Growth hormone insulin-like growth factor-1 prolactin dopamine≥/
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
58 Terms
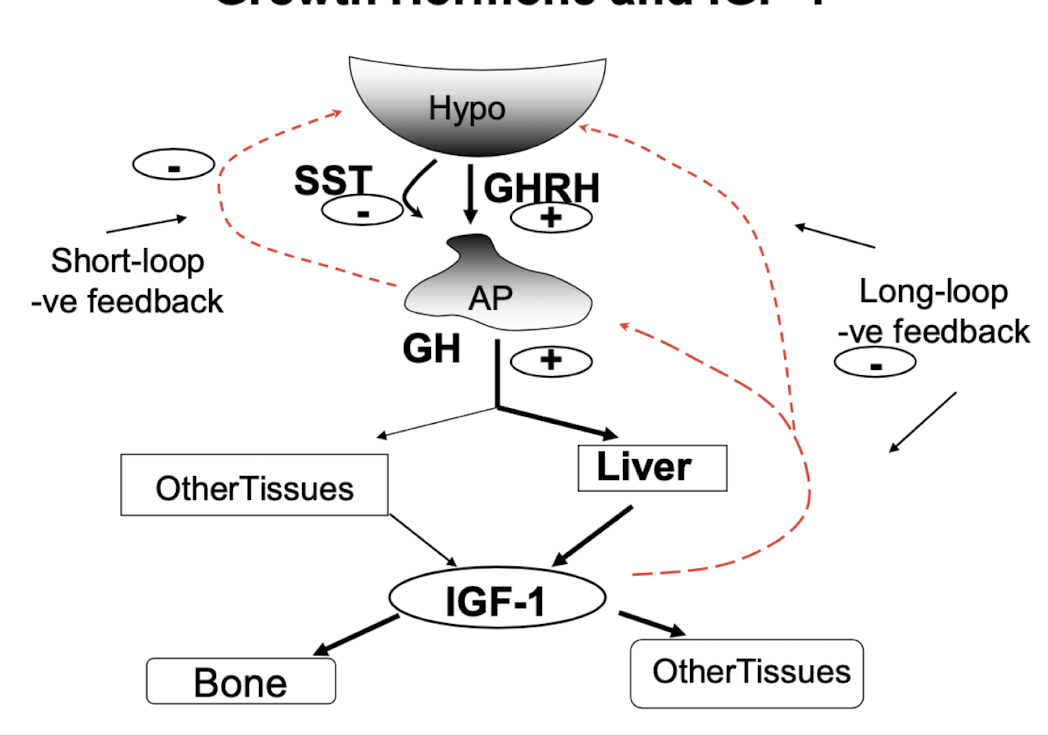
hypothalamic-pituitary-growth hormone axis
what stimulates the release of growth hormone (GH)
hypothalamic secretion of growth hormone-releasing hormon (GHRH) or ghrelin
what inhibits the release of GH
somatostatin
what does GH stimulate
the liver to synthesize and secrete insulin-like growth factor-1
what does IGF-1 do
promotes systemic growth
inhibits GH release from the anterior pituitary gland

when is GH expressed at high concentrations
during puberty
in which manner is GH secreted
in a pulsatile manner (large pulses at night during sleep)
what are GH’s anabolic effects mediated by
Insulin like growth factors → IGF-1
what does GH promote
lipolysis, gluconeogenesis and protein synthesis
IGF-1 is released into the circulation by what
hepatocytes in response to stimulation by GH
what do both GH and IGF-1 promote
skeletal and soft tissue growth
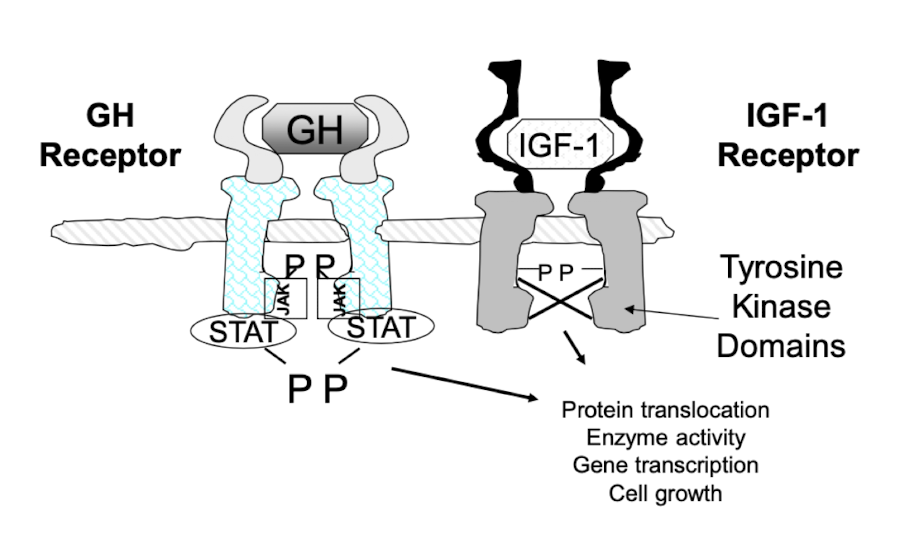
what are GH and IGF-1 receptors similar in
structure and action
GH deficiency
cause of retarded growth or possibly dwarfism
can be heritable or acquired
can be: a hypothalamic defect (GHRH defect), a pituitary problem → tumor, trauma, infection
clinical manifestation of GH deficiency
cardiovascular
psychosocial problems
decreased muscle and bone mass
increased body fat (face)
low energy and reduced strength
poor libido and sleep patterns
diagnosis of GH deficiency
measurement of serum GH levels (basal and stimulated GH levels often needed)
dwarfism occurs when
an individual is short in stature resulting from a medical condition caused by slow growth
Disproportionate dwarfism is characterized by
one or more of the body parts being relatively large or small in comparison to those of an average size adult, with growth variations in specific areas being apparent (Achondroplasia + GH deficiency)
proportionate dwarfism
the body appears normally proportioned, but is unusually small (GH deficiency)
Therapy for GH deficiency
Recombinant human Gh (rhGH) such as somatropin (Accretropin)
Mecasermin (rhIGF-1/rhIGFBP-3)
Sermorelin (synthetic form of GHRH)
recombinant human GH (rhGH) - somatotropin (Accretropin)
given SC in the evening (3-7X/week)
what is Somatropin given to children for
deficiencies such as chronic renal disease (CRD)
turner’s syndrome
these children would have their IGF-1 levels and their height monitored over time and therapy would be continues until the growth spurt has ceased
why would somatropin be given to adults
GH deficiency
AIDS wasting
short bowel syndrome
anti-aging
why has GH therapy been abused in athletes
due to its anabolic properties
when is Mecasermin used (rhIGF-1/rh;GFBP-3)
in children with
GH receptor defects
antibodies to GH
what is rhlGFBP
the binding protein responsible for maintaining IGF-1 half lfe
when is Sermorelin (synthetic form of GHRH) used
it is not useful if the deficiency occurs at the level of the pituitarygland but it can be used diagnostically to differentiate between hypothalamic and pituitary disease → if successful, would be @ the hypothalamic level, nt pituitary
GH excess
Gigantism
Acromegaly
gigantism
excessive linear growth when epiphyses of growth plates still unfused in young
very rare condition - significantly shortened life
acromegaly
characterized by soft tissue swelling
GH excess in adulthood; uncommon
other conditions that might accompany acromegaly
arthropathy (form of arthritis)
visceromegaly (enlargement of abdominal organs)
respiratory and cardiovascular problems
gastrointestinal tumors
how is acromegaly diagnosed
by elevated serum IGF-1 or GH and cause is usually associated with a tumor of the anterior pituitary
surgery successful if the tumor is microadenoma, otherwise radiation can also be applied
GH excess drug therapy
Octreotide
Pegvisomant
Octreotide (generic, sandostatin, somatostatin analogue)
inhibits Gh release
longer halflife than SST
depot forms available
Pegvisomant (somavert; GH antagonist)
decreases IGF-1
Newly approved; alternative to somatostatin analogs
dopamine agonist
prolactin
a peptide hormone produced in the anterior pituitary (lactotrophs)
what receptor is prolactin receptor similar to
GH receptor
what does prolactin do
causes breast development and milk production following birth
treatment for prolactin deficiency
there is no treatment for prolactin deficiency; prolactin excess does not always result in adverse symptoms
what may too much prolactin cause
too much prolactin (frequently bc of a prolactin secreting pituitary tumor) may cause inappropriate breast development and lactation (particularly problematic in med) as well as reproductive difficulties
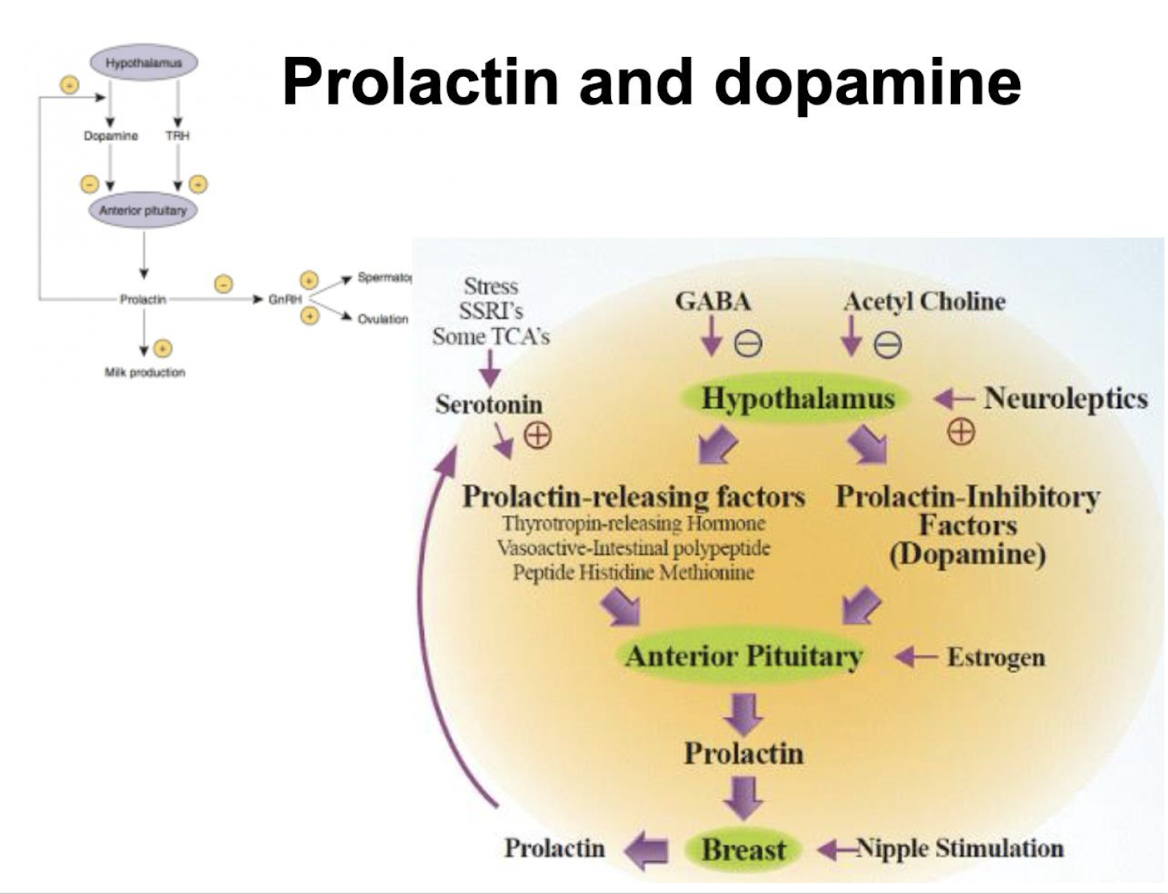
what is dopamine normally released by and what does it do
dopamine normally released by the hypothalamus to decrease prolactin secretion from the pituitary, so dopamine-like drugs can be used to decrease prolactin
what is pituitary prolactin secretion regulated by
endocrine neurons in the hypothalamus → the neurosecretory tuberoinfundibulum (TIDA) neurons of the arcuate nucleus that secrete dopamine (aka prolactin inhibitory hormone)
what receptors does dopamine act on and what does it cause. what happens in the absence of dopamine?
dopamine acts on D2 receptors of lactotrophs, causing inhibition of prolactin secretion
in absence of dopamine, prolactin cells secrete prolactin continuously
what effect does TRH have on prolactin release
TRH has a stimulatory effect on prolactin release, however, Prl is the only adenohypophyseal hormone whose principal control is inhibitory
prolactin and dopamine: drug therapy
dopamine-like drugs can be used to decrease prolactin
what are drugs used to decrease prolactin
Bromocriptine and cabergolide
what do bromocriptine and cabergolide do
stimulate D2 dopamine receptors in the anterior pituitary to decrease prolactin secretion
used if an individual is diagnosed with prolactin secreting tumour (prolactinoma)
administration of dopamine analogues includes oral, intravaginal (reduces nausea observed with oral form) and subcutaneous deposits which are longer acting
acromegaly can also result following what
development of a pituitary tumor that may secrete GH and prolactin
growth hormone and prolactin -
related protein hormones released by anterior pituitary
GH stimulates
growth, directly and indirectly via IGF-1 synthesis in the liver
GH controlled by
somatostatin (-ve) and GH releasing hormone (+ve) from hypothalamus
GH deficiency
dwarfism in development; excess: gigantism in development, acromegaly in adulthood
prolactin stimulates what
lactation, controlled by hypothalamic dopamine (-ve), inhibits reproduction
prolactin excess (pituitary microadenoma, common in women)
stimulates breast, causes infertility
excess GH in acromegaly can be inhibited by what
somatostatin analogs, or dopamine D2 (pituitary dopamine receptor) agonists because of similarity between GH producing and prolactin producing cells
D2 agonists (many drugs, bromocriptine main example)
inhibit Gh and prolactin secretion
Main D2 drug uses:
suppression of prolactin from pituitary microadenoma, restoration of fertility in hyperprolactinemic pts