P - Psychopathology
1/83
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
psychopathology definition
undesirable state producing severe impairment to a person’s social and personal functioning, often causing anguish
deviates from the social/statistical norms, causes distress to the individual and others
Definitions of abnormality
Deviation from social norms
Failure to function adequately
Deviation from ideal mental health
Statistical infrequency
Deviation from social norms
Norms: standards of behaviour that are regarded as acceptable within a given society
behaviour that doesn’t follow social patterns/rules; varies across cultures/eras
e.g. clinically abnormal: antisocial personality disorder (may lack conscience and behave aggressively as they experience little to no guilt)
Deviation from social norms - Strengths
strengths:
can help people as it highlights when its needed
distinguishes between normal and abnormal
protects society
Deviation from social norms - limitations
Limitations:
subjective - dependent on the society
change over time - often related to moral standards that vary over time as social attitudes change
human rights abuse - Szasz, mental illness used as a form of control
situational versus developmental norms
cultural relativism - must be views in the context of the culture it comes from
Failure to function adequately
Inability to cope with day-to-day life, caused by psychological discomfort
Rosenhan and Seligman 1989
Suffering → sense of loss
Maladaptive → prevents individual from achieving life goals
Vividness and unconventionality → way abnormal people behave in situations
Unpredictability and loss of control → inappropriate/uncontrolled behaviour
Irrationality and incomprehensibility → not always clear why they behave that way
Observer discomfort → when we see unspoken rules of social behaviour broken
Violation of moral and ideal standards → what happens if out of date?
global assessment of functioning → DSM-5
Failure to function adequately - Strengths
Strengths:
matches sufferer’s perspective → most seeking clinical help believe they are suffering
checklist → allows people to access their level of abnormality
accesses degree of abnormality → GAF scored on continuous scale
observable behaviour → allows judgement of others on whether someone is functioning
Failure to function adequately - Limitations
Limitations:
abnormality does not equal disfunction
subjective components (e.g. distress)
awareness → person may not realise abnormality of habits (e.g. hygiene)
Deviation from ideal mental health
when a person fails to strive for/achieve self-actualisation
Jahoda 1958
self attitudes → sense of identity/high self esteem
personal growth → extent of individual growth/development
integration → ability to cope with stress
autonomy → degree to which someone is independent of social influences
perception of reality → clear and not disturbed
environmental mastery → extent to which someone is successful and well-adapted
Deviation from ideal mental health - Strengths
Strengths:
positive approach to mental health
goal setting → identifies exactly what is needed to achieve normality
holistic → views individual as whole person rather than individual behaviours
Deviation from ideal mental health - Limitations
Limitations:
overdemanding criteria → self actualisation only achieved by few
subjective criteria → not clearly defined and dependent on self-report
changes overtime → religious visions=schizophrenia
collectivist societies → would reject autonomy as a criteria
Statistical Infrequency
Idea that certain behaviours are statistically rare within a population → dependent on normal distribution curve
statistical infrequency - Strengths
Strengths:
objective → once method of collection and ‘cut off point’ has been decided
overall view → provides data on what behaviours are infrequent within a population
no value judgements → not ‘wrong’, just less frequent
based on real, unbiased data
statistical infrequency - Limitations
Limitations:
not all infrequent behaviours are abnormal (e.g. high intelligence)
not all abnormal behaviours are infrequent (10% chronically depressed)
cultural factors - a behaviour may be normal/abnormal within different cultures
Phobias - definition
Anxiety disorder characterised by uncontrollable, extreme, irrational, and enduring fears - disproportionate to actual risk
10% of population
2:1=Female : Male
Phobias → behavioural symptoms
avoidant/anxiety response → confrontation=high anxiety response, efforts made to avoid
disruption of functioning → avoidance and anxiety so extreme they interfere with daily functioning
Phobias → emotional symptoms
persistent and excessive fear → due to presence/anticipation of feared stimulus
fear from exposure to phobic stimulus → overwhelmed, faint, aware but uncontrolled
Phobias → cognitive symptoms
irrational nature of thoughts → resistant to rational arguments
recognition of exaggerated anxiety → generally consciously aware
Types of phobias
simple phobias
social phobias
agoraphobia phobias
Simple phobias
Fear of specific things and environments
animal phobias (spiders)
injury phobias (blood)
situational phobias (flying)
natural environment phobias (water)
Social phobias
involves perception of feeling judged (F2FA and DFMH)
performance phobias (playing at concert/eating)
interaction phobias (dating/interview)
generalised phobias (others present)
Agoraphobia phobias
fear of leaving home/safe place
can be brought on by simple phobias
e.g. fear of contamination
Explanation for phobias
BEHAVIOURAL APPROACH via two process model
Acquisition (onset) → classical conditioning (traumatic experience)
Maintenance → operant conditioning (avoidance of fear = negative reinforcement)
Explanations for phobias - Behavioural approach limitations
Limitations:
reductionist and deterministic, internal processes ignored, not all trauma = phobias
tabula rasa → fear of falling
individual differences
could be vicarious
Treatments for phobias → systematic desensitisation
aims to extinguish undesirable behaviour ‘fear; by replacing it with a more desirable one ‘relaxation
reciprocal inhibition: process of inhibiting anxiety by substituting a competing response
identifying phobia/fear
learn relaxation techniques (progressive muscle relaxation
create hierarchy of fear (least to most)
work through hierarchy, learning to use relaxation techniques in presence of feared object
helps to unlearn maladaptive behaviours and replace them with adaptive → recondition
in vivo = real object, in vitro = imaginary
Treatment for phobias → flooding
straight to the top of hierarchy and imagine/have direct contact with most feared scenarios
cannot make usual avoidance responses peaks at such high levels it cannot be maintained and eventually subsides
Treatment for phobias → systematic desensitisation evaluation
Denholtz, Hall and Mann 1978 → 60% of clients treated for flying phobias continued to fly in 3.5yr follow up period
works better for some phobias not others (social and agoraphobia more improvement)
takes around 6-8 sessions
gives client control but therapist must first find source of anxiety
evidence that exposure therapy more effective
Treatment for phobias → flooding evaluation
Wolpe, girl forced into car and driven for 4hrs until hysteria eradicated
Rothbaum, used VS for exposure therapy, less harm and embarrassment
Depression → definition
Affective mood disorder involving lengthy disturbance of emotions (including feelings of despondency and hopelessness)
20% of population
women twice as vulnerable as men (post-natal, hormone fluctuations, more likely to report, societal aspects)
can occur in cycles, episodes generally lasting 2-6m
can begin in adolescence→ onwards, avg. age of onset in late 20s, decreased in last 50 yrs as rates increase
Depression → diagnosis
DSM-5
at least 5 symptoms apparent everyday for at least two weeks, w impairment to general functioning evident that is not accountable for by other medical conditions/events
Unipolar depression or major
without mania, only depression, more severe can have delusions and social impairment
25%F, 12%M
don’t respond well to anti-depressants, but combo of anti-depressants and anti-psychotics work
Unipolar depression → behavioural symptoms
loss of energy → fatigue/lethargy/inactivity
social impairment → reduced official interactions
weight changes → significant decreases/increases
poor personal hygiene → reduced incidence of washing
sleep pattern disturbance → insomnia/oversleeping
Unipolar depression → Emotional symptoms
loss of enthusiasm → lessened concern/pleasure
constant depressed mood → overwhelming sadness
worthlessness → constant reduced worth/guilt
Unipolar depression → cognitive symptoms
delusions → generally guilt, punishment, disease
reduced concentration → attention/indecisive
thoughts of death → death/suicide
poor memory → poor retrieval
Bipolar depression or manic
two types: OR diathesis stress model → vulnerability+events=dep
endogenous depression → related to internal biochemical and hormonal factors
exogenous depression → related to stressful life experiences
less common → 2% equally divided between sexes
onset usually from 20-50
mixed episodes of mania and depression
mania: intense but inappropriate elation = hyperactivity, distractibility, excessive talking, disruptive thought processes
Bipolar depression → behavioural symptoms
high energy levels → high social and sexual
reckless behaviour → risk taking and dangerous
talkative → fast, endless speech without regard for others
Bipolar depression → emotional symptoms
elevated mood states → constant and intense euphoria
irritability → frustrated if they don’t get their way
lack of guilt → social inhibition and lack of guilt
Bipolar depression → cognitive symptoms
delusions → and grandiose, can believe others are persecuting them
irrational thought processes → reckless thinking
Explanations of depression - cognitive
generally in terms of faulty/irrational though processes and perceptions, focus on maladaptive cognitions
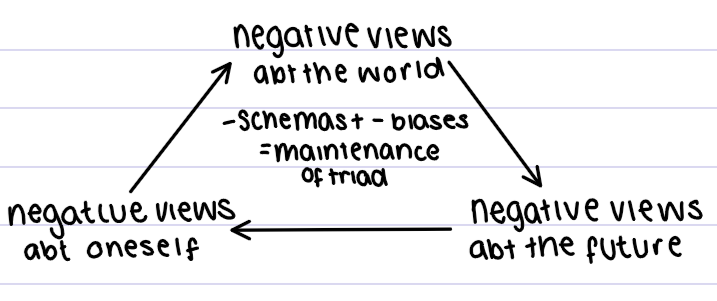
Beck 1976 → cognitive triad
believed people become depressed because world is seen through negative schemas which dominate thinking, triggered when in situation to how learned
schemas develop in childhood and adolescence, when authority figures place unrealistic demands
negative schemas fuelled by cognitive biases → misperceive reality
Beck 1976 → types of schemas
Ineptness schema
Self-blame schema
Negative self-evaluation schema
Ineptness schema
depressives expect to fail
Self-blame schema
depressives feel responsible for all misfortune
Negative self-evaluation schema
constant reminder of worthlessness
Beck 1976 → cognitive biases
Arbitrary inference
Selective abstraction
Overgeneralisation
Magnification and Minimisation
Arbitrary inference
conclusions drawn in absence of sufficient evidence
Selective abstraction
conclusions drawn from just one part of a situation
Over-generalisation
sweeping conclusions based on single event
Magnification and minimisation
exaggeration in evaluations of performance
Ellis’ ABC model
believed depressives mistakenly blame external events for unhappiness, interpretation of events and distress
Activating event → something happens in environment
Beliefs → what you think about the event
Consequences → emotional/behavioural response
activating event triggers untrue emotion, consequentially have negative view of themselves and lack of confidence
Evaluation of the cognitive explanation for depression
McIntosh and Fischer challenge Back as they tested the three elements and found no clear separation
Boury et al. found depressives misinterpret facts and experiences in a negative way and feel hopelessness about the future
less success in explaining and treating manic component
other aspects (e.g. genes) considered → not rlly cog.
high success when treating depression with cognitive therapies → deny causation as thought and depression are more bidirectional
Explanations of depression - biological
hereditary
Plomin gene mapping of other 3000 12yr old twins, genetics for 66% of hereditability of cognitive abilities (key feature of depression)
Wender, depressed adopted children, generally had depressed biological parent
Explanations of depression - behavioural
learned
Lewinsohn → negative life events leads to a decrease in positive reinforcements and learned helplessness
or social learning theory
Depression → rational thoughts
based on reality → individual seeing things as they really are, allows individual to achieve goals and real full potential, only experience emotions they can handle
Depression → irrational thoughts
distorts idea of reality → blocks/stops you from achieving goals and life purposes
→ extreme emotions which persist and cause distress → harmful to self and others
Treatment of depression → Cognitive behavioural therapy
main psychological treatment, central idea behind is that beliefs, expectations and cognitive biases affect self perception and approach to problems
Two main:
Rational Emotive Behavioural Therapy (REBT), based on Ellis’ ABC model
Treatment of Negative Automatic Thoughts (TNAT), based on cog. triad, schemas, biases
central idea of both is to challenge and restructure maladaptive ways of thinking into adaptive
Kendall and Hammen → clarify, change and challenge both cognitive and behavioural processes (challenge interpretive bias)
Treatment of depression → Beck 1976 CBT
reality testing, more than just replacement of negative to positive, emphasises homework and hypothesis testing
predictions=pessimistic, fear=groundless
~20 sessions over 16 weeks
Strategies:
behavioural activation (identify fun activities and do them)
graded homework (practice new ways of thinking)
though catching
cognitive reconstruction
problem solving (find root and test it)
Treatment of depression → REBT procedure
Reframing → challenge through reinterpretation, 1-2 sessions per week over 15 weeks, therapist and client work together
Educational → learn relationship between thoughts, emotions and behaviour
Behavioural activation and pleasant event scheduling → increase physiological activity and participation
If improvement in mood and activity = opportunity to challenge thoughts
given goals between sessions
hypothesis testing of negative thoughts through behavioural coping skills
Treatment of depression → drug therapy
Antidepressants have physical affect of increasing serotonin production
selective serotonin reuptake inhibitors (common→fluoxetine)
Treatment of depression → evaluation of CBT
Hollon et al. 40% of moderately to severely depressed patients treated with CBT for 16w relapsed within the following 12m → 45% w drug, 80% for placebo
Department of Health 2011, reviewed treatments and found CBT to be most effective, but didn’t endorse use alone
trained therapists essential to effectiveness → ethical concerns as easy to abuse for dependence
many believe thought process and depression to have a bidirectional relationship
relatively short time frame for long term benefits (cost effective)
unsuitable for patients who lack focus, may enhance symptoms instead
OCD → definition
characterised by persistent, recurrent, unpleasant thoughts and/or repetitive, ritualistic behaviours
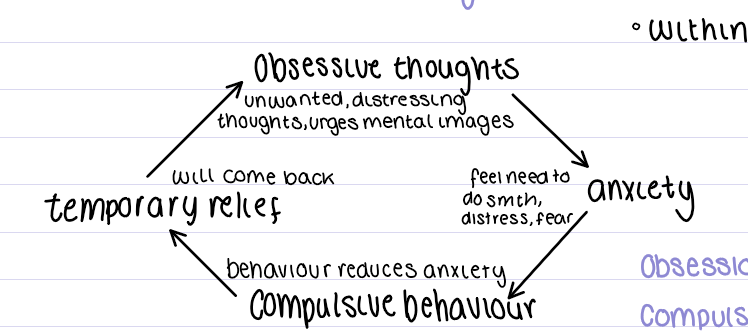
OCD thought cycle and population
obsessions and compulsions are very time consuming and therefore interfere with ability to conduct everyday activities
2% of population, no real gender differences in rate but present in types
F: contamination and cleaning
M: religious and sexual
M have an earlier onset, with more gradual but severe symptoms
Obsessive-Compulsive and related disorders in the DSM-5
OCD
Hoarding disorder: compulsive gathering of possessions and inability to part
Trichotillomania: compulsive hair pulling
Excoriation: compulsive skin pulling
Obsession vs Compulsion
O: forbidden/inappropriate ideas and visual images that aren’t based in reality
C: intense, uncontrollable urges to repetitively perform tasks and behaviours to reduce distress
Obsessions: Behavioural symptoms
Hinder everyday functioning → obsessive ideas of forbidden/inappropriate type creates anxiety
Social impairment → anxiety levels generated so high, limits ability to conduct meaningful interpersonal relations
Obsessions: Emotional symptoms
extreme anxiety → persistent inappropriate thoughts or persistent inappropriate/forbidden ideas create excessively high levels of anxiety
Obsessions: Cognitive symptoms
Recurrent and persistent thoughts → constantly repeated obsessive and intrusive thoughts
Recognised as self generated → most understand thoughts and images are self-invented
Realisation of inappropriateness → understand but cannot consciously control
Attentional bias → perception focused on anxiety generating stimuli
Common obsessions
contamination
fear of losing control
perfectionism
religion
Compulsions: behavioural symptoms
Repetitive → feel compelled to repeat behaviours in response to obsessions
Hinder every day functioning and social impairment
Compulsions: Emotional symptoms
distress → recognition that compulsion behaviours cannot be consciously controlled = strong feeling of distress
Compulsions: Cognitive symptoms
uncontrollable urges → feel they will reduce anxiety
realisation of inappropriateness
Common compulsions
excessive washing and cleaning
excessive checking
repetition
mental compulsions
hoarding
OCD diagnosis
presence of obsessive and compulsive symptoms on most days for 2 weeks
Explanations of OCD: biological approach
determined by physiological means with treatments based on chemical means
also called the medical model, two explanations:
hereditary influence of genetics
damage to neural mechanisms
Explanations of OCD: Genetic
Lewis 1936 → 37% had parents with OCD, 21% had siblings with OCD hence suggesting genetic vulnerability
Nestadt et al. 2010 → reviewed twin studies, 68% of MZ twins shared OCD, support genetic influence
unlikely single gene causes OCD, but combination (polygenic) - Taylor 2013 up to 230 different genes involved
COMT gene → regulates breakdown of dopamine implicated in OCD, decreased activity of gene=increased levels of dopamine
SERT gene → affects transport of serotonin, decreased activity=decreased serotonin
Explanations of OCD: Neural
link to breakdown of immune system functioning
PET scans show high levels of activity in orbital frontal cortex
abnormal brain circuits
abnormal serotonin levels
Neural explanations of OCD: immune system
(e.g. strep throat) → Lyme disease and influence (often why onset seen in children)
Neural explanations of OCD: orbito-frontal cortex
associated with higher level thought processes and conversion of sensory information
help initiate activity upon receiving impulse to act and stop when lessened
difficulty switching off impulses → obsessions
Neural explanations of OCD: abnormal brain circuits
areas of frontal lobe abnormal
caudate nucleus normally supresses signals from OFC (sends signal to thalamus about worry)
if caudate nucleus damaged, fails to supress minor worry signals
Neural explanations of OCD: abnormal serotonin levels
high dopamine and low serotonin, SSRIs reduce OCD symptoms (block reabsorption)
Treatments for OCD → Drug therapy
antidepressants, e.g. SSRIs, elevate serotonin allowing the OFC to function at normal levels
most common → Prozac for adults, Sertaline for 6yr olds, Fluvoxamine for 8yr olds and older
Julien 2007, SSRIs show (although symptoms do not fully disappear) between 50-80% of OCD patients improve to live semi-normally
ONLY GIVEN IF SSRIs INEFFECTIVE:
anxiolytic drugs → anxiety lowering properties (e.g. benzodiazepines, slows CNS)
antipsychotic drugs → dopamine lowering effect
Treatments for OCD → Psychosurgery
last resort, involves destroying brain tissue to disrupt cortico-striatal circuit by use of radiofrequency waves, effects OFC, thalamus, and caudate nucleus = decrease in symptoms
recent movement towards using deep brain stimulation
relatively small success rate with serious side effects that can’t be undone, acceptable only for severe forms when no response to other treatments
10% of patients with OCD get worse overtime, even with drug treatments
Treatments for OCD → CBT
focus on changing obsessional thinking to reduce anxiety created (HIT relive → repeated exposure),
come to understand thought and action are not the same through realistically accessing risk
encouraged to disregard former maladaptive ones
most effective with drug treatments
Treatments for OCD → Evaluation
Pitcher 2004, had 35% decrease of symptoms after surgery; complications → seizures, but were at risk of suicide so relative success
O’Conner 1999, 3 conditions (drug, CBT, combo), most success with drug and CBT combo