B6: Endo Exam 1 (1-7)
1/220
Earn XP
Description and Tags
Thyroid disorders: because your neck decided it should control your energy, mood, weight, and sanity—with zero training.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
221 Terms
pituitary gland
What is a small pea-like structure located in the sella turcica below the hypothalamus and is a part of the hypothalamic-pituitary-adrenal axi?
hypothalamic-pituitary-adrenal (HPA) axis
What is a major neuroendocrine system that regulates many body process through direct signaling and feedback interactions between organs, glands, and hormones?
pituitary gland
What receives messages from the hypothalamus and is able to relay these messages via hormones to other parts of the body?
TRH
What hormone:
-targets thyrotoph cells
-stimulates the release of TSH which acts on the thyroid gland to release T3 and T4
GHRH
What hormone:
-targets somatotroph cells
-stimulates the release of GH which acts on the liver to release IGF-1
GnRH
What hormone:
-targets gonadotroph cells
-stimulates the release of LH or FSH which acts on the ovary to release progesterone and testosterone as well as the testis to release testosterone and inhibin
CRH
What hormone:
-targets corticotroph cells
-stimulates the ACTH which acts on the adrenal gland to release cortisol
pituitary tumor
What is the most common reason or cause for disorders of the pituitary?
true
T/F: most pituitary tumors are not cancerous, the tumor grows on or near the pituitary gland and disorders occur
mass effect
Changes in function of structures next to or near the pituitary causes _____ ___ with Sx
pituitary tumors
What disorder:
-benign
-"incidentalomas" -- often found accidentally
-if pts already have a diagnosed cancer, metastasis should be considered
-tumors <10 mm = microadenomas
-tumors >10mm = macroadenomas
-most common type = PRL secreting
-most common Sx = HA, visual field defects, CN palsies
-Superior extension of a tumor compresses the optic chiasm --> bitemporal hemianopsia
-lateral extension into cavernous inuses results in ophthalmoplegia, diplopia, or ptosis due to compression of CN III, IV, VII due to compression of V1/V2
microadenoma
What disorder:
-benign
-<1 cm in diameter
Eval + Tx:
-initial labs to rule out pituitary hypersecretion or hypopituitarism
-if pt does not have mass effect or pituitary hypersecretion then surgery is not warranted and can observe
-reassess with imaging in one year
-then reassess every 1-2 yrs for at least 3 yrs before reducing follow up
macroadenoma
What disorder:
-benign
->1 cm in diameter
Eval + Tx:
-initial labs to rule out pituitary hypersecretion or hypopituitarism
-if pt does not have mass effect or pituitary hypersecretion then surgery is not warranted and can observe
-repeat pituitary hormone assessment + imaging in 6 mos then yearly up to 3 yrs then reduce follow up frequency
surgery via endoscopic transsphenoidal approach
What is the 1st line of therapy for pituitary tumors that require treatment (e.g., cause mass effect or hyper/hypo secretion)?
medical therapy
What is the 1st line of therapy for pituitary tumors that require treatment (e.g., cause mass effect or hyper/hypo secretion) and are PROLACTINOMA?
surgery
Indications for _________ (1st line treatment) for pituitary tumors include decompression of mass effect, preventing of further tumor expansion, and normalization of hormone levels
hypopituitarism
What disorder:
-condition in which there is a deficiency of one or more pituitary hormones
-it can be congenital (e.g., Kallmann syndrome) in origin or acquired (tumors, irradiation, surgery, external blunt trauma, empty sella syndrome, pituitary apoplexy, sheehan syndrome)
-acquire defects such as a tumor, specifically a macroadenoams in the sella, is the most common cause of hypopituitarism
-Dx in pts w/ secreting or non-secreting pituitary masses involves a combo of static and stimulatory blood tests
meningioma
What disorder:
-difficult to distinguish from non-functioning pituitary adenomas
-typically enhance on MRI
-classic "bird beak" sign if occurs on base of skull over sella
meningioma
ID
craniopharyngioma
What disorder:
-childhood tumor in the brain that is derived from the remnants of Rathke pouch
-most common cause of pituitary hypofunction in children
-benign tumor on histology but it can have malignant type behavior with invasion in local structures
-it can cause HA and visual field deficits (bitemporal hemianopsia)
-surgery usually required rendering pt to have pan-hypopituitarism for life
sheehan syndrome
What disorder:
-severe post-partum hemorrhage causing ischemic infarct of the pituitary
-due to the pituitary being enlarged because of pregnancy, the pituitary is hypoperfused and can infarct
-the mother may present with failure to lactate, absent menstruation
pituitary apoplexy
What disorder:
-hemorrhage of the pituitary gland likely from a pituitary adenoma that can cause severe HA, visual impairment, and features of hypopituitarism
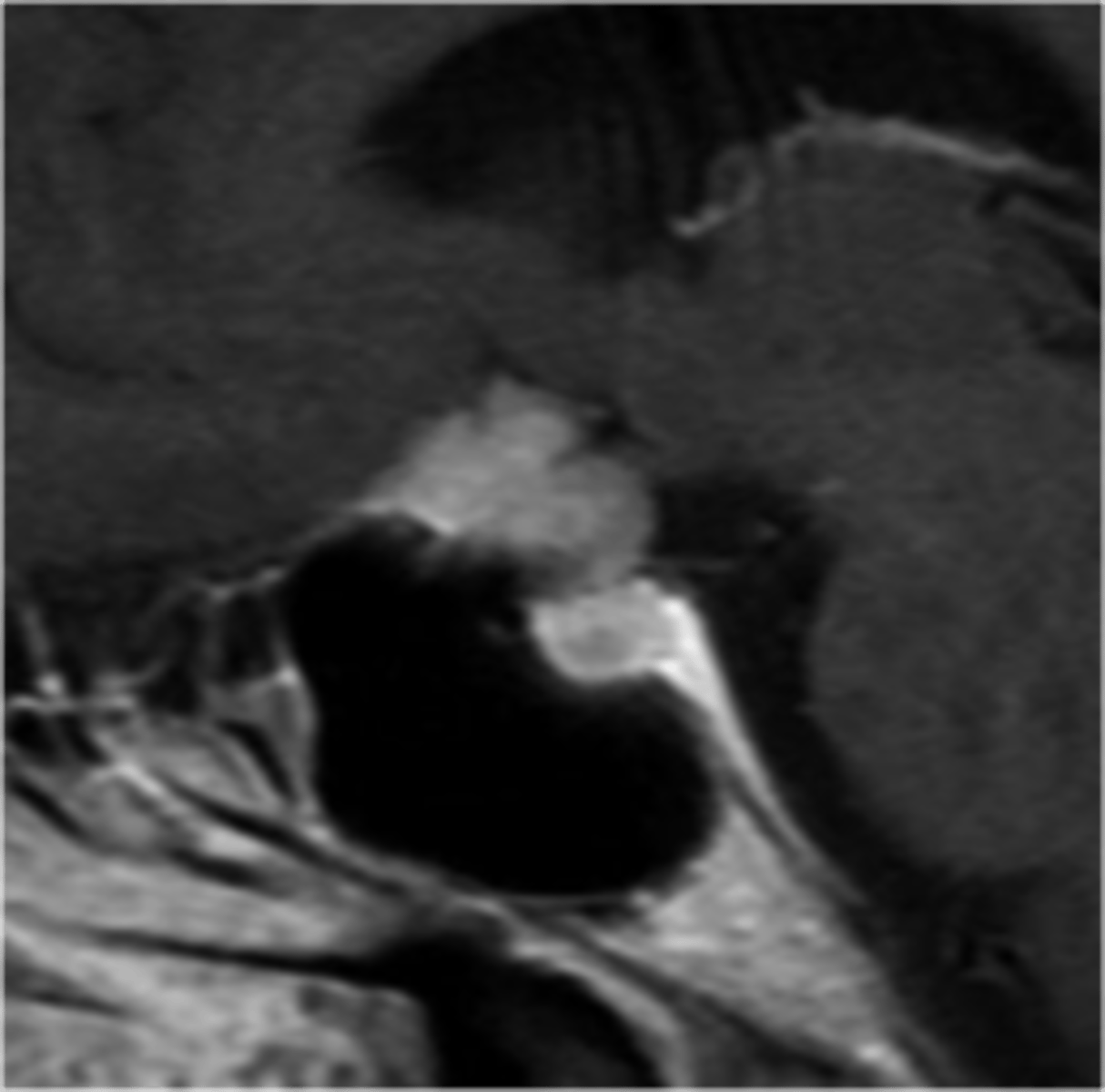
empty sella syndrome
What disorder:
-radiologic finding on MRI consisting of an enlarged sella turcica not entirely filled by pituitary tissue
-pituitary may be small, compressed, lining the enlarged sella, or maybe it just cannot be visualized
-incidental
-primary is caused by herniation of subarachnoid space and fluid into sella, compressing the normal pituitary gland due to sellar diaphragm incompetence, increased ICP, or volumetric changes in pituitary gland
-secondary can be related to pituitary tumor infarct (most commonly macroadenomas)
primary
(primary/secondary) empty sella syndrome:
- caused by herniation of subarachnoid space and fluid into sella, compressing the normal pituitary gland due to sellar diaphragm incompetence, increased ICP, or volumetric changes in pituitary gland
secondary
(primary/secondary) empty sella syndrome:
-related to pituitary tumor infarct (most commonly macroadenomas)
Kallman's syndrome
What disorder:
-aka congenital hypogonadotrophic hypogonadism
-most common cause of pre-pubertal GnRH deficiency
-mutation of KAL1 gene- usually X linked
-GnRH deficiency is the main problem --> undetectable LH and FSH
-classic form of hypogonadotropic hypogonadism
-associated with anosmia (KAL1 encodes anosmin). GnRH neurons originate outside the CNS in the epithelium of the medial part of olfactory placode (associated w/ congenital agenesis of olfactory bulbs)
-typically affects males but can occur in females
-Tx = treat hypogonadism with hormone replacement
ACTH excess
The initial tests to test for _________ include:
-24 hr urine free cortisol (x2)
OR
-nocturnal salivary cortisol (x2)
OR
-overnight low-dose dexamethasone test
ADH excess
The initial tests to test for _________ include:
-simultaneous serum sodium
-serum osmolality
-urine sodium
-urine osmolarity
GH excess
The initial tests to test for _________ include:
-IGF-1
TSH excess
The initial tests to test for _________ include:
-TSH
-free (or total) thyroxine
PRL excess
The initial tests to test for _________ include:
-PRL
ACTH deficiency
The initial tests to test for _________ include:
-simultaneous 8am ACTH
-cortisol
ADH deficiency
The initial tests to test for _________ include:
-simultaneous serum sodium
-urine and serum osmolarity
LH and FSH deficiency
The initial tests to test for _________ include:
-simultaneous LH, FSH
-8am total testosterone (male) OR
-8am estradiol (female)
TSH deficiency
The initial tests to test for _________ include:
-simultaneous TSH
-free (or total) thyroxine
GH deficiency
The initial tests to test for _________ include:
-IGF-1
ACTH deficiency
The confirmatory tests to test for _________ include:
-ACTH stimulation test
ADH deficiency
The confirmatory tests to test for _________ include:
-water deprivation test
GH deficiency
The confirmatory tests to test for _________ include:
-GHRH-arginine
-insulin tolerance
-glucagon stimulation
-ghrelin agonist stimulation
FSH and LH
What are gonadotropins which work in regulating sexual differentiation, the production of sex steroids, and gametogenesis?
hint: production is responsible for puberty and fertility
males
in (males/females):
-FSH receptor are located in sertoli cells and seminiferous tubules where they stimulate sperm maturation
-LH receptors on Leydig cells in the testis stimulate the production of androgen
-Together, LH and FSH induce spermatogenesis
females
in (males/females):
-ovarian FSH receptors on granulosa cells induce the biosynthesis of estrogen
-LH receptors on ovarian thecal cells stimulate the synthesis of ovarian androgens and steroid precursors that granulosa cells aromatize into estrogens
-together the secretion of FSH and LH regulate the menstrual cycle
LH and FSH deficiency
What disorder:
-acquired forms can be tumor that interferes with normal production such as Rathke pouch cysts, craniopharyngiomas, infections, trauma, infiltrative diseases (hemochromatosis, sarcoidosis)
-congenital causes can be due to Kallman syndrome as discussed previously
-functional gonadotropin deficiency can be seen in chronic illness, starvation, Cushing syndrome, anorexia nervosa
-another presentation can be female college athletes
-classic presentation are patients in their second or third decade of life with poorly or absent sexual characteristics, inability to enter puberty, and amenorrhea or infertility
-diagnosis would include low testosterone in men or low estradiol in women in the presence of low or normal levels of FSH and LH
-occasionally a provocative test with leuprolide could be done to distinguish cause of decreased hormone secretion
Tx:
-Females --> FSH and LH (hCG) analogues to induce ovulation w/ conjugated estrogens and medroxyprogesterone acetate or low-dose contraceptive pills. Estrogen-containing transdermal patches are also available
-Males --> testosterone supplementation, hCG alone or with FSH can be used to induce spermatogenesis in men
LH and FSH excess (tumors)
What disorder:
-most gonadotrophinomas are clinically silent except when their size results in neurologic findings such as visual field problems or HA
-majority of gonadotropinomas secrete small amounts of LH or FSH which would have no clinical manifestations
-no clinical syndrome is uniquely associated w/ these tumors
Tx:
-b/c major symptoms of gonadotropin producing tumors or non-functioning adenomas are related to local mass effects and extrasellar extension, the goal is to reduce size of tumor
-transphenoidal surgery usually can completely or partially reverse any hypopituitarism and visual field impairment
ACTH
What hormone:
-39 AA peptide hormone that is formed from a precursor molecule, pro-opiomelanocortin (POMC) and is synthesized and secreted by corticotrophs in the anterior pituitary
-it is stimulated by hypothalamic CRH
-stimulates release of glucocorticoids (cortisol) from adrenal cortex
-if there is abnormalities with the pituitary, then these can be increase or decrease in cortisol produced
primary adrenal insufficiency
What disorder:
-Affected Glands: adrenal glands
-Affected Hormone Levels: cortisol low, ACTH high
-Affected blood levels: Na+ low, K+ high
-Replacement required: cortisol, aldosterone
-S/Sx = will have hyperpigmentation of the skin or hyperkalemia
-Dx = 1st test = AM serum cortisol + ACTH, confirmatory test is cosyntropin stimulation test (synthetic ACTH) if morning cortisol is in indeterminant range. IF the coritsol DOES NOT change, the lesion is adrenal gland in origin
secondary adrenal insufficiency
What disorder:
-Affected Glands: pituitary glands
-Affected Hormone Levels: cortisol low, ACTH low, other hormone deficiencies (hypothyroidism)
-Affected blood levels: Na+ and K+ relatively normal
-Replacement required: cortisol
-most common cause = exogenous glucocorticoid treatment suppresses hypothalamic-pituitary adrenal axis. The sudden discontinuation of exogenous glucocorticoids or an unmet increased need for them because of intervening severe stress can cause symptoms and signs of glucocorticoid deficiency
-S/Sx = weight loss, fatigue, muscle weakness, orthostatic symptoms, nausea, vomiting, diarrhea, abdominal pain. The pt will NOT!!!! have hyperpigmentation of skin or hyperkalemia
-Dx = 1st test = AM serum cortisol + ACTH, confirmatory test is cosyntropin stimulation test (synthetic ACTH) if morning cortisol is in indeterminant range. IF the coritsol rises after cosyntropin, lesion is pituitary in origin.
-Tx = hydrocortisone glucocorticoid replacement
tertiary adrenal insufficiency
What disorder:
-Affected Glands: hypothalamus
-Affected Hormone Levels: cortisol low, ACTH low, other hormone deficiencies (hypothyroidism)
-Affected blood levels: Na+ and K+ relatively normal
-Replacement required: cortisol
Cushing's disease
What disorder:
-ACTH producing pituitary tumor
-S/Sx = weight gain, sleep disturbances, emotional lability, oligomenorrhea and amenorrhea and hirsutism and worsening acne in women, proximal m. weakness
-PE = central obesity, large violaceous striae on abdomen, under breasts, in axilla, and in upper inner thighs, abnormal adipose tissue between the scapula ("buffalo hump") or in supraclavicular space, moon facies, increased hematocrit contributes to facial plethora (ruddy cheeks), hair growth increased, multiple ecchymoses on trunk and extremities
-Dx = 1st test is to order 24 hr urine cortisol or a late night salivary cortisol OR a low dose dexamethasone suppression test. 2nd test is an ACTH level, if elevated then disorder central but if normal you know it's within the adrenal glands and ID w/ CT or MRI of abdomen and surgically resect. 3rd test to order is high dose dexamethasone suppression test. If the test suppresses cortisol --> pituitary lesion. If fails to suppress cortisol --> ectopic lesion and require scan to find the lesion
-Tx = remove cause of tumor secreting ACTH by transsphenoidal surgery. If remission not achieved following surgery, irradiation with or without medical therapy
nelson syndrome
What is a disorder in which there is enlargement of pre-existing ACTH secreting pituitary adenoma after BL adrenalectomy for refractory cushing disease?
TSH
What hormone:
-controls thyroid function and growth
-regulation of secretions is regulated by hypothalamic TRH and by negative feedback of itself
-dysfunction (hyper/hypo) is mostly due to PRIMARY dysfunction
secondary hypothyroidism
What disorder:
-Low Free T3/T4 and TSH
-isolated TSH defect relatively rare and usually related to genetic factor
-cause can be from pituitary masses impinging on thyrotrophs or euthyroid sick syndrome, non-thyroid illness, medications
-Sx = cold intolerance, weight gain, dec. appetite, hypoactivity, lethargy, fatigue, weakness, constipation, dec. reflexes, bradycardia, dry, cool skin and coarse, brittle hair, diastolic HTN, myxedema (facial/periorbital), myxedema coma
-Tx = replacement of dose T4 (levothyroxine)
secondary hyperthyroidism
What disorder:
-elevated free T4/T3 and elevated TSH
-pituitary adenoma that secretes TSH
-in addition to classic findings of hyperthyroidism (heat intolerance, weight loss, inc. appetite, hyperactivity, diarrhea, inc. reflexes, tachycardia, palpitations, arrhythmias, warm moist skin, fine hair, systolic HTN, osteoporosis and hypercalcemia, apathetic thyrotoxicosis) pts have a diffuse goiter, visual field defects, HA, and menstrual irregularities in women
-Tx = transsphenoidal resection OR somatostatin analogues before surgery
PRL
What hormone:
-stimulates breast epithelium to produce milk
-secretion inhibits GnRH which delays post-partum ovulation (natural contraception) in females and spermatogenesis in males
-secretion inhibited by dopamine
-a serum level ordered to assess for function
PRL deficiency
What disorder:
-normal concentration is 15-20 pg/mL
-may prevent adequate lactation in nursing mothers and may be a reliable marker for hypopituitarism when seen with another pituitary hormone deficiency
-can be seen in hyperthyroidism b/c TRH suppressed
-lactation not completely absent because nipple stimulation may be sufficient start milk production
hyperprolactinemia
What disorder:
-Besides a secreting adenoma, dopamine antagonists such as antipsychotics, and stimulation of nipple or baby crying can cause release
-The typical presentation will be a premenopausal female with galactorrhea and oligomenorrhea. She may also have headaches or vision changes.
-can also suppress GnRH therefore LH and FSH. As a result, Sx of hyperprolactinemia may also be manifestations of low estrogen levels such as infertility, decreased libido, and vaginal dryness.
-Males can present with decreased libido and headaches, do not get galactorrhea as there is no lobular units of breast
-Osteopenia may be a direct effect of an elevated prolactin level on the bone as its indirect effects on estrogen.
-If there is a secreting tumor, usually medications in the form of dopamine agonists can successfully treat and decrease tumor size even if the tumor is causing mass effect
-Always want to find first if there is a reversible cause of prolactin secretion: nipple stimulation, baby crying, medication such as antipsychotics. If not, get MRI.
-1st Line of treatment of choice are Dopamine agonists (Cabergoline and Bromocriptine). Cabergoline is more popular because of fewer side effects
GH
What hormone:
-aka somatotropin
-main regulator of growth of bone, increased muscle mass, and a variety of other tissues in the body
-can act directly on its own receptors, or it is mediated by a serum factor/hormone secreted by the liver which is called somatomedin/IGF-1
-stimulates glycogenolysis and gluconeogenessis so if there is excess or deficiency the pt will ahve abnormal glucose levels
-excess can cause acromegaly in adults or gigantism in children
GH deficiency
What disorder:
-due to hypothalamic defects or from congenital disorders of the pituitary gland (craniopharyngioma, germinoma, ependymoma, meningioma, medulloblastoma, glioma, Rathke cleft cyst, arachnoid cyst)
-usual manifestation = child slow growth w/ short stature (>2 SD below norm)
-Due to effects of other hormones on growth, children are not born small for gestational age but growth hormone deficiency can manifest as hypoglycemia
-other S/SX = inc. body fat, hypogonadism, small genitalia
-children usually diagnosed when they are found to be shorter than their peers at well baby visits, first entering school, or at puberty
-if occurs in adults --> muscle wasting and hypoglycemia
-Dx = IGF-1, IGFBP-3, and GH helpful to confirm. Insulin tolerance test can be done where regular insulin is given IV and then blood drawn to measure glucose and GH levels.
-Tx = replace w/ recombinant GH
GH excess
What disorder:
-can be due to pituitary adenomas w/ proliferation of pituitary somatotrophs that produce excessive and uncontrolled amounts of GH OR by ectopic production of growth hormone by islet cell tumors or lymphomas or by ectopic production of growth hormone releasing hormone in bronchial carcinoid tumors, small cell lung cancers, medullary thyroid cancers, or pheochromocytomas
-can also be commonly in weightlifters or athletes to improve athletic performance
-S/Sx = coarse facial features that are not noticed immediately but only in retrospect after looking at photographs, HA, bitemporal hemianopsia, include tall stature, macroglossia, frontal bossing, gapping of teeth, change of hat size, large hands, large feet, impaired glucose tolerance, diastolic heart failure, HTN
-In Acromegaly patients should not get taller as growth plates are already fused, but bones can get wider and organs and tissue can get bigger
GH excess
What disorder:
-use GH and serum IGF-1 to make diagnosis. GH is secreted in a pulsatile manner and at high amplitudes, random measurements are NOT very useful for diagnosing or excluding acromegaly.
-A better integrated index of GH production and a more useful way to screen for acromegaly is to measure IGF-1 levels
-after diagnosis made, brain MRI should be obtained to determine the extent of tumor growth
-Tx = Transsphenoidal surgery, medical therapy can include somatostatin analogues such as octreotide or dopamine agonists such as cabergoline, or growth hormone antagonists
-Mortality: increased 2-3 fold likely due to cardiovascular and cerebrovascular complications. Most patients develop myocardial hypertrophy which can be associated with ischemic heart disease and heart failure
ADH and oxytocin
the posterior pituitary will involve the hormones ___________ which are synthesized in specialized neurons in the hypothalamus, housed in the paraventricular and supraoptic nuclei.
-These pro hormones (provasopressin and pro-oxytocin) are packaged in the hypothalamus and transported via the long axons that form the supraopticohypophysial tract
-The pro hormones are converted into Vasopressin and oxytocin while being transported and are stored in the posterior pituitary
-When a stimulus arrives, physiologic release of vasopressin or oxytocin from the posterior pituitary, allows the hormones to go into the general circulation
oxytocin
What hormone:
-in charge of milk secretion or milk let down
-suckling stimulates tactile receptors in the nipple producing an afferent signal to the hypothalamus that causes a synchronized release of oxytocin from posterior pituitary
-upregulation of uterine receptors increase uterine smooth muscle contractions in response to release at end of pregnancy
-no pathologic syndromes of excess or deficiency of secretion have been identified
-has similar structure to ADH, high levels can activate ADH Rs
ADH
What hormone:
-primary physiologic action = water retain
-synthesized in paraventricular and supraoptic nuclei
-central sensing system for controlling the release of ADH is located in a small area of the hypothalamus just anterior to third ventricle
-osmoreceptors control release of ADH to allow H2O retention and stimulate thirst to cause water repletion
-works on V2 receptors in CD principal cells to cause water retention (anti-diuresis)
-stimulus for secretion is increased plasma osmolarity
-can be released due to low BP or intravascular volume depletion but it is more sensitive to changes in osmolality and it is the osmoreceptors that determine main function
-in diseases, osmolytes (e.g., Na+) will be low or high and concentrations of osmolarity of plasma and urine will be used to determine disease
-deficiency/abnormality = central and nephrogenic diabetes insipidus
-excess = SIADH
diabetes insipidus
What disorder:
-excretion of large volumes of hypotonic urine associated w/ insipid (tasteless) urine with polyuria (increased urination) and polydipsia (increased thirst)
-large urine volume, usually in excess of 50 to 60mL/kg/day must be distinguished from an increased frequency of small urine volumes and from large volumes of isotonic or hypertonic urine, both of which have different clinical significance
-Characterized by the production of large amounts of dilute urine, urine specific gravity < 1.006, urine osmolality < 300 mOsm/kg
-The test used to diagnose is the Water Deprivation test; you then differentiate Central from Nephrogenic by giving Desmopressin.
-central can be transient if damage is below the hypothalamic median eminence or in posterior pituitary
central diabetes insipidus
What disorder:
-due to inability of the hypothalamus-posterior pituitary to secrete/synthesize vasopressin in response to increased osmolality
-no concentration of the dilute glomerular filtrate taking place in the renal collecting duct, and consequently a large volume of hypotonic (dilute) urine is excreted
-Levels of vasopressin in plasma are unmeasurable or inappropriately low for the plasma osmolality. Most cases are acquired, idiopathic, or genetic
-Serum osmolality will be high, urine osmolality will be low
nephrogenic diabetes insipidus
What disorder:
-caused by inability of an otherwise normal kidney to respond to vasopressin
-Etiology of the disease can be genetic from familial nephrogenic diabetes insipidus or acquired. Common reasons are chronic use of Lithium (used to treat bipolar disorders), demeclocycline ( used to treat SIADH ), fluoride ( previously used in fluorocarbon anesthetics), and from electrolyte abnormalities such as hypokalemia and hypercalcemia
-Serum osmolality will be high, urine osmolality will be low
SIADH
What disorder:
-due to excess amount of ADH secretion
-Causes include secretion from a pituitary tumor, ectopic ADH by malignant neoplasms (particularly small cell carcinoma of the lung), drugs that increase ADH secretion like SSRIs, carbamazepine, cyclophosphamide), Head trauma, CNS disorders
-Patients can present with nausea, fatigue, or possibly even coma or seizure
-Characterized by excess free water retention, euvolemic hyponatremia, with increased urine osmolality>serum osmolarity
-diagnosis of EXCLUSION when pt has hyponatremia
-Urinary sodium > 40 mEq per L b/c aldosterone is suppressed and atrial natriuretic peptide has increased secretion
-order serum + urine sodium and osmolarity
Tx: remove offending agents if found and address any other medical issues if found. 1st line = water restriction. 2nd line = salt tablets, IV hypertonic saline. IF this doesn't work --> demeclocycline, samsca
-As always, increase sodium concentration slowly as rapid correction of chronic hyponatremia cause cause Central pontine myelinolysis
thyroid gland
What is a bi-lobed structure found anterior to the trachea at the level of C5-C7 and receives very rich blood supply from the thyroid arteries?
thyroglobulin
What is stored in the colloid of thyroid gland?
T3 and T4
thyroglobulin is released as __________ but is first stored EXTRACELLULARLY in the follicular lumen as colloid
thyroid gland
If the ________ is obstructing the carotid aa. or jugular vv., it can cause a bruit
T3
What thyroid hormone has about 10X greater biological activity (receptor affinity) and is the more active form in tissues?
iodine
_________ is required for thyroid hormone synthesis and, therefore, its deficiency is the most common cause of goiter, hypothyroidism, and mental deficiency worldwide
Wolff-Chaikoff effect
If you have normal iodine stores, the __________ will shut down thyroid production when large doses of iodine are present
Jod-Basedow effect
If you have low iodine stores, the __________ will stimulate thyroid production when large doses of iodine are present
TRH
_________ is secreted by the hypothalamus and stimulates secretion of TSH by anterior pituitary
TSH
____________ secretion is stimulated by TRH and inhibited by free T3 via negative feedback
TSH
What is the first test to order when trying to determine thyroid function?
TSH
What test is the most sensitive indicator of thyroid function w/ normal pituitary?
true
T/F: Measurement of T3 is not generally indicated in patients with hypothyroidism because the T3 level is conserved and may remain within normal range even in patients with significant hypothyroidism
TSH levels
Treatment for thyroid disorders is determined by __________
TSH
Generally, abnormal titers of Abs do NOT require treatment UNLESS ____ is abnormal
hashimoto's thyroiditis
Anti-TPO Abs are most clinically seen with _________
anti-thyroglobulin antibody
What antibodies would you use to monitor thyroid cancer treatment?
anti-TPO antibody
What antibodies are most commonly seen with Hashimoto's thyroiditis?
anti-TSHR antibody
What antibodies are most commonly seen with Graves' disease?
graves disease
anti-TSH receptor Abs are most commonly seen with ______________
RAIU
What test:
-measures iodine uptake by the thyroid
-CONTRAINDICATED for pts who are pregnant and breastfeeding
-elevated w/ thyrotoxicosis (indicates endogenous production of thyroid hormones)
-low uptake w/ subacute, silent, or post-partum thyroiditis
thyroid gland
When palpating and inspecting the lower anterior neck for the ____________, we are looking for:
• Diffuse or asymmetrical gland enlargement
• Tracheal deviation
• Lymphadenopathy
• JVD
• nodules
primary
___________ hypothyroidism:
-thyroid hormone deficiency caused by intrinsic dysfunction of the thyroid gland that disrupts synthesis + secretion of T3/T4
-↑TSH and ↓Free T4
-most commonly hashimoto's thyroiditis in developed countries
-Etiology: surgical resection of thyroid, autoimmune, radioactive iodine therapy tx for hyperthyroidism, external beam radiation therapy for head and neck cancer, large amounts of iodine exposure from radiocontrast dyes/topical disinfectants/amiodarone, lithium, masses, sarcoidosis, hemochromatosis, histiocytosis, surgery, head trauma, sheehan's syndrome --> basically anything that impairs normal hypothalamic or pituitary control of thyroid gland
secondary or tertiary
___________ hypothyroidism:
-central hypothyroidism
-deficient thyroid gland function due to inadequate or ineffective TSH from pituitary (secondary) or hypothalamus (tertiary)
-seen with other hormone dysfunctions and brain pathology
-Etiology: should be suspected w/ known hypothalamic or pituitary disease, pituitary mass/lesion, S/Sx of hypothyroidism and other hormonal deficiencies
hypothyroidism
(hyper-/hypo-) thyroidism:
-decreased metabolism --> fatigue, lethargy, weight gain despite poor appetite, cold intolerance, constipation, weakness, hair loss, memory lapses, worsening of dementia
-accumulation of matrix substances --> dry skin, hoarseness, edema
-decreased hearing, myalgia, arthralgias, paresthesias, depressed mood w/ limited initiative, pubertal delay
-Females: precocious puberty, menorrhagia, amenorrhea, galactorrhea
-Elderly: apathy, depression, memory loss, dec. cognitive function, secondary bone loss
-PE: bradycardia, diastolic HTN, mild hypothermia, coarse/dry/yellow/cool skin, diffuse scalp thinning and lateral eyebrows, brittle nails, diffuse slowing of DTR w/ marked delay in relaxation, normal/atrophic/diffusely enlarged thyroid
TSH
What is the SINGLE BEST TEST for hypothyroidism eval?
TSH and free T4
What labs do you order for eval of hypothyroidism?
mild/subclinical
If the pt labs return and they have increased TSH and normal free T4, you consider them to have _____________ hypothyroidism and you should check anti-TPO Abs
overt
__________ hypothyroidism:
-TSH: inc
-Free T4: dec
-Plan: treat
subclinical
__________ hypothyroidism:
-TSH: slightly inc
-Free T4: WNL
-Plan: treat if S/Sx, goiter, Abs, or pregnant
central
__________ hypothyroidism:
-TSH: dec or WNL
-Free T4: dec
-Plan: MRI, further work up
levothyroxine
The treatment for hypothyroidism is _________________, a synthetic thyroid hormone (T4) that SHOULD BE TAKEN ON AN EMPTY STOMACH FIRST THING IN THE MORNING & avoid iron and Ca2+ containing meds and food near ingestion
6 weeks
You should check TSH again in ______ weeks after starting levothyroxine therapy (monitor free T4 w/ secondary hypothyroidism)