PSYC111 module 2 (sensation & perception)
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Sensation, perception
registering of sensory info by the brain
assignment of meaning to that sensory info
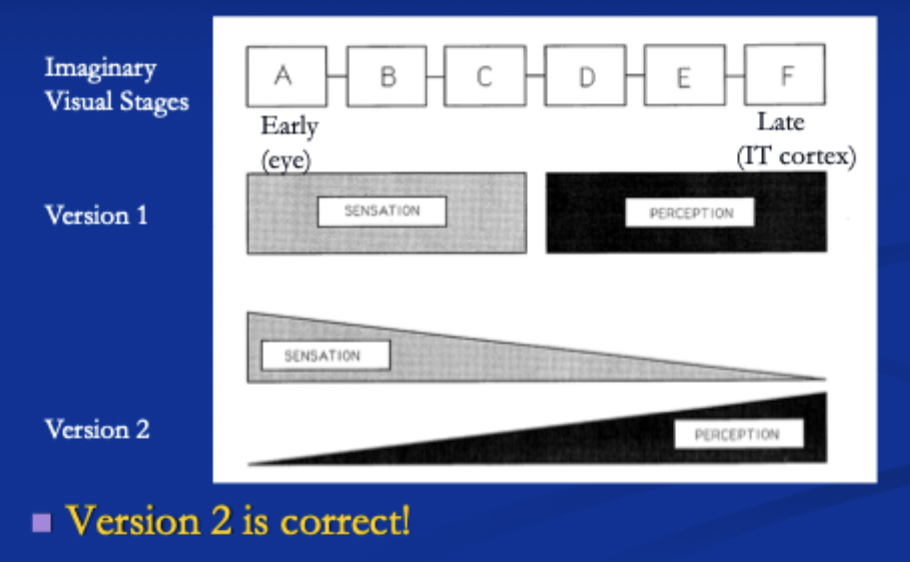
Are sensation and perception the same or different processes?
They all do sensation and perception. Early on in the visual system there is more sensation but there is still a little bit of perception.
As you get to the end of the visual system there is more perception and less sensation
How is sensory info implemented neurally?
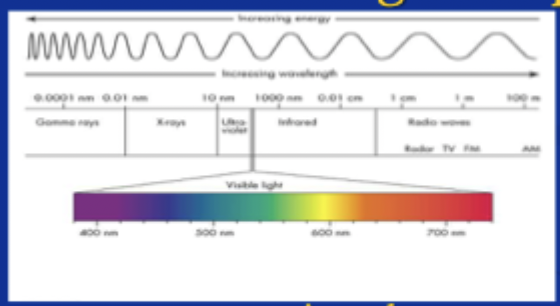
Sensory organs absorb energy
Energy is transduced into neural signal
neural signal sent throughout the brain for further processing
Wavelength, Amplitude
Colour that you see
How bright you see the colour
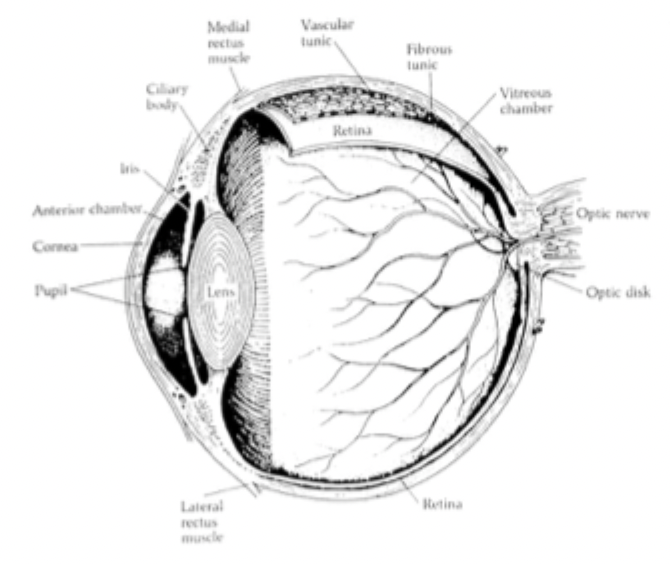
Outer layer of eye
Cornea
Transparent, focuses image on retina
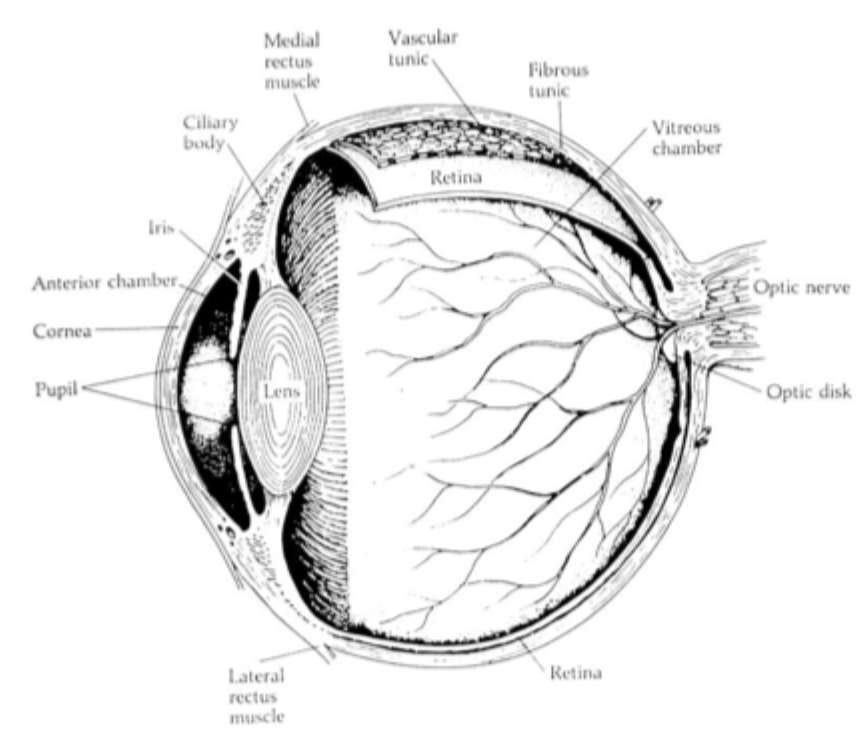
Middle layer of eye
Choroid (vascular tunic)
eye’s blood supply, provides nutrients to keep tissue alive and discards waste
doesn’t cover the whole eye
Fluid is in the anterior and posterior chambers which reaches cornea and lens
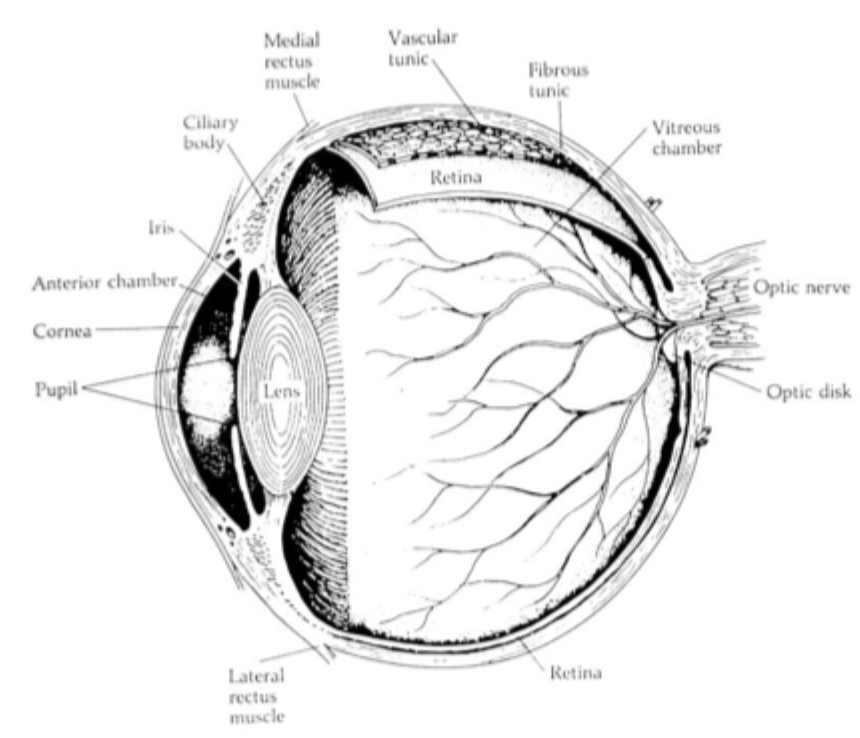
Inner layer of eye, cataracts
Iris= can extend and contract them, this changes the size of your pupil
Pupil= becomes bigger or smaller to let more or less light in
Lens= behind pupil, attached to muscles that pull or push the lens to focus eyes near or far (accommodation)
Cataracts
condition that makes lens cloudy, can make you blind
taking cataracts out will allow them to see again.
If you are born with it and don't take the lens out before the critical visual period of development you still won't be able to see.
retina
Surrounds the eye
Contains photoreceptors (rods & cones) that convert electromagnetic energy into neural signal
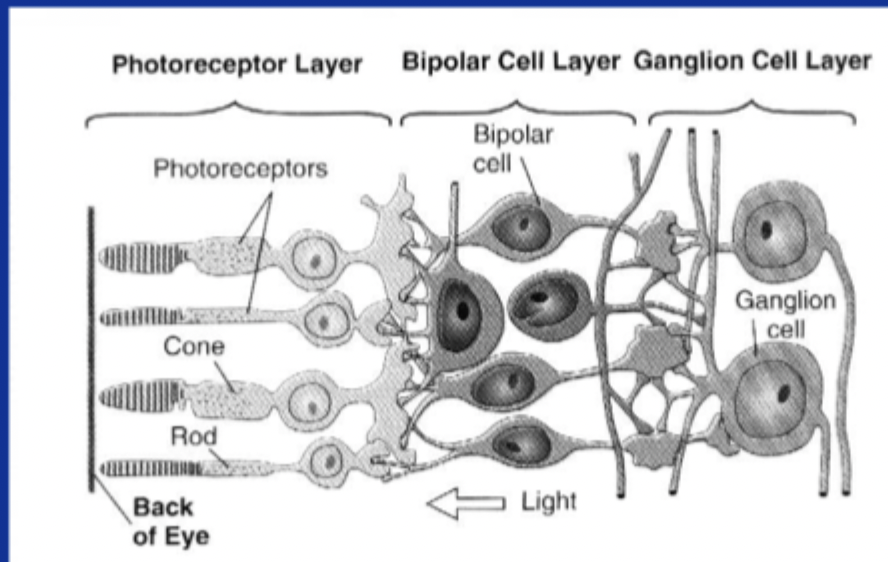
Rods vs cones
Perform transduction (electromagnetic energy → neural signal)
120 mil, no colour, active at night, high resolution, peripheral
7 mil, colour, active during daytime, low resolution, almost all are in fovea, central
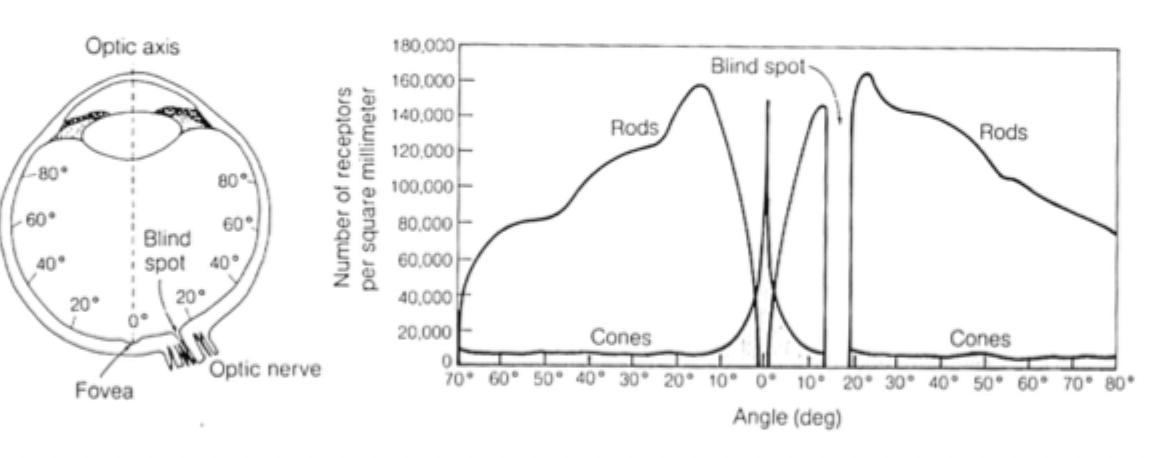
blindspot, Optic nerve, Bipolar cells & retinal ganglion cells
has no photoreceptors, where the axons of the ganglion cells exit the eye
axons of ganglion cells, size of pencil
engage in processing visual image
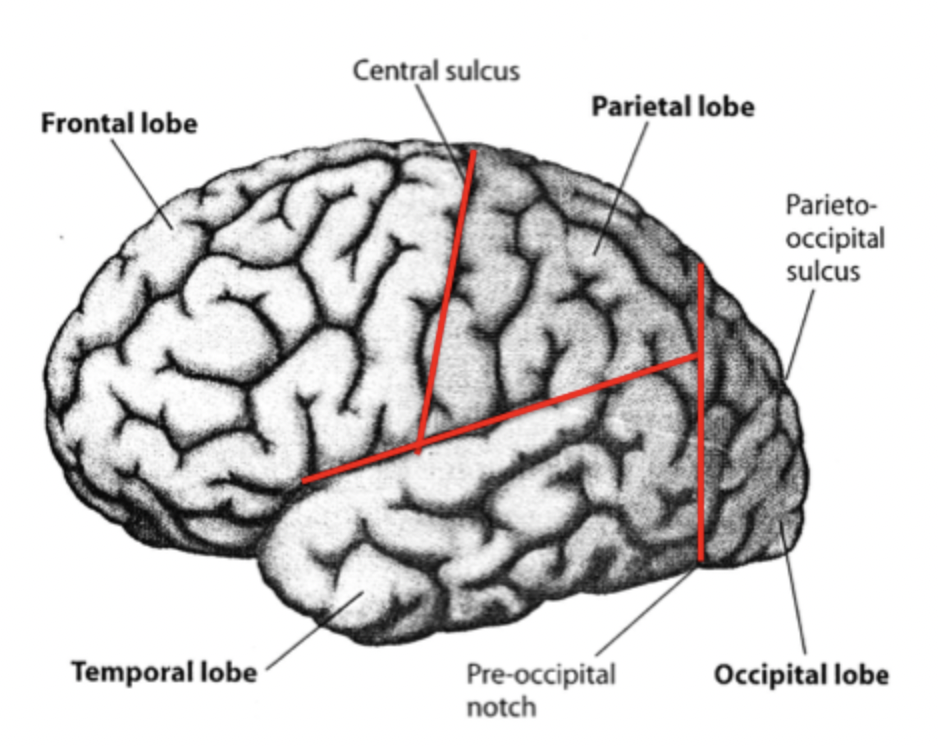
Central sulcus, lateral sulcus, Pareto-occipital sulcus
cortex,sub cortex and lobes of the brain
convolutions, layer below convolutions
Occipital lobe= ONLY visual functions
Temporal= auditory, visual and memory
Parietal= spatial processing, damage to right parietal= ignore left side
Frontal= executive functions, motor, organizing behavior, integrates info, sends motor info to motor cortex
Visual pathways
Eyes→ subcortex. Eyes to lateral geneculate nucleus (LGN). Nasal fibres cross over, temporal don’t.
Subcortex→ cortex. LGN to primary visual cortex (V1) in occipital lobe.
Cortical visual pathways beyond V1
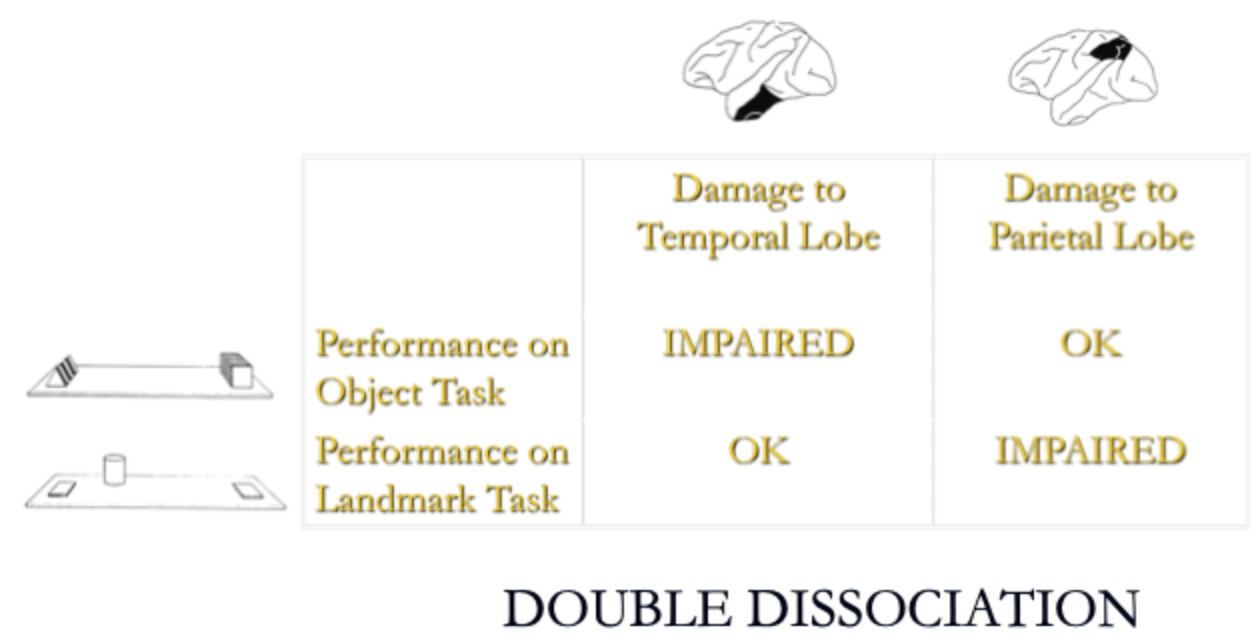
Mishkin & Ungerleider 1982. Monkeys trained on object discrimination task and landmark discrimination test.
Visual discrimination task= one object will have a reward when you pick it up. See if they go back to the one with the reward in the next trials even when position of objects change
Landmark discrimination task= reward is hidden under an object but both objects look the same. The object closest to the cylinder is the one with the reward.
After learning both tasks half got parietal lesions and half temporal lesions
temporal lobe important for object discrimination, parietal lobe for landmark discrimination
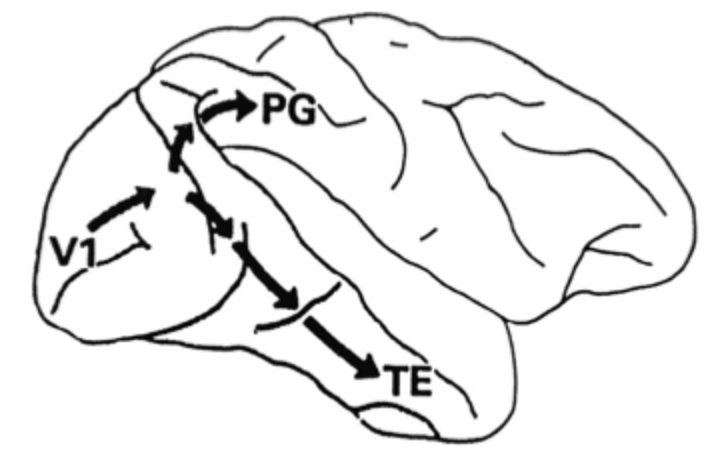
Mishkin & Ungerleider 1982. Beyond V1
Beyond V1 info travels along dorsal and ventral streams
Dorsal= goes into parietal lobe, Important for position (where) of objects, spatial vision
Ventral= goes into temporal lobe, important for (where) of objects, pattern vision
neural properties along visual system
Electrophysiology studies= wires in brain to see AP of neurons
From eyes up to V1= Rods and cones (change in illumination), retinal ganglion cells and LGN cells create spots of light, V1 cells like lines more than spots of light.
Beyond V1 (in ventral visual stream)= Inferior temporal (IT) cortex. Grandmother cells respond to certain shapes (feature detectors)
Retinotopic mapping= Point-to-point mapping of external world onto a brain area. V1 and before. V1 is in the back of occipital lobe. After V1 no retinotopic mapping.
Visual system
As you go higher into visual system (away from eyes) info becomes more complex
features that drive a cell change, from basic illumination levels (rods & cones) to spots of light (RG cells, LGN cells) to lines (V1) to complex features (IT cortex cells).
Where info has to be changes from small specific areas (V1 cells) to large space (IT cells)
Lateral inhibition
They look like different shades even though both squares are 20 units and are the same colour. Cells are inhibiting the neighboring colour.
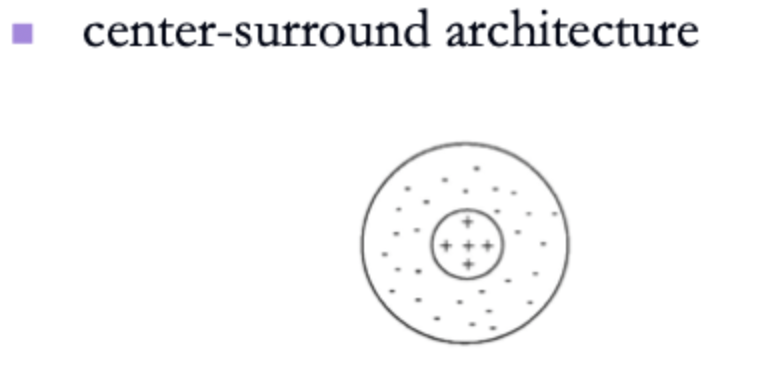
Retinal ganglion cells like dots
Centre surround architecture increases contrast and brightenss contrast
Herman grid illusion
arises from centre surround architecture of RGCs
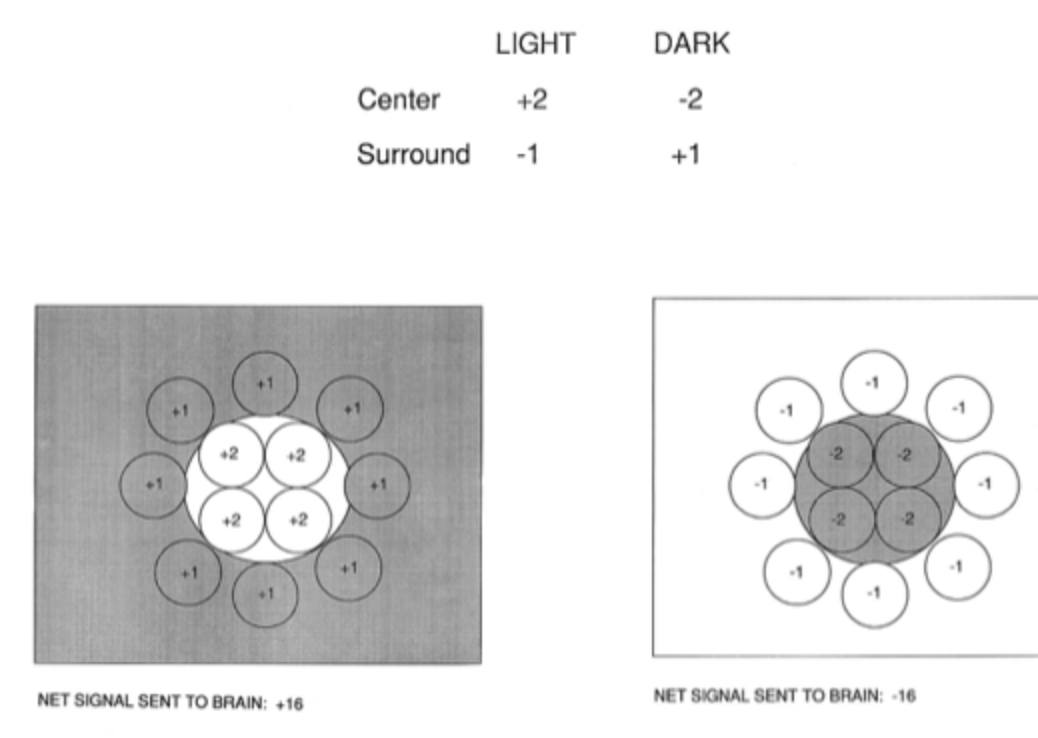
when bathed in diffuse light or darkness the brain sends nothing bc the numbers cancel out
When presented with dark or light dot the RGC sends maximum signal

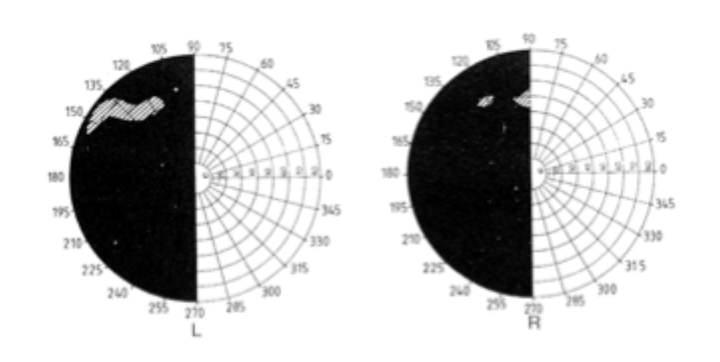
Damage at:
Right optic nerve= right monocular blindness
Optic chiasm= bitemporal hemianopia
Right optic tract= Left homonymous hemianopia
Right V1= Left homonymous hemianopia with macular sparing (dot in middle)
Patient DB, blindsight
removal of tumour in right occipital lobe
Left homonymous hemianopia
Can’t identify static or moving object (bc info bypassing V1) but can localise it in space (info reaching dorsal/where path)
Sensing moving object= info reaching V5
Achromatopsia, Akinetopsia
Absence of colour vision, damage to V4, can result from missing cones, colour blindness
Absence of motion vision, damage to V5, can see that something is moving but can’t see the object
Visual agnosias
Inability to name object even though you can see it well. All have preserved colour and motion perception.
apperceptive= Bilateral damage to V1, peppery mask, failure of object recognition, poor matching & copying.
Dorsal simultagnosia= bilateral damage to parietal lobes, failure of object recognition bc spatial perceptual impairment, can recognise objects but not more than one at a time, can’t see all objects at the same time
ventral simultagnosia= damage to ventral stream beyond V4, failure of object recognition bc complex perceptual impairment, can see multiple objects but not clearly
Associative= Damage to higher order (than V5). copying of images is normal but slavish (struggling). Fail incomplete figures test quicker.
Top-down vs bottom-up theories, interactive theories of pattern perception
context dependent, hypothesis testing, knowledge and experience,
Detail dependent, building on small features until details emerge, sensory info, Evidence= errors & confusion.
theories that accomodate both
binocular cues
Retinal disparity= 2 images at different depths will result in diff image distances on the retina, brain interprets it as depth
Convergence & divergence= near objects make eyes converge, far objects cause eyes to diverge, brain interprets it as depth
Monocular cues
Interposition= Object covering another object is closer than the one that is being covered
Relative size= people smaller in the picture are further away but irl they are the same size
Linear perspective
Heightened plane= not very powerful clue, objects
Texture gradient
Light and shadow
Young Hemlotz trichromatic theory
3 cones in the retina and each are maximally sensitive to a certain colour
cones sensitive to blue, some to green and some to red (short, medium and long wavelengths)
doesn’t account for why colour blindness is in pairs and why we get colour after effects
Opponent process theory
Bipolar RGCs are opponent process cells
Short wavelength= blue/yellow opponent cells
Medium wavelength= red/green opponent cells
Long wavelengths= black/white opponent cells
Renes Descartes early 1600s
brain symmetrical
thought that there was a structure that unites everything and is between the two hemispheres (pineal gland)
WRONG
Gal &Spurzheim early 1800s
Phrenology= Bumps associated with skills, dents associated with under-developed behaviors.
Faculties= odd behaviors mapped onto the brain
Problems= No actual correlations between bumps and depression on the outside of the skull and the brain.
Paul Broca 1861
Only thing Tan could say is "tan"= language impairment. Comprehension is fine but motor impairment.
Tan had big lesion in the left frontal lobe. This is the brocas area.
Language is localised in the left frontal lobe
brocas aphasia= difficulty with language output
Karl Wernicke 1873
Language problem in patient, output is normal but comprehension impaired.
Lesion in left temporal lobe
Fritsch and Hitizig 1870
motor cortex caused contralateral (opposite) movement of body parts
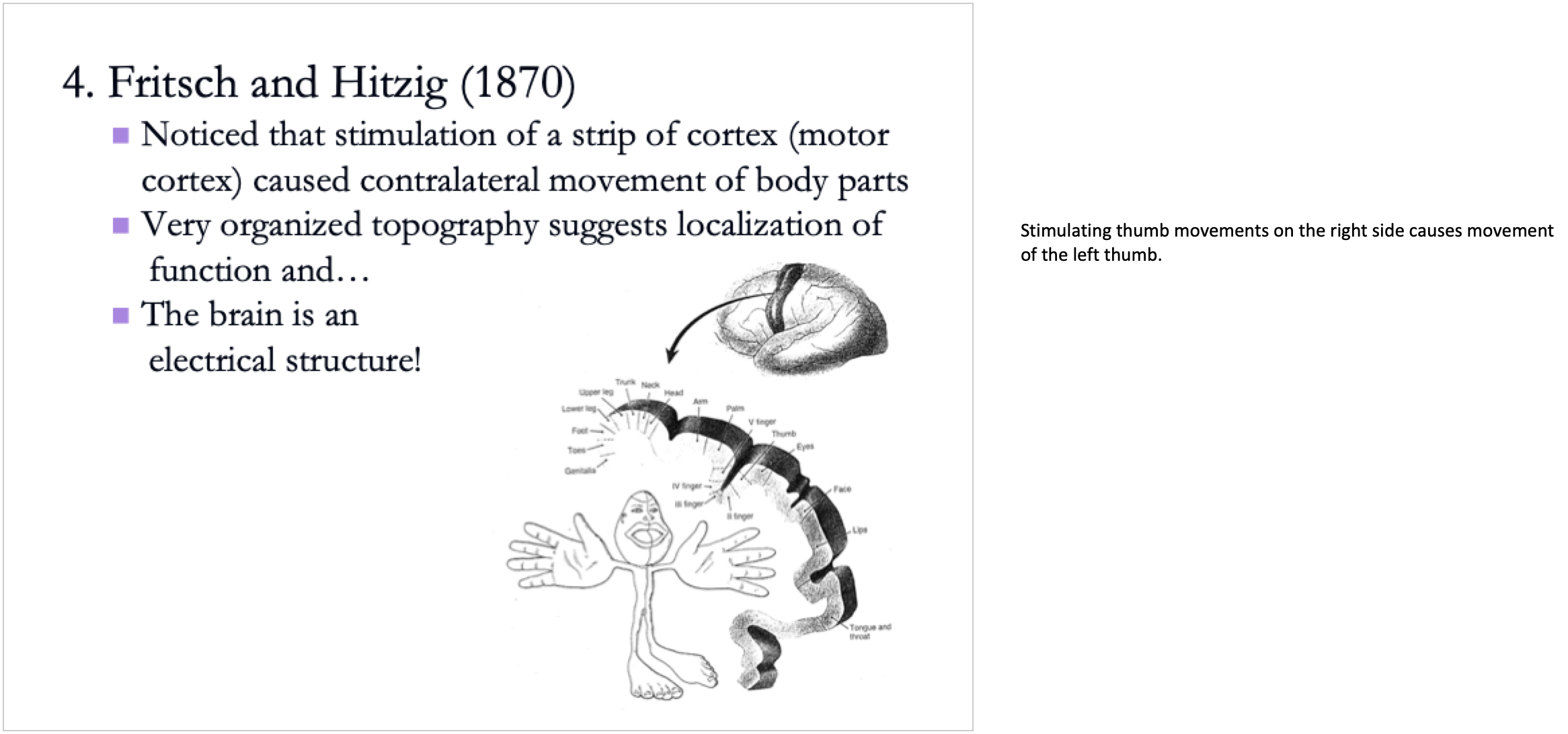
Stimulating thumb movements on the right side causes movement of the left thumb.
Damage to occipital lobe
Blindness & blindness
Apperceptive agnosia
Temporal lobe parts, damage
Lateral surface= superior, middle, inferior temporal gyrus
Medial surface= medial temporal lobe
Superior temporal damage (auditory)
deafness
Wernickes aphasia
Auditory agnosia
Middle & inferior temporal damage
Achromatopsia, Akinetopsia
Ventral simultagnosia
Associative agnosia
medial temporal lobe
Left= Hearing okay, verbal memory impaired
Right= Copying okay, visual memory impaired
Patient HM
Removed medial temporal lobe= old memories still there but new memories not saved as much
retrograde amnesia
Anterograde amnesia
Mirror-drawing task, tower of Hanoi
ppl with medial temporal lobe damage do have some spared memory. Draw outline of star and then trace by using reflection in mirror. First time you are bad at it, memory helps you improve as you do it more times
Multiple memory systems
Declarative= affected by medial temp lobe impairment
Nondeclarative= not affected by MTL impairment, improve over many trials
e.g. riding a bike, mirror drawing task
Person that has MTL impairment won't remember doing it 10mins later but if given the task again they can do it
Left parietal lobe damage
Agraphia= Difficulty in writing, difficulty in organising information on the page
Acalculia= Difficulty in mathematics, because impairment in organizing information, don’t know where to put the numbers
Right/left confusion
Dyslexia
Difficulty drawing (details)
Right parietal lobe damage
difficulty recognising unfamiliar view of object
Difficulty drawing (overall shape)
Contralateral neglect= Only sees one side. Instead of turning to the left she swings whole body around until stuff comes into view.
tests for contralateral neglect
right parietal lobe damage
Line or letter cancellation
Line bisection= Middle part of the right half of the line instead of the middle of the whole line
Neglect is a post-perceptual problem bc both right and left are processed but only one side is seen (burning house and Milan pizza experiments)
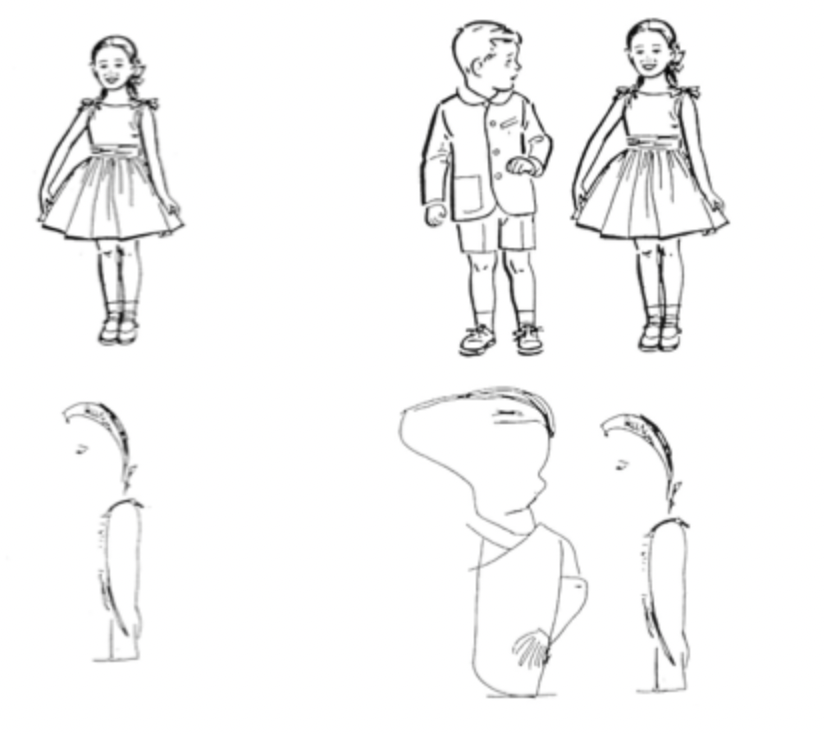
Ego centred vs Object centred neglect
ignore entire left half but not right. Draws the girl but not the boy
doesn’t matter where in the visual field the object is the left half of the object is ignored. Draws the right half of the girl and right half of the boy
What is being neglected? Driver, Baylis, Goodrich & Rafael 1994
Ppl with contralateral neglect= Saw the gap in the left half but not in the right half because of ego
It looks like object based neglect but its actually ego because there is an axis that reinstates ego based neglect
Damage to the right parietal lobe neglect the left, have to be right handed
Damage to the left parietal lobe neglect the right if they are left handed
Frontal lobe
Motor cortex
Premotor cortex (damage= brocas aphasia)
Prefrontal cortex
Orbitofrontal cortex

Loss of divergent thinking
Frontal lobe damage (prefrontal cortex)
Word fluency test= "how many words can you write that start with the letter S". Impairment to prefrontal cortex would cause you to think of less words, can't generate as many words. "how many words can you write starting with C but only 4 letters long". Rule breaking, ignore the instruction.
Design fluency test= Low output or high output with the same figure over and over again

Impairment to frontal lobe
Brocas aphasia
Loss of divergent thinking
Impairments with response inhibition
Stroop interference test= read colour not word
Environmental dependency syndrome (exaggerated imitation of others or using things infront of them)
Change in personality
Wisconsin card sorting test
tests for response inhibition for frontal lobe damage
"pick up a card from the deck and match it with one of the 4 cards"
Will be told whether it is correct or incorrect. Not clear which one to match it to.
By the third trial you should be able to figure out the pattern. When getting 10 right in a row it is now incorrect but should be able to figure out the new rule
Person with impairment in pre frontal cortex will take a lot more trials to figure it out