B5 Path E1 PQs
1/108
Earn XP
Description and Tags
Robbins Review, quizzes
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
109 Terms
A 68-year-old man presented with a painless white patch over the edentulous mandibular gingiva. He had a 50-year history of heavy smoking, and a history of alcoholism. A biopsy was taken and the microscopic appearance is shown in the attached figure. What is the most likely diagnosis in this patient?
Erythroplakia
Squamous cell carcinoma
Verrucous carcinoma
Leukoplakia
Pyogenic granuloma
A 32-year-old woman presented in early May 2019 with the chief complaint of blisters and ulcers on her lower lip for the past two days. She reported a history of fever three days earlier, which was followed by appearance of blisters on the inner and outer side of her lower lip. Most of the intraoral blisters ruptured in two days. There was history of similar lesions two times in the past, in early April 2019 and late February 2019, which were healed within a week without taking any medication. There was no history of similar lesions elsewhere on the body especially genital, eye or on skin. On physical examination, multiple vesicles with scab formation, few millimeters in size were present below vermillion border of lip and on lower labial mucosa surrounded by an erythematous area. Ulcers were mildly tender on palpation. Bilateral submandibular lymphadenopathy was also noted. The base of the large ulcer was scraped with a spatula and sent to a pathology laboratory. What would a histopathological examination most likely show?
Intranuclear inclusion bodies in keratinocytes
Hyphae and neutrophils within the stratified squamous epithelium
Mononuclear inflammatory cells within small vessel walls
Dysplastic changes
Enlarged and swollen keratinocytes with cytoplasmic clearing
Intranuclear inclusion bodies in keratinocytes
A 60-year-old woman presented with a main complaint of a mass on the right side of her tongue. For the last four months she observed a lump on the tongue displaying alarming growth over a three week period. The lesion was painful when the patient moved her tongue or while eating. The patient was a lifelong smoker who smoked 20 cigarettes a day for the majority of her adult life. On intraoral examination, a 1.5 x 2.0 x 1.5 cm exophytic mass was found in the middle third position of the right lateral border of the tongue. The mass showed a central ulcer appearing to infiltrate the tongue musculature. Enlarged lymph nodes were palpable in her neck on both sides. A biopsy under local anesthesia was carried out. What would histopathological examination most likely show?
Full-thickness dysplasia of the stratified squamous epithelium
Round laminated eosinophilic structures in the center of tumor cell nests
Warty-like papillomatosis
Highly cellular spindle cell proliferation in herringbone pattern
Hyperplastic stratified squamous epithelium with elongated rete ridges
Round laminated eosinophilic structures in the center of tumor cell nests
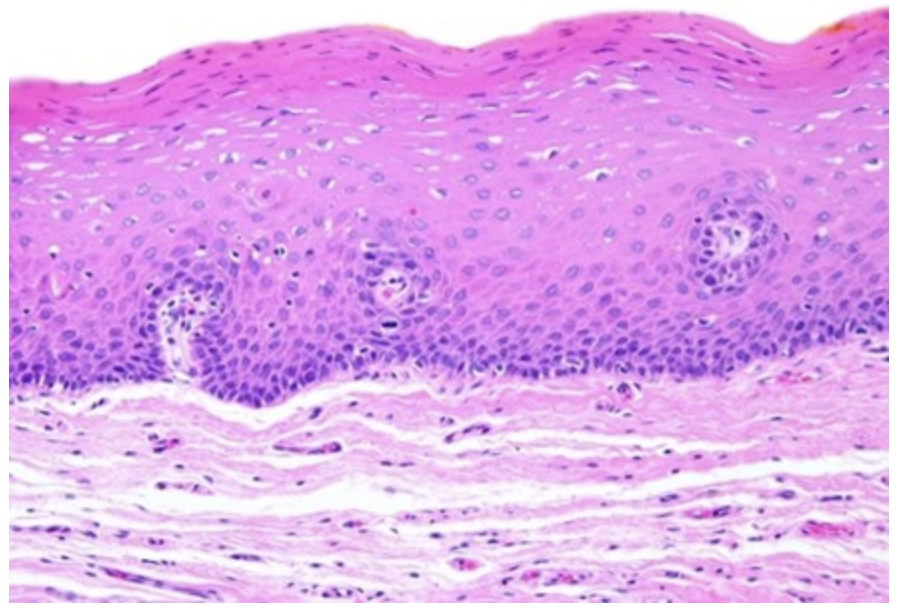
An 84-year-old woman presented to oral surgery center with chief complain of an asymptomatic, white intra-oral growth, associated with discomfort during mastication. Oral examination revealed a thickened whitish plaque with a warty surface (1.5 x 1.5 cm) in the hard palate. A biopsy revealed a stratified squamous epithelium with marked surface keratinization. The well-differentiated proliferating epithelium showed large and bulbous rete ridges that invaded lamina propria in a pushing manner. The epithelial cells exhibited minimal pleomorphism and minimal mitotic activity. The underlying connective tissue of lamina propria showed infiltration of numerous inflammatory cells. Which of the following features would most accurately characterize this tumor type?
It is a high-grade variant of oral squamous cell carcinoma
It occurs primarily in smokeless tobacco users
Has a unique predilection for bone metastases
The recommended treatment is surgical excision associated with radical neck dissection
It is the most common histologic type of oral malignancy followed by squamous cell carcinoma
It occurs primarily in smokeless tobacco users
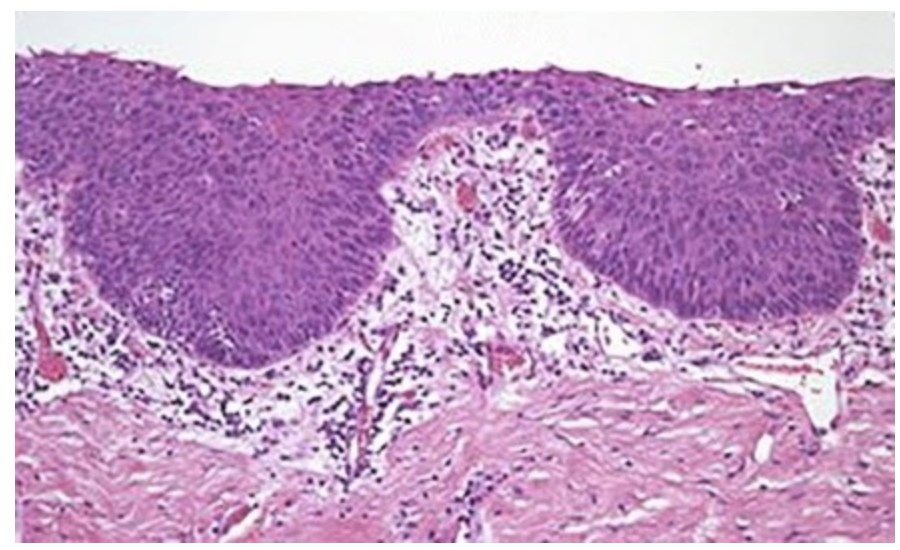
A 62-year-old man visited the dental clinic for restorative consultation regarding his failing maxillary dentition. The patient had not seen the dentist in many years. During his comprehensive oral examination, the periodontist discovered an asymptomatic red, macular lesion on the left posterior hard palate, 1.5 × 1.5-centimeter in diameter. The patient was not wearing a denture, and no other obvious source of irritation could be identified. A 30-year history of smoking was elicited. An incisional biopsy of the palatal lesion was performed, and the microscopic appearance is shown in the attached figure. What is the most likely diagnosis?
Erythroplakia
Squamous cell carcinoma
Verrucous carcinoma
Aphthous stomatitis
Pyogenic granuloma
Erythroplakia
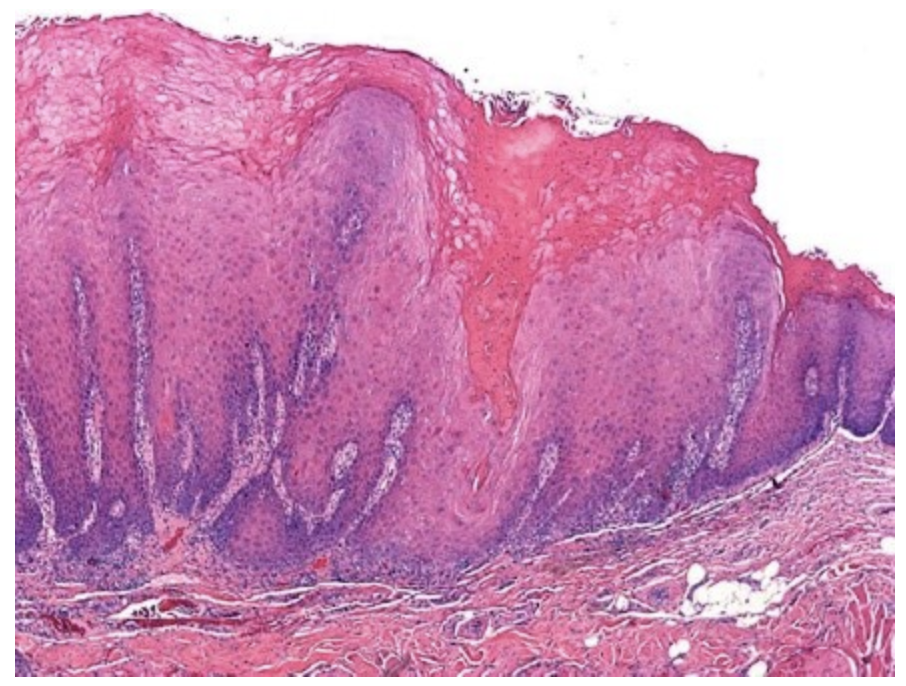
A 65-year-old man presented with a chief complaint of painless growth on the right corner of the mouth for the last two years. The patient had a history of tobacco chewing 3-4 times a day for the last 30 years. On physical examination, an exophytic, white mass was seen intra orally involving the right buccal mucosa and extending extra orally to the corner of mouth. The lesion was approximately 4 x 4 cm in size, well-defined and elevated from adjacent mucosa with irregular and firm margins. An incisional biopsy of the mass was performed. The microscopic appearance of the biopsy specimen is shown in the attached figure. Which of the following is the most likely diagnosis?
Erythroplakia
Oral hairy leukoplakia
Pyogenic granuloma
Squamous cell carcinoma
Verrucous carcinoma
Verrucous carcinoma
A study was designed to determine the frequency of histological types of salivary gland tumors. Salivary gland biopsy slides from the files of the Department of Oral Pathology of University of California San Francisco Medical Center from 1990 to 2018 were retrieved and reexamined. These included 713 consecutive cases of primary salivary gland tumors. The microscopic slides were reexamined and the histopathological diagnosis was reconfirmed according to the 2017 WHO classification. The frequency of different benign and malignant salivary tumors in both major and minor glands was analyzed. Which of the following would most likely be identified as the most common salivary gland tumor in this study?
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Warthin tumor
Pleomorphic adenoma
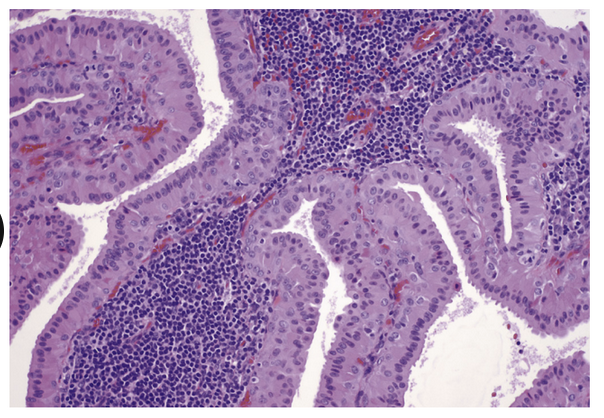
A 47-year-old woman is admitted with a two-month history of pain localized in the right cheek. On physical examination, an elastic hard mass in the right retromandibular region is revealed. Head and neck magnetic resonance imaging (MRI) shows a well-defined tumor of 3.2 cm in size in the deep lobe of the right parotid gland. A right total parotidectomy with identification and preservation of the facial nerve is performed. The microscopic appearance of the tumor is shown in the attached figure. The diagnosis is:
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Warthin tumor
Warthin tumor
A 50-year-old woman is admitted complaining about a painless swelling in the left submandibular region for the past eight months. The swelling had been gradually increasing in size and not associated with constitutional symptoms nor related to food. On physical examination, a solitary spherical swelling of 4 cm diameter is noted. The swelling is tender, immobile, firm, and adherent to the underlying structures. The skin over the swelling is indurated. The submandibular lymph nodes on the left side are enlarged. Surgical excision of the mass is performed under anesthesia. The microscopic appearance of the tumor is shown in the attached figure. The diagnosis is:
Acinic cell carcinoma
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Warthin tumor
A 68-year-old man presents with complaints of pain and swelling of the right submandibular region. The patient reports that he noticed swelling in this region about four years earlier and then again two years earlier but did not seek professional medical attention at these times. The patient admits that he thought he should seek medical attention only when the gradually enlarging lesion had recently become painful. Physical examination reveals a tender swelling localized to the right submandibular region with a hard consistency. Absent salivary flow from the right Wharton’s duct is also noted. A hard, white material is felt by palpation at the ostium of the right Wharton’s duct. A plain X-ray shows a radiopaque mass in the right submandibular gland. The right submandibular salivary gland was surgically excised and an impacted sialolith measuring approximately 4 x 2 cm was removed. Which of the following is most likely to be present in the histopathologic examination of the excised submandibular gland parenchyma?
Cavities not lined by epithelium containing mucin
Diffuse lymphocytic infiltration, interstitial fibrosis, squamous metaplasia of duct epithelium.
Ducts lined by columnar cells in a myxoid and chondroid stroma
Edema, hyperemia, bacteria, increased numbers of neutrophils, and abscesses.
Extensive lymphocytic cell infiltration with atrophy of secretory acini
Diffuse lymphocytic infiltration, interstitial fibrosis, squamous metaplasia of duct epithelium.
A 53-year-old woman presented with 7-year history of dryness of eyes and one-year history of dryness of mouth. The patients also reported pain of her proximal metacarpophalangeal joints (MCP) and proximal interphalangeal joints (PIP) that was worse in winter. She also gave a history of few episodes of purplish discoloration of the skin of her lower extremities. Physical examination showed bilateral parotid gland enlargement, and tenderness and swelling of the PIP and MCP joints. A nonblanching purpuric rash was present on her bilateral lower extremities from toes up to her knees. Which of the following is the most appropriate diagnostic study at this time?
Antinuclear antibody
Anti-Ro antibodies
Complete blood count
Erythrocyte sedimentation rate
Rheumatoid factor
Anti-Ro antibodies
A 21-year-old woman complaining of a large cystic swelling in the left side of her neck was referred to a dental surgeon by her primary care provider. No dental pathology was identified, and the patient was referred to the ear, nose, and throat department. The swelling had been present for approximately three months; it exhibited no change with eating, chewing, or swallowing. There had been no discharge. On examination a nontender, diffuse, cystic mass could he seen and felt in the left submandibular area. Routine laboratory studies and the thyroid panel were within normal limits. Contrast-enhanced CT scan demonstrated a large rim-enhanced fluid attenuation mass occupying the left sublingual space. The patient underwent a left neck surgical exploration. A multilobated cystic lesion, deep to the platysma and wrapped around the sublingual gland was discovered. The cyst was excised along with extirpation of the left sublingual gland. At surgery, the cystic lesion was found to be filled with a viscous and yellowish fluid. Histopathological evaluation revealed a cavity filled with mucin and lined by connective tissue with inflammatory cells. Which of the following is the most likely diagnosis?
Ranula
Mucocele
Mucoepidermoid carcinoma
Primary Sjögren syndrome
Acute bacterial submandibular sialadenitis
Ranula
A 6-month-old girl presents with a history of pain in abdomen, vomiting and constipation of 8 days duration. On examination there is diffuse abdominal distension, however no abdominal mass is palpable. Results of laboratory investigations are unremarkable. Abdominal ultrasound and abdominal CT scan show a giant abdominal cystic mass. Exploratory laparotomy confirms a cystic mass in abdominal cavity along the mesenteric border of ileum situated 20 cm proximal to the ileocecal valve, measuring about 20 × 5 cm in size. The cystic mass is removed together with the adjacent ileum. Closer examination shows that the proximal portion of the cystic mass is blind end and the distal portion communicates with the ileum. Microscopically, sections from the cyst wall disclose a well-preserved tunica muscularis propria, tunica submucosa, tunica muscularis mucosae and a typical ileal mucosa. Which of the following is the most likely diagnosis?
Intestinal duplication
Intestinal atresia
Omphalocele
Malrotation with volvulus
Colojejunal fistula
Intestinal duplication
A study was designed to determine the spectrum of variations that can occur in congenital esophageal atresia and tracheoesophageal fistula. Medical records of 181 newborns admitted for management of congenital esophageal atresia in the Pediatric Surgical Center, Seattle were reviewed. The anatomy of each variant was carefully reviewed based on the surgical findings. Which of the following is most likely to be identified as the most common variant of congenital esophageal atresia and tracheoesophageal fistula in this study?
Isolated esophageal atresia without tracheoesophageal fistula
H-type tracheoesophageal fistula with no atresia
Esophageal atresia with proximal and distal tracheoesophageal fistula
Esophageal atresia with proximal tracheoesophageal fistula
Esophageal atresia with distal tracheoesophageal fistula
Esophageal atresia with distal tracheoesophageal fistula
A male neonate was delivered by cesarean section at 35 weeks’ gestation with a birth weight of 2,140 g. At birth, the infant had difficulty swallowing. Feeding produced severe coughing spells and choking. He was intubated and subsequent passage of a nasogastric tube was unsuccessful. The initial x-ray showed a gasless abdomen and a high thoracic position of the nasogastric tube. Which of the following is the most likely diagnosis?
Achalasia
Diaphragmatic hernia
Infantile hypertrophic pyloric stenosis
Esophageal atresia
Zenker diverticulum
Esophageal atresia
A two-month-old male infant was brought to the emergency department with a four-day history of frequent vomiting occurring shortly after breastfeeding. The vomiting was forceful, ejecting the stomach content to a distance. The baby had an uncomplicated, term, vaginal delivery with a birth weight of 3.7 kg (8.1 pounds). The child’s parents denied any recent fever, coughing, or other complaints. Physical examination revealed bilaterally clear breath sounds, bowel tones in all quadrants, and a soft, non-tender abdomen. A small, moveable, oval mass was palpated in the child’s epigastric region. The patient was breastfed in triage. He appeared hungry and very eager to feed. Three minutes after breastfeeding, the patient experienced forceful vomiting of the recently consumed breast milk. Which of the following is the most likely diagnosis?
Achalasia
Diaphragmatic hernia
Infantile hypertrophic pyloric stenosis
Esophageal atresia
Zenker diverticulum
Infantile hypertrophic pyloric stenosis
A two-week-old, full-term boy was seen in the clinic with a three-day history of yellow colored drainage coming from the umbilicus. He was feeding well and seemed appropriate for his age. Physical examination revealed an alert, active, and well-developed infant. Vital signs were normal. The heart, chest, extremities, skin, and neurologic examination were grossly normal. The abdomen was nontender and nondistended. There was a yellow, soft substance emerging from the umbilicus with minimal erythema and tenderness at the umbilicus. A barium enema was obtained to evaluate the intra-abdominal anatomy and the discharge from the umbilicus. The retrograde filling of the small bowel with radiopaque contrast material revealed a fistulous connection from the umbilicus to a segment of the small bowel located 30 cm proximal to the ileocecal valve. The contrast streamed out of the umbilicus onto the anterior abdominal wall. Which of the following is the basic defect that explains this infant’s clinical and radiological findings?
Umbilicoileal fistula
Omphalomesenteric duct sinus
Omphalomesenteric cyst
Atrophic omphalomesenteric duct
Meckel diverticulum
Umbilicoileal fistula
A 17-year-old athletic young man presented with a history of acute onset of massive hematochezia resulting in syncope. He underwent multiple blood transfusions and endoscopic examination of the upper and lower gastrointestinal tract, with no success in finding the source of bleeding. At the time of admission, the patient had a hemoglobin level of 10 g/dL (normal: 12-17 g/dL) and a hematocrit level of 30% (normal: 37%-49%). Physical examination findings were unremarkable, and the abdomen was soft, nontender, and non-distended. CT scan of the abdomen and pelvis after administration of oral and intravenous contrast agents showed a tubular structure with central hypodensity communicating with the small bowel above the bladder. This was thought to represent blood within the small bowel lumen. At laparoscopy, a pouch measuring 10 cm in length and about the size of a finger in diameter was found on the antimesenteric border of the ileum. The distance separating it from the ileocecal valve was 40 cm. The pouch was resected and the tissue specimen sampled for pathologic analysis showed small-bowel mucosa with presence of focal areas of heterotopic gastric mucosa. Which of the following is the most likely diagnosis?
Meckel diverticulum
Atrophic omphalomesenteric duct
Ileal duplication
Mallory-Weiss syndrome
Esophageal varices
Meckel diverticulum
A 21-year-old woman presented with chief complaint of epigastric pain. Upper endoscopy showed a hyperemic antral gastric mucosa without mucosal atrophy, and biopsies were taken from the lesser curvature of the antral region, gastric body, and gastric fundus. Biopsy specimens of the lesser curvature of the antral region showed a lymphocytic and plasma cell inflammatory infiltrate confined largely to mucosa occupied by gastric pits. The surface epithelium was infiltrated by a few neutrophils. Biopsy specimens from the body and fundus showed no pathological changes. Which of the following is the most likely diagnosis?
Acute H. pylori gastritis
Autoimmune gastritis
Chronic H. pylori gastritis
Eosinophilic gastritis
Lymphocytic gastritis
Chronic H. pylori gastritis
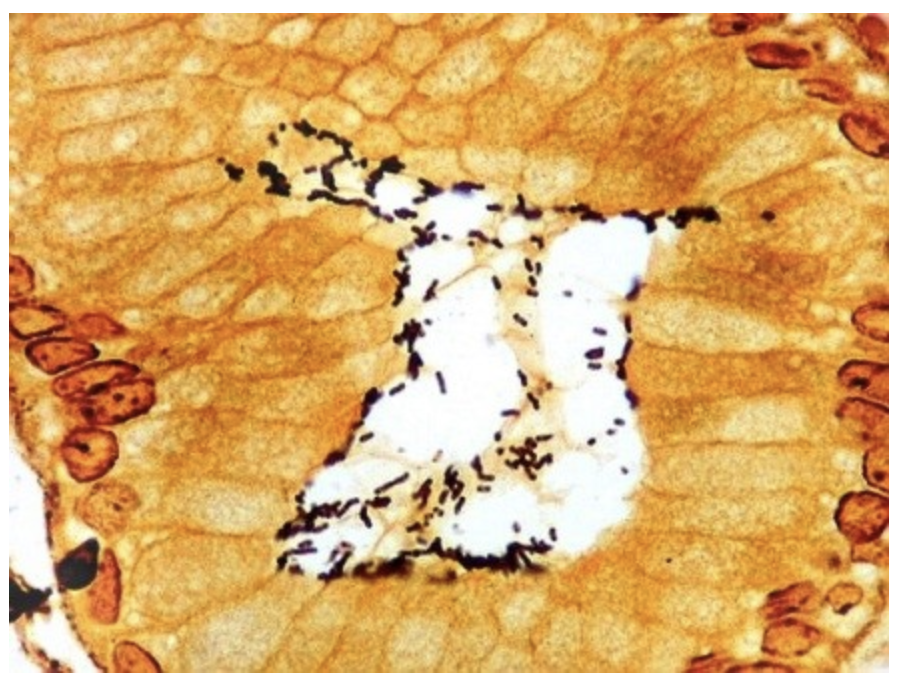
A 40-year-old woman presented with persistent epigastric pain of several months. She reported three episodes of vomiting without diarrhea. The physical examination showed no pathological findings other than a mild tenderness in the upper left abdomen. Upper endoscopy revealed an erythematous antral mucosa. The microscopic appearance of a gastric biopsy specimen stained with Warthin-Starry is shown in the attached figure. Which of the following is the most likely diagnosis?
Chronic H. pylori gastritis
Autoimmune gastritis
Reactive gastropathy
Stress gastropathy
Ménétrier disease
Chronic H. pylori gastritis
A 56-year-old woman presented with generalized fatigue and new onset dyspnea on exertion of three-week duration. The patient had been diagnosed with myasthenia gravis four years previously after which pyridostigmine treatment was initiated. On admission, her vitals and physical examination were normal except for a heart rate of 132 beats per minute, and pale conjunctiva. Laboratory studies revealed low hemoglobin and low hematocrit. Her peripheral blood smears disclosed megaloblastic anemia. Further anemia workup revealed a vitamin B12 deficiency at 60 pg/mL (normal: 250–950 pg/mL). Upper endoscopy showed atrophic mucosa in the gastric body. Urea breathing test was negative. Which of the following histopathological lesions are most likely to be seen in a biopsy from the gastric body?
Elongated gastric pits with a corkscrew appearance.
Eosinophils diffusely infiltrating the gastric wall from mucosa to serosa.
Lymphocytes and plasma cells infiltrating lamina propria from the surface epithelium to the muscularis mucosae and in between antral type tubular glands.
Lymphocytes, plasma cells, and neutrophils infiltrating the superficial lamina propria occupied by gastric pits.
Marked congestion of dilated capillaries and veins in mucosal and submucosal layers in the absence of any inflammatory cell infiltrate.
Lymphocytes and plasma cells infiltrating lamina propria from the surface epithelium to the muscularis mucosae and in between antral type tubular glands.
A 40-year-old woman underwent upper gastrointestinal endoscopy for screening purposes. Six months prior to screening, she had been diagnosed with adult-onset type 1 diabetes mellitus. She was receiving insulin therapy for type 1 diabetes mellitus but had not been prescribed proton-pump inhibitors. Upper endoscopic examination revealed small nodules deep in the body and fundus mucosa. Multiple biopsies were taken from the gastric antrum, body, and fundus. Histopathological examination of the biopsy specimens taken from the lesser curvature of the gastric antrum revealed no atrophy or inflammation, whereas biopsy specimens from the greater curvature of the gastric corpus exhibited uneven infiltration of plasma cells and lymphocytes involving the full thickness of the lamina propria. Which of the following laboratory studies is most likely to confirm the diagnosis?
Blood test for antibodies to H. pylori.
Blood test for antiparietal autoantibodies.
Gastric acid secretion test
Gastrin test
Total serum protein test
Blood test for antiparietal autoantibodies.
A 42-year-old man presented with a two-month history of abdominal discomfort, anorexia, and weight loss. An upper endoscopic examination showed a 3 × 7 cm ulcerated mass, located 50 cm from the incisors, in the distal gastric antrum. The mass was confirmed on endoscopic ultrasound which also revealed the presence of gastrohepatic lymphadenopathy measuring up to 1.6 cm in maximum diameter. A gastric biopsy was performed, and the microscopic appearance of the biopsy specimen is shown in the attached figure. Molecular studies of tumor cells would most likely reve al abnormalities in which of the following genes encoding?
Adenomatous polyposis coli
β-catenin
E-cadherin
P16 protein
P53 protein
E-cadherin
A 58-year-old man was admitted with upper abdominal dull pain that had persisted for one month. The patient had no relevant past medical history. The results of the physical examinations were unremarkable. Laboratory investigation showed that the patient’s serum carcinoembryonic antigen was elevated to 1945 mcg/L (normal: 0-2.5 mcg/L). An upper endoscopic examination revealed a large fungating mass with a central ulceration at the lesser curvature extending from the angle to the antrum of the stomach. CT scan of the abdomen and pelvis revealed thickening of the wall of the antrum, enlarged lymph nodes at the lesser curvature, and multiple hepatic metastases. A gastric biopsy was performed, and the microscopic appearance of the biopsy specimen is shown in the attached figure. Molecular studies of tumor cells would most likely reveal abnormalities in which of the following genes encoding?
Adenomatous polyposis coli
β-catenin
E-cadherin
P16 protein
P53 protein
A 44-year-old woman presented to a community hospital with melena, weakness, and orthostatic dizziness. She reported a six-month history of rhythmic burning pain in the epigastric abdomen that occurred about 90 minutes after meals. Physical examination revealed stable vital signs, pallor, and a benign abdominal examination. Rectal examination revealed melena and no visible hemorrhoids. Laboratory studies on admission revealed a hemoglobin of 4.1 g/dL (normal: 10-16 g/dL), leukocyte count of 7,500 cells/mm3 (normal: 4,000-10,000 cells/mm3) with a differential count of 60% neutrophils, 25% lymphocytes, 10% monocytes, and 5% eosinophils (normal: neutrophils 40-73%, lymphocytes 20-44%, monocytes 3-13%, and eosinophils 0-6%). Platelet count was 200,000 cells/mm3 (normal: 140,000-400,000 cells/mm3). Her renal and liver functions, and coagulation panel were within normal limits. What is the most likely cause of melena in this patient?
Mallory-Weiss syndrome
Peptic ulcer disease
Esophageal varices
Gastric adenocarcinoma
Eosinophilic esophagitis
Peptic ulcer disease
A 20-year-old man was admitted for severe third-degree burns. He had sustained 45% total body surface area burns over his anterior trunk. Escharotomy was performed associated with skin grafting over his anterior trunk on the 5th admission day. In the immediate post-operative period, he developed acute hematemesis, vomiting 180 mL of fresh blood. He became hypotensive, and his hemoglobin level decreased to 7 g/dL compared with 17 g/dL preoperatively. Upper endoscopy revealed numerous bleeding erosions along the fundus and body of the stomach and numerous blood clots. Which of the following is most likely to explain this patient’s gastrointestinal bleeding?
Peptic ulcer disease
Esophageal varices
Cushing ulcers
Curling ulcers
Zollinger-Ellison syndrome
Curling ulcers
An 8-month-old boy was admitted with 10 days of progressive vomiting. On neurological examination, the patient was lethargic and irritable, with an upgaze palsy. Head MRI revealed a 3 cm-diameter heterogeneously enhancing posterior fossa mass centered within the floor of the fourth ventricle associated with peritumoral edema. The patient underwent suboccipital craniotomy for resection of the tumor. The results of the intraoperative frozen section were consistent with medulloblastoma, grade IV. On postoperative day 2, the patient had melena and his hematocrit fell from 36% postoperatively to 17.3% (normal: 31-41%). Upon further questioning, the family reported a 3-month history of occasional coffee-ground emesis and melena prior to admission. There was no history of burn, sepsis, major trauma, or prior medication ingestion. The patient was transferred back to the pediatric intensive care unit where he underwent transfusion with packed red blood cells. Upper gastrointestinal endoscopy revealed several large hemorrhagic erosions in the duodenal bulb and descending part of duodenum. Which of the following is most likely to explain this patient’s gastrointestinal bleeding?
Peptic ulcer disease
Cushing ulcers
Curling ulcers
Esophageal varices
Mallory Weiss syndrome
Cushing ulcers
A 44-year-old man presented with a 4-week history of epigastric pain, nausea, vomiting, and generalized edema resulting in an 18-pound weight loss since symptom onset. Physical examination on admission showed bilateral pitting edema up to his knees. His cardiac and pulmonary examination were normal. Laboratory studies were all normal except for serum albumin which was 1.8 mg/dL (normal: 3.5-5.5 g/dL) and serum gastrin of 21 pg/mL (normal: 0-100 pg/mL). Urinalysis was also normal without protein. Upper gastrointestinal endoscopy revealed thickened gastric folds. Gastric biopsy showed marked foveolar epithelial hyperplasia. The most likely diagnosis is:
Gastric carcinoma
Zollinger-Ellison syndrome
Autoimmune gastritis
Reactive gastropathy
Ménétrier disease
Ménétrier disease
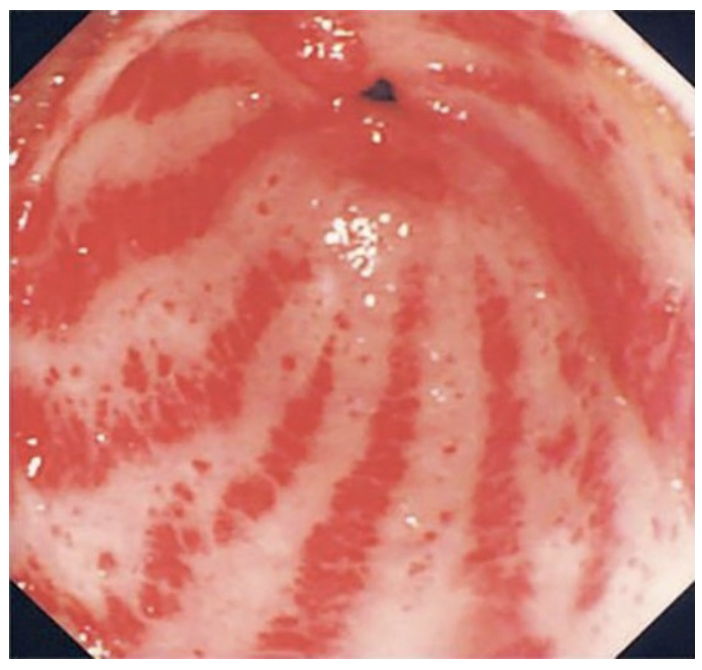
A 76-year-old woman, known to have multiple medical problems, was admitted for further work up for symptomatic anemia. Patient was complaining of fatigability, dizziness, and occasional black stool for about six months before admission. No history of hematemesis or rectal bleeding was noted. Patient’s past medical history was significant for hypertension, dyslipidemia, and systemic sclerosis. Upon examination, he looked pale and lethargic but with stable vital signs and without postural hypotension. Laboratory studies revealed a hemoglobin of 7.6 g/dL (normal: 10-16 g/dL) and hematocrit of 24% (normal: 36-48%). White blood cell and platelet counts were normal. Serum iron study showed low serum iron levels. Her renal and liver functions, and coagulation panel were within normal limits. The endoscopic appearance of her stomach is shown in the attached figure. Which of the following is the most likely diagnosis?
Gastric antral vascular ectasia
Portal hypertensive gastropathy
Dieulafoy lesion
Esophageal varices
Mallory Weiss syndrome
Gastric antral vascular ectasia
A 45-year-old man presented with chief complaint of epigastric pain and nausea, which had appeared three weeks previously. Upper gastrointestinal endoscopy revealed a duodenal ulcer located in the duodenal bulb. Laboratory studies showed a hemoglobin of 11.5 g/dL (normal: 12-18 g/dL). His serum Helicobacter pylori IgG antibody, stool H. pylori antigen, and rapid urease tests were all positive. Which of the following is the most likely pathophysiological mechanism underlying this patient’s duodenal ulcer?
Prostaglandin inhibition
Increased gastric acid production
Decreased gastric acid production
Decreased bicarbonate secretion
Decreased gastrin secretion
Increased gastric acid production
A 51-year-old man from Kolkata has an area of depres-
sion in his mouth that has enlarged over the past 7 months.
On oral examination, there is a 1.5 × 0.7 cm velvety, erythema-
tous area with focal surface erosion on his left buccal mucosa.
The lesion is excised and on microscopic examination there is
dysplastic squamous epithelium. Which of the following is the
most likely risk factor for developing this lesion?
A Candidiasis
B Dental malocclusion
C Epstein-Barr virus infection
D Immunosuppression
E Eating hot, spicy food
F Tobacco chewing
F Tobacco chewing

10. A 49-year-old man has used chewing tobacco and snuff
for many years. On physical examination the lesion shown in
the figure is seen on the hard palate. It cannot be removed by
scraping. A biopsy is performed, and microscopic examination
of the lesion shows a thickened squamous mucosa. Four years
later, a biopsy specimen of a similar lesion shows carcinoma in
situ. Which of the following is the most likely diagnosis?
A Oral thrush
B Lichen planus
C Leukoplakia
D Pyogenic granuloma
E Xerostomia
C Leukoplakia
11 A 54-year-old man, a nonsmoker, has a nonheal-
ing ulceration at the base of his tongue on the right side for
2 months. On examination this lesion is 1 cm in diameter
with irregular borders. Biopsy of the lesion is performed and
microscopic examination shows infiltrating squamous cell car-
cinoma. Which of the following infectious agents is most likely
to be associated with this lesion?
A Candida albicans
B Herpes simplex virus (HSV)
C Human papillomavirus (HPV)
D Prevotella intermedia
E Group A streptococcus
C Human papillomavirus (HPV)
7 A 42-year-old man has had a constant bad taste in his
mouth for the past month. On physical examination there are
white fluffy patches on the sides of his tongue. These cannot
be scraped off. A biopsy is taken and on microscopic examina-
tion shows squamous epithelial hyperkeratosis, parakeratosis,
and koilocytosis. Immunohistochemical staining for Epstein-
Barr virus (EBV) is positive. Which of the following is the most
likely risk factor for his oral lesions?
A Chronic alcohol abuse
B Diabetes mellitus
C HIV infection
D Pernicious anemia
E Sjögren syndrome
C HIV infection
A 25-year-old man notices several 0.3-cm, clear vesicles
on his upper lip after a bout of influenza. The vesicles rupture,
leaving shallow, painful ulcers that heal over the course of 10
days. Three months later, after a skiing trip, similar vesicles
develop, with the same pattern of healing. Which of the fol-
lowing microscopic findings is most likely to be associated
with these lesions?
A Budding cells with pseudohyphae
B Mononuclear inflammatory infiltrates
C Neutrophils within abscesses
D Squamous epithelial hyperkeratosis
E Intranuclear inclusions
E Intranuclear inclusions
6 A 35-year-old, HIV-positive man complains that he has
had a “bad” taste in his mouth and discoloration of his tongue
for the past 6 weeks. On physical examination, there are areas
of adherent, yellow-to-gray, circumscribed plaque on the lat-
eral aspects of the tongue. This plaque can be scraped off as a
pseudomembrane to show an underlying granular, erythema-
tous base. What is the most likely diagnosis?
A Aphthous ulcer
B Cheilosis
C Hairy leukoplakia
D Herpetic stomatitis
E Leukoplakia
F Oral thrush
F Oral thrush
32 A 57-year-old man notices a lump on the right side of
his face that has become larger over the past year. On physical
examination, a 3- to 4-cm firm, mobile, painless mass is pal-
pable in the region of the right parotid gland. The oral mucosa
appears normal. He does not complain of difficulty in chewing
food or talking. The mass is completely excised, and histologic
examination shows the findings in the figure. What is the most
likely diagnosis?
A Mucoepidermoid carcinoma
B Non-Hodgkin lymphoma
C Pleomorphic adenoma
D Sialolithiasis
E Sjögren syndrome
F Warthin tumor
F Warthin tumor
30 A 95-year-old man has noted swelling of his lower lip
for the past month. On examination, there is a fluctuant, 1-cm
nodule with a blue, translucent hue just beneath the oral mu-
cosa on the inside of his lip. The lesion is excised, and on mi-
croscopic examination shows granulation tissue. What is the
most likely etiology for this lesion?
A Eating chili peppers
B French kissing
C HIV infection
D Local trauma
E Pipe smoking
D Local trauma
29 A 69-year-old man has a major psychosis. He has been
bothered by pain on the left side of the face for 2 weeks. On
physical examination, there is a tender area of swelling 4 cm
in diameter beneath the skin, anterior to the left auricle above
the angle of the jaw. CT scan of the head shows cystic and
solid areas in the region of an enlarged left parotid gland.
After a course of antibiotic therapy, there is only minimal
improvement. A parotidectomy is performed. Microscopic
examination of the excised gland shows acute and chronic
inflammation, with fibrosis and abscess formation, duct lithi-
asis, and atrophy of acini. Which of the following infectious
agents is most likely to be found in this gland?
A Epstein-Barr virus
B Human papillomavirus
C Prevotella intermedia
D Rubeola virus
E Staphylococcus aureus
E Staphylococcus aureus
28 A 67-year-old man with Parkinson disease has experi-
enced an increasingly dry mouth for the past 3 months, and
this interferes with eating and swallowing. He has noted dry
eyes as well. On physical examination he has minimal tremor
at rest; there are no other abnormal findings. Laboratory stud-
ies show no detectable autoantibodies. Which of the following
is the most likely cause for his findings?
A Alcohol ingestion
B Anticholinergic drug use
C Candidiasis
D Sialadenitis with blockage of salivary duct
E Sjögren syndrome
F Tobacco use
B Anticholinergic drug use
33 A 60-year-old woman noticed an enlarging “bump” be-
neath her tongue for the past year. She does not smoke or use
alcohol. On physical examination, there is a 2.5-cm, movable,
submucosal mass arising in the minor salivary glands on the
buccal mucosa beneath the tongue on the right. Histologic ex-
amination of the excised mass shows that it is malignant and
locally invasive. The tumor recurs within 1 year. Which of the
following is the most likely diagnosis?
A Non-Hodgkin lymphoma
B Mucoepidermoid carcinoma
C Primitive neuroectodermal tumor
D Pleomorphic adenoma
E Squamous cell carcinoma
F Warthin tumor
B Mucoepidermoid carcinoma
1 A 23-year-old primigravida gives birth at term to a boy
infant. Ultrasound examination before delivery showed poly-
hydramnios. A single umbilical artery is seen at the time of
birth. The infant vomits all feedings, and then develops a fever
and difficulty with respirations within 2 days. A radiograph
shows both lungs and the heart are of normal size, but there
are pulmonary infiltrates and no stomach bubble. What is the
most likely diagnosis?
A Achalasia
B Diaphragmatic hernia
C Esophageal atresia
D Hiatal hernia
E Pyloric stenosis
F Zenker diverticulum
C Esophageal atresia
2 A 24-year-old man has developed abdominal pain and
increasing fatigue over the past 6 months. On physical exami-
nation, he is afebrile and appears pale. On palpation, there is
mild pain in the right lower quadrant of the abdomen. There
are no masses, and bowel sounds are active. Laboratory stud-
ies show hemoglobin, 8.9 g/dL; hematocrit, 26.7%; MCV,
74 μm3; platelet count, 255,000/mm3; and WBC count, 7780/
mm3. His stool is positive for occult blood. Upper gastroin-
testinal endoscopy and colonoscopy showed no lesions. One
month later, he continues to experience the same abdomi-
nal pain. Which of the following is most likely to cause this
patient’s illness?
A Acute appendicitis
B Angiodysplasia
C Celiac disease
D Diverticulosis
E Giardia lamblia infection
F Meckel diverticulum
F Meckel diverticulum
4 A 24-year-old woman gives birth to term infant after an
uncomplicated pregnancy. Apgar scores are 9 and 10 at 1 and
5 minutes after birth. The infant’s length and weight are at the
55th percentile. There is no significant passage of meconium.
Three days after birth, the infant vomits all oral feedings. On
physical examination, the infant is afebrile, but the abdomen
is distended and tender, and bowel sounds are reduced. An
abdominal ultrasound scan shows marked colonic dilation
above a narrow segment in the distal sigmoid region. A biopsy
specimen from the narrowed region shows an absence of gan-
glion cells in the muscle wall and submucosa. Which of the
following is most likely to produce these findings?
A Colonic atresia
B Hirschsprung disease
C Intussusception
D Necrotizing enterocolitis
E Trisomy 21
F Volvulus
B Hirschsprung disease
3 A 23-year-old woman, G2, P1, gave birth at term to a
boy of normal weight and length following an uncomplicated
pregnancy. The infant initially did well, but at 6 weeks, he
began feeding poorly for 1 week, and his mother noticed that
much of the milk he ingested was forcefully vomited within
1 hour. Now, on physical examination, the infant is afebrile,
and there are no external anomalies. A midabdominal mass is
palpable. Bowel sounds are active. The medical history indi-
cates that both the mother and her first child had the same ill-
ness during infancy. Which of the following conditions is most
likely to explain these findings?
A Annular pancreas
B Diaphragmatic hernia
C Duodenal atresia
D Pyloric stenosis
E Tracheoesophageal fistula
D Pyloric stenosis
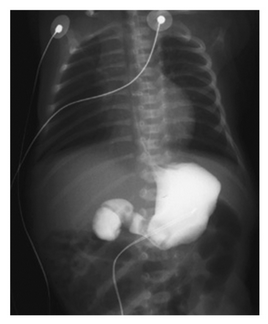
A 24yo, G2, P1001, woman has a screening ultrasound that shows polyhydramnios at 17 weeks gestation. She gives birth at term to a boy who on examination has no abnormal findings. Since birth, he has often vomited after feedings. An infant radiograph with contrast enhancement shows the findings in the figure. What is the most likely diagnosis?
Acute pancreatitis
Annular pancreas
Chronic pancreas
Islet cell adenoma
Pancreatic adenocarcinoma
Pyloric stenosis
Annular pancreas
6 A 22-year-old woman has had multiple episodes of aspi-
ration of food associated with difficulty swallowing during the
past year. On auscultation of her chest, crackles are heard at the
base of the right lung. A barium swallow shows marked esoph-
ageal dilation above the level of the lower esophageal sphincter.
A biopsy specimen from the lower esophagus shows an absence
of the myenteric ganglia. What is the most likely diagnosis?
A Achalasia
B Barrett esophagus
C Plummer-Vinson syndrome
D Sliding hiatal hernia
E Systemic sclerosi
A Achalasia
7 A 24-year-old woman living in eastern Bolivia has had
increasing difficulty with swallowing both liquids and solids
for the past year. She has substernal discomfort from a feeling
that foods “get stuck” going down. On examination her BMI
is 18. A barium swallow radiologically shows marked esopha-
geal dilation. An endoscopic biopsy is obtained and micro-
scopically shows reduced ganglion cells in myenteric plexus
along with lymphocytic infiltration. Which of the following
organisms is most likely infecting this woman?
A Bordetella pertussis
B Candida albicans
C Corynebacterium diphtheriae
D Herpes simplex virus
E Trypanosoma cruzi
E Trypanosoma cruzi
8 A 53-year-old man consumes a very large meal, washed
down with considerable alcohol. The ensuing discomfort
prompts him to take an emetic, but soon afterward he devel-
ops lower chest pain. Physical examination reveals crepitus
in subcutaneous tissue over his chest along with tachycardia
and tachypnea. Which of the following abnormalities of the
esophagus is most likely present in this man?
A Stricture
B Achalasia
C Ectopia
D Rupture
E Varices
D Rupture
9 A 30-year-old man has sudden onset of hemateme-
sis after a weekend in which he consumed large amounts of
alcohol. The bleeding stops, but he has another episode under
similar circumstances 1 month later. Upper gastroesophageal
endoscopy shows longitudinal tears at the gastroesophageal
junction. What is the most likely mechanism to cause his
hematemesis?
A Absent myenteric ganglia
B Autoimmune inflammation
C Herpes simplex virus infection
D Portal hypertension
E Vomiting
F Widened diaphragmatic crura
E Vomiting
10 A 16-year-old boy who is receiving chemotherapy for
acute lymphoblastic leukemia has had pain for 1 week when
he swallows food. Physical examination shows no abnormal
findings. Upper gastrointestinal endoscopy shows 0.5- to
0.8-cm mucosal ulcers in the region of the mid to lower esoph-
agus. The shallow ulcers are round and sharply demarcated,
and have an erythematous base. Which of the following is
most likely to produce these findings?
A Aphthous ulcerations
B Reflux esophagitis
C Herpes simplex esophagitis
D Gastroesophageal reflux disease
E Mallory-Weiss syndrome
C Herpes simplex esophagitis
27 A 53-year-old woman has had nausea, vomiting, and
midepigastric pain for 5 months. On physical examination, there
are no significant findings. An abdominal CT scan shows gastric
outlet obstruction. Upper gastrointestinal endoscopy shows an
ulcerated 2 × 4 cm bulky mass in the antrum at the pylorus. A
urease test is positive. Which of the following neoplasms is most
likely to be seen in a biopsy specimen of this mass?
A Adenocarcinoma
B Leiomyosarcoma
C Neuroendocrine carcinoma
D Non-Hodgkin lymphoma
E Squamous cell carcinoma
A Adenocarcinoma
19 A 72-year-old man takes large quantities of nonsteroidal
anti-inflammatory drugs (NSAIDs) because of chronic degen-
erative arthritis of the hips and knees. Over the past 2 weeks,
he has had epigastric pain with nausea and vomiting and an
episode of hematemesis. On physical examination, there are
no remarkable findings. A gastric biopsy specimen is most
likely to show which of the following lesions?
A Acute gastritis
B Adenocarcinoma
C Epithelial dysplasia
D Helicobacter pylori infection
E Hyperplastic polyp
A Acute gastritis
21 A 51-year-old woman has been feeling increasingly
tired for the past 7 months. There are no remarkable findings
on physical examination. Laboratory studies include hemo-
globin, 9.5 g/dL; hematocrit, 29.1%; MCV, 124 μm3; platelet
count, 268,000/mm3; and WBC count, 8350/mm3. The retic-
ulocyte index is low. Hypersegmented polymorphonuclear
leukocytes are found on a peripheral blood smear. The serum
gastrin is markedly increased. Antibodies to which of the fol-
lowing are most likely to be found in this patient?
A Gastric H+,K+-ATPase
B Gliadin
C Helicobacter pylori
D Intrinsic factor receptor
E Tropheryma whippelli
A Gastric H+,K+-ATPase
22 A 59-year-old man has had nausea and vomiting for
5 months. He has experienced no hematemesis. On physical
examination, there is no abdominal tenderness, and bowel
sounds are present. Upper gastrointestinal endoscopy shows
erythematous areas of mucosa with thickening of the rugal
folds in the gastric antrum. The microscopic appearance of a
gastric biopsy specimen with a Steiner silver stain is shown
in the figure. Which of the following factors is most likely
responsible for this gastric mucosal pathology?
A Cysteine proteinase
B Cytotoxin-associated gene A
C Heat-stable enterotoxin
D Shiga toxin
E Verocytotoxin
B Cytotoxin-associated gene A
26 A 49-year-old woman has a history of peptic ulcer disease
for which she has been treated with proton pump inhibitors. She
has had nausea with vomiting for the past 2 months. Upper GI
endoscopy reveals three circumscribed, round, smooth lesions
in the gastric body from 1 to 2 cm in diameter. Biopsies are taken
and microscopically show the lesions to consist of irregular
glands that are cystically dilated and lined by flattened parietal
and chief cells. No inflammation, Helicobacter pylori, metaplasia,
or dysplasia is present. What is the most likely diagnosis?
A Fundic gland polyps
B Gastric adenomas
C Hyperplastic polyps
D Hypertrophic gastropathy
A Fundic gland polyps
23 A 47-year-old woman with a lengthy history of heart-
burn and dyspepsia experiences sudden onset of abdominal
pain. On physical examination, she has severe mid epigastric
pain with guarding. Bowel sounds are reduced. An abdomi-
nal plain film radiograph shows free air under the left leaf of
the diaphragm. She is immediately taken to surgery, and a
perforated duodenal ulcer is repaired. Which of the following
organisms is most likely to have produced these findings?
A Campylobacter jejuni
B Cryptosporidium parvum
C Giardia lamblia
D Helicobacter pylori
E Salmonella typhi
F Shigella flexneri
G Yersinia enterocolitica
D Helicobacter pylori
24 A 35-year-old man has had epigastric pain for more than
1 year. The pain tends to occur 2 to 3 hours after a meal and is
relieved if he takes antacids or eats more food. He has noticed
a 4-kg weight gain in the past year. He does not smoke and
drinks 1 glass of Johannisberg Riesling daily. The result of a
urea breath test is positive, and a gastric biopsy specimen con-
tains urease. He begins a 2-week course of antibiotics, but on
day 4, he feels better and discontinues treatment. Three weeks
later, the epigastric pain recurs. If he does not seek further
treatment, which of the following complications is he most
likely to develop?
A Carcinoid syndrome
B Fat malabsorption
C Hematemesis
D Migratory thrombophlebitis
E Vitamin B12 deficienc
C Hematemesis
18 A 38-year-old woman has had nausea for 6 months.
She reports no vomiting or diarrhea. On physical examina-
tion, there are no remarkable findings. Upper gastrointestinal
endoscopy shows diffuse gastric mucosal erythema with focal
mucosal erosions, but no ulcerations. The esophageal and
duodenal mucosal surfaces appear normal. Gastric biopsies
are obtained and microscopic examination shows focal muco-
sal hemorrhage, loss of the surface epithelium, and increased
numbers of neutrophils, lymphocytes, and plasma cells in an
edematous mucosa. No Helicobacter pylori organisms are seen.
Laboratory studies show a normal serum gastrin level. Which
of the following pharmacologic agents is most likely to pro-
duce these findings?
A Aspirin
B Chlorpromazine
C Cimetidine
D Clindamycin
E Omeprazole
A Aspirin
20 A 54-year-old, previously healthy man sustained an
extensive thermal burn injury involving 70% of the total body
surface area of his skin. He was hospitalized in stable condi-
tion. Three weeks after the initial burn injury, he developed
melanotic stools. His blood pressure dropped to 80/40 mm
Hg, and his hematocrit declined to 18%. Where are gastroin-
testinal ulcerations most likely to be found in this man?
A Colon
B Duodenum
C Esophagus
D Ileum
E Stomach
E Stomach
A 42yo man presents with long-standing abdominal pain after meals, which is relieved by over.the.counter antacids. The patient has lost 9kg (20lbs) in the last year. Physical examination reveals peripheral edema and ascites. Lab studies show decreased serum albumin but normal levels of transaminases and gastrin. Gross and microscopic examination of this patient’s stomach would most likely show which of the following pathologic changes?
atrophic gastritis
enlarged rugal folds
intestinal metaplasia
multiple hemorrhagic ulcers
proliferation of neuroendocrine cells
enlarged rugal folds

An African American male presents with a non-scrapable plaque on his tongue. He has a history of injection drug use and currently uses IV heroin 3-4 times a week. No medical records and no immunization history known. CD4+ count is 410/mm3. This patient’s condition is most likely caused by?
Candida albicans
C. diphtheriae
Cytomegalovirus
EBV
HHV-8
EBV
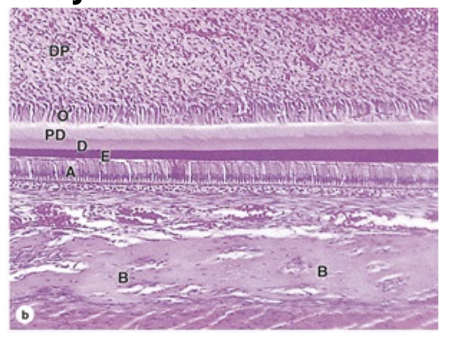
What are the 7 tooth layers?
DP, O, PD, D, E, A, B
A 2 year old male with an unknown immunization history is seen in the pediatricians office due to painful swelling of his right jaw. A PCR of the patient saliva reveals infection with the mumps virus. The doctor explains to the mother that this virus causes an infection of the parotid glands, which is self limited typically. The excretory ducts of human salivary glands are lined with?
Pseudostratified columnar epithelium
Simple cuboidal epithelium
Stratified columnar epithelium
Stratified squamous epithelium
Transitional epithelium
Simple cuboidal epithelium
A patient reports to your office with a large abcess near the left lower premolar area. On exam, you notice the abscess is protruding under the surface of the gingiva and causing severe inflammation. The patient asks you to explain the structures of the tooth and gingiva. The patient asks you to clarify what the periodontal ligament is. What would you tell you patient?
The ligament plays a role in creating dentin
The ligament binds the cementum and the mandible
The ligament cements the tooth to the alveolar ridge
The ligament plays a role in carrying nutrients
The ligament binds the cementum and the mandible
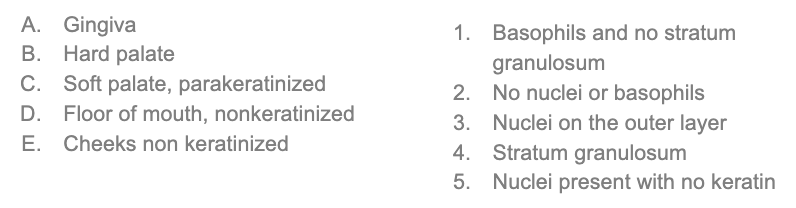
Match the correct description to the type of oral mucosa.
A. 4,2
B.4,2
C.1,3
D.5
E.5
Keratinization within the oral cavity helps with mechanical stress and acts as a protective factor
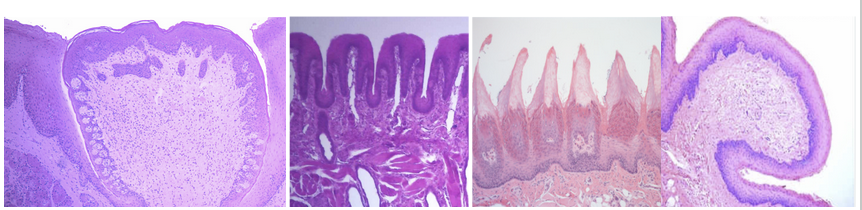
Label the types of lingual papillae and identify which contains the majority of taste buds and which are keratinized. Which are most numerous in children?
Circumvallate (most taste buds)
Foliate (kids)
Filiform (keratinized)
Fungiform
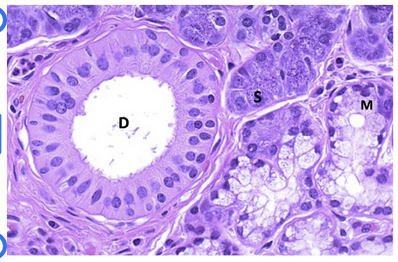
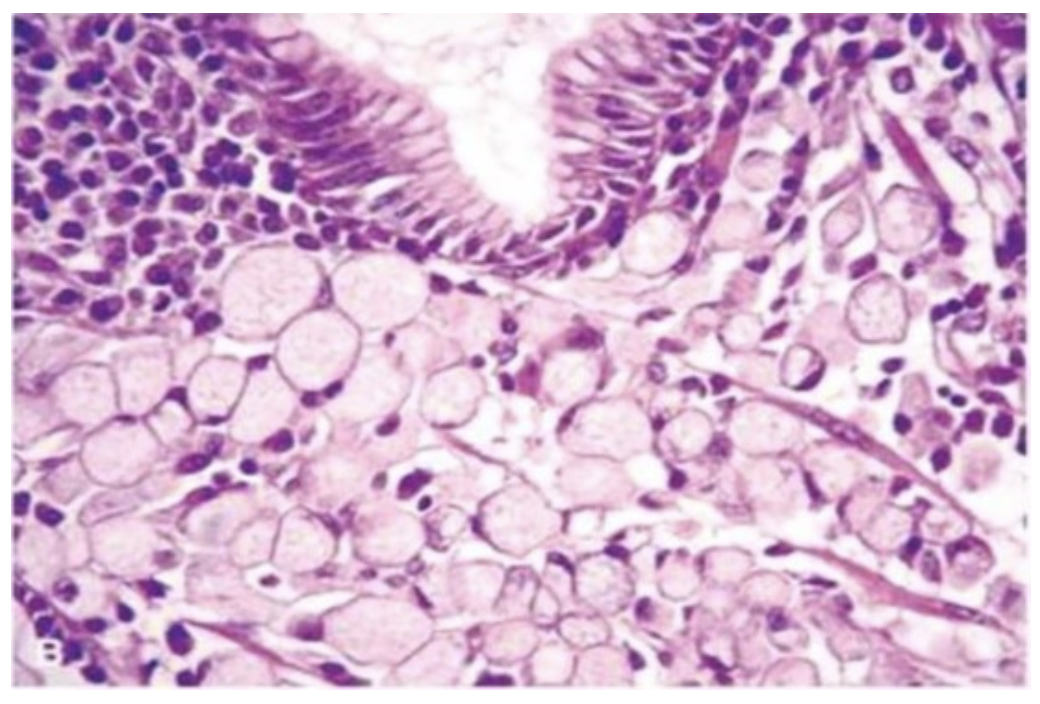
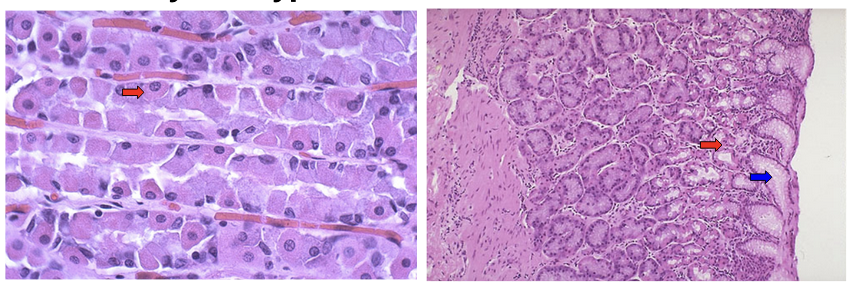
A patient reports to the office with complaints of a tender mass on the right jaw. He reports it has been slowly growing and previously did not hurt. On biopsy, the below tissue is shown (normal histology). What is the composition of the cell type(s) biopsied?
Mucionoid
Serous
Mucinous and Serous
None of the above
Mucinous and Serous
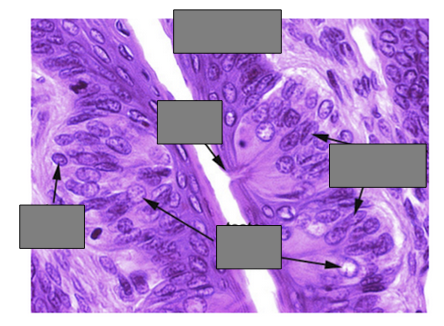
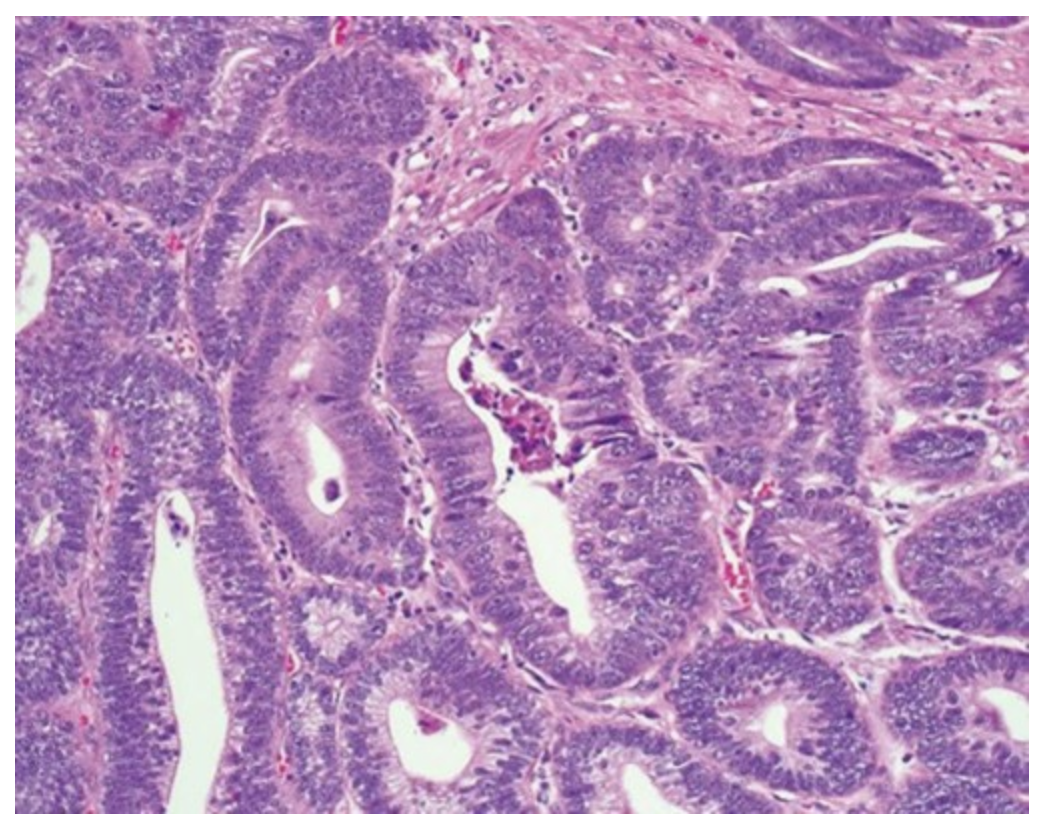
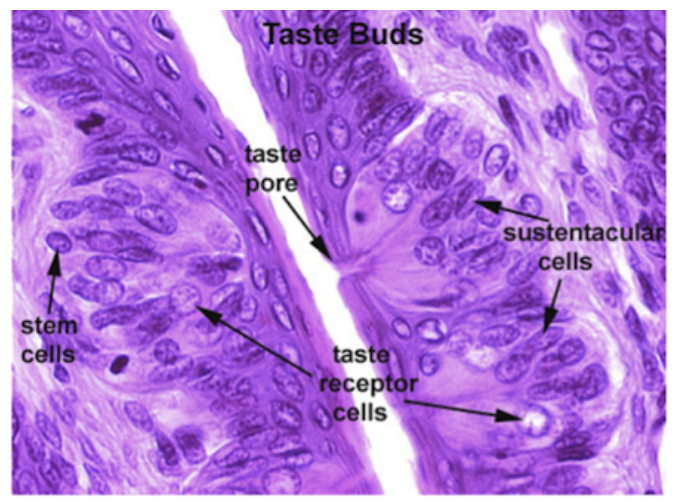
Label the arrows. What is the most likely biopsy source?
A 42-year-old man has had a constant bad taste in his mouth for the past month. On physical examination there are white fluffy patches on the sides of his tongue. These cannot be scraped off. A biopsy is taken and on microscopic examination shows squamous epithelial hyperkeratosis, parakeratosis, and koilocytosis. Immunohistochemical staining for Epstein-Barr virus (EBV) is positive. Which of the following is the most likely risk factor for his oral lesions?
A. Chronic alcohol abuse
B. Diabetes mellitus
C. HIV infection
D. Pernicious anemia
E. Sjögren syndrome
C. HIV infection
A 54-year-old man, a nonsmoker, has a nonhealing ulceration at the base of his tongue on the right side for 2 months. On examination this lesion is 1 cm in diameter with irregular borders. Biopsy of the lesion is performed and microscopic examination shows infiltrating squamous cell carcinoma. Which of the following infectious agents is most likely to be associated with this lesion?
A. Candida albicans
B. Herpes simplex virus (HSV)
C. Human papillomavirus (HPV)
D. Prevotella intermedia
E. Group A streptococcus
C. Human papillomavirus (HPV)
A 17-year-old girl notices a small, sensitive, gray-white area forming along the lateral border of her tongue 2 days before the end of her final examinations. On examination by the physician’s assistant, the girl is afebrile. There is a shallow, ulcerated, 0.3-cm lesion with an erythematous rim. No specific therapy is given, and the lesion disappears within 2 weeks. The history shows that the girl does not use tobacco or alcohol. Which of the following is the most probable diagnosis?
A. Aphthous ulcer
B. Herpes simplex stomatitis
C. Leukoplakia
D. Oral thrush
E. Sialadenitis
A. Aphthous ulcer
A 25-year-old man notices several 0.3-cm, clear vesicles on his upper lip after a bout of influenza. The vesicles rupture, leaving shallow, painful ulcers that heal over the course of 10 days. Three months later, after a skiing trip, similar vesicles develop, with the same pattern of healing. Which of the following microscopic findings is most likely to be associated with these lesions?
A. Budding cells with pseudohyphae
B. Mononuclear inflammatory infiltrates
C. Neutrophils within abscesses
D. Squamous epithelial hyperkeratosis
E. Intranuclear inclusions
E. Intranuclear inclusions
A 58-year-old man, a cigar smoker, visited his dentist for a routine dental examination. The dentist noticed lesions with the clinical (A) and histologic (B) appearance shown in the figure. The medical history showed no major medical problems. Which of the following etiologic factors most likely contributed to the development of these lesions?
A. Chronic sialadenitis
B. Dental caries
C. Eating smoked foods
D. Herpes simplex virus type 1
E. Smoking tobacco
E. Smoking tobacco
A 51-year-old man from Kolkata has an area of depression in his mouth that has enlarged over the past 7 months. On oral examination, there is a 1.5 × 0.7 cm velvety, erythematous area with focal surface erosion on his left buccal mucosa. The lesion is excised and on microscopic examination there is dysplastic squamous epithelium. Which of the following is the most likely risk factor for developing this lesion?
A. Candidiasis
B. Dental malocclusion
C. Epstein-Barr virus infection
D. Immunosuppression
E. Eating hot, spicy food
F. Tobacco chewing
F. Tobacco chewing
A 43 year old female presents with xerostomia and xerophthalmia. Palpable enlarged parotid glands are found on exam. Her last dental visit uncovered numerous dental caries. Which of the following antibodies is most closely associated with this patient’s disease process?
Anticentromere antibodies
anti-dsDNA antibodies
anti-Jo-1 antibodies
anti-SSA antibodies
anti-U1 RNP antibodies
anti-SSA antibodies
A 32 year old female presents to the office for evaluation of pain and swelling in her mouth and neck. She says that 4-5 times per year, a swollen, tender mass develops under her jaw that resolves on its own without medication. The patient is up to date on immunizations. She has a temperature of 102F. There is a tender, palpable mass on the right neck below the mandible. Scant purulent drainage is seen on the floor of the mouth. The most likely cause of this patient's condition is?
H. Influenzae
Paramyxovirus
Prevotella species
S. aureus
Strep pneumoniae
S. aureus
A women presents in the office with a large mass protruding from her lower mandibular region. She reports being up to date with immunizations and the mass has been slow growing. On surgical excision and removal, pathology and genetic testing was ordered. The mass showed chromosomal rearrangements affecting PLAG1 and ductal and myoepithelial cells were present. What is the likely diagnosis?
Pleomorphic adenoma
Warthin tumor
Mucoepidermoid carcinoma
Adenoid cystic carcinoma
Pleomorphic adenoma
A 45 year old female had a mass removed from her parotid gland, near the tail. Below is the image seen under microscope. In addition, the image shows large polygonal cells with abundant basophilic granular cytoplasm. What is the likely diagnosis?
Warthin Tumor
Acinic Cell Carcinoma
Adenoid cystic carcinoma
Sialadenitis
Acinic Cell Carcinoma
A 65 year old male presents with a large mass on the right parotid region. On exam, the patient reports a history of 30 pack years smoking. A biopsy is taken of the mass before further putting the patient at surgical discomfort. He is diagnosed with a Warthin Tumor. What is a likely histological presentation?
Basophilic granular cytoplasm
Decreased mitochondria
Epidermoid cells, intermediate cells, and glandular components
Cribuniform patterns of myoepithelial cells
Lymphoid tissue with reactive germinal centers
Lymphoid tissue with reactive germinal centers
A 36-year-old man presents for evaluation of progressive difficulty swallowing both solids and liquids. An upper endoscopy reveals no mechanical obstruction, and a manometry study is ordered. Histological examination of the upper gastrointestinal tract is performed. A cross-section of a tubular organ is shown under high-power microscopy. The tissue shows nonkeratinized stratified squamous epithelium with underlying submucosa and a muscularis externa that includes both skeletal and smooth muscle fibers. Which of the following best describes the organization of the muscularis externa in this region?
A) Inner oblique, middle circular, outer longitudinal layers of smooth muscle
B) Entirely skeletal muscle forming a well-defined circular and longitudinal layer
C) Skeletal muscle in the inner layer, transitioning to smooth muscle in the outer layer
D) Skeletal muscle in the upper third, mixed muscle in the middle third, and smooth muscle in the lower third
E) Two smooth muscle layers forming a well-defined sphincter near the gastroesophageal junction
D) Skeletal muscle in the upper third, mixed muscle in the middle third, and smooth muscle in the lower third
A histological section of gastric mucosa is taken from the fundus of the stomach. The epithelium consists of simple columnar cells that extend into the lamina propria to form deep invaginations known as gastric pits and glands. One cell type within the gland is characterized by a large, pyramidal shape, an eosinophilic cytoplasm, and an extensive system of intracellular canaliculi lined by microvilli. Which of the following best describes the function of this cell type?
A) Secretes pepsinogen for protein digestion
B) Produces acidic mucin to assist in mixing chyme
C) Synthesizes and secretes hydrochloric acid and intrinsic factor
D) Releases serotonin to stimulate smooth muscle contraction
E) Regenerates epithelial lining and resides at the base of the gland
C) Synthesizes and secretes hydrochloric acid and intrinsic factor
A histologic section is taken from the wall of the proximal duodenum during evaluation of a patient with chronic peptic ulcers. The submucosa reveals clusters of pale-staining glands composed of cells with mucigen-rich, clear cytoplasm and basally located nuclei. Which of the following best describes the function of the glands shown?
A) Secretion of hydrochloric acid to promote protein digestion
B) Production of alkaline mucus to neutralize acidic chyme from the stomach
C) Release of pepsinogen for proteolysis in the gastric lumen
D) Secretion of acidic mucin to lubricate intestinal contents
E) Activation of enterocyte enzymes through the release of bile salts
B) Production of alkaline mucus to neutralize acidic chyme from the stomach
A histologic sample is taken from a segment of the gastrointestinal tract. It reveals numerous goblet cells within simple columnar epithelium, arranged along straight, tubular intestinal glands without villi. The mucous produced by these goblet cells is notably more abundant and viscous than that seen in similar cells from a proximal portion of the GI tract. Which of the following best explains the functional role of the increased mucous production in this region?
A) Neutralizes acidic chyme delivered from the stomach
B) Facilitates enzymatic digestion and nutrient absorption
C) Enhances peristaltic mixing with bile and pancreatic enzymes
D) Protects the mucosa from mechanical damage due to dehydration of luminal contents
E) Provides a vehicle for fat-soluble vitamin absorption
D) Protects the mucosa from mechanical damage due to dehydration of luminal contents
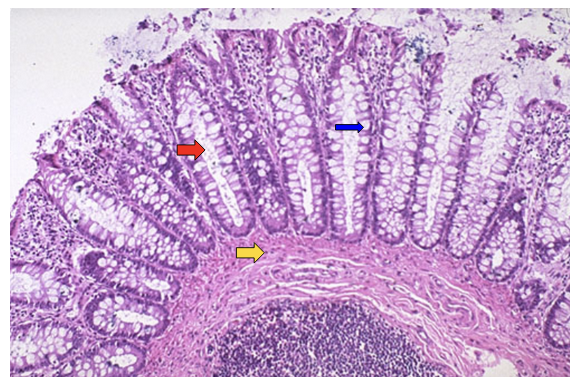
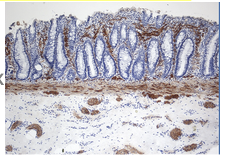
Identify structures found in the colon.
Red arrow:
crypt
Blue arrow:
Goblet cell (secreting mucin)
Yellow arrow:
Submucosa
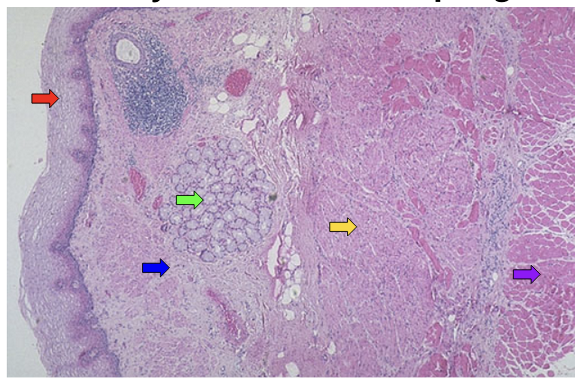
Identify structures in esophagus.
Red arrow: non-keratinizing squamous mucosa
Green arrow: mucus gland
Blue arrow: submucosa
Yellow arrow: smooth muscle
Purple arrow: skeletal muscle
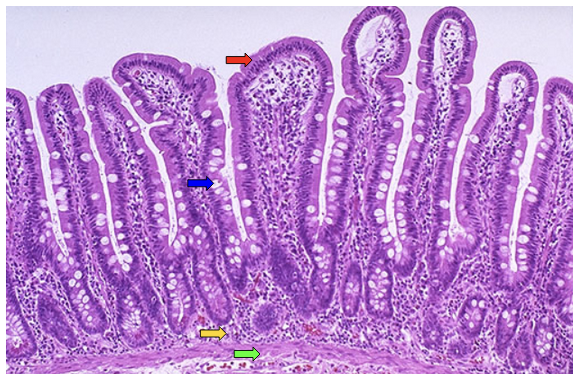
Identify structures in small intestine.
Red arrow: villi
Blue arrow: goblet cell
Yellow arrow: lamina propria
Green arrow: muscularis mucosa
Identify cell type from small intestine:
Paneth cell:’
Located at base of crypt
secrete enzymes and defensins to protect against microbes
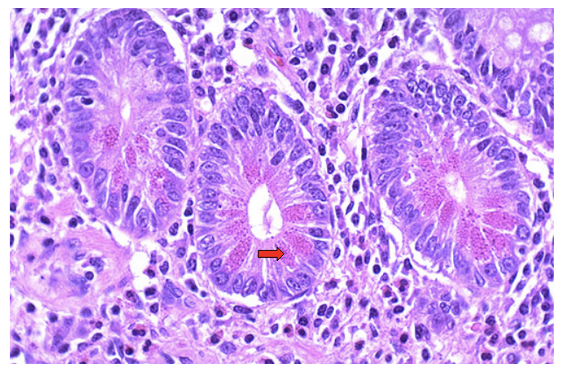
Identify cell type from stomach.
Red arrow: parietal cell (pink in color) (secret HCL and intrinsic factor)
Blue arrow: gastric pits
A 29 year old woman presents to the hospital for a C-section at 38 weeks gestation. Prenatal ultrasounds have demonstrated polyhydramnios since the second trimester. On delivery of the infant, the infant appears normal. During breast feeding the child begins to choke and drool. Nonbilious emesis and a cyanotic appearance are seen on recurrent feedings. He abdomen is nondistended and bowel sounds are heard. What is the likely diagnosis?
Pure esophageal atresia
Surfactant deficiency
Tetralogy of fallot
Transesophageal fistula
Transient tachypnea of the newborn
Transesophageal fistula
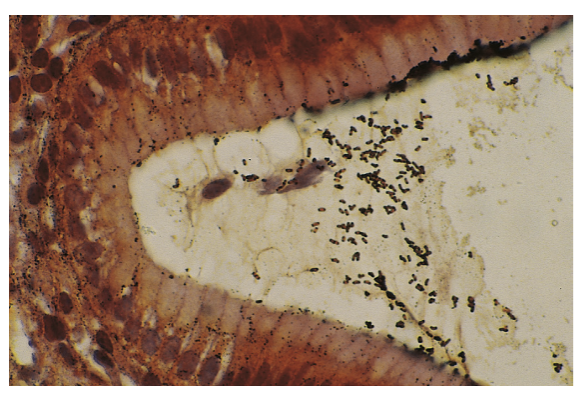
A 3 month old boy is brought to the ER with a 3-day history of fever, explosive diarrhea, a soft abdomen, vomiting, and lethargy. Anorectal manometry is abnormal. Biopsy of the rectal tissue is stained for acetylcholinesterase. A sample of the biopsy is negative for calretinin and positive for silver impregnation. The most likely cause of the patient's symptoms are?
The absence of ganglion cells at the submucosal and myenteric plexuses
Deficiency of the argyrophil plexus
Lack of AChE activity in the mucosa
Small immature ganglion cells in the submucosal plexus
Thick nerve trunks accompanied by the giant ganglia
The absence of ganglion cells at the submucosal and myenteric plexuses
A 2 year old male is brought to the ER with a 2 day history of nausea, vomiting, and abdominal pain. A green tinge was noted in the vomit by his mother. He has been crying for hours. His mother states these are new symptoms. Abdominal examination reveals moderate tenderness in the epigastric without guarding. MR choli-pancreatography reveals the presence of dorsal and ventral pancreatic ducts. Which of the following mechanisms most likely underlies the patient's condition?
abnormal septation of the caudal foregut
Encircling of the pancreatic tissue around the duodenum
Failure of fusion of pancreatic ductal system
Hypertrophy of the pyloric sphincter
Incomplete canalization of the duodenum lumen
Failure of fusion of pancreatic ductal system

A 1 day old newborn is in the NICU for evaluation. He was born at term, via uncomplicated delivery. The mother did not receive prenatal care. She admits to smoking 2-3 cigarettes daily, no drug or alcohol use. There is no evidence of cyanosis and he moves his extremities well. Abdominal exam is shown below. The pathogenesis of the patient’s condition involves?
A congenital defect in the pleuroperitoneal membrane
Failed closure of the caudal fold
Failure of the extra embryonic gut to return to the abdominal cavity
Incomplete closure of the umbilical ring following physiological herniation of the intestines
Incomplete rotation of the midgut in utero
Failure of the extra embryonic gut to return to the abdominal cavity
A 4 year old male is brought to an urgent care with a mother concerned about maroon blood in his stool. She reports a good appetites, no new dietary changes, and he has not been vomiting, constipated, or had diarrhea. No hemorrhoids or anal fissures on exam. The abdominal radiograph shows a normal bowel gas pattern and no obstructions. The patient is transported to a children's hospital and a technetium-99m pertechnetate scan is performed. The most likely location of the patient's underlying pathology is located?
2 ft distal to the ileocecal valve
2 ft proximal to the ileocecal valve
2 ft proximal to the sigmoid colon
2 in distal to the ileocecal valve
2 in proximal to the ileocecal valve
2 ft proximal to the ileocecal valve
A 22-year-old woman has had multiple episodes of aspiration of food associated with difficulty swallowing during the past year. On auscultation of her chest, crackles are heard at the base of the right lung. A barium swallow shows marked esophageal dilation above the level of the lower esophageal sphincter. A biopsy specimen from the lower esophagus shows an absence
of the myenteric ganglia. What is the most likely diagnosis?
A. Achalasia
B. Barrett esophagus
C. Plummer-Vinson syndrome
D. Sliding hiatal hernia
E. Systemic sclerosis
A. Achalasia
A 68-year-old man from Birmingham, England, has had “heartburn” and substernal pain after meals for 25 years. For the past year, he has had increased pain with difficulty swallowing both liquids and solids. On physical examination, there are no remarkable findings. Upper gastrointestinal endoscopy shows an ulcerated lower esophageal mass that nearly occludes the lumen of the esophagus. A biopsy specimen of this mass is most likely to show which of the following neoplasms?
A. Adenocarcinoma
B. Carcinoid tumor
C. Leiomyosarcoma
D. Non-Hodgkin lymphoma
E. Squamous cell carcinoma
A. Adenocarcinoma
A 30-year-old man has sudden onset of hematemesis after a weekend in which he consumed large amounts of alcohol. The bleeding stops, but he has another episode under similar circumstances 1 month later. Upper gastroesophageal endoscopy shows longitudinal tears at the gastroesophageal junction. What is the most likely mechanism to cause his Hematemesis?
A. Absent myenteric ganglia
B. Autoimmune inflammation
C. Herpes simplex virus infection
D. Portal hypertension
E. Vomiting
F. Widened diaphragmatic crura
E. Vomiting
An 82 year old man presents to the office with a 1 year history of difficulty swallowing and regurgitation of undigested food. He states that his symptoms have progressively worsened since their onset. A lateral barium contrast esophagogram reveals an outpouching near the pharyngoesophageal junction, as shown. Which of the following muscles forms a border through which this outpouching transverses?
Cricopharyngeus
Middle pharyngeal constrictor
Posterior cricoarytenoid
Stylopharyngeus
Superior pharyngeal constrictor
Cricopharyngeus
A 57-year-old woman has had burning epigastric pain after meals for more than 1 year. Physical examination shows no abnormal findings. Upper gastrointestinal endoscopy shows an erythematous patch in the lower esophageal mucosa. A biopsy specimen shows basal zone squamous epithelial hyperplasia, elongation of lamina propria papillae, and scattered intraepithelial neutrophils with some eosinophils. Which of the following is the most likely diagnosis?
A. Barrett esophagus
B. Esophageal varices
C. Iron deficiency
D. Reflux esophagitis
E. Systemic sclerosis
D. Reflux esophagitis
A 56 year old male has a family history of colon carcinoma. He reports regular bowel movements without hematochezia or melena and denies any change in stool caliber or character. He undergoes a screening colonoscopy. During the procedure 3 polyps are removed. The histology of each polyp is examine. Which of the following polyps is most concerning for the development of additional, future adenomas or carcinoma?
Inflammatory polyps
Hyperplastic polyps with distorted glands lined with foveolar epithelium and edematous stroma
Fundic gland polyps with cystically dilated glands
Polyp consisting of dysplastic columnar cells with mucin depletion and pencil shaped nuclei with hyperchromasia
Polyp consisting of dysplastic columnar cells with mucin depletion and pencil shaped nuclei with hyperchromasia