Looks like no one added any tags here yet for you.
Define hypersensitivity
immune system: overreaction to a foreign antigen
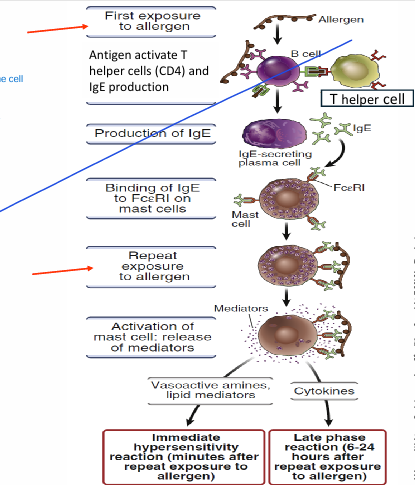
Type 1 hypersenstivity = allergies/anaphylactic
1) Sensitization phase of b cells = prior exposure to antigen
Ex. peanuts -> you eat peanuts (aka antigen)
-> antigen causes immune cells to ACTIVATE
-> activate T helper cells -> communicate w/ B cells
-> switch AB that b cells are producing
-> plasma cells start producing IgE AB
-> now we have specific AB against PEANUT
2) b4 IgE binds to antigen, it binds to MAST CELL, eosinophil, basophil (granulocytes)
- mast cells/eosino/baso covered with IgE AB
3) Later on when re-exposed to antigen (peanut)
- antigen encounters lots of mast cells COATED w/ IgE
-> degranulation occurs (antigen binds to AB ALREADY w/ mast cells)
-> release lots of histamine/cytokines
-> immediate hypersenstivity rxn (increased vascular perm/dilation from histaaine)
4) Degranulation (consequences of T1 hypersenstivity):
lots of histamine, prostaglandin, leukotriens release (degranulation)
Histamine: leads to vascular permeability, vasodilation, smooth muscle contraction
Prostaglandin = VD
Leukotrienes = smooth muscle contraction
Cytokines (late phase) = inflammation
What is anaphylaxis?
Systemic hypersensitivity type 1 rxn
- degranulation occurs systemically (everywhere)
- histamine/prostaglandin disbributed EVERYWHERE in the body
= death within 2-4min
SYSTEMIC VASODILATION/vascular permeability = decrease BP + contraction of smooth muscle (bronchoconstriction messes up the respiratory system)
Type 2 hypersensitivty = AB mediated
(think babies)
1) What causes type 2 hypersenstivity?
2) Discuss the mechanism (baby)
1)
- Transfusion rxn (wrong blood)
- Graves disease
- erythroblastosis fetalis (child/mother blood are incompatible)
2)
A:
- 1st pregnancy mother (Rh+) delivers bby (Rh-)
- baby in contact w/ mother
- mothers body detects foreign antigen (Rh-)
- T help cells call for B cells
- B cells produce IgM (first responder) *but at this pt baby is already out so no more antigen present
- Memory b cell are produced to rmbr this Rh- antigen
B:
- 2nd pregnancy occurs
- Memory b cell activate AB(IgG - SPECIFIC) & attacks fetal RBC
(rhogam to prevent this)
(type 2 hypersenstivity)
Discuss the mechanism for blood transfusion
You have A blood, blood given is B
TLDR = opsonization + complement system
AB attach to type B blood
→ activate complement system
→ induce cell lysis
OR
AB attach to type B blood
→ activate opsonization
→ increase phagocytes
→ +marker for more phagocytes to come
Overall: massive destruction of RBC = accumulate bilirubin = detrimental effects
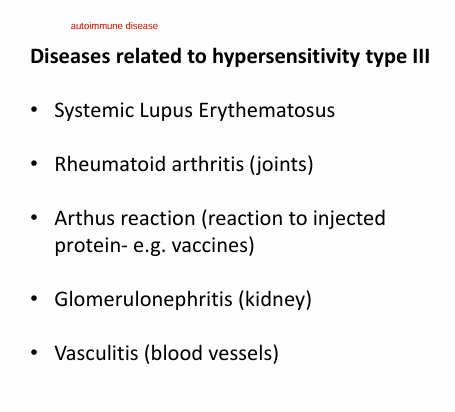
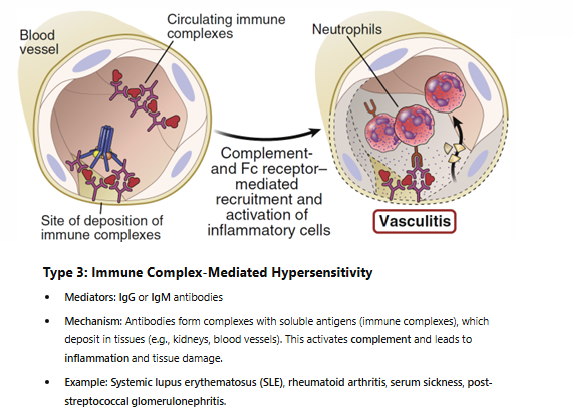
Type 3 hypersenstivity - immune complex mediated.
Discuss the mechanism.
TLDR: Immune complex = IgG + IgM ABs deposited in tissue → impaired clearing + deposition → causes inflammation + tissue injury
Immune complexes (clusters of AB)
- bigger, heavier, larger = harder for us to eliminate
- deposit in our small blood vessels
- start recruiting complement system (recruit neutrophil/macrophage) later on
- we can’t clear fast enough → damage surrounding tissue
- leads to cell destruction
= vasculitis (inflammation of blood vessels)
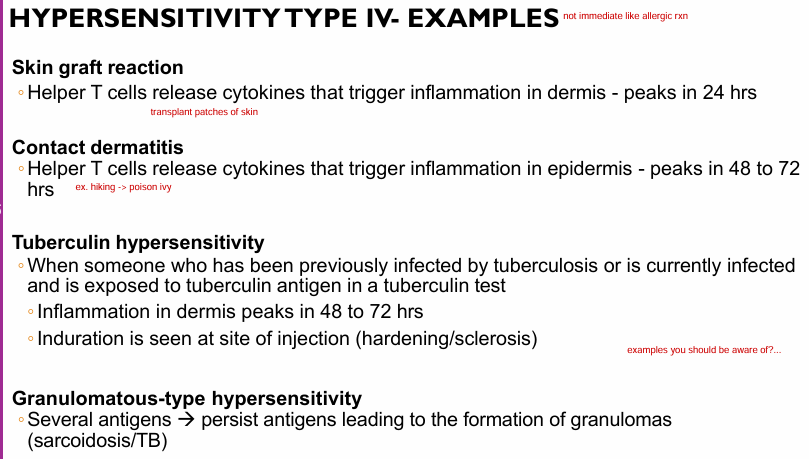
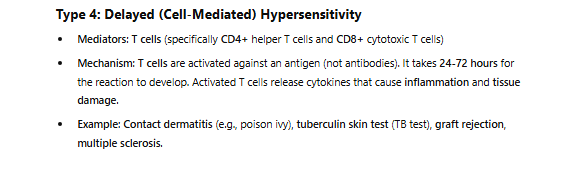
Type 4 hypersenstivity - delayed type
Discuss the mechanism.
Delayed b/c cells take more time than AB
(not about AB, talking about exacerbated sensitization of T cells - TAKES TIME NOT IMMEDIATE)
1) Helper T cells (CD4) or Cytotoxic (CD8) T cells activated
2) Sensitization of Tcells (NOT ABs)
- first exposure = sensitization
3) 2nd exposure/persistent antigen
- t cells activate macrophages
- macrophages overreactive → secrete a lot of cytokines
→ cause exacerbated inflammation
*note its both CD4 and CD8. CD4 above occurs, CD8 will kill it directly
Define autoimmune disease
immune system attacks itself
- loss of self tolerance
(lost ability to look @ our cells as “our own cells”, think its foreign)
What triggers autoimmune diseases?
1) infection
2) geographic location
3) climates
4) lifestyle
5) genetics
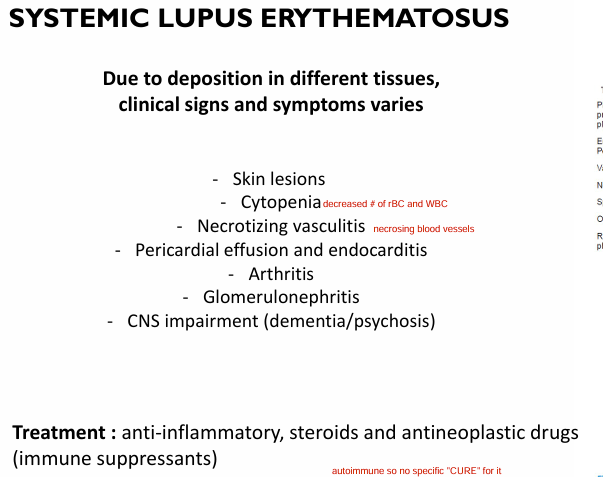
Discuss SYSTEMIC LUPUS ERTHEMATOSUS mechanism
for eli: Autoantibodies = AB your immune system makes by mistake (attacking your own healthy cells)
Multisystem autoantibodies form immunocomplexes → mainly antinculear AB (ANA) which targets DNA & RNA (others also attack, RBC/WBC)
→ immunocomplexes deposit in many tissues (aka hypersensitivity type 3) → mainly arteries/blood vessels
→ we can’t clear fast enough → cause chronic inflammatory response
→ accumulation leads to complement system
→ induces inflammation and necrosis
What are clinical signs and symptoms of SLE?
What are treatments?
1) skin lesions
2) cytopenia (decreased # of RBC & WBC)
3) necrotizing vasculitis (necrosing blood vessels)
4) arthritis
5) no specific “cure”
- anti inflammatory, steroids, antineoplastic drugs (immune suppresants)
6) glomerulonephritis
pericardial effusion/endocarditis
What are risk factors for SLE?
-genetic
-sex hormones (affects women)
-chronic administration of drugs
What are the diagnosis/prognosis of SLE?
Lab findings:
- presence of autoantibodies
- low RBC, WBC
- low platelets
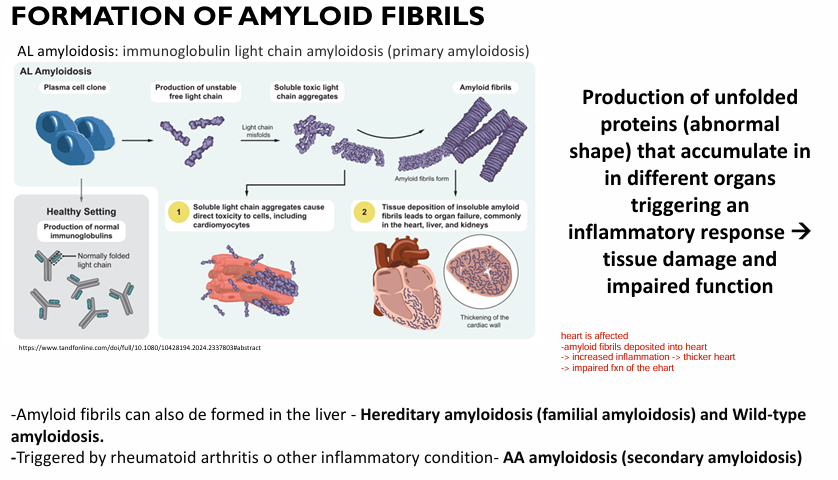
Discuss amyloidosis.
1) what are amyloids?
2) what mechanism induces an inflammatory response in amyloidosis?
0) NOT AUTOIMMUNE, hereditary
1) insoluble proteins produced by our body (normally shape)
2) MISFOLDED amyloid protein (amyloid fibrils) deposited in several organs causing:
- inflammation
- tissue damage
- impaired function
→ amyloid fibrils = seen as foreign → macrophage activated, release cytokines → leads to inflammation
What are the symptoms of organs affected by amyloidosis?
(heart, kidney, GI tract)
1) Heart = arrhythmias + heart failure
2) kidney = renal failure
3) GI tract = malabsoprtion/diahrea
*note depends on magnitude of deposition of amyloid in organs
What is an immunodeficiency disease?
impaired immune function
recurrent infections w/ common pathogen
Define and give examples of a primary vs. secondary immunodeficiency disease.
Primary (congenital - heredity/at birth)
ex. IgA deficiency
- IgA is linings (if you don’t have those, more susceptible to respiratory/GI tract infections)
ex. Digeorges syndromes (thymus aplasia)
- thymus is important for maturation of T cells. No t cells = worsened immune system
Secondary = acquired (ex. AIDS, infected by HIV)
Discuss the following about AIDS:
1) Microorganisms involved
2) Mechanism of action
3) Transmission methods (later)
1) microorganism = HIV
2)
- HIV = RNA retrovirus
- HIV enters host cell (CD4 helper)
- RNA virus trancribes to DNA
- HIV DNA becomes part of Tcell DNA
- Virus replicates, destroying T cells
- Destroying T helper cells = no cytoxic t cells OR B cells = weak immune system
- AIDS = immune system so damaged body is unable to fight infections and sieases
Discuss the following about AIDS:
4) Common clinical features
Acute:
- swollen lymphs
- initial infection
- decreased CD4 count (t helper cells)
Latent:
- generalized lympadenopathy
- CD4 count normal
- minor infections
- dormant ~10years
Clinical AIDS:
- Death
- Pneumonia
- Chronic diarrhea
Discuss the following about AIDS:
3) Transmission methods
3)
-sexual contact (vaginal secretion, semen, breast milk)
- shared needles (drug use)
- blood transfusion
- mother to child (vertical)
How can we clinically prove HIV and monitor?
Lab findings:
- CD4 count <200cells/nanoL
Monitor via:
- PCR or CD4 count