Electrolyte Disorders
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
What electrolytes are not included on a BMP?
Magnesium and Phosphorus
How much of water makes up total body weight?
60% with 2/3 being intracellular where as 1/3 is extracellular
What is osmolarity?
total solute concentration in a fluid compartment
what solutes determine the calculated osmolality of the ECF?
Sodium, Glucose, and Urea
What substances contribute to an elevated osmolal gap?
Mannitol and Ethanol
What is tonicity?
the ability of solutes to generate an osmotic driving force that causes water movement from one compartment to another
How is tonicity increased?
a solute must be confined to the ECF compartment i.e increased Na+ will increase tonicity causing cells to shrink
What determines the size of extracellular fluid volume (ECFV)?
total amount of Na+ in the ECF and volume status of the patient
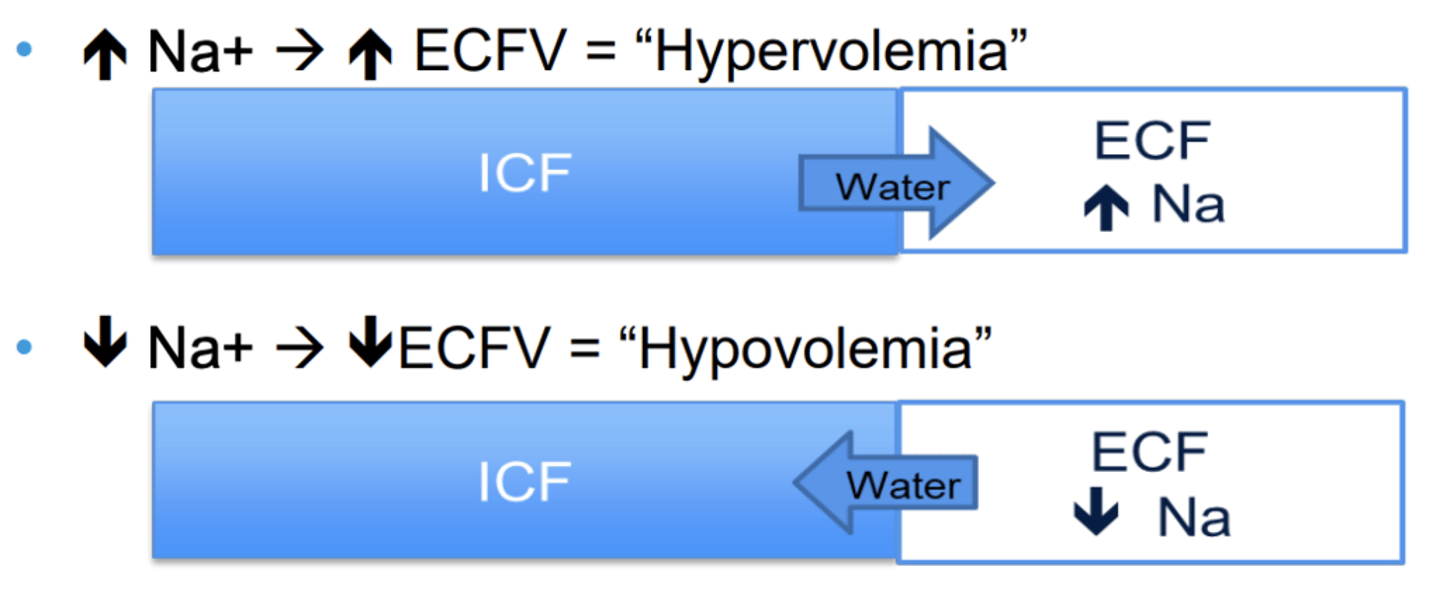
What does an abnormal serum Na+ indicate?
sign of a disorder of water regulation

What are the causes of hypovolemia?
GI losses, Renal losses, Skin losses, Fluid sequestration, Hemorrhage
What are the signs of hypovolemia?
Increased thirst, decreased turgor, dry mucous membranes, oliguria, tachycardia, postural hypotension
What are the causes of hypervolemia?
Liver disease, Heart Failure, and Kidney Failure
What are the signs of hypervolemia?
SOB, Orthopnea, PND, Crackles, JVD, peripheral edema
What influences water retention?
Thirst and ADH (vasopressin or arginine vasopressin)
What influences salt retention?
Renin-Angiotensin system
What are the functions of aldosterone?
1. Increase renal Na+ retention (in effect, ↑ECFV)
2. Increase renal K+ excretion
What is the most common electrolyte abnormality in hospitalized patients?
Hyponatremia
What are the severity levels for hyponatremia?
Mild: 125-135
Mod: 120-125
Severe: <120
Lethal: <120 with seizures
What are the symptoms of hyponatremia?
HA, dizziness, N/V, lethargy, weakness, confusion, seizures, delirium, coma (cerebral edema!)
What are the causes of hyponatremia?
Pseudohyponatremia and Redistributive hyponatremia
What is Pseudohyponatremia?
Serum Na < 135 but NORMAL osmolality (iso-osmolar) seen in hyperlipidemia and hyperproteinemia
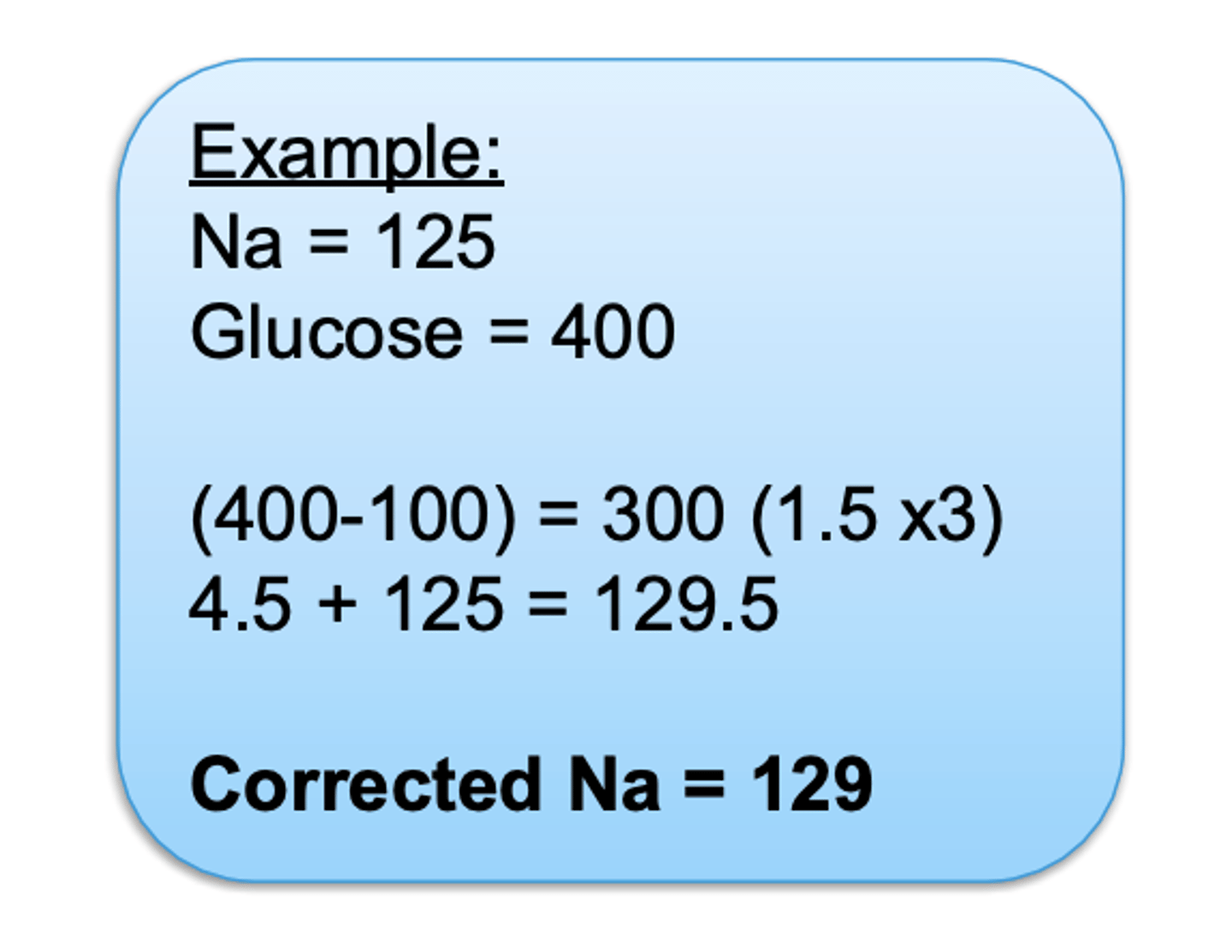
What causes Redistributive hyponatremia?
osmotically active solutes in the ECF, that draw H2O from cell, diluting serum sodium concentration seen in hyperglycemia
What are the causes of Hypovolemic Hyponatremia?
Renal Loss (Na+ >20): Diuretics, renal tubular acidosis, diuresis, Addison's
Extra-renal Loss (Na+ <20): GI loss, cuteanous loss, pancreatitis, obstruction, peritonitis
What is the treatment for Hypovolemic Hyponatremia?
replace fluid losses (with isotonic fluid, ie. NS), and treat the underlying cause
What causes hypervolemic hyponatremia?
Hepatic cirrhosis, CHF, renal failure
What is the treatment for hypervolemic hyponatremia?
diuretics, dialysis, fluid restriction
What causes Euvolemic Hyponatremia?
SIADH, polydipsia, hypothyroidism, adrenal insufficiency, glucocorticoid excess
What are the hallmark findings for SIADH?
Low serum osmolarity with concentrated urine and euvolemia (urine Na+ >40, osmolarity >100)
What is the treatment for Euvolemic Hyponatremia?
fluid restriction (1.5 L/day), treat underlying cause.
What is the rate that hyponatermia should be corrected?
Acute: ≤10 mEq/L in the first 24 hours and ≤18 mEq/L in 48 hours
Chronic: ≤8 mEq/L in the first 24 hours
What can a rapid increase in serum sodium cause?
cerebral pontine myelinolysis (CPM) or osmotic demyelination syndrome (ODS)

What is hypernatremia?
A hypertonic disorder due to serum sodium >145mEq/L leading to brain cell shrinkage secondary to increased ECF osmolarity
What causes hypernatremia?
GI losses, skin loss, diuretics, lithium
What are the symptoms of hypernatremia?
thirst, AMS, neuromuscular irritability, focal neuro deficits, seizures, arginine vasopressin disorder
What is arginine vasopressin disorder (diabetes insipidus)?
either caused by AVP deficiency or resistance
What is the characteristic finding of arginine vasopressin disorder?
Urine is dilute with low osmolarity and sodium (<250) with polyuria (50-60 ml/kg/day)
How to differentiate between AVP-D and AVP-R?
AVP-D: low or undetectable plasma copeptin and increase in osmolarity after desmopressin
AVP-R: minimal or no response to desmopressin administration
What is the treatment for AVP-R?
Ensure adequate free water intake to match urinary losses and add Thiazide diuretic if needed
What is the treatment for generalized hypernatermia?
stop water loss and replace water deficit (orally, NG, IV)
What occurs if water is replaced too rapidly?
seizures, brain damage, and CPM
How is water deficit calculated?
Normal TBW - Current TBW
What is hypokalemia?
< 3.5 mEq/L
What causes hypokalemia?
diuretics (MC), insulin, caffeine, GI losses, burns, magnesium deficiency
What is the clinical presentation of hypokalemia?
weakness, fatigue, cramps, arrhythmia, hyporeflexia, flaccid paralysis, hypercapnia
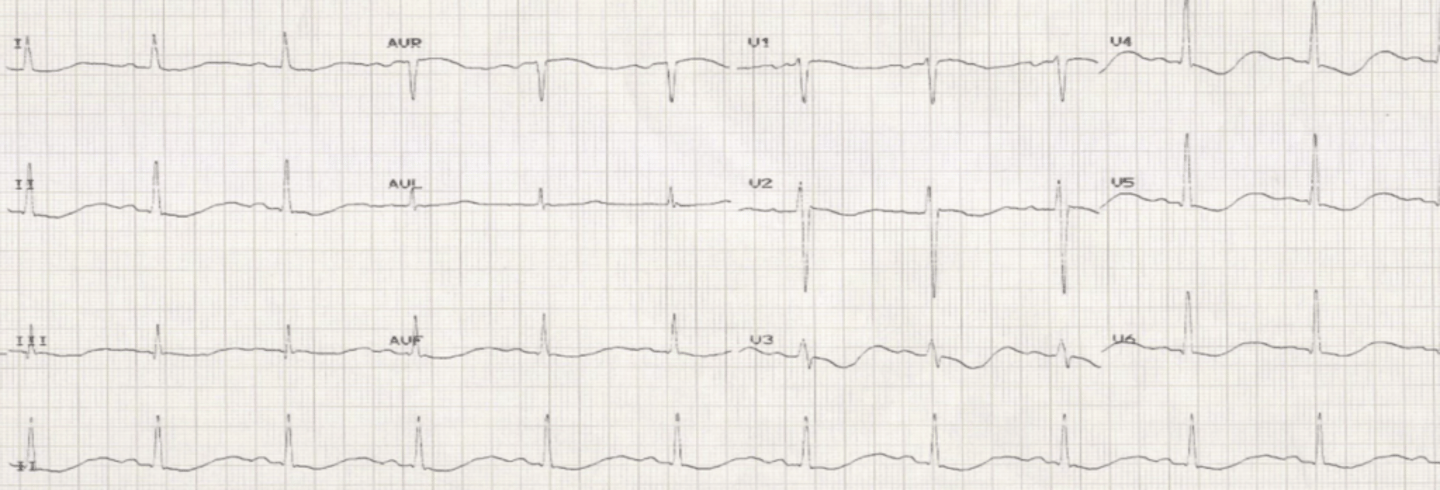
What ECG findings are consistent with hypokalemia?
Flattened T waves, prominent U waves, PVCs, depressed ST segments
What is the treatment for hypokalemia?
Potassium replacement orally or IV if needed (Must be given slowly) +/- Magnesium replacement and Digoxin
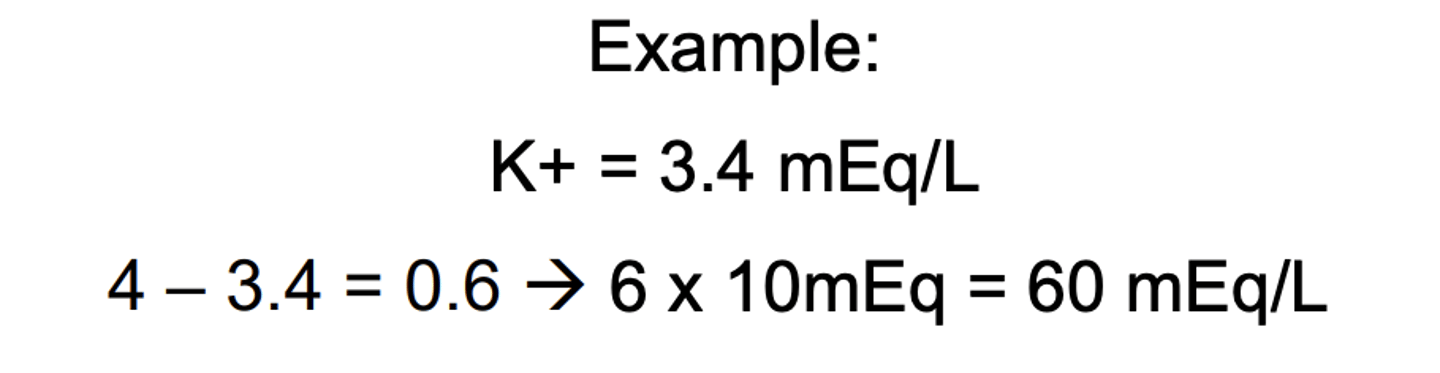
What is the replacement rate for hypokalemia?
For every 0.1 mEq/L below 4mEq/L, Give 10 mEq/L
What is hyperkalemia?
K > 5 mEq/L and severe > 6.5 mEq/L
What are the symptoms of hyperkalemia?
asymptomatic, muscle weakness
What ECG findings are seen with hyperkalemia?
Peaked T waves, widened QRS, junctional rhythm, V-fib
What are causes of hyperkalemia?
Hemolysis, Renal Failure (#1), Metabolic Acidosis, Spironolactone, ACE/ARB, NSAIDs, increased dietary/medication intake
What is the emergent management of Hyperkalemia?
1) IV Calcium
2) Sodium bicarbonate, Insulin IV + D50W, Nebulized albuterol
3) IV Lasix, PO potassium binders, emergent dialysis
What is the less emergent management of Hyperkalemia?
Potassium binders (Lokelma), Diuretics, and correct underlying cause
How is total calcium measured?
free (ionized) + protein-bound
What is ionized calcium?
Physiological active form, unaffected by serum albumin level
What is complexed calcium?
calcium bound to small anions (citrate, lactate, etc.) to prevent clotting
What is protein-bound calcium?
bound to albumin
What is hypercalcemia?
Calcium >10.1
What is the symptoms of hypercalcemia?
Stones, Bones, Abdominal Moans, and Psychiatric Groans
What are the causes of hypercalcemia?
Malignancy (>13), primary hyperparathyroidism, thiazides, lithium, antacids, vitamin A anaogs (accutane)
What is the equation for corrected calicum?
measured total calcium + [0.8x (4-albumin)]
What is the treatment for hypercalcemia?
IV fluids, calcitonin, bisphosphonates, dialysis
What causes hypocalcemia?
hypoparathyroidism, vitamin D deficiency, renal disease, bisphosphonates, cinacalcet
What are the symptoms of hypocalcemia?
hyperreflexia, spontaneous twitching, muscle cramps, tingling, numbness
Chvostek's and Trousseau's Sign
How is hypocalcemia managed?
IV calcium gluconate
What causes hypophosphatemia?
inadequate intake (supply or absorption), urinary losses, vitamin D deficiency, malabsorption, refeeding syndrome
What is the clinical presentation of hypophosphatemia?
metabolic encephalopathy and hypoventilation
What causes hyperphosphatemia?
CKD or phosphate-containing laxatives
What is the treatment for hyperphosphatemia?
oral phosphate binders and calicum carbonate
What is hypermagnesemia?
> 2.2
What are some signs of hypermagnesemia?
weakness, hypotension, N/V
What ECG changes are seen with hypermagnesemia?
widened QRS, prolonged PR interval, prolonged QT interval
What is the treatment of hypermagnesemia?
IV calcium gluconate, IV fluids, IV lasix, dialysis
What is hypomagnesemia?
Mg < 1.8
What causes hypomagnesemia?
chronic alcoholism, chronic diarrhea, diuretics, nutritional deficiency, long term PPI use
What are the symptoms of hypomagnesemia?
lethargy, anorexia, N/V, weakness, tetany, seizures, arrhythmias
What is the treatment for hypomagnesemia?
IV or IM magnesium sulfate