Looks like no one added any tags here yet for you.
Define STI and STD
Sexually transmitted infections (STIs) are infections that are primarily spread through sexual contact (oral, anal, or genital sex)
• Caused by microorganisms passed from one person to another through blood, semen, vaginal fluids, or other body fluids
Sexually transmitted diseases (STDs) are infections that progress to disease.
Explain the importance of studying STIs
1. Public Health Impact: significant public health issue due to their prevalence and potential complications
2. Health Consequences: untreated STIs can lead to serious health problems, including infertility, cancer, and increased risk of HIV
3. Economic Burden: treatment and management of STIs impose a substantial economic burden on healthcare systems
Describe the current state/trends of sexually transmitted infections within the US
• Trends in HPV pre and post vaccination
1/5 people in the US have an STI, 68 million infections
26 million new STIs in 2018
75-80% of sexually active adults will be infected at some point in their life
almost ½ of new infections in ages 15-24
Top 3 in prevalence: HPV, HSV-2, Trichomoniasis
Top 3 in incidence: HPV, Trichomoniasis, Chlamydia
Top viral: HPV
Top bacterial: chlamydia
Top parasitic: trichomoniasis
Explain the unique challenges placed on sexually transmitted diseases
Shame in testing and treatment
It’s fun!!!
Perception that they are trivial
Lack of clarity on what constitutes sexual transmission
There are moral values placed on the behaviors associated with STDs that are not placed on transmission of other diseases
Explain how epithelium tissue type impacts sexual transmission
Mucosal Epithelium
found in genital tract, rectum, and oral cavity. characterized by a moist surface that allows pathogens to enter
More prone to microtears and abrasion, provides entry points for pathogens
Many STDs (HIV, gon, and chlam) preferentially infect mucosal tissue due to accessibility and favorable environment
Keratinized Epithelium
found in areas like skin and outer genitalia
keratinized layer acts as a physical barrier, reduces likelihood of pathogen penetration
some pathogens (HPV) can infect this tissue, can lead to conditions like genital warts
Explain how mode of transmission (i.e. contact, abrasion) impacts sexual transmission
Varied Modes of Transmission
• Many are the result of vaginal, oral, or anal sex with infected partner
Non-penetrative transmission
• kissing or close contact: examples include crabs (pubic lice), scabies
• mother to child during birth: examples include syphilis, gonorrhea, HIV, herpes
• breastfeeding: examples include HIV
Specific transmission requirements
• Crabs requires contact
• HPV requires abrasion or microtears
• HIV requires exchange of bodily fluids
Focus on gonorrhea, chlamydia, and syphilis
Age and sex demographics for chlamydia and syphilis
decrease in chlamydia and gonorrhea, increase in syphilis
$1 billion in direct medical cost for chlamydia, gonorrhea and syphilis
Bacterial STI agents
Chlamydia trachomatis – Chlamydia
genital discharge, inflammation
Neisseria gonorrhea – Gonorrhea
genital discharge, pain
Treponema pallidum – Syphillis
lesions (1O), rash (2O), gummas, neurological, cardiovascular (3O)
Viral STI agents
Hepatitis B (HBV)
• viral hepatitis
Herpes simplex 1 and 2 (HSV):
• Herpes
• lesions, oral and genital
Human immunodeficiency virus 1 and 2 (HIV):
• Acquired immunodeficiency syndrome (AIDS)
Human papiloma viruses (HPV):
• cervical cancer, genital warts
HPV trends since vaccine
88% down in teen girls, 81% down in young women
Define the basic characteristics of the Neisseria gonorrheae bacterium (i.e., morphology, cell wall architecture, competence, capsule, motility)
gram negative
found in pairs (diplococci)
motile (uses twitching)
not commensal (unlike many other forms of Neisseria)
frequently found in neutrophils in exudate from infection
Describe key epithelial surfaces infected in men and women
Generally infects area of columnar epithelium or non-keratinized squamous epithelium
In males – infection of epithelium of urethra
In females – infection of endocervical epithelium (transition zones of columnar and stratified squamous epithelium), may also infect urethra.
Define key symptoms of N. Gonorrhoeae in men
Almost always symptomatic (approx 90%), can vary in severity of symptoms
Usually confined to the anterior urethra
Inflammation results in swelling, redness, and pain
Dysuria – pain during urination
May infect prostate and even progress to testicles possibly causing sterility
Rectal infections may occur and are frequently asymptomatic
Explain general epidemiological trends of gonorrhea
• Age group: most common in 20-24
• Sex: more common in men after age 20
• Location: mostly southern united states
• Race/Ethnicity: mostly black individuals, least in asian and white
• Antibiotic resistance: rise in resistance to ciprofloxacin, azithromycin and tetracycline. resistance to penicillin currently trending down
Define key symptoms of N. Gonorrhoeae in women
Infection of endocervix and possibly urethra
may extend through uterus and affect fallopian tubes and ovaries possibly causing sterility
The keratinized epithelium of the adult vagina is not susceptible to infection. However vaginal infection can occur in children
Rectal infections may occur but are frequently asymptomatic
Approx 50% of infections are asymptomatic
Untreated gonorrhea infections are responsible for ~15% of PID
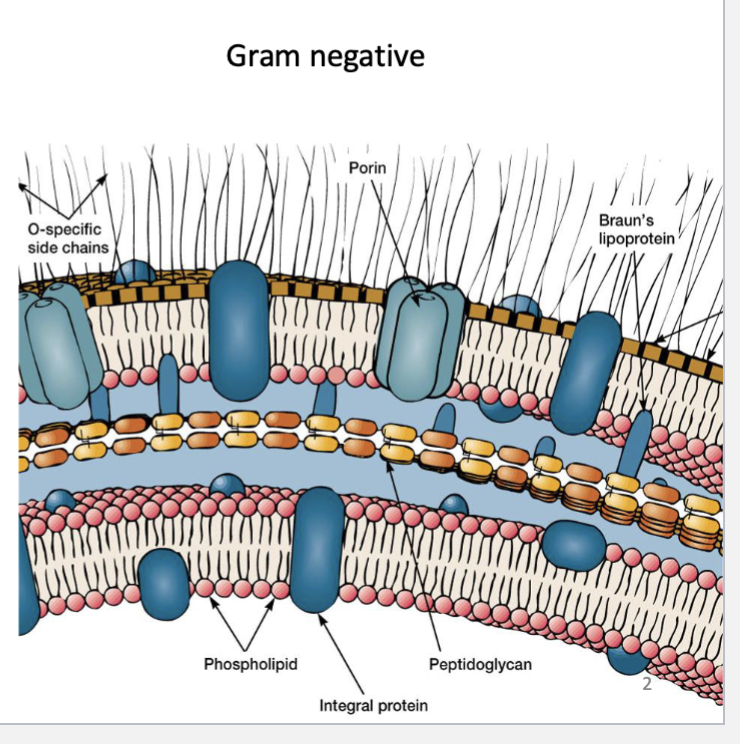
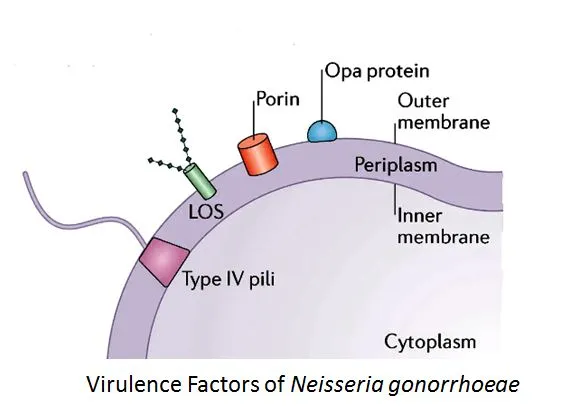
Identify the basic features of Gram negative cell wall and which are of particular interest in Neisseria
N. gonorrhoeae does not have a capsule
Has lipooligosaccharide (LOS) on its surface
Opa proteins and porin important for pathogenesis
Type IV pilus for movement and adherence to epithelium
Compare and contrast five different types of bacterial motility
Swimming, swarming, twitching, gliding, floating
swarming, swarming, and twitching associated with pathogens
swarming twitching and gliding occur on surface, swimming and floating are in 3D area
swarming is social behavior, the rest are individual
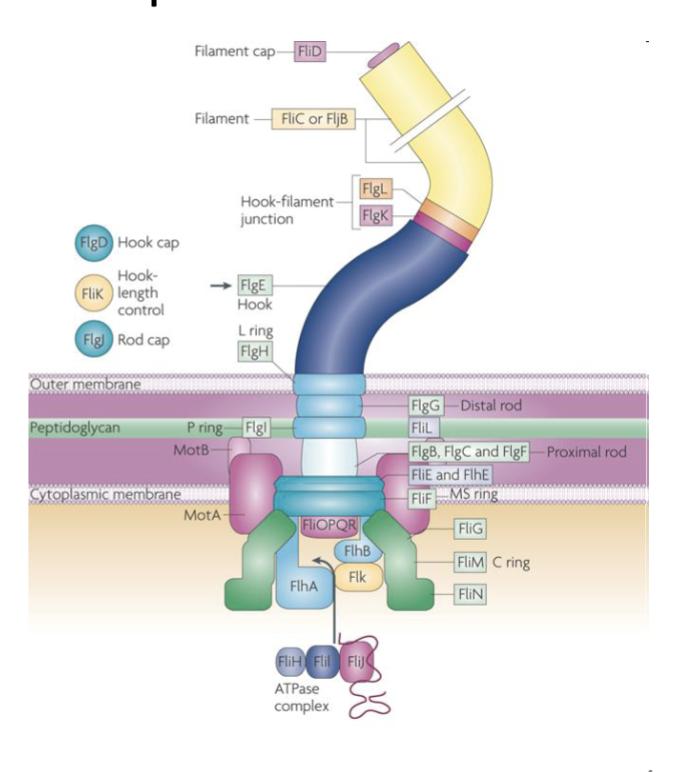
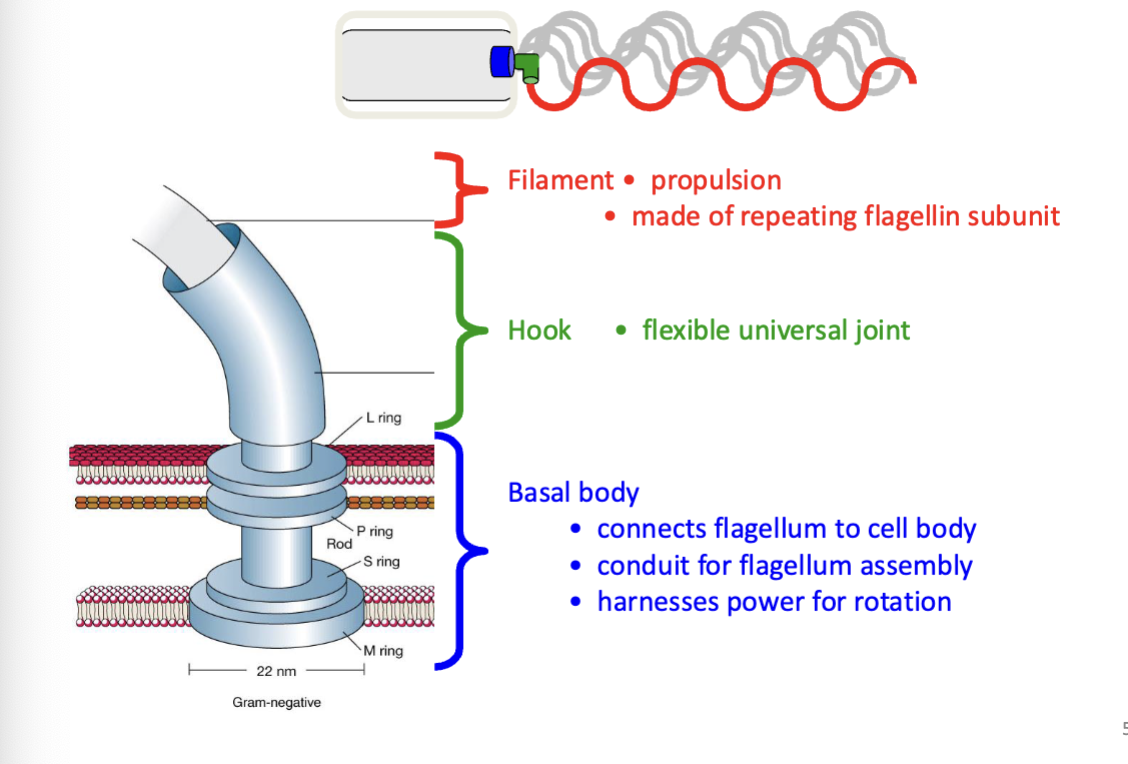
flagellum components
• a massive molecular machine that spans the cell envelope.
• built as a complex of more than 30 different proteins.
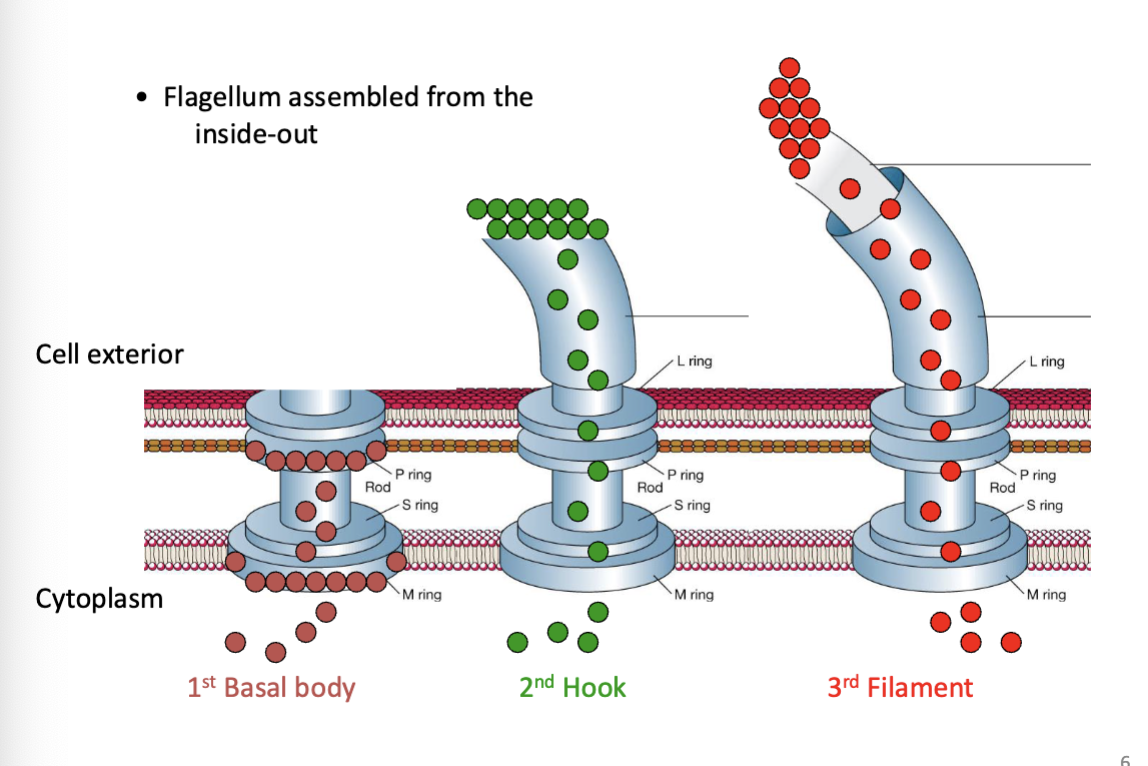
• subunit assembly must be perfectly timed and accurately ordered.
Describe the different functions of different types of pili
Some involved in adhesion (type I), some involved in motility (type IV), some involved in genetic transfer (“sex pili”)
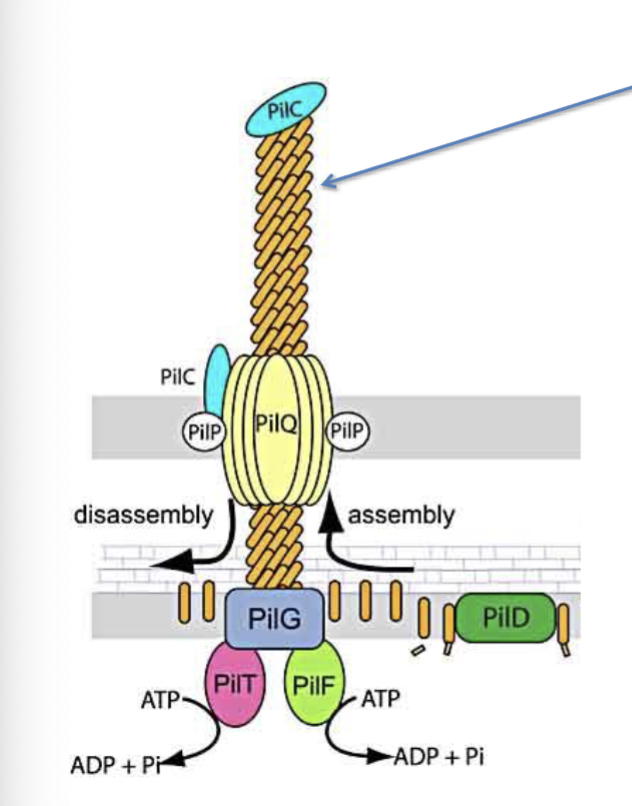
Describe the structure of the type IV pilus
PilE (arrow)- major pilin
PilC- acts as the adhesin
PilF- drives extension pushing PilE monomers through PilG to add to cell proximal end of the pilus and push it through PilQ
PilT- drives retraction causing removal of PilE monomers from cell proximal end of pilus
Monomers remain stored in the inner membrane for re-use
PilC is necessary for binding epithelial cells and establishing infection
Explain the basic mechanism of pilus extension and retraction
Extension:
Pilus subunits are polymerized and pushed out of the bacterial cell membrane by a motor protein (e.g., PilB in type IV pili).
This extends the pilus outward to interact with surfaces or host cells.
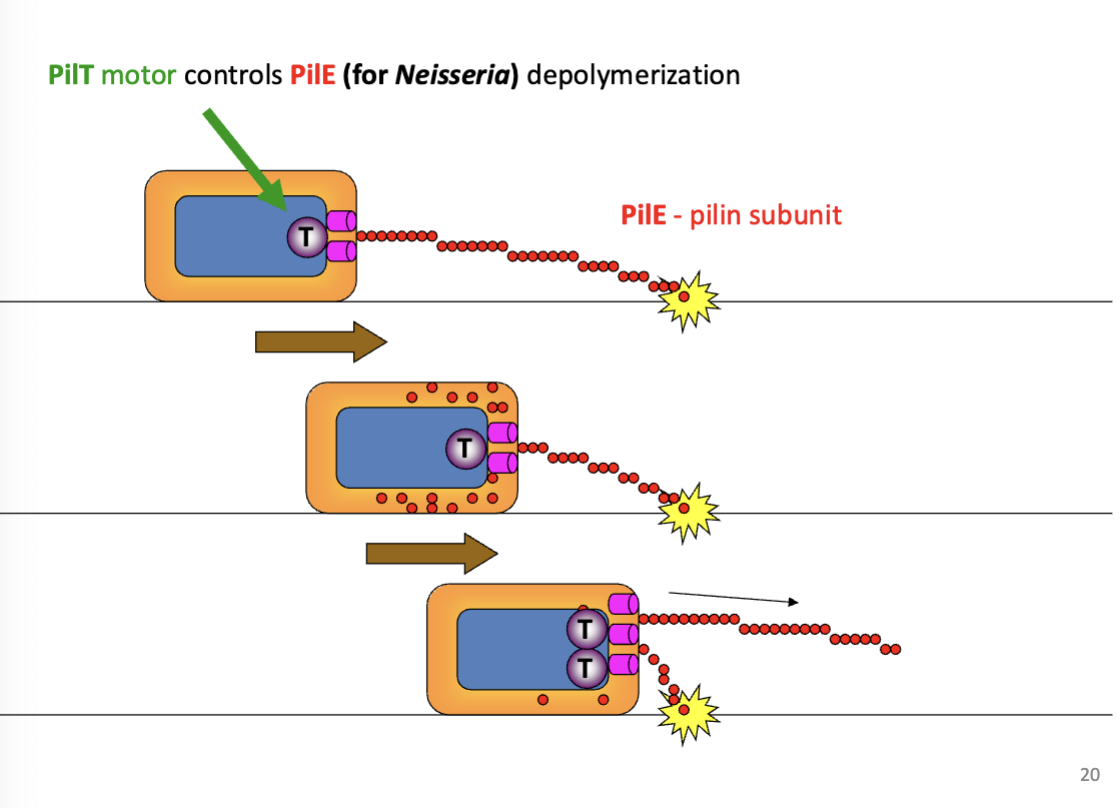
Retraction:
A separate motor protein (e.g., PilT in type IV pili) depolymerizes the pilus subunits, pulling the pilus back into the cell.
Retraction generates mechanical force, which can help bacteria move, attach, or uptake DNA (in transformation).
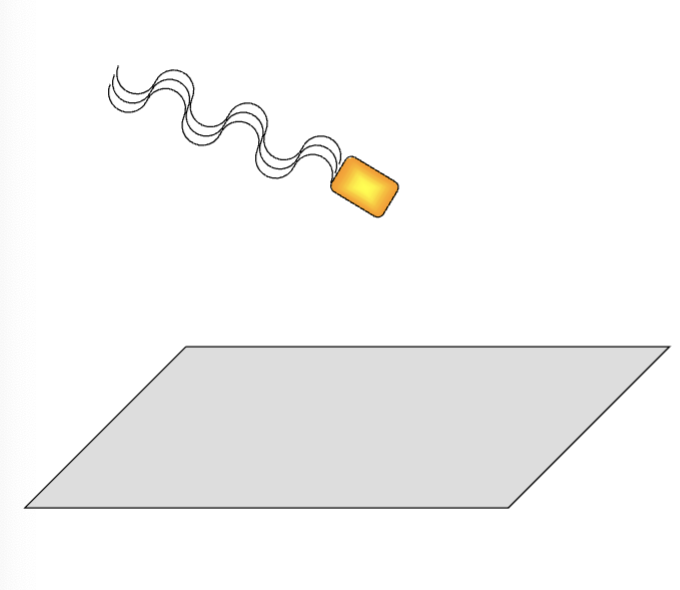
swimming motility
takes place in liquid, individual movement, powered by rotating flagella
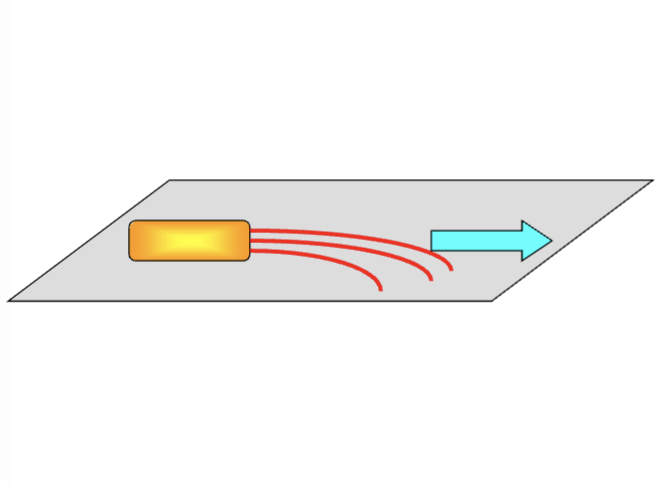
swarming motility
surface motility, social behavior, requires flagella, requires a surfactant to reduce surface tension, cells become hyperflagellate
twitching motility
surface motility, type IV pilus mediated, pilus extends and attaches to surface, then retracts and pulls cell along. jerky movement over surfaces hence “twitching”
flagellum ultrastructure
flagellum assembly
flagellum power
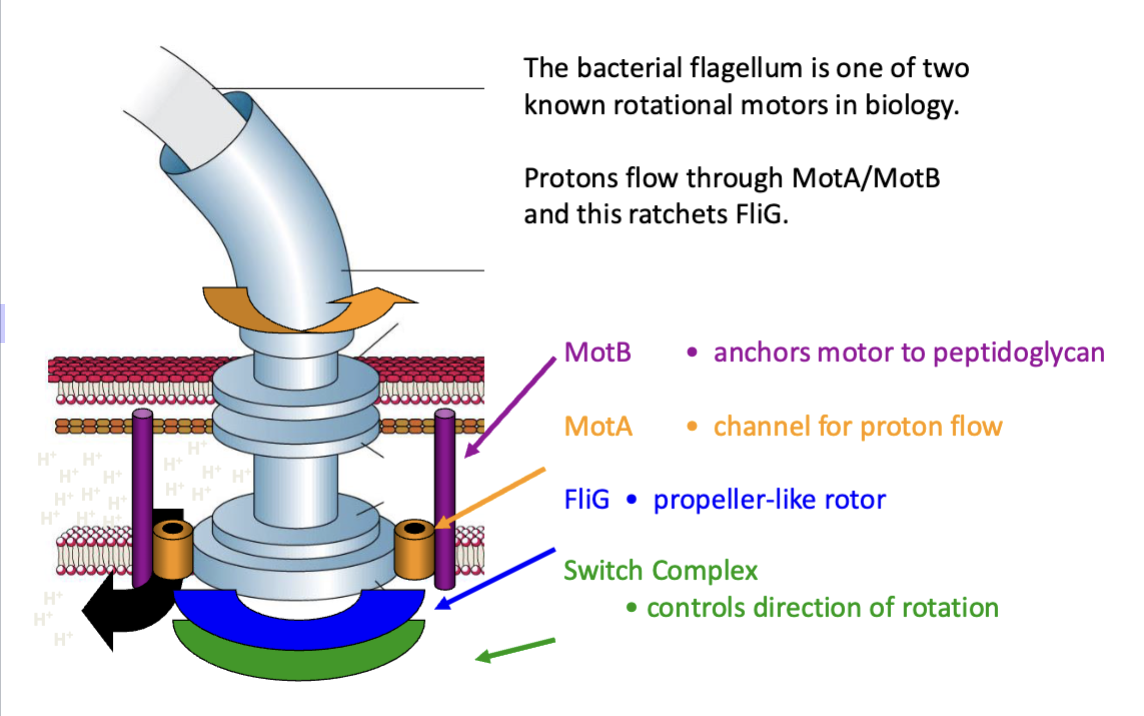
The bacterial flagellum is one of two known rotational motors in biology.
Protons flow through MotA/MotB and this ratchets FliG.
MotB- anchors motor to peptidoglycan
MotA- channel for proton flow
FliG- propeller-like rotor
Switch complex- controls directions of rotation
Neisseria: Opa
Opa proteins are outer membrane proteins that bind to cell surface proteins
antigenic variation: At least five different genes. Expression is regulated by phase variation.
Neisseria: Porin
Trimeric structure found in outer membrane
Nutrient acquisition
Recognized by TLR2
Binds and neutralizes effects of components of the complement cascade
Resists complement opsinization
ooperate with pili to help with internalization by neutrophils
Can translocate into host cells and modulate ROS production and apoptosis.
Strains of the same species can express different porins
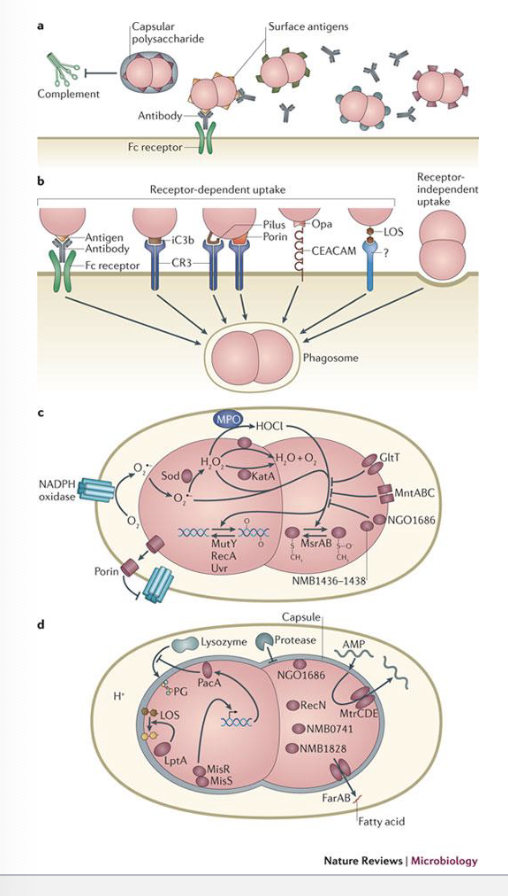
Describe the three general mechanisms that neutrophils use to take up microorganisms.
Opsonin-dependent (complement and antibodies) – inhibited by Neisseria
Opsonin-independent (receptor interaction and phagocytosis) – mediated by Neisseria
Receptor independent – phagocytosis, trigger not defined
Describe the various interactions of Neisseria with neutrophils
• How is it taken up be the neutrophil?
• How does it inhibit specific neutrophil mechanisms that typically inhibit/destroy microorganisms?
Once microbe is inside the neutrophil releases reactive oxygen species (ROS) that should kill the bacteria
Neisseria have ways to inhibit ROS production and action
They detoxify ROS by the production of specific enzymes (catalase, superoxide dismutase)
Increased use of oxygen by bacteria blunts ROS production and porin translocates to cellular membranes and disrupts ROS production
Non-oxidative killing occurs through antimicrobial peptides, proteases and lysozyme (cell wall disruption)
Neisseria encode enzymes that modify the LOS and peptidoglygan to protect the bacteria from these factors
Multiple transferable resistance system (MtrCDE) removes antimicrobial peptides from the phagosome
Describe the various interactions of Neisseria that inhibit the adaptive response
-express IgA1 protease that degrades mucosal antibody.
-Inhibits CD4+ cell function (T-helper, macrophage) and kills B-cells
-Dendritic cells do not fully activate, so response is muted
Overall a suppressed local response to infection contributing to bacterial persistence
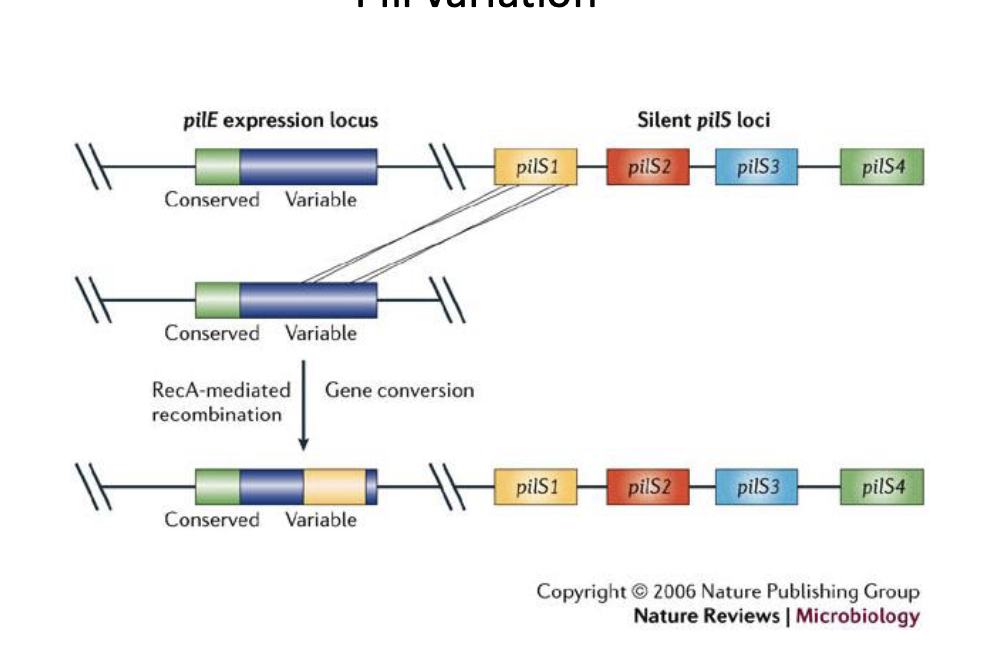
Neisseria: Pili
Type IV pilus for movement and adherence to epithelium
PilC attaches to epithelial cells through interaction with a host surface protein (CD46)
The pilus is also required for natural competence. Takes up DNA
antigenic variation: multiple copies of pilE stored and silent. Can be switched into transcriptionally active site to change pilE type
Neisseria: LOS
LOS is displayed on the surface of the bacterial cell
Analogous to LPS in other Gram negatives
Recognized by TLR4
Endotoxin
Highly stimulatory to the human immune system
Protects against antimicrobial peptides
Adheres to the asialoglycoprotein receptor on urethral cells
Specific LOS modifications (certain sugars) prevent complement deposition and phagocytosis
antigenic variation: Strains of the same species produce different LOS glycoforms by changing the expression of the glycosyltransferases they use.
Describe the first observations of AIDS (i.e., when and where were the first cases observed, what symptoms were displayed)
On June 5, 1981, the CDC published a brief but significant article in its weekly bulletin
• reports of five young men who were all sexually active, gay, and suffering from Pneumocystis pneumonia.
• considered the unofficial beginning of the AIDS epidemic in the United States.
On July 3, 1981, another article appeared, this time describing Kaposi’s sarcoma as well as pneumocystosis in 26 young homosexual men from New York City, and California.
• All had been diagnosed during the previous 30 months.
• Kaposi’s sarcoma is normally a relatively mild skin cancer affecting mainly older men of Mediterranean descent, but in these 26 patients, it was aggressive and deadly.
Commonalities:
Sexually active homosexual men
Rare diseases caused by generally benign organisms/pathogens
Wasting
Low CD4+ T-cell count
Define AIDS
HIV+ individuals with:
• a CD4+ T-cell count less than 200/ul of blood
OR
• CD4+ T-cells accounting for less than 14% of total lymphocytes
OR
• suffering from one of 26 diseases, now including invasive cervical cancer and recurrent pneumonia (both more prevalent in women)
Explain the key factors that lead to the AIDS epidemic
Origins and Early Spread
HIV originated from (SIV) in primates in Central Africa early-to-mid 20th century.
Unprotected Sexual Practices
Injection Drug Use
Blood Transfusions and Medical Practices
Social Stigma and Government Inaction
Lack of Early Awareness
Globalization and Healthcare Inequities
Lack of Effective Treatments
Economic Disparities
Define retroviruses
A virus that uses an enzyme called reverse transcriptase to convert its RNA into DNA. The retrovirus then integrates its viral DNA into the DNA of the host cell, which allows the retrovirus to replicate.
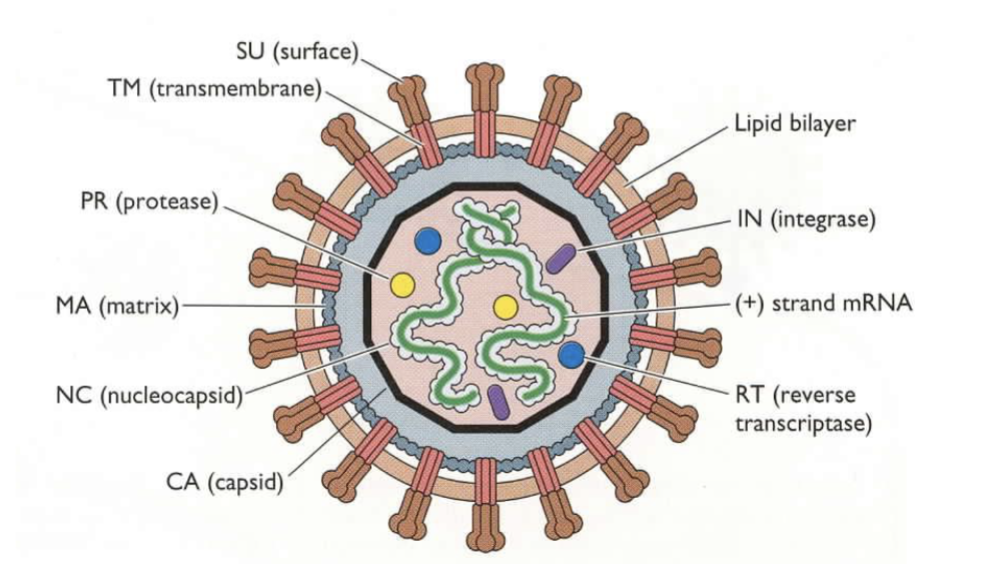
identify key particle components of HIV
Glycoproteins (SU, TM)
Gag proteins (MA, NC, CA)
Genome – 2 copies + tRNA
Enzymes – RT, IN, PR
Explain the origins of HIV
Current data indicate that SIVs have crossed species to humans at least 12 times giving rise to 4 HIV-1 groups (M, N, O and P), and 8 HIV-2 groups (A-H). Only HIV-1M has become pandemic.
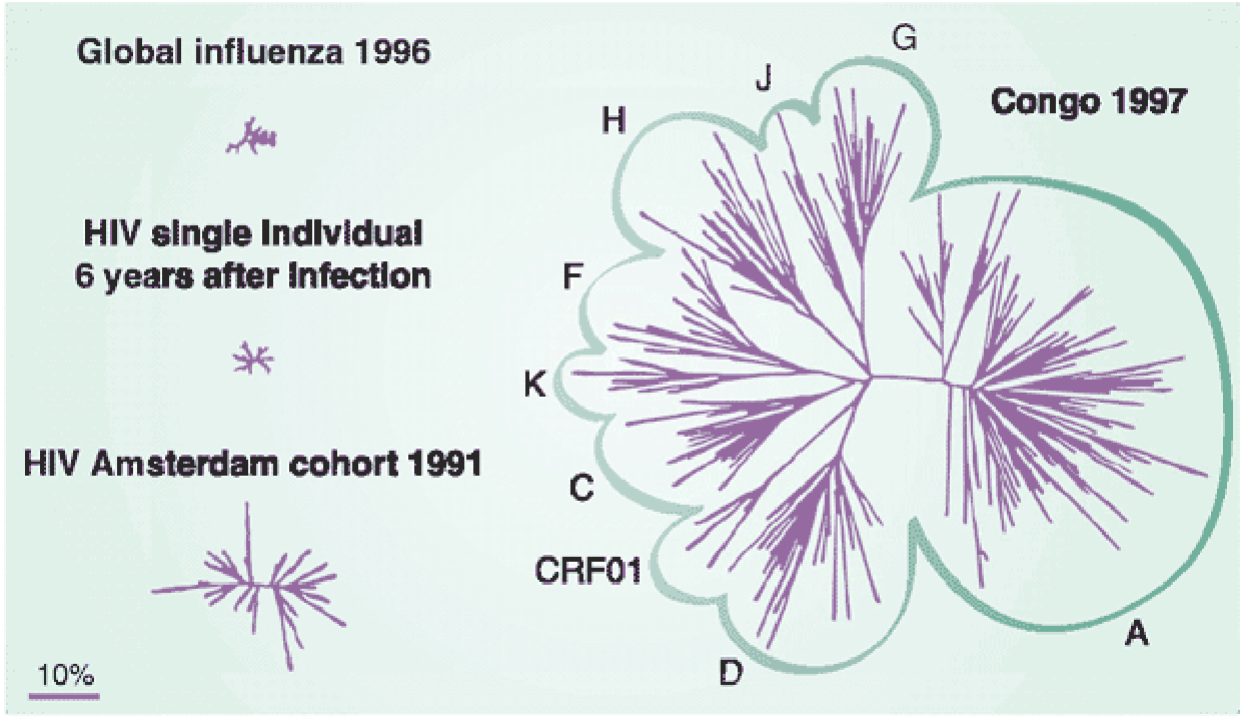
Explain the diversity of HIV and the drivers of speciation
Polymerase error rate
• RT makes mistake appx once every 10,000 nt
• “Hot spots:” certain regions of the genome have an error rate that is 500 times higher
• Quasi-species: exists as a complex mixture of closely related variants
Selective pressure
• Host immune responses and antiretroviral therapy drive the evolution of HIV variants with advantageous traits
Isolation and new environments (new host)
• HIV populations can diverge when isolated or when introduced into new hosts, leading to distinct viral lineages
Founder effect
• When a small subset of the viral population, establishes a new infection, the genetic diversity is reduced, potentially influencing future evolution
Define and describe the HIV provirus
the viral DNA form of HIV integrated into the host cell’s genome via the enzyme integrase.
forms after reverse transcription of the viral RNA
remains a permanent, latent part of the host's DNA.
can stay dormant, evading immune detection, or become active, producing new viruses.
identify the different receptors and co-receptors used for HIV infection
• Describe how the co receptor usage correlates with the transition to AIDS
primary receptor: CD4
Co-receptors: CCR5 on dendritic cells, macrophage and activated Th-cells (early stage)
CXCR4 on non-activated Th-cells (late stage)
Change in co-receptor usage correlates with transition to AIDS
Identify the viral protein used for attachment
gp120
binds to CD4 on the cell surface
undergoes a conformational change that exposes regions that bind to chemokine receptor
binding of chemokine receptor changes solvent exposure of gp41 and induces a conformational change that expose gp41 fusion peptide
Describe the mechanism of action of various attachment inhibitors
CCR5 Inhibitor: Maraviroc binds to and changes the shape of coreceptor CCR5 such that it is not recognized by the gp120 coreceptor binding sites
gp120 Inhibitors: temsavir binds to the gp120 site required for CD4 attachment, blocking viral entry.
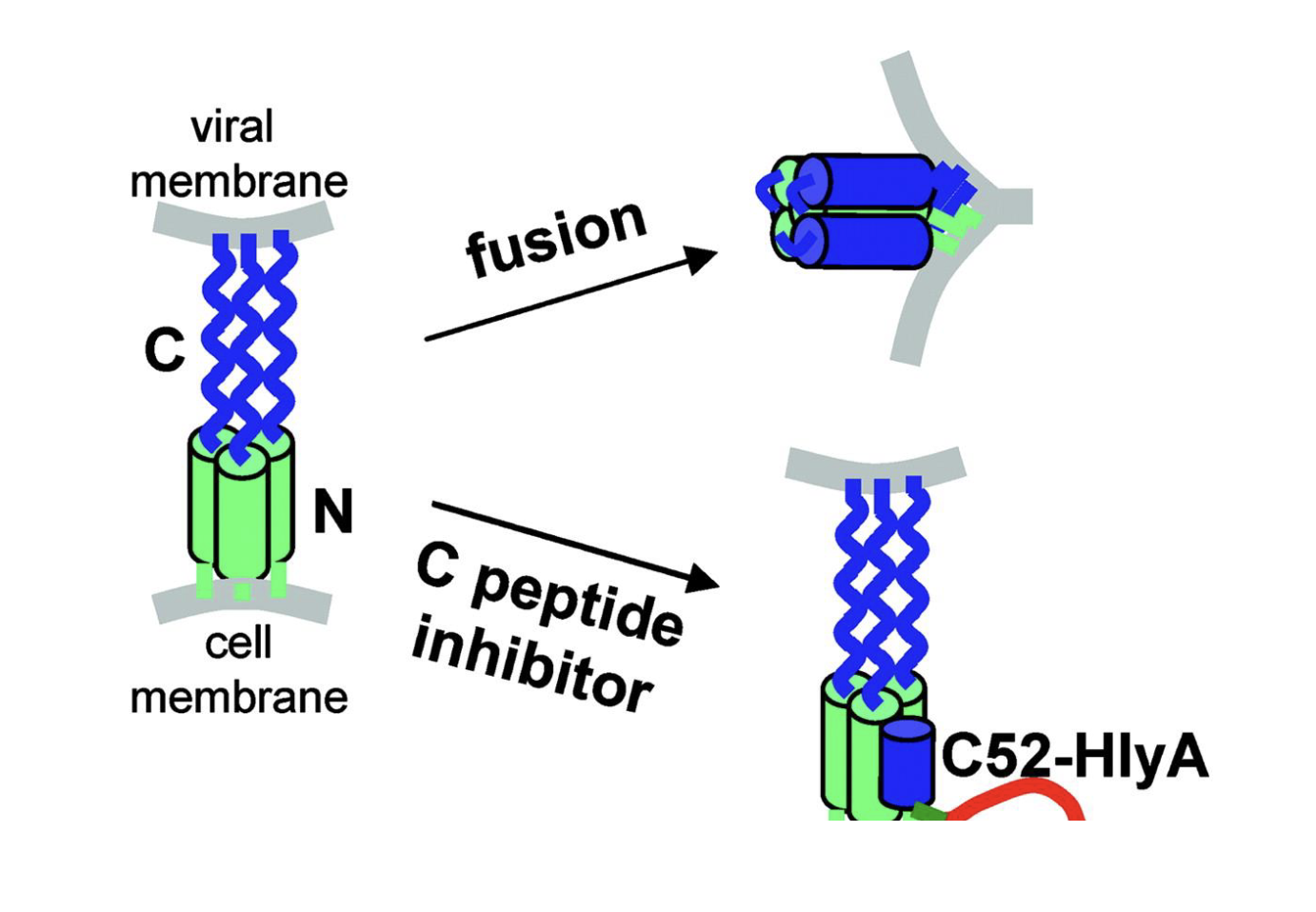
identify the viral fusion protein
The viral fusion protein of HIV is gp41.
It is part of the HIV envelope glycoprotein complex (along with gp120). After gp120 binds to the CD4 receptor and co-receptor (CCR5 or CXCR4), gp41 facilitates the fusion of the viral and host cell membranes, allowing the viral capsid to enter the host cell.
Describe the fusion mechanism used by HIV
Attachment: The viral gp120 binds to the CD4 receptor on the host cell, followed by interaction with a co-receptor (CCR5 or CXCR4).
Conformational Change: Binding to the co-receptor triggers structural changes in the envelope protein complex, exposing the gp41 fusion protein.
Insertion: The fusion peptide of gp41 inserts itself into the host cell membrane.
Formation of a Fusion Complex: gp41 folds back on itself, forming a six-helix bundle. This structure brings the viral envelope and host cell membrane into close proximity.
Membrane Fusion: The two membranes merge, creating a pore through which the viral capsid enters the host cell.
Describe the mechanism of action of fusion inhibitors
Targeting gp41: Fusion inhibitors bind to the gp41 protein and prevent it from forming the six-helix bundle needed for membrane fusion.
Blocking Membrane Fusion: By disrupting the structural changes in gp41, the viral envelope cannot merge with the host cell membrane, halting the entry of the viral capsid into the cell.
Describe the mechanism of action of the capsid inhibitor
Multi-stage target: binds to the viral capsid protein and prevents nuclear transport, virus assembly and release, and capsid assembly in new virions
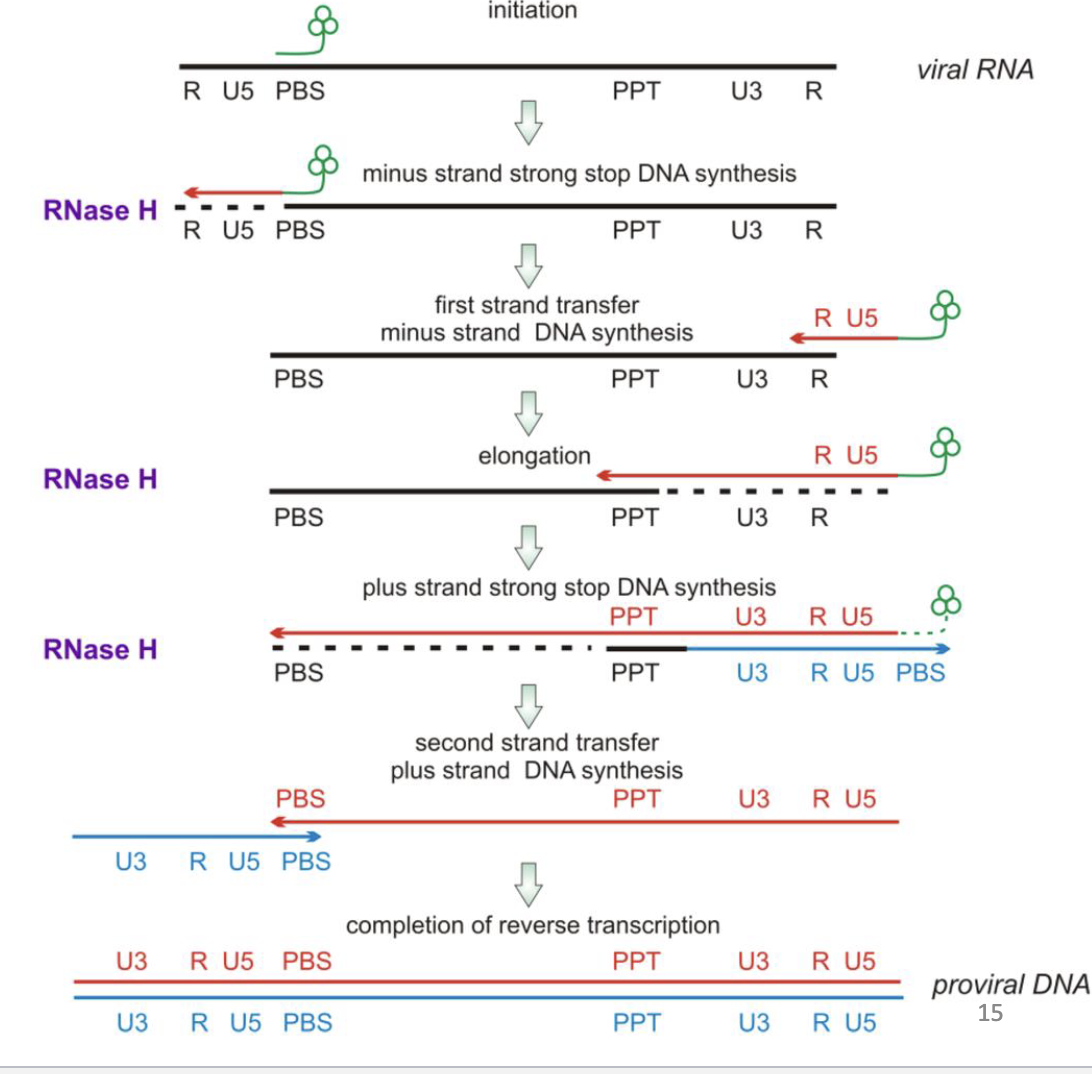
Describe how reverse transcriptase creates proviral DNA from the positive sense RNA genome
1. Synthesis of the Minus-Strand DNA (First Strand)
RT uses the viral RNA genome as a template and a host tRNA molecule as a primer.
It synthesizes a complementary DNA strand (minus-strand DNA) from the RNA template, moving in the 5′ to 3′ direction.
As RT synthesizes DNA, it degrades the RNA template through its RNase H activity, except for a small RNA fragment called the polypurine tract (PPT).
2. Synthesis of the Plus-Strand DNA (Second Strand)
The remaining RNA PPT fragment acts as a primer for the synthesis of the complementary DNA strand (plus-strand DNA).
RT synthesizes this second strand using the newly created minus-strand DNA as a template.
3. Formation of Double-Stranded Proviral DNA
RT facilitates strand transfer and recombination events, ensuring the ends of the DNA (long terminal repeats or LTRs) are properly aligned and completed.
The resulting proviral DNA is a linear, double-stranded molecule containing LTRs at both ends, which are crucial for integration into the host genome.
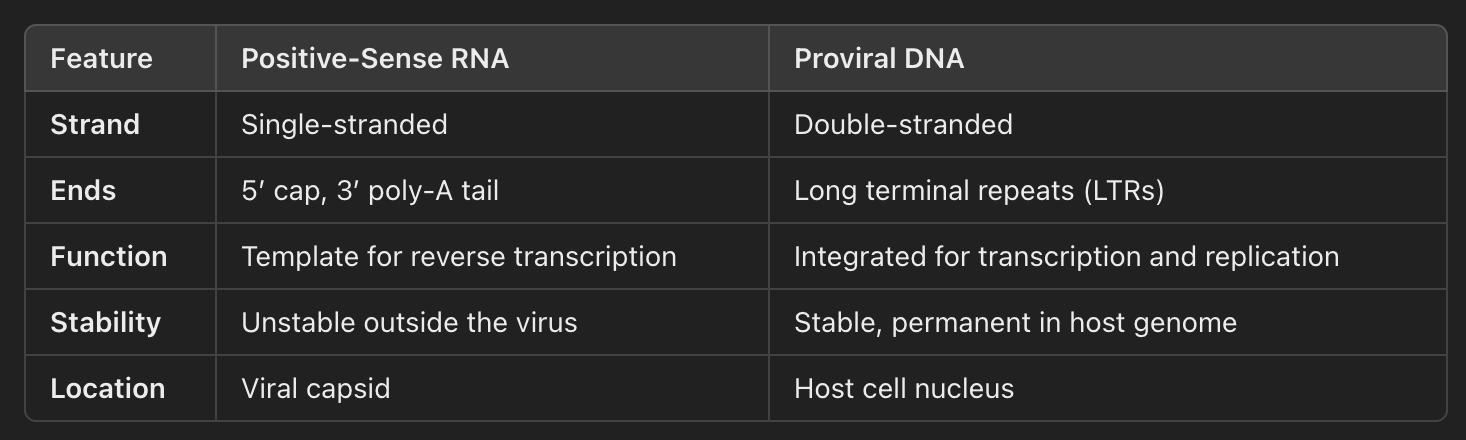
Compare and contrast the structural features of the positive sense RNA genome vs the proviral DNA
Describe the mechanism of action of NRTI and NNRTIs
NRTIs are nucleoside analogs that mimic DNA building blocks. They get incorporated into the viral DNA during reverse transcription and block elongation due to the lack of a 3’-OH
NNRTIs bind NON-COMPETITIVELY near the RT active site causing structural changes that inhibit the efficiency of nucleotide addition
Describe the function and mechanism of action of integrase
Integrase (IN)
• Catalyzes viral DNA integration into the host chromosome, by performing a series of DNA cutting and joining reactions
• Begins with site-specific endonucleolytic cleavage of the 3’-OH ends of the viral DNA
• Then assembles the pre-integration complex (PIC), along with other viral and cellular factors, on the ends of the viral DNA, which migrates into the host nucleus.
• IN catalyzes the insertion of the viral DNA into host chromosomal DNA (strand transfer step)
• Integrase inhibitors traditionally target the strand transfer step (INSTI)
Describe how HIV transcription within the host
Steps of HIV Transcription:
Activation of Proviral DNA:
After integration, the proviral DNA remains latent but can be activated by host cell signals
NF-κB, Sp1, and other host transcription factors bind to the LTRs, initiating transcription.
Transcription by Host RNA Polymerase II:
The host RNA polymerase II enzyme transcribes the proviral DNA into a long RNA transcript.
This RNA includes both the genomic RNA (for packaging into new virions) and the mRNA for viral protein synthesis.
Processing of RNA:
The full-length RNA is spliced by host machinery to produce different types of mRNA, including:
Full-length genomic RNA: Used to produce new viral genomes.
Spliced mRNAs: Used to produce viral proteins (e.g., Gag, Pol, Env).
Translation and Packaging:
The viral mRNAs are translated into viral proteins by the host cell’s ribosomes.
The full-length genomic RNA is packaged into new virions along with viral proteins (Gag, Pol, Env).
Compare and contrast gag vs gag-pol
• Make sure you know the components of each
Polyprotein – large protein that is cleaved into smaller proteins in a temporally defined way.
Uncleaved and cleavage intermediates may have distinct functions from fully processed
products.
Gag-Pol production requires a -1 frameshift during translation to access the pol “ORF”
GAG: Polyprotein responsible for packaging genome, forming internal structure of the virus particle, and acquisition of lipid bilayer.
Describe the function of MA, CA, and NC (part of GAG)
MA interacts with membranes and gp41 cytoplasmic tails
CA forms “cage” around the viral RNA genome
NC binds to viral genomic RNA
Describe the role and process of HIV maturation.
The virus that is initially released is non-infectious
Cleavage of Gag and Gag-Pol by the viral protease is required for infectivity
This leads to an observable morphological change
Gag initially arranged like spokes
Cleavage liberates individual proteins
CA forms conical structure surrounding NC-RNA complex
Describe the function and mechanism of action of HIV protease
cleaves the viral polyproteins (Gag and Gag-Pol) into functional proteins, enabling virion maturation.
produces structural proteins (e.g., Capsid, Matrix) and enzymes (e.g., Reverse Transcriptase, Integrase) required for assembling infectious particles.
Describe the mechanism of action of protease inhibitors
Binding to Protease:
PIs bind to the active site of HIV protease, mimicking the natural substrates (polyproteins) but resisting cleavage.
Inhibition of Cleavage:
By occupying the active site, PIs prevent the protease from cleaving the viral polyproteins into structural proteins (e.g., Capsid, Matrix) and enzymes (e.g., Reverse Transcriptase, Integrase).
Production of Immature Virions:
Without proper cleavage, the virus produces immature, non-infectious particles that cannot infect new cells.
Explain the difference between susceptible and permissive
susceptible - virus can attach and enter cell
determined by extracellular components of host cell
permissive - virus can replicate and produce infectious progeny
determined by intracellular environment of host cell
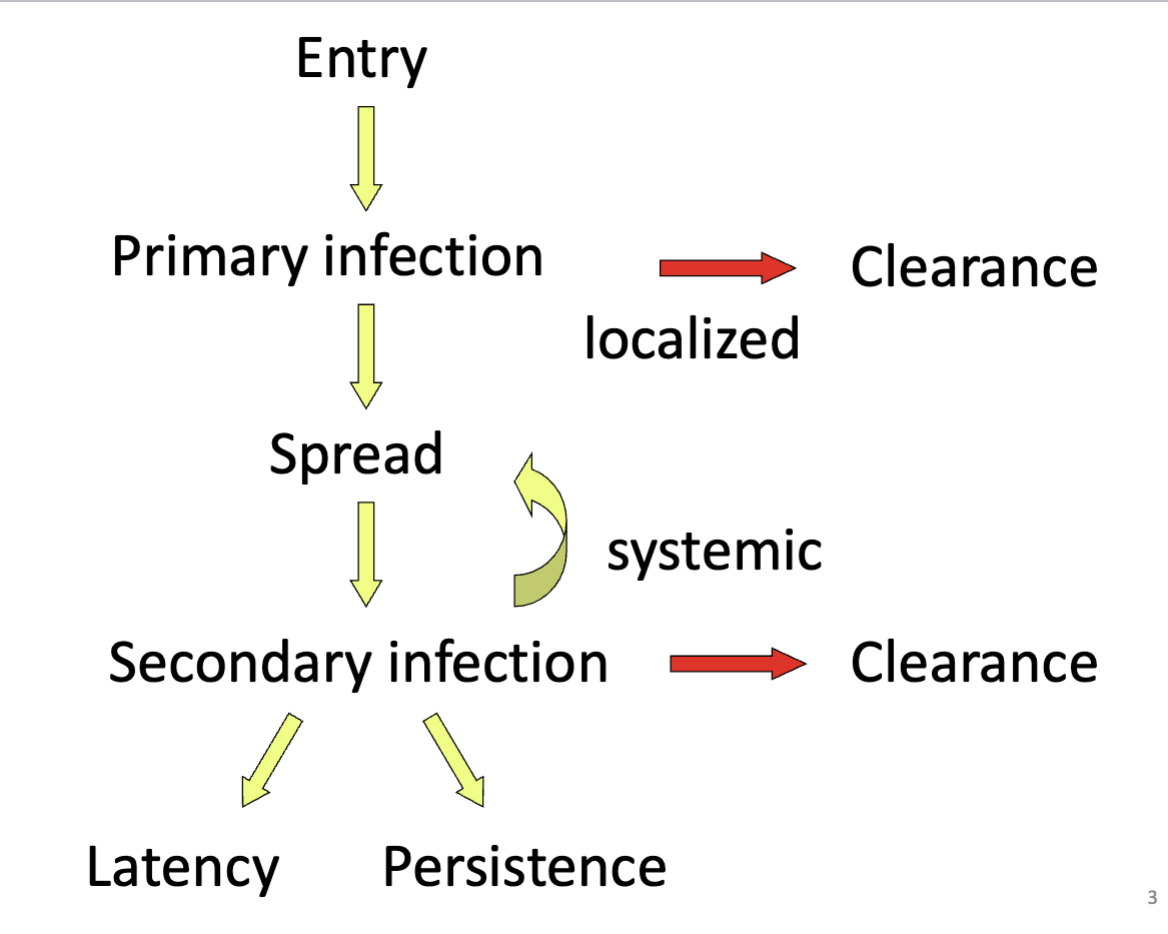
Describe the pathway from primary infection to latency
Explain the different methods that HIV uses to infect/breech epithelial cells
Physical damage:
- Access to underlying tissue (macrophage and dendritic cells)
- Stimulates inflammatory response
- Sex creates a mild inflammatory response
Antigen presenting cells:
- Tissue specific macrophage and DCs either become infected or sequester HIV
Transcytosis:
- M-cells sample lumen of gut and transport antigen to basolateral surface to lymphoid foci (Peyer’s patches)
Transmigration:
- APC transit across epithelial barrier
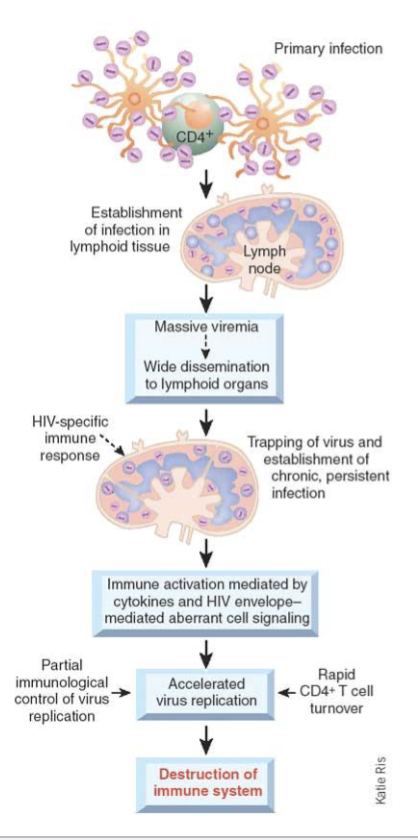
Explain how initial HIV infection leads to systemic spread
APCs possessing antigen migrate to lymphoid centers
DCs are primarily responsible for bringing HIV to lymph nodes.
High-level replication of HIV in lymph node along with expansion of follicular DC which trap HIV in node, leads to lymphadenopathy (swollen or enlarged lymph nodes)
Infection of macrophage and T-h cells increases
Increased tissue pathology in lymph node results in follicular involution (loss of tissue integrity) and increase in viremia
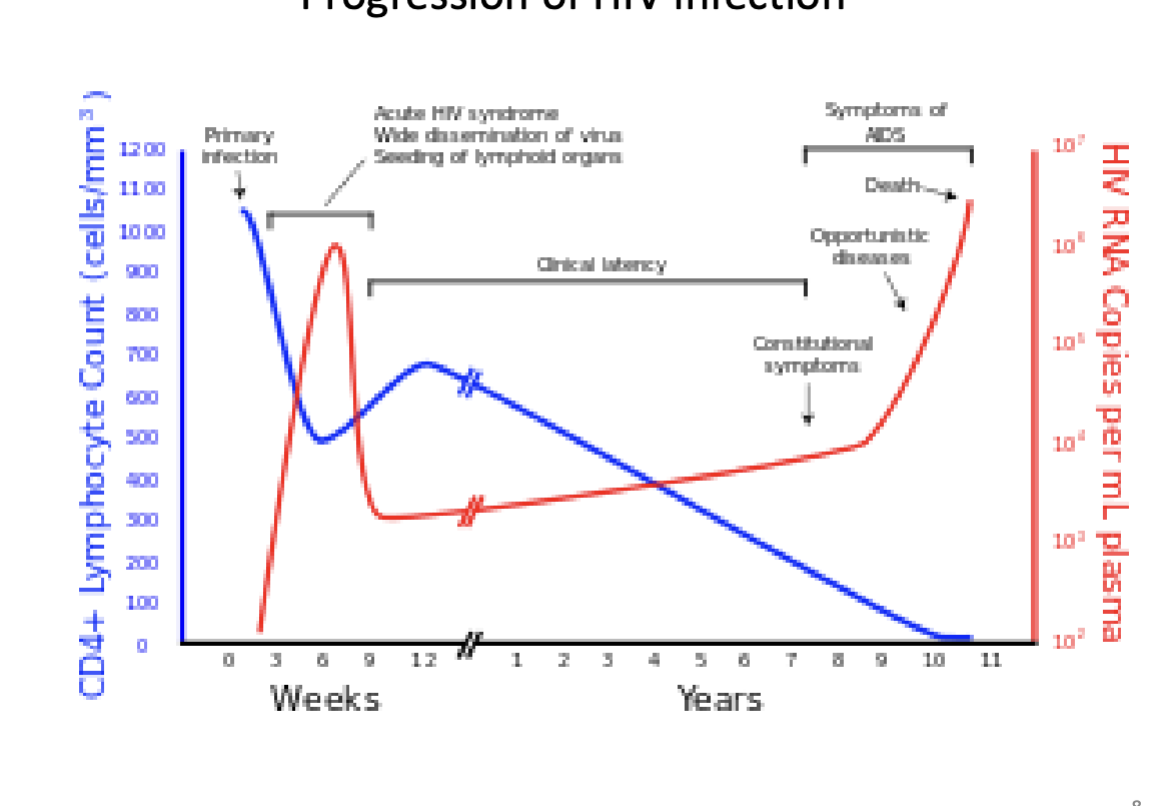
Describe the different stages of HIV progression
Pay close attention to the differences between RNA replication vs CD4+ cell count at each stage
Describe the role of dendritic cells in HIV infection and progression to AIDS
HIV Capture: Dendritic cells (DCs) capture HIV through surface receptors, often without becoming infected.
Virus Transport: DCs transport HIV to lymph nodes, where they efficiently transmit the virus to CD4+ T cells, amplifying infection.
Immune Evasion: HIV exploits DCs to avoid immune detection, using them to spread rather than trigger effective antiviral responses.
Chronic Activation: DCs contribute to immune activation by producing inflammatory signals, which accelerate T-cell depletion and immune system exhaustion.
Progression to AIDS: By facilitating early infection, viral spread, and chronic inflammation, DCs play a key role in weakening the immune system and advancing the disease.
Describe the role of macrophage cells in HIV infection and progression to AIDS
HIV Entry: Macrophages, expressing CD4 and CCR5, are early targets for HIV and act as reservoirs due to their resistance to cell death.
Viral Reservoirs: They sustain long-term infection and spread the virus to tissues like the brain and lymph nodes.
Immune Dysfunction: Infected macrophages release HIV and inflammatory cytokines, depleting CD4+ T cells and causing chronic inflammation.
AIDS Progression: By maintaining viral replication and disrupting tissue repair, macrophages drive immune failure and opportunistic infections.
Describe the role of activated T helper cells in HIV infection and progression to AIDS
Origin – lymphoid, thymus
Function – expansion of adaptive immune response, both humoral and cell-mediated
Cell surface markers – CD4, CCR5 (activated), CxCR4 (non-activated)
HIV infection – activated T-h cells infected largely in the lymph node. In late HIV infection all T-h cells can be infected. Resting T-h cells may act as reservoir when no HIV gene expression is occurring
Describe the role of progenitor stem cells in HIV infection and progression to AIDS
Origin – they are derived from self renewing stem cells
Function – give rise to lymphoid and myeloid lineages
Cell surface markers – CD34, CD4, CD8, MHC-1......
HIV infection – act as long term reservoir for HIV proviral DNA. HIV particles can be produced following certain differentiation signals.
The finding that these cells contain integrated proviral DNA is concerning as they are are long-lived, and store the virus in a manner that prevents clearing using antivirals, but virus can be re-activated
Explain the importance of the switch in co-receptors for pathogenesis
switch from CCR5 to CXCR4 accelerates HIV pathogenesis.
Early infection: CCR5-tropic strains, which primarily infect macrophages and memory CD4+ T cells.
late infection: CXCR4-tropic strains emerge, targeting a broader range of CD4+ T cells, including naïve cells.
This switch leads to faster CD4+ T cell depletion, increased cytopathicity, and rapid progression to AIDS.
Explain HAART and current treatment plans
Highly active antiretroviral therapy (HAART)
Use of multiple drugs to combat virus, slows the emergence of resistant virus
Usual therapy:
3 drugs – 2 NRTIs
1 from the following: INSTI, NNRTI, or PI
Combinations are important, resistance to one inhibitor may lead to resistance to others, or may lead to sensitivity to others.
If an individual is tested positive for HIV, they can get tested to determine the CD4 count.
• When CD4 drops below 200 cells/μL, the patient should also be treated with antibiotics to prevent bacterial infections.
•goal: find a treatment regimen w he least amount of side effects and reduces HIV viral load the most.
• Viral suppression = less than 200 copies of HIV per milliliter of blood.
• Successful treatment leads to “undetectable” level of HIV and no risk of HIV transmission. However, HIV is still dormant in small number of reservoir cells and patient must continue therapy for remainder of life to maintain “undetectable” status.
• Continual testing of the viral load will be done every 3-4 months to determine how well your treatment plan is working.
Describe the problems of drug cost and supply
lifetime cost of treating one HIV+ American is ~$420, 295
As of 2023, 30.7 million people globally with HIV were accessing ART (77%)
explain the difference between PEP and PrEP
PEP (post-exposure prophylaxis)
– Emergency situations
– Started with 72 hours after exposure
– 4 week course of medication
PrEP (pre-exposure prophylaxis)
– People at risk for HIV take daily medicines to prevent HIV
explain the different modes of transmission and preventative mechanisms associated with each
1. Blood-blood – IVDU, transfusions and blood products
Viable prevention methods: needle exchange programs, blood testing, donor restriction
2. Sexual – Heterosexual and homosexual
Viable prevention methods: ABC, abstinence, monogamy, condom use
3. Mother-child – in utero, intrapartum, breast feeding
Viable prevention methods: HAART during pregnancy (26%>2%), C-section delivery, formula feeding
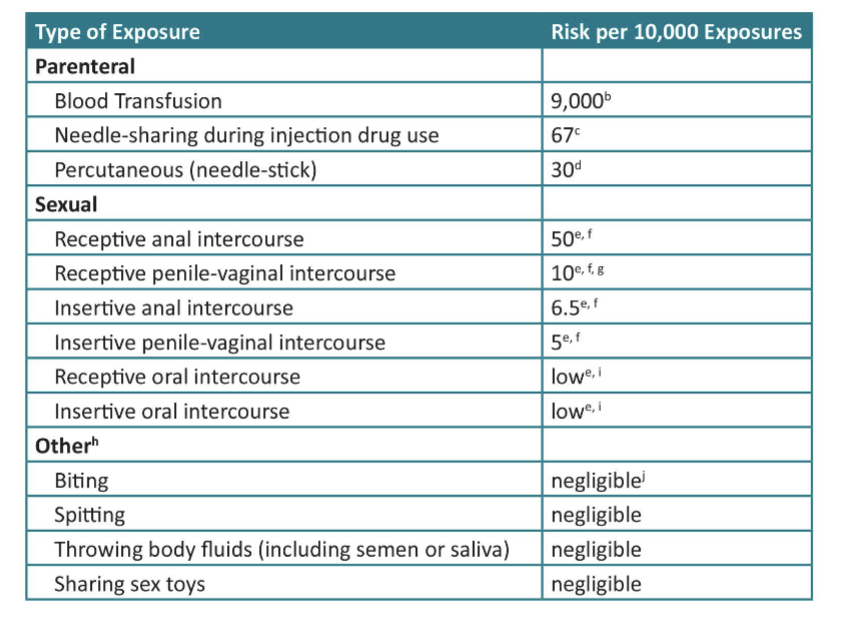
HIV explain the risk associated with different types of exposure
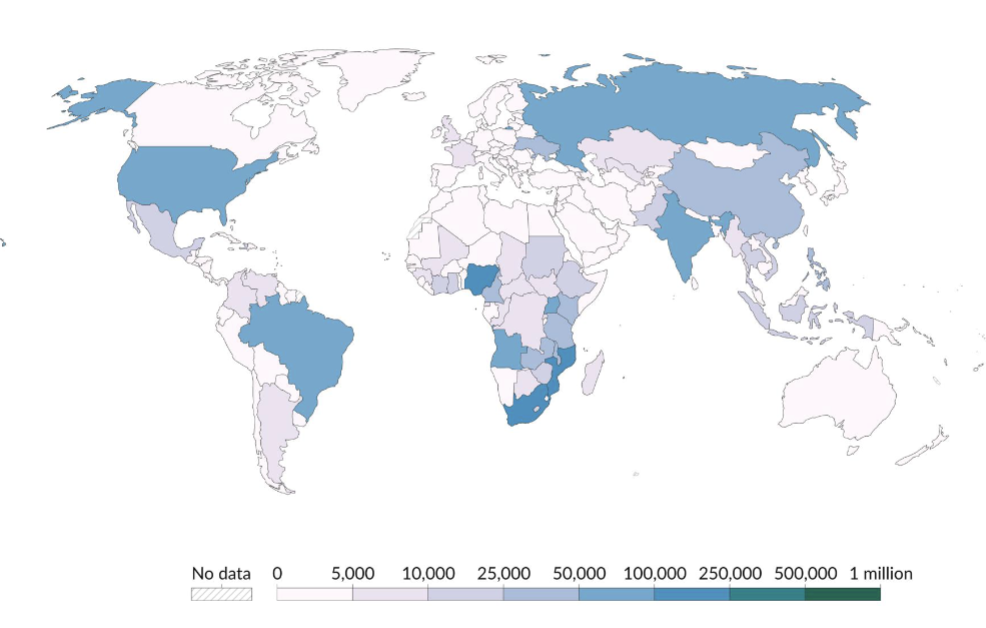
Describe the current trends in new HIV infections globally and in the US
US: half of new causes in the south
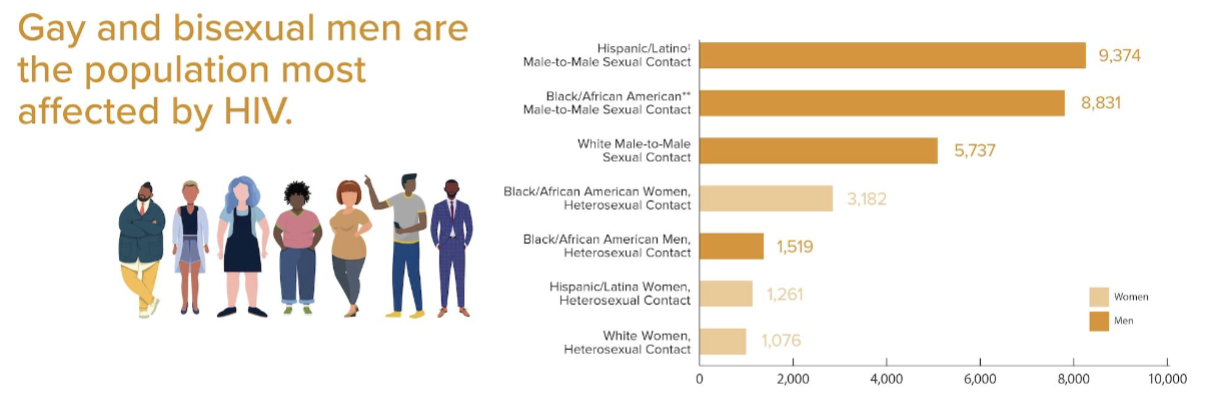
describe the groups most at risk in U.S.
explain contributing factors to transmission
Stigma – coming out is difficult, homophobia, “moral” judgment
- being HIV+ carries an additional stigma
- impacts physical and mental health, ability to make healthy choices (drug use)
- isolation, difficulty integrating into social networks
Poverty – access to health care
- education, more educated more likely to know status
- socioeconomic status inversely correlates with HIV prevalence
Complacency – belief that HIV is not a death sentence
- underestimating effects on quality of life
- availability of medicine
- underestimating personal risk
Recreational drugs - Methamphetamine is a huge problem in increased risk behavior.
- Its cheap, long lasting high, inhibitions reduced, libido & endurance increased
- It is estimated that 12 million people in the US over the age of 12 have tried meth.
That’s 1 in 20 over age 12!!!
One study showed that 20% of urban MSM had used in the prior 6 months.
explain the 95-95-95 target and its importance in the AIDS epidemic
Adopted by United Nations Member States in June 2021
• Achieving this target would end AIDS epidemic by 2030
• By 2025:
– 95% of all people living with HIV will know their HIV status
– 95% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy
– 95% of all people receiving antiretroviral therapy will have viral suppression
Describe the key priorities of the Global AIDS Strategy
End inequalities. End AIDS.
Outlines framework to address inequalities that are preventing progress to ending AIDS epidemic
Goal is to get every country on track to end AIDS epidemic by 2030