Cancer Genetics - Hereditary Polyposis Colorectal Cancer Syndromes
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
12 Terms
APC Associated Polyposis Conditions
Familial Adenomatous Polyposis (FAP)
Attenuated FAP (AFAP)
Gastric Adenocarcinoma and Proximal Polyposis of the Stomach (GAPPS)
Familial Adenomatous Polyposis
FAP
APC
Autosomal dominant
De novo rate: 20 - 25%
Characterized by hundreds to thousands of adenomatous colonic polyps
Colorectal adenomatous polyps begin to appear in 20s to 30s
Average age of polyp diagnosis is 16 years
By 35 years old, 95% of people with FAP have polyps
Without colectomy, colorectal cancer is inevitable
The average age of colorectal cancer in untreated is 39 years old
93% by 50
Non-malignant features
Osteomas - bony growths most commonly found on skull and mandible
Dental abnormalities
CHRPE
Desmoid tumors - benign tumors that are invasive but do not metastasize
Adrenal masses
Attenuated FAP
AFAP
APC on chromosome 5q21
Autosomal dominant
Characterized by fewer colonic polyps than classic FAP but still a significant risk for colorectal cancer
Average of 30 polyps, <100 polyps
Average age of colorectal cancer diagnosis is 50 - 55 years
Cumulative risk for colorectal cancer risk by age 8- is estimated at 70%
Thyroid and duodenal risk similar to classic FAP
Typically no extraintestinal manifestations
Adenomatous Polyposis Testing Criteria
Recommend testing if personal history of one or more of the following:
>= 20 cumulative adenomas
Multifocal / Bilateral Congenital Hypertrophy of Retinal Pigment Epithelium (CHRPE)
Flat, pigmented spot found in the back of the eye
Cribiform-morular variant of thyroid cancer
Family history of polyposis and family unwilling / unable to have testing
Consider testing if personal history of one or more of the following:
Between 10 - 19 cumulative adenomas, desmoid tumors, hepatoblastoma, unilateral CHRPE, or individual meets criteria for serrated polyposis syndrome with at least some adenomas
Gastric Adenocarcinoma and Proximal Polyposis of the Stomach
GAPPS
APC on chromosome 5q21
Autosomal dominant
Characterized by Gastric polyps called Fundic Gland Polyps
Intestinal-type gastric adenocarcinoma: 13 - 25%
Typically no significant duodenal or colorectal polyposis
APC I1307K
Common variant reported in Ashkenazi Jewish population
NOT FAP
MUTYH - Associated Polyposis Syndrome
MAP
MUTYH
Autosomal recessive
Characterized by ten to a few hundred colonic polyps
Sometimes have colorectal cancer with no polyposis
Treatment of manifestations
CRC polyps should be removed
Duodenal polyps should be excised
Thyroid findings should be evaluated by thyroid specialist
Surveillance
Colonscopy
Upper endoscopy and duodenoscopy
Thyroid ultrasound
Individuals with heterozygous MUTYH inheritance
Offer average moderate-risk colorectal screening based on family history
Peutz-Jeghers Syndrome
STK11
Autosomal dominant
Clinical Diagnosis
Two or more Peutz-Jeghers-type hamartomatous polyps of GI tract
Mucocutaneous hyperpigmentation of the mouth, lips, nose, eyes, genitalia or fingers
Family history
Dark blue or brown moles around mouth, eyes, nostrils, and anus
Dark moles on the hands and feet
Individuals with PJS develop hamartomatous polyps
GI - small intestine, stomach, large bowel
Extraintestinal sites - kidneys, lungs, gall-bladder, nose, bladder and ureters
Increased risk for colorectal, intestinal, gastric, pancreatic, breast, cervical, lung, testicular and ovarian cancer
Females are at risk for sex cord tumors and cervical cancer
Males can develop sertoli cell tumors of the testes
Secrete estrogen and can lead to gynecomastia
Juvenile Polyposis Syndrome
BMPR1A and SMAD4
Autosomal dominant
50% of individuals meeting clinical criteria have detectable mutations
Clinical Diagnosis
5+ juvenile polyps (type of hamartoma) of the colon
Juvenile refers to a type of polyp
Multiple juvenile polyps in GI tract
Any number of juvenile polyps with a family history of JPS
Clinical Characteristics
Childhood-onset
Polyps cause iron deficiency anemia and bleeding
Significantly increased risks for cancer (colorectal, stomach, and small intestines
Risk for GI cancer range from 11% to 86%, mostly colon cancer
Hereditary Hemorrhagic Telangiectasia (HHT)
SMAD4 variant
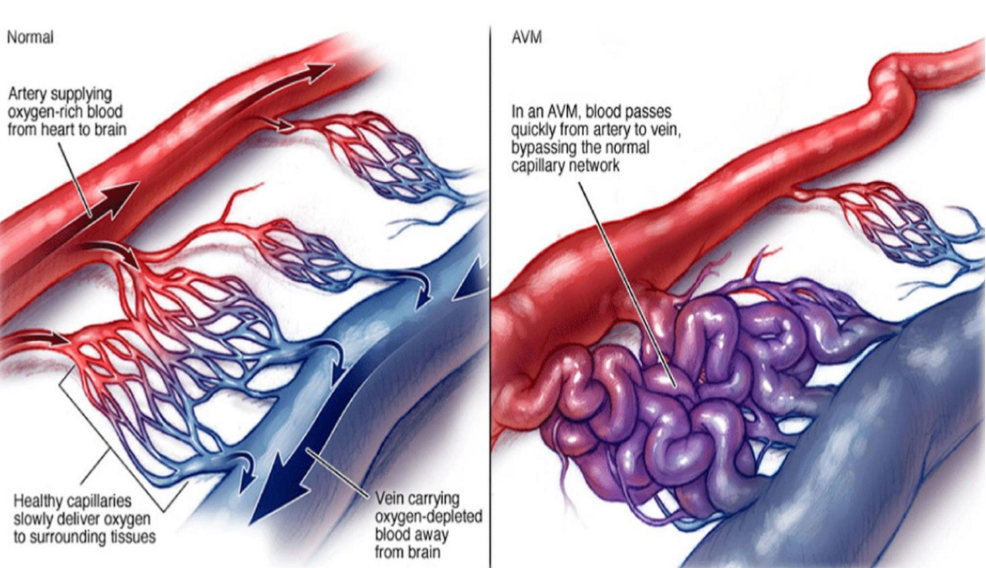
HHT features - arterial-venous malformations (AVMs), epistaxis (nosebleeds), telangiectasias, digital clubbing
Atrial-Venous Malformations
Tangle of blood vessels that irregularly connects arteries and veins
Result from the development of irregular connections between arteries and veins
Serrated Polyposis Syndrome
Increased risks for colorectal polyposis and colorectal cancer
Clinical diagnosis
>=5 serrated lesions / polyps all being >=5 mm in size, with >=2 being >=10 mm in size
>20 serrated lesions / polyps of any size with >=5 being proximal to the rectum
NO clearly causative gene for most cases
Some associations with RNF43 gene have been identified
Biallelic pathogenic variants in MUTYH gene
Colonic Adenomatous Polyposis of Unknown Etiology (CPUE)
Individuals with cumulative lifetime >=10 - 20 adenomas without a PV identified in a polyposis gene
Management / Surveillance
Prior to managing CPUE, multigene testing including all polyposis and colorectal cancer genes should be considered
PVs associated with adenomatous polyposis include but not limited to monoallelic PVs in APC, GREM1, POLE, POLD1 and AXIN2 and biallelic PVs in NTHL1, MUTYH, MBD4, MLH3, and MSH3 genes