CSF, Ventricles, and Hydrocephalus
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
What is CSF and what are the four roles of CSF?
CSF is a clear colorless fluid that is acellular and is produced within the ventricular system and fills the space around the brain and spinal cord within the subarachnoid space
1) Has four roles as seen above
How is CSF produced
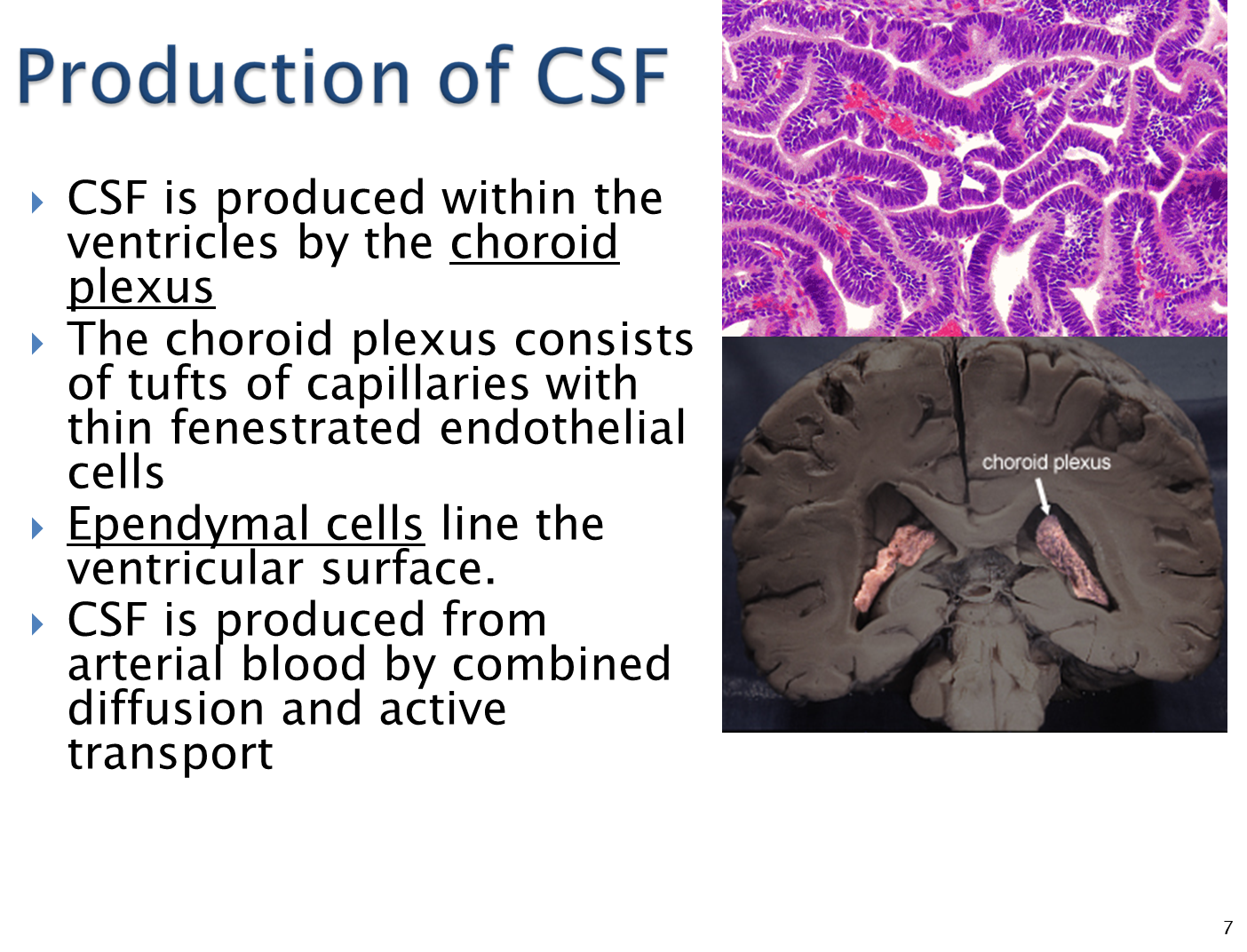
1) CSF is produced by the choroid plexus in the ventricles
→ the choroid plexus is made of tufts of capillaries with thin fenestrated endothelial cells
→ the CSF is produced from arterial blood via active and passive transport
2) the ventricles themselves are lined with ependymal cells
What is a Lumbar Puncture?
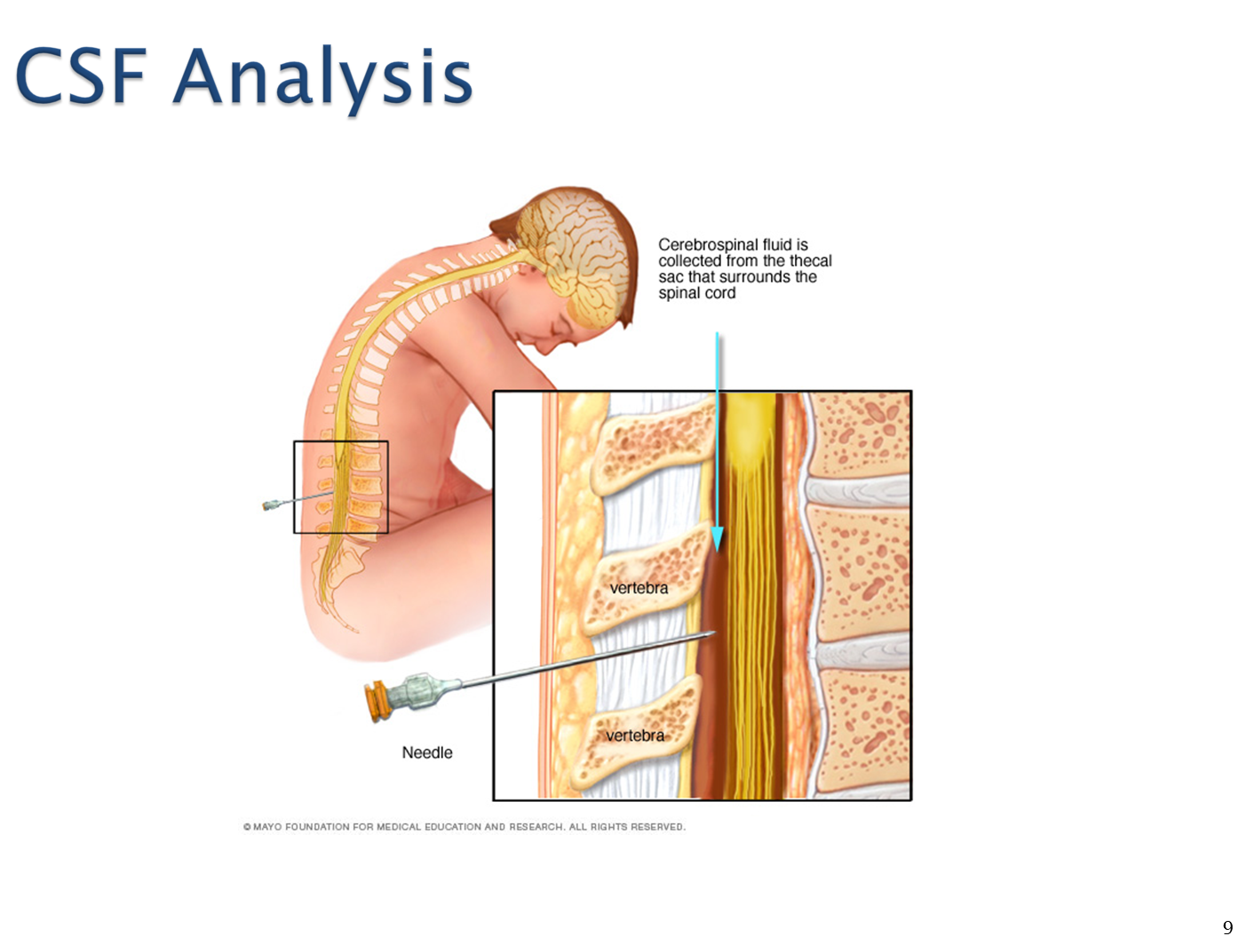
Cerebrospinal fluid is tested via a spinal tap/lumbar puncture where a needle is inserted into the fecal sac
→ allows us to take a sampling of the CSF in order to test for any abnormalities such as the presence of cells or infection
What are the Ventricles and how does CSF flow?
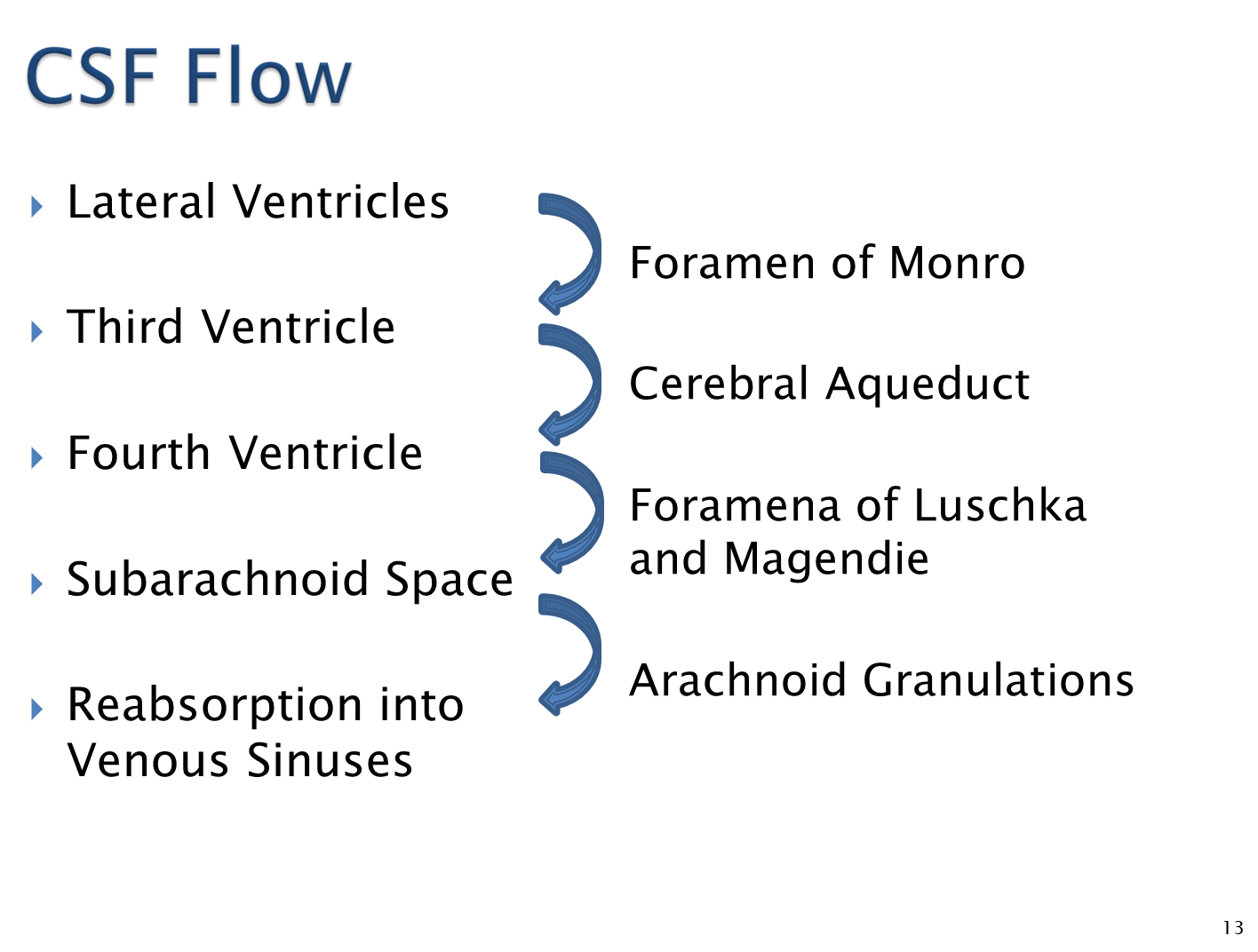
Ventricles are outpouchings that form during the development of the neural tube and contain CSF and are lined by ependymal cells
1) Two lateral ventricles produce CSF which pass through the foramen of monro into the third ventricle
→ the third ventricle then passes into the fourth ventricle within the brainstem via the aqueduct of sylvius
→ foramena of luschka (lateral) and magendie (midline) then pass the fourth ventricle to the subarachnoid space
→ subarachnoid space passes CSF via the arachnoid granulations where it is reabsorbed into venous sinuses
What does it mean that there is compensation in the skull based on the compartments?
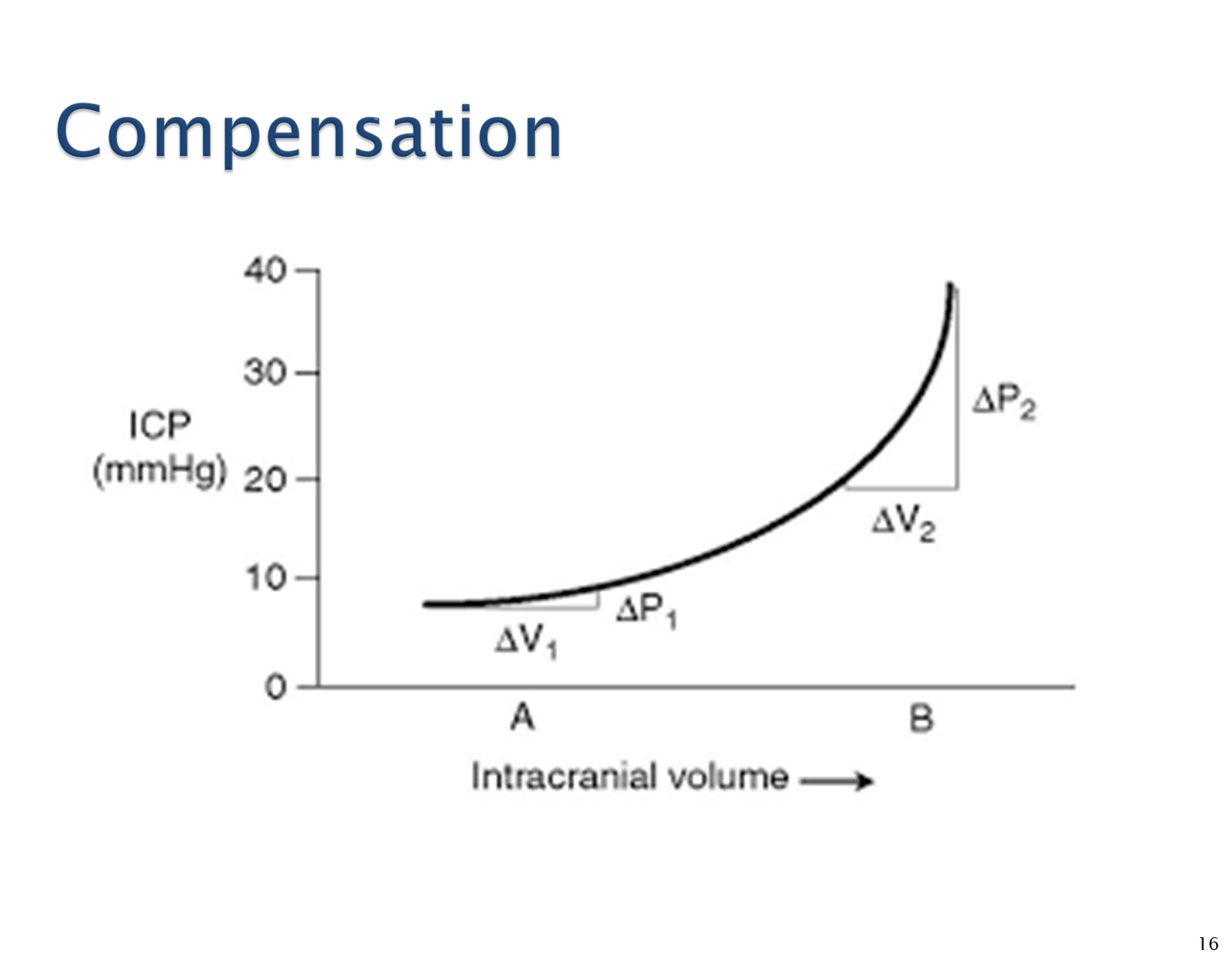
1) Skull acts as a box and it cannot expand. The skull contains brain, blood, and CSF
→ If there is an increase in one part there needs to be a decrease in the other in what is known as the Monro-Kelli principle
2) When compensation cannot occur there is an increase in intracranial pressure when volume increases
→ as pressure increases there is an increased risk of herniation and direct injury to the brain
→ patients may also have decreased cerebral perfusion pressure (CPP) which is equivalent to mean arterial pressure - intracranial pressure
What symptoms might you expect in a patient with increased pressure in the brain?
Patients often present with headaches that worsen when lying down or straining
→ can often also have nausea, vomiting, blurred vision, and confusion
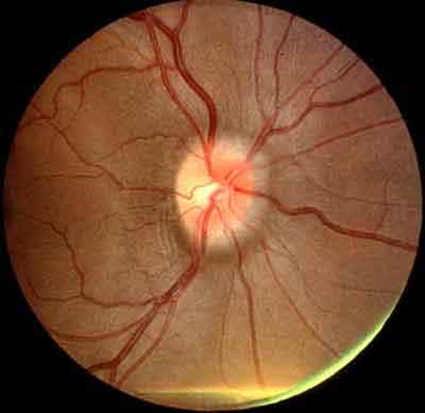
On examination you may see the optic nerve protruding towards you during a HEENT exam
→ may also have impaired eye movement due to abducens nerve weakness
What is Cushing’s Triad?
triad of hypertension, bradycardia, and irregular respirations that occurs during periods of increased intracranial pressure
What is Herniation?
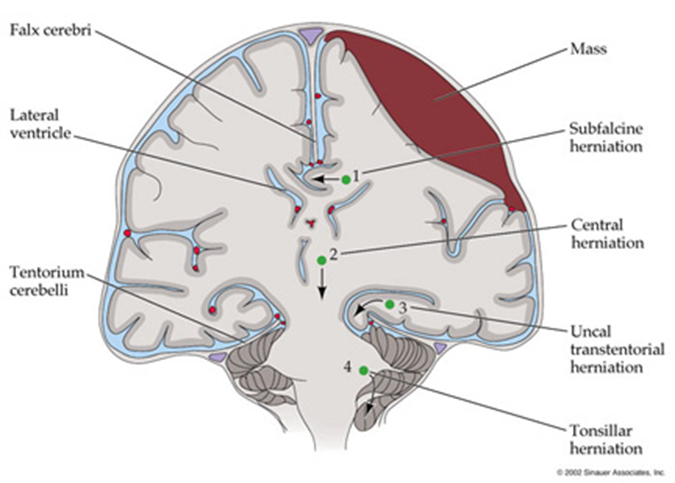
Herniation is where brain tissue is forced from one region into another. It comes in four types
1) Subfalcine
→ when brain tissue (usually the cingulate gyrus) herniates underneath the falx cerebri
2) Central
→ when midbrain tissue and diencephalon are pushed straight downward through the tentorial notch onto the brainstem and cerebellum
3) Uncal/Transtentorial
→ when the medial portion of the temporal lobe (uncus) herniates medially over the tentorium cerebeli, a sheet of dura
→ the uncus will push on cranial nerve III or cerebral peduncle
→ often presents as a dilated unreactive pupil
4) Tonsillar
→ cerebellar tonsils are pushed downward through the foramen magnum
What is Hydrocephalus? What are the three causes?

Hydrocephalus is excess CSF in the intracranial cavity. Can be caused by three things
1) excessive CSF production
→ rare mechanism for hydrocephalus, and is typically associated with some malignancy
2) obstruction of CSF flow
→ Lesion in the brain that blocks the flow of CSF through the ventricular system
3) impaired CSF reabsorption
→ occurs when arachnoid granulations are clogged or damaged blocking the venous sinuses to reabsorb CSF
What is the difference between communicating and non-communicating hydrocephalus?
Communicating - excessive CSF or impaired CSF reabsorption
Non-communicating - some kind of obstruction