Pupil1
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
3 functions of pupils
- regulate light
- reduce spherical and chromatic aberrations
- increase depth of focus through the accommodation response
which pathway is involved in pupil miosis?
parasympathetic pathway
fibres involved during pupil constriction - inner circular muscles
what pathway is involved during pupil mydriasis?
oculosympathetic pathway
fibres involved - radial fibres dilate
when does miosis occur
light reflex
accommodative reflex
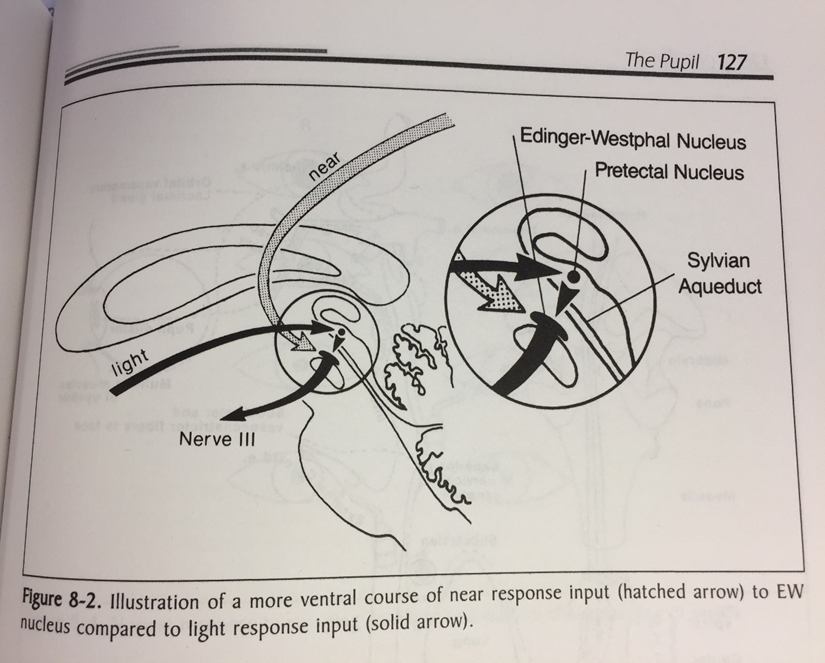
describe the parasympathetic pathway in normal light reflex
- - periphery - light stimulus - optic nerve- optic chiasm - light falls on retina
- afferent neurones (rgc) create signal travels→ visual pathway via chiasm
- 2/3rds along the way, some axons divert → pretectal nucleus
→ info relayed to EWS bilaterally→ Efferent pathway - oculomotor nerve - synapse in ciliary ganglion red nucleus
- pupil fibres travel with 3rd nerve to iris sphincter muscles for constriction (miosis)
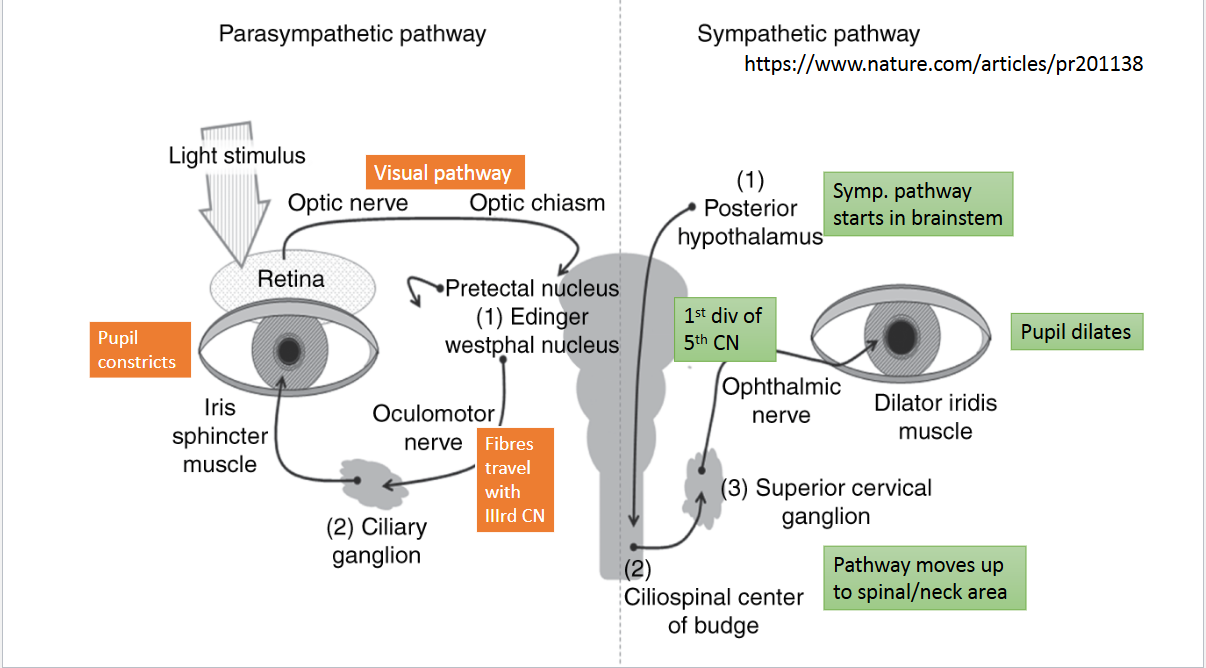
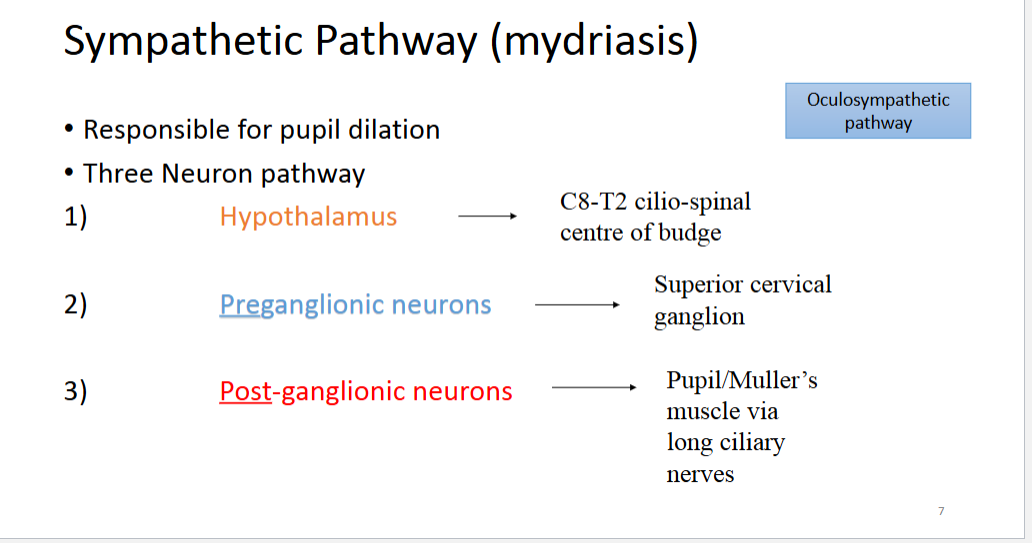
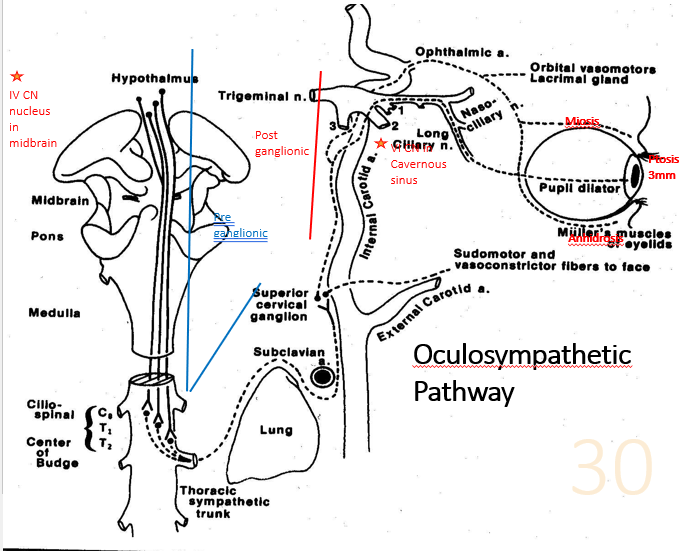
describe pathway for sympathetic pathway
- originates in the posterior hypothalamus
- 1st order neuron travels down brainstem + spinal cord to level of C8-T2/ciliospinal centre of budge
- 2nd order neuron (preganglionic neuron) leave spinal cord and enter paravertebral chain and terminate in the superior cervical ganglion found at the skull base
- 3rd order neuron (postganglionic neuron) ascend with the ICA and join ophthalmic nerve in the cavernous sinus into the orbit via superior orbital fissure to the dilator iris muscle - midriatric pupil
summary of the sympathetic pathway
- originates in posterior hypothalamus -> down brainstem to C8-T2/cilliospinal centre of budge
- preganglionic neurons -> superior cervical ganglion
- post ganglionic neuron -> pupil/Muller muscle via long ciliary nerves
describe the near reflex
neurons -> visual cortex from LGB
optic radiations
visual cortext
& represented in area 19 - near response
- from area 19, cortical fibres descend via internal capsule and synapse with EWS nuclei
- continue pathway for light reflex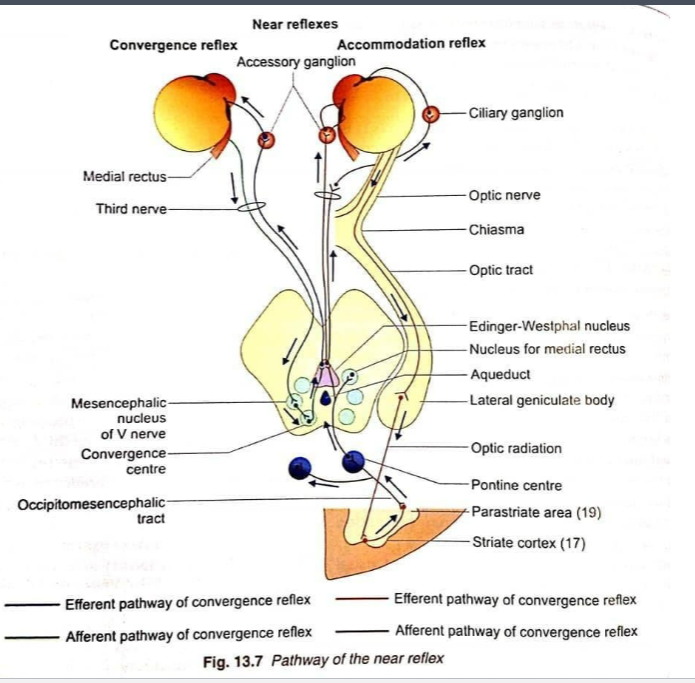
causes of irregular pupils?
trauma
iris tumours
coloboma
posterior adhesions to the lens (synechiae)
whats aniridia?
absence of iris
what's corectopia?
displaced pupil
why would a 3rd nerve palsy cause pupil involvement?
efferent parasympathetic fibres travel in outer layers of 3rd nerve so external compression onto 3rd nerve causes pupil involvement
what occurs in holmes-adie tonic pupil?
-Lesion in the ciliary ganglion
Mostly affects women (30s-40s)
No response to direct/consensual light reflex
Accommodative response impaired
Due to denervation and supersensitivity
Possible reduction in knee jerk reflex
WILL REACT TO
0.125% PILOCARPINE
or METACHOLINE
CHLORIDE (2.5%)
is
which pathway is affected in dorsal midbrain/parinaud's syndrome
parasympathetic pathway affected
pupils don't constrict to light but normal constriction to accommodative target occurs
occurs in dorsal midbrain
light pathway knocked out but near pathway intact
convergence retraction nystagmus - eyes converge when looking into elevation
what are uniocular causes of a constricted pupil?
horner's syndrome
anterior segment inflammation
what is a binocular cause of a constricted pupil?
argyll robertson
convergence/accommodative spasm
another name for an RAPD? and where does lesion occur
relative afferent pupillary defect
marcus gunn pupil
Lesion - afferent pathway
• Retina, optic nerve or anterior visual pathway
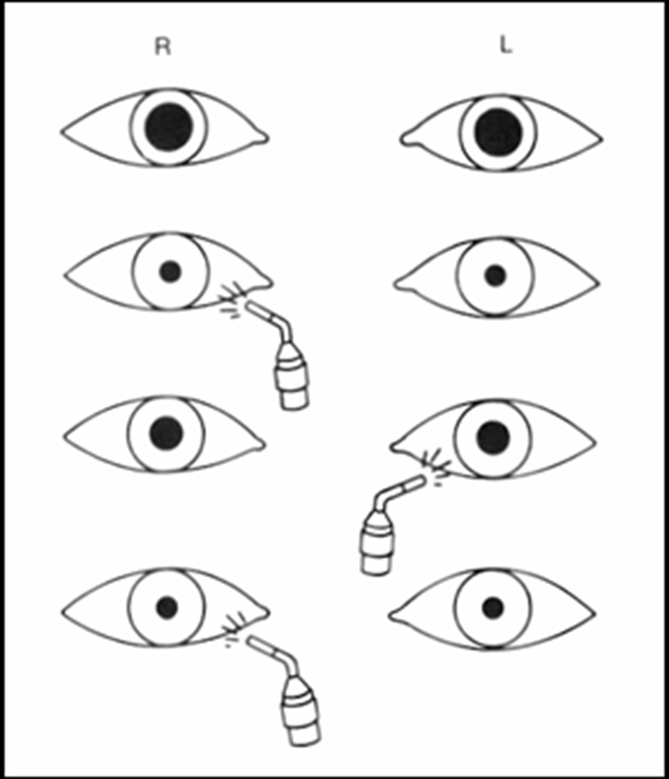
• Diagnosed by the swinging flashlight test
• The affected pupil will dilate instead of constrict when
the light is transferred from the normal eye to the
abnormal eye.
• Direct response<consensual response
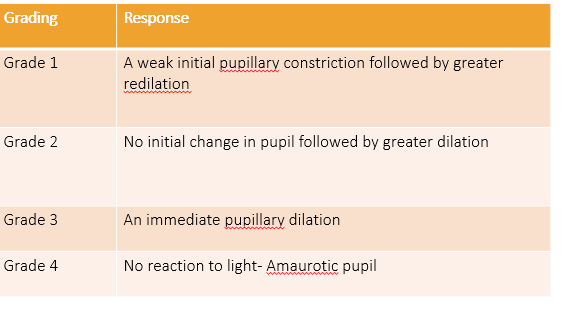
what are the grades pf RAPD
grade 1 - weak initial pupillary constriction, followed by greater redilation
g2 - no initial change of pupil followed by greater dilation
g3 - an immediate pupillary dilation
g4 - no reaction to light - amaurotic pupil
1. Functions of Pupils Under Normal Circumstances
Regulates Light: Adjusts the amount of light entering the eye.
Reduces Aberrations: Minimizes spherical and chromatic aberrations.
Increases Depth of Focus: Improves the clarity of objects at different distances.
Miosis (Parasympathetic Pathway):
Purpose: Constricts pupils.
Mechanisms:
Light reflex.
Accommodative reflex
Mydriasis (Sympathetic Pathway):
Purpose: Dilates pupils.
Mechanisms:
Oculosympathetic pathway.
4. Parasympathetic Pathway
Retinal Ganglion Cells: Afferent signals originate → Synapse in Pretectal Nucleus: Axons diverge from the optic tract to the superior colliculus. →EWS→ 3rd never pathway → red nucleus - Preganglionic fibers synapse in the ciliary ganglion → Post ganglionic →Iris Sphincter constrict the pupil
begins in retina → optic nerve→pretectual nucleus → EWS→ ciliary ganglion → sphincter pupillae
Factors Influencing Size
Factors Influencing Size:
Age, light intensity, drugs (pharmaceutical/recreational), emotions (fear, attraction).
Techniques:
Observe shape, size, symmetry.
Test direct and consensual light reflexes.
Perform the swinging flashlight test.
Assess accommodation reflex.
Common Pupil Abnormalities
Anisocoria:
Unequal pupil sizes.
Physiological: Equal difference in dim and bright light (usually <0.8 mm).
trauma
coloboma - congenital defect of iris
correctopia - misplaced pupil
heterochromia - different iris colors
Mydriatic Pupil:
check light reaction in dark conditions
greater aniscoria in bright light may indicate:
3rd NP
associated w potisis, strabismus ee - down & out & anisocoria
affected muscles - IR, IO, MR, = inferior branch of 3rd nerve
common causes of 3NP
microvascular - normal pupil - no pain
aneurysm - pain, pupil involvement, emergency surgery
trauma or tumor affecting brainstem, CS or orbital apex
3rd Nerve Palsy: EOM defects, ptosis, accommodation loss.
Holmes-Adie Tonic Pupil: Parasympathetic pathway lesion (e.g., viral/bacterial infection).
Dorsal Midbrain Syndrome: Light-near dissociation.
Acute Glaucoma: High IOP, painful red eye.
Trauma or pharmacological dilation.
Miotic Pupil:
Causes include:
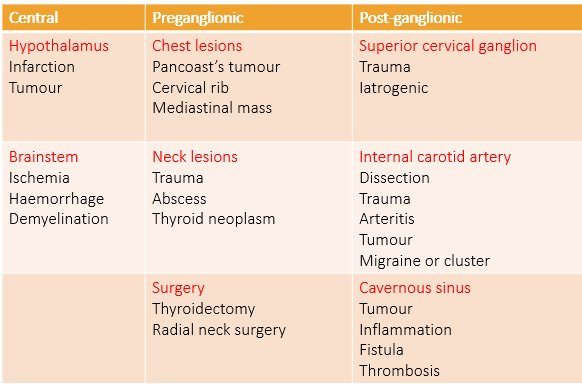
Horner’s Syndrome: Ptosis, miosis, anhidrosis.
Argyll Robertson Pupil: Poor response to light, intact near reflex (e.g., neurosyphilis).
Convergence Spasm: Often associated with accommodative issues
Failure to dilate…….?
Uniocular
Horner’s syndrome
Anterior segment inflammation
Binocular
Argyll Robertson
Convergence/Accommodative spasm
Dorsal Midbrain Syndrome:
Light-near dissociation.
bilateral night near dissociation - pupil accommodates but doesn’t react to light
causes
tumor= pineal gland, MS or damage near superior collicolus, strokes, hydrocephalus, A/V malformation
symptoms
convergence retraction nystagmus during upward gaze
difficulty elevating eyes
lid retraction
Pupillary light-near dissociation,
Associated with lesions in the dorsal midbrain.
Horner’s Syndrome:
Characteristics:
Ptosis = disinnervation of muller's muscle
miosis= sm pupil
anhidrosis= no sweating on affected side = effect of vasiconstrictor fibers of the face
causes
trauma
lung cancer
spinal issues
congenital defects
Tests:
Cocaine Test: Dilates normal pupil but not Horner’s.
Paredrine Test: Differentiates lesion location (first/second vs. third-order neuron)
8. RAPD (Relative Afferent Pupillary Defect)
Lesion in afferent pathway (e.g., retina, optic nerve).
damage to optic nerver or retina= pre chiasmal
Detected by the swinging flashlight test:
Affected pupil dilates instead of constricting when light swings from the normal to the abnormal eye.
Causes: Optic neuropathy, retinal detachment, TED (optic nerve compression), dense cataract, , diabetic retinopathy- amaurotic eye- dense amblyopia
10. Rare Pupil Disorders
Springing Pupil: Dilation during migraines.
Tadpole Pupil: Sectoral dilation, often benign.
Midbrain Corectopia: Eccentric/oval pupil associated with rostral midbrain disease
accommodation and convergence spasm
overactive accommodation & MR o/a
symptoms
diplopia
esotropia
blurred vision
causes
hypermetropia without correct lenses
presbyopia leading to over accommodation
Diagnostic testing & therapeutic interventions
iridotomy/iridectomy - laser treatment for conditions like glaucoma
Testing for pupillary abnormalities
bright light vs dim light anisocoria differentiation
light near dissociation in specific syndromes
drug testing for differential diagnosis - e.g. cocaine
LND
Adie's or tonic pupil: A disorder that causes one or both pupils to be abnormally dilated
Parinaud syndrome: A rare condition that can include LND, convergence-retraction nystagmus, and up gaze palsy
Argyll-Robertson pupils: A pupil that constricts poorly to light but constricts well when viewing something nearby
Aberrant regeneration of the third nerve: Lesions in the ciliary ganglion or postganglionic nerve can cause LND
Optic neuropathy
what controls the pupil
A: The pupil is controlled by both sympathetic and parasympathetic nervous fibers.
What is spasmus nutans and when does it occur?
A: Spasmus nutans is an acquired form of nystagmus seen in children, usually within the first 2 years of life.
: The triad of spasmus nutans includes:
1) Nystagmus (involuntary eye movement),
2) Head bobbing,
3) Torticollis (twisting of the neck).
: Head bobbing and torticollis are thought to be compensatory mechanisms to improve vision by reducing the nystagmus' frequency and asymmetry.
Ocular Motor Apraxia (OMA)
A: OMA is a condition where there is a defect or absence of voluntary eye movement control. Children with OMA struggle to move their eyes in a specific direction, especially horizontally.
A: To compensate, they use a head thrust to track objects, as they cannot initiate horizontal eye movements. Vertical eye movements typically remain unaffected.
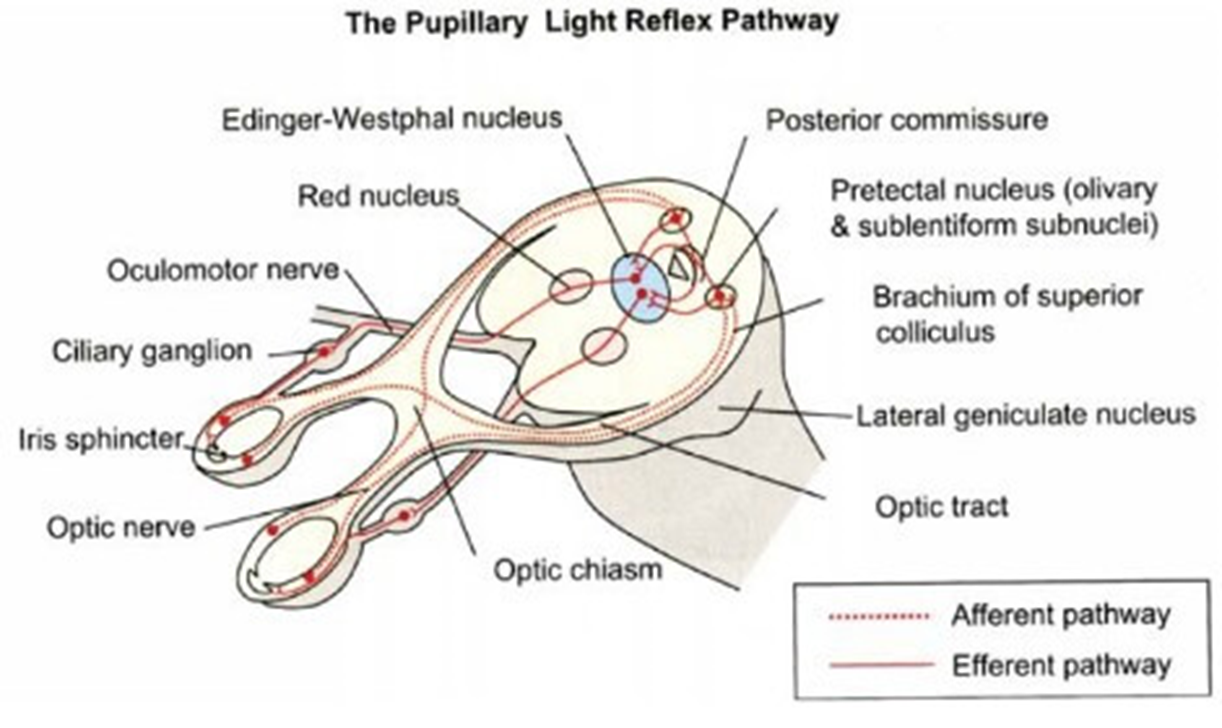
Q: Describe the pupillary light reflex pathway.
A: 1) Light hits the retina, initiating signals in retinal ganglion cells.
2) Signals travel through the visual pathway.
3) Some axons diverge to the pretectal nucleus, relaying to the Edinger-Westphal nucleus (EWN)
4) EWN sends signals via the third cranial nerve, through the ciliary ganglion to the sphincter muscle of the iris, causing pupil constriction.
Oculocardiac Reflex (OCR)
OCR is triggered by stimulation of the vagus nerve due to traction on the extraocular muscles (EOMs), often seen in pediatric fractures, causing a reduction in heart rate (bradycardia)
Q: Describe the oculocardiac reflex (OCR) pathway.
A: 1) Afferent limb: Trigeminal nerve (CN V) carries signals from stretch receptors via ciliary nerves to ciliary ganglion, then to trigeminal nucleus.
2) Efferent limb: CNS processes information, communicates with vagus nerve (CN X) motor nucleus.
3) Vagal impulses travel to sinoatrial node, causing bradycardia.
what is the Near reflex
The near reflex (or near response) occurs when focusing on a close object.
Accommodation:
Convergence:
Pupillary Constriction:
The neurons carry on to the visual cortex from LGB, optic radiations = area 19 - visual cortex
area 19 - interprets near object.
Signals → via descending fibers → thru internal capsule.
fibers synapse in the EW nucleus of midbrain.
Parasympathetic fibers (via CN III and ciliary ganglion) cause:
Accommodation (lens thickens).
Pupillary constriction.
Signals to MR muscles of both eyes = convergence.
pupil size depends on
Age
Hippus
Light intensity
Accommodation
Drugs
Pharmaceutical
Recreational
Psychosensory
Attraction
Fear
How do you asses pupil
Observation
Shape
Size (look for anisocoria)
Direct light reflex
Consensual light reflex
Swinging flashlight test
Accommodative reflex
Look for other abnormalities
Eyelids
Eye position
what are the main pupil abnormalities
Anisocoria
Mydriatic pupil
Miosed pupil(s)
Irregular pupils
Trauma
Iris tumours
Coloboma
Posterior adhesions to the lens (Synechiae)
Causes of a mydriatic pupil
Failure to constrict……..?
IIIrd N palsy
Holmes-Adie Tonic pupil
Dorsal midbrain syndrome
Acute glaucoma
Trauma
Pharmacological accident
Hutchinson pupil (coma)
IIIrd N palsy
Compressive
Aneurysm: Junction of Posterior communicating artery (PCA) and internal carotid artery
Associated with other EOM defects
Accommodation affected
Aberrant regeneration
Holmes-Adie Tonic Pupil
Lesion in the ciliary ganglion
Bacterial/ viral infection
Mostly affects women (30s-40s)
No response to direct/consensual light reflex
Accommodative response impaired - N reduced
Due to denervation and supersensitivity
an enlarged pupil that constricts slowly in bright light:
WILL REACT TO 0.125% PILOCARPINE
or METACHOLINE CHLORIDE (2.5%)
parasympathetic dysfunction - ciliary ganglion involvement
Possible segmental iris palsies and reduced knee reflex
Horners syndrome
Characteristics: - PAREDINE - order neurone TEST & COCAINE
PTOSIS, MIOSIS, ANHYDROSIS
Additional characteristics
Heterochromia (congenital cases)
Apparent enophthalmos
Can be associated with contralateral IVth N (nuclear/fascicular) or VIth N (cavernous sinus)
Anisocoria increses in dim light
Cocaine (2-4%) dilates a nomal pupil but not a Horner’s !
1st (central), 2nd (Preganglionic) or 3rd (Post-ganglionic)order neuron lesion differential diagnosis
Differential diagnosis test: PAREDRINE (1% Hydroxyamphetamine) drops will fully dilate the pupil if 1st or 2nd order neuron lesion, but subnormal dilation if 3rd neuron.
Second Order neuron lesion- Pancoast’s tumour
can lead to horners
Argyll Robertson
Usually bilateral miotic pupils
May be asymmetrical
Poor dilation in the dark and to mydriatics
Light-Near dissociation
NO response to light
Responds to near target
Hallmark of neurosyphilis
Site of lesion: Region of the Sylvian aqueduct in the rostral midbrain
no diplopia
Afferent Pupillary Defect- (Marcus Gunn Pupil)
Some of the conditions that exhibit RAPD are:
Optic Neuropathy
Extensive retinal damage (Central retinal artery/vein occlusion, marked retinal detachment)
TED – optic nerve compression
Amaurotic pupil- “Blind Eye”
Mild RAPD- amblyopia
parasympathetic pathway - constriction
Parasympathetic Pathway
Retinal Ganglion Cells: Afferent signals originate here.
Synapse in Pretectal Nucleus: Axons diverge from the optic tract to the superior colliculus.
Edinger-Westphal Nucleus: Bilateral relay of information.
Third Nerve Pathway: Preganglionic fibers synapse in the ciliary ganglion.
Iris Sphincter Activation: Postganglionic fibers constrict the pupil.