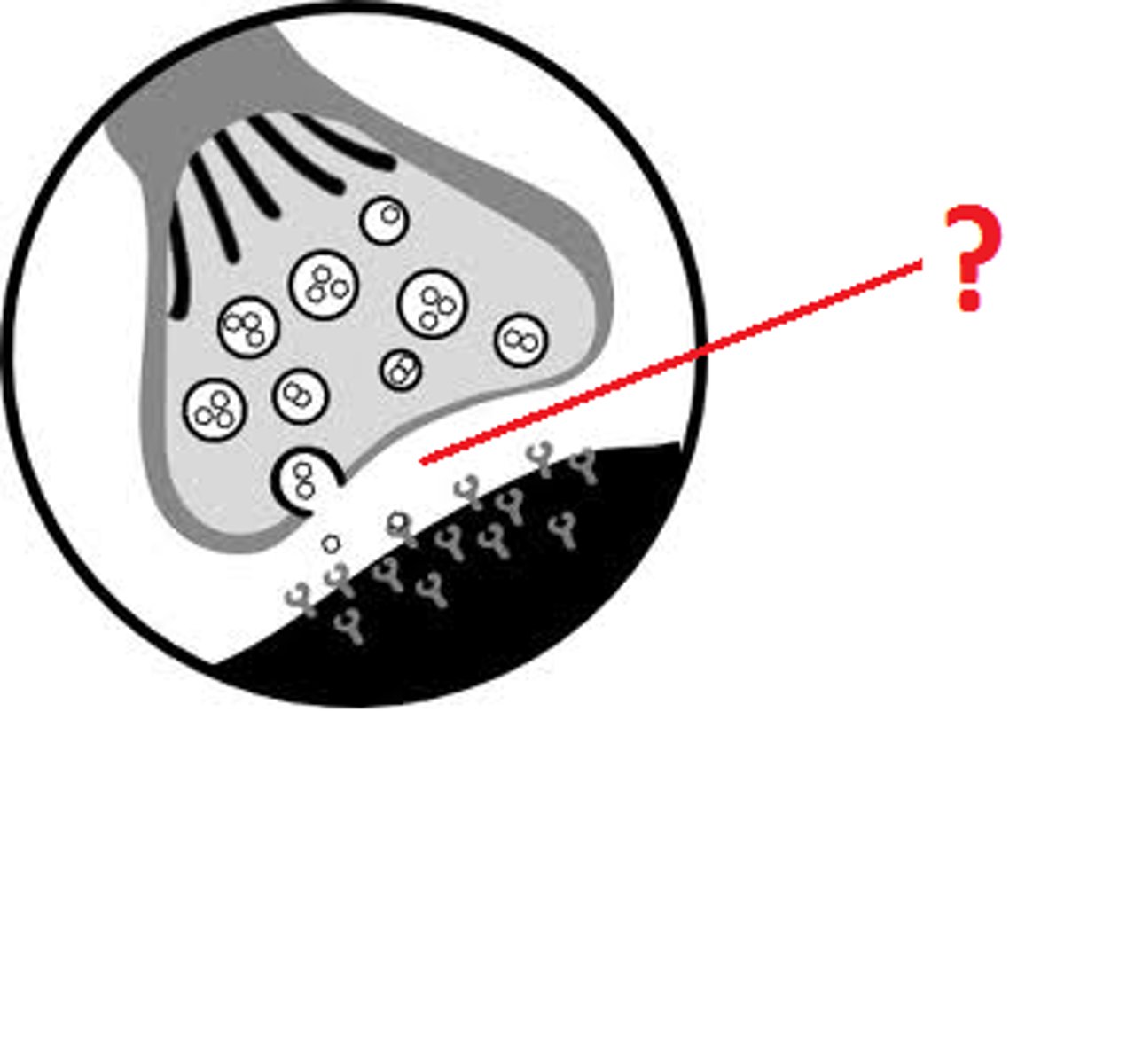
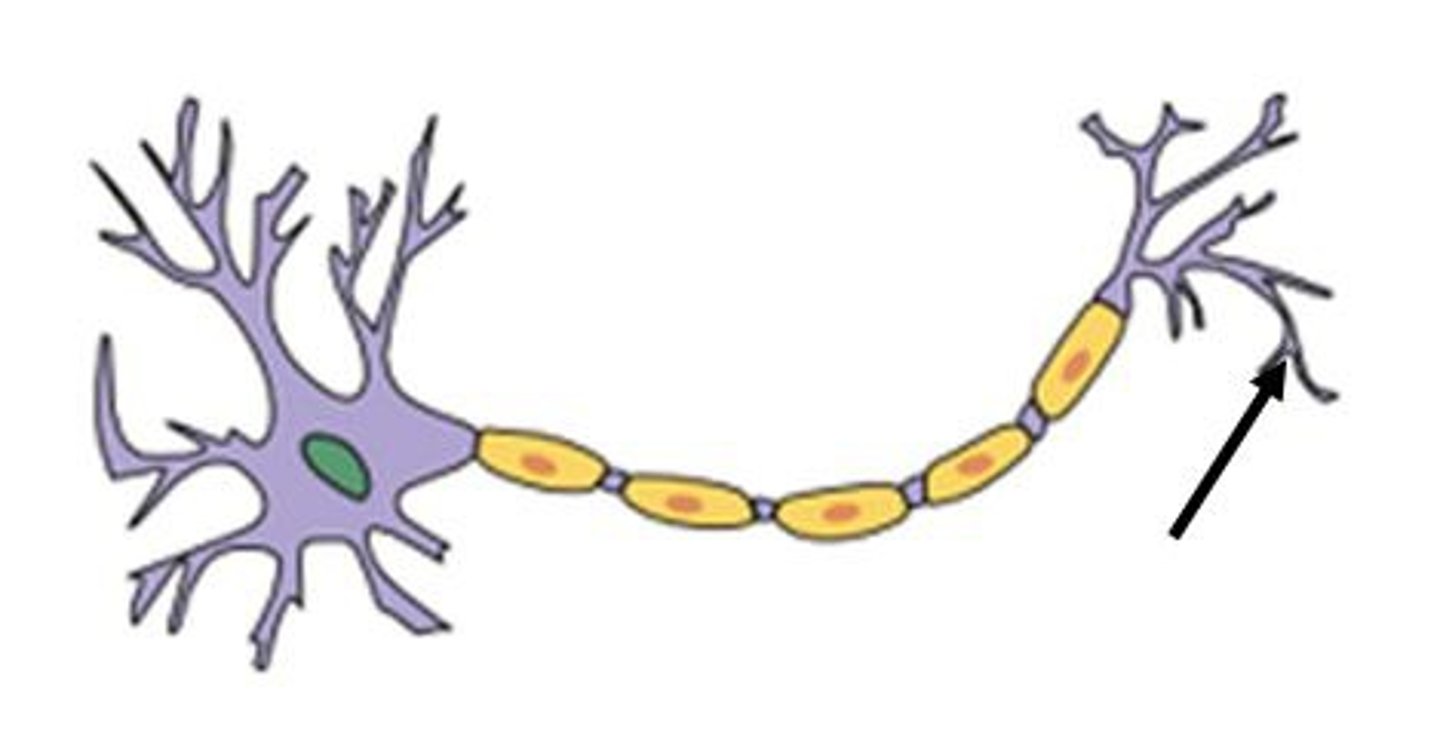
Axon Terminal / Terminal Bouton
The nerve part of the neuromuscular junction or a motor end plate is a cluster of enlargements at the end of the axonal process that stores chemical messenger molecules, neurotransmitters.
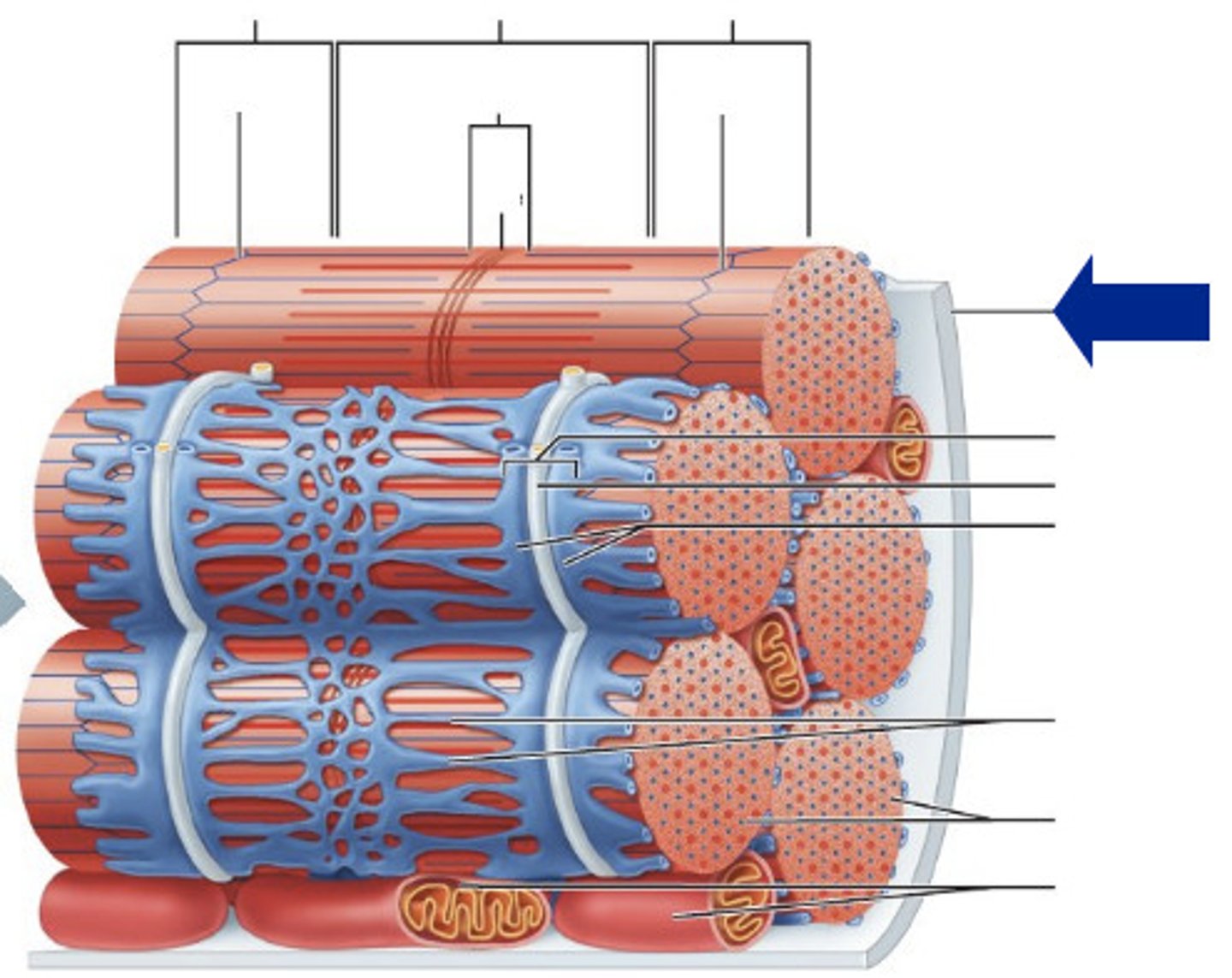
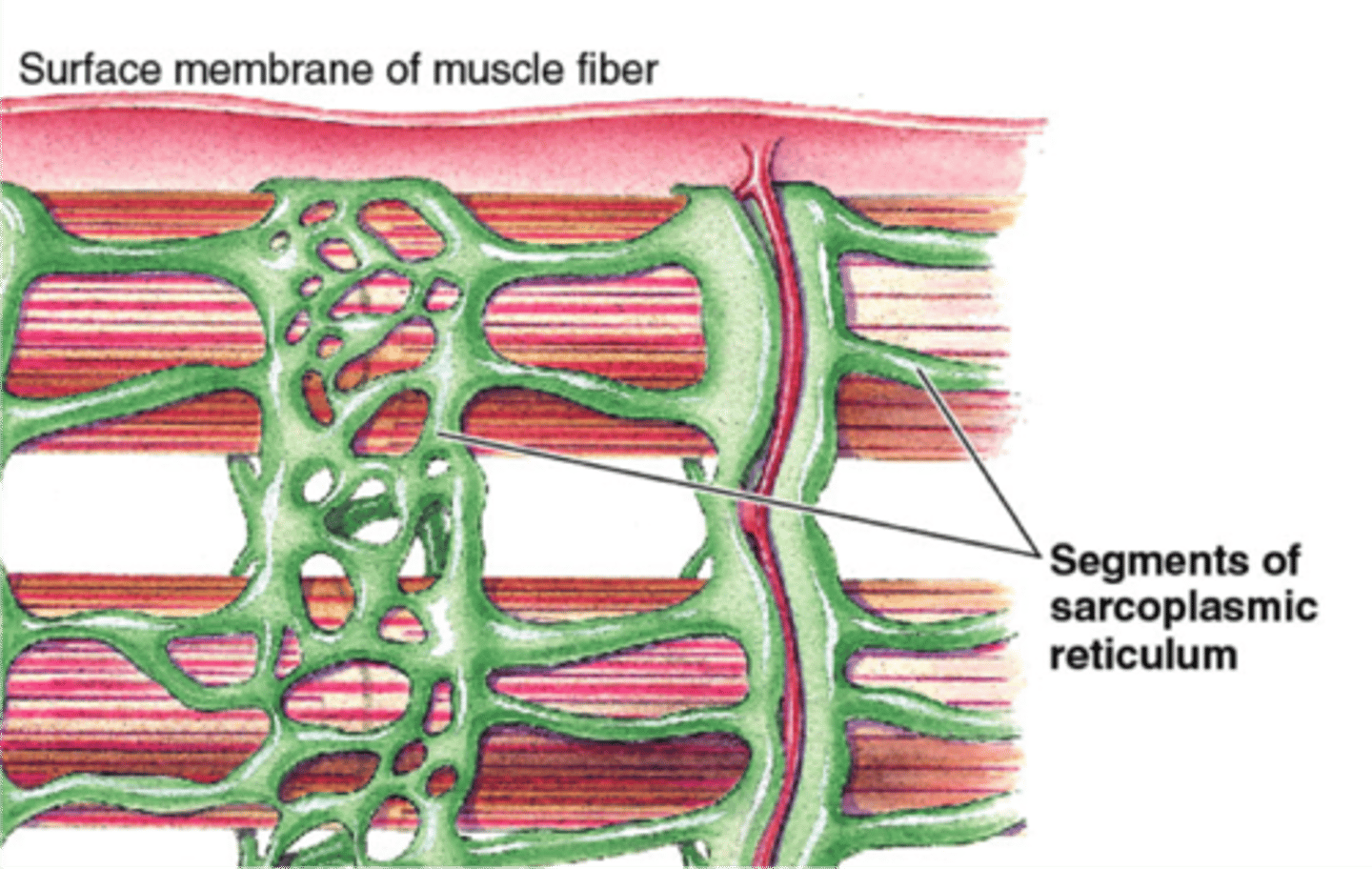
Sarcoplasmic Reticulum
An elaborate smooth endoplasmic reticulum whose interconnecting tubules surround each myofibril like the sleeve of a loosely crocheted sweater surrounds your arm. Most SR tubules run longitudinally along the myofibril. Store large quantities of calcium ions (Ca 2+). These ions are released when the muscle is stimulated to contract.
T Tubule - (Transverse Tubules)
Deep invaginations of the sarcolemma that run between each pair of terminal cisterns
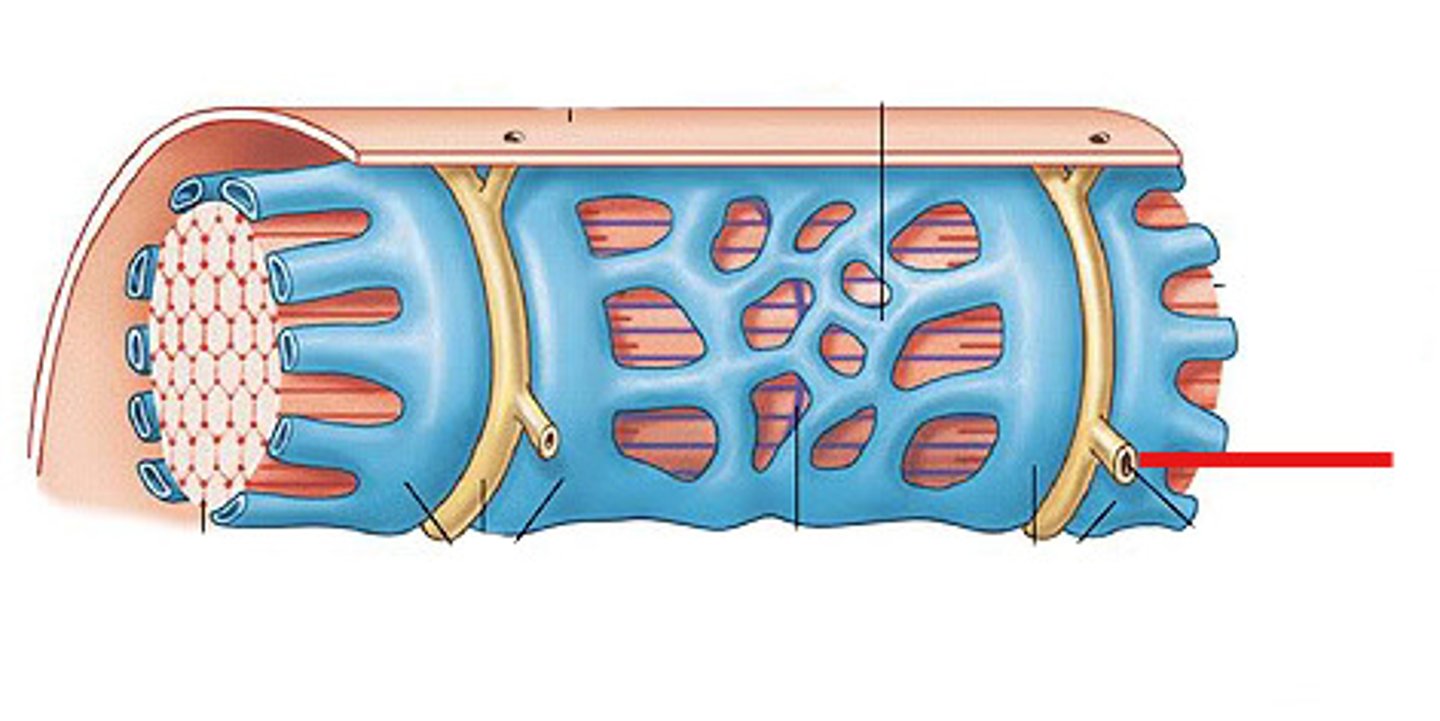
Terminal Cistern
Sarcoplasmic reticulum (SR) form larger, perpendicular cross channels over the junction between each A band in a myofibril and its adjacent I bands (A-I junctions). Store large quantities of calcium ions (Ca 2+). These ions are released when the muscle is stimulated to contract.
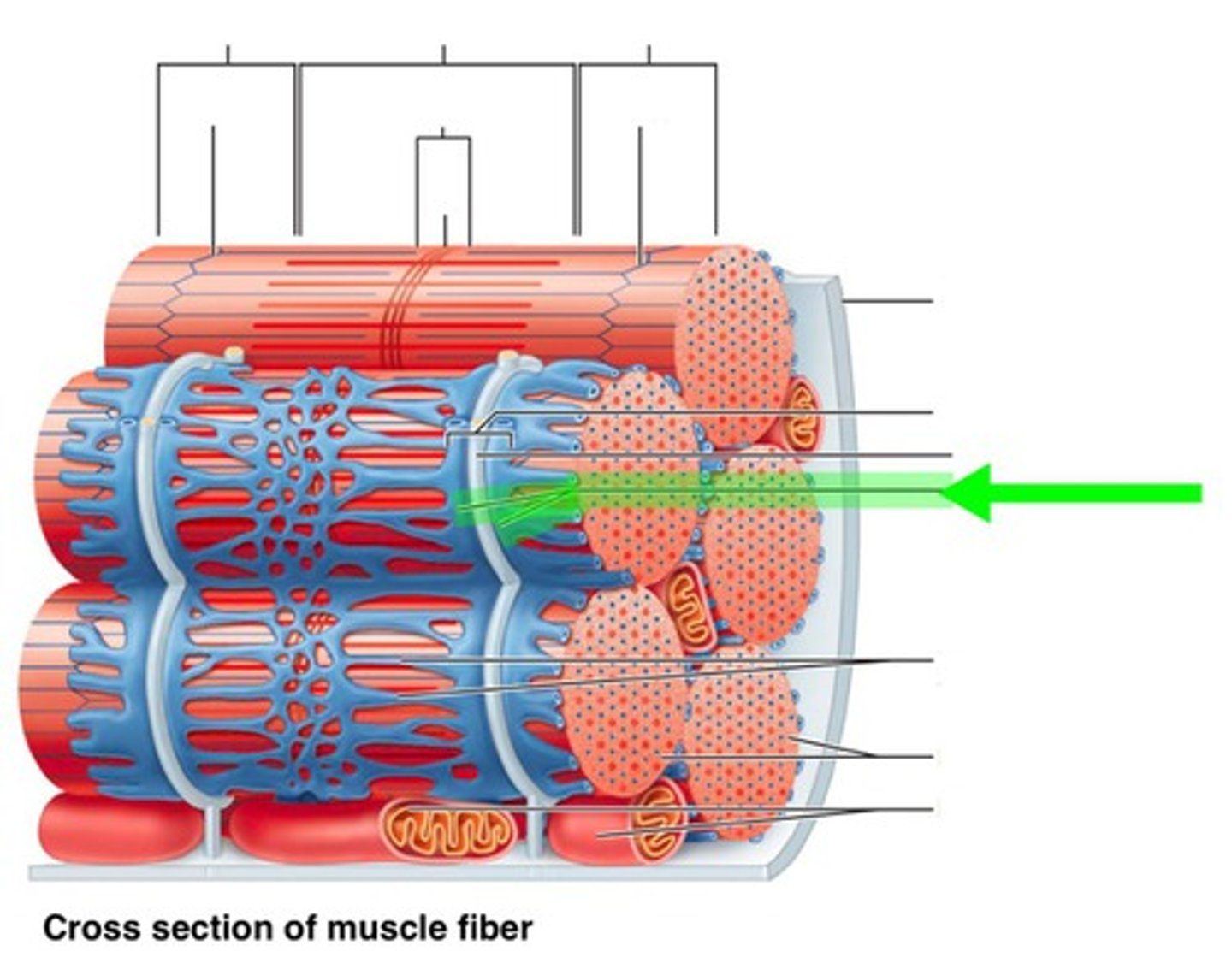
Triad
The complex of the T tubule flanked by two terminal cisterns at the A-I junction
Concentric Contraction
Concentric contraction is the more familiar type, in which the muscle shortens and does work—picking up a book or kicking a ball. When contracting concentrically, a muscle generates force while shortening.
Eccentric Contraction
Eccentric contraction occurs when a muscle generates force as it lengthens. When contracting eccentrically, a muscle generates force while lengthening. This type of contraction is essential for controlled movement and resistance to gravity. Eccentric contraction occurs in many movements that resist gravity: going down stairs, running downhill, landing from a jump. Whenever muscles are acting as a brake, they are contracting eccentrically.