Rad Bio Final
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
What are the 4 (5) R’s? For what type of RT?
conventional fractionated RT
Redistribution (Sensitize Tumors)
Reoxygenation (Sensitize Tumors)
Repopulation & Repair (Preserve Normal Tissues)
Radiosensitivity
In what direction do the 4 R’s work during inter-fraction interval?
opposing
What is Redistribution?
cell-cycle progression into RT-sensitive phases
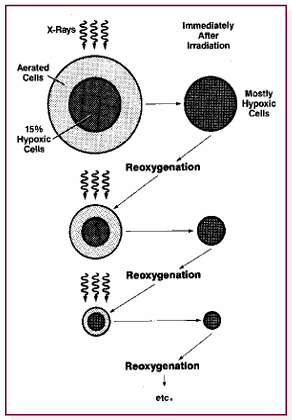
What is Reoxygenation?
oxygenation of surviving hypoxic tumor cells → Fractionation helps to overcome hypoxia
How does Repopulation and Repair affect tumors and normal tissues?
Tumors: decreases rad sensitivity (avoids tumor proliferations)
early-reacting normal tissues: increases rad tolerance with increasing overall treatment time
How is Radiosensitivity modeled?
LQ
What type of fractionation regime will best improve tumor control?
Shorter schedule…
don’t extend duration beyond original prescribed time (avoid tumor proliferation)
Reduce treatment time (counter tumor proliferation)
Inter-fractionation as long as possible (spare normal tissue)
______ Responding normal tissues have similar responses to tumors
Early
Why are late responding normal tissues… late responding?
slow or negligible proliferation
Why do large tumors present less local control after a single fraction treatment?
hypoxic
Clustered DNA damage is a marker for what type of particle?
High LET (Large energy over small distance)
____ are more potent than _____ at recruiting γH2AX
Protons, photons
size and frequency of radiation-induced foci vary as function of what?
Radiation quality (proton > photon), dose, time
as LET _____ OER ______
increases, decreases
Because direct action. less oxygen fixation
Why is oxygen less important for high LET killing?
direct action and less oxygen fixation
What type of radiation is best used for hypoxic tumors?
High LET
How does cell cycle radiosensitivity vary with High LET?
High LET shrinks variation in cell cycle radiosensitivity…. High LET gives better tumor control for slowly growing tumors (many S-phase cells)
2 types of tumors best candidates for High LET?
Hypoxic, slow growing (????)
DNA radical damage caused by chemical repair would best be intervened with..?
Radiation PROTECTOR
DNA oxidation/break/cell death caused by Enzymatic repair would best be intervened with…?
Radiation MITIGATORS?
Radiation Protectors act in what time scale?
up to ms
Radiation mitigators act in what time scale?
seconds to years
Radiation sensitizer does what to the therapeutic ratio curves?
pushes to the left, use tumor selective sensitizer to target the tumor
Radioprotector does what to therapeutic ratio curve?
Pushes to the right, ideally target normal tissues
Radiation Protectors, Mitigators, and Therapeutic agents should each be given when, in relation to time of exposure?
Protectors: Before exposure
Mitigators: After exposure, but before symptoms
Therapeutic Agents: After symptoms occur
What is Amifostine used for?
Radiation protector… delivered minutes before radiation
Why is LD50/60 for Chernobyl ~2x that of Hiroshima & Nagasaki?
Better medical intervention, not in war time
What dose may requiree bone marrow transplant?
7.5-10 Gy
What are the prodromal symptoms of Acute Radiation Syndrome and their doses? From least most severe…
Skin
Hematopoietic (2-8Gy) - death by destruction of Bone Marrow
Gastrointestinal (5-12 Gy) - death by fluid and electrolyte loss.. due to depletion of stem cells
CNS + Cerebrovascular (CNS + CVS) (>20 Gy - 100) - neurologic and cardio breakdown, rapid death within days
What is LD50/60 definition? Values for humans with/without medical intervention?
The lethal dose of radiation causing 50% mortality within 60 days
4 Gy without, 6 Gy with
What limited range of dose is a bone marrow transplant useful?
7 - 10 Gy
How does vomiting onset time change with acute Whole Body Dose?
Faster with increasing dose
from 2hr (1-2Gy) to less than 10 min (>8 Gy)
Min Whole Body dose equivalent for diarrhoea?
4-6 Gy
During what phase is damage expressed?
Latent Phase
How does damage expression timing change with ARS?
decreases with increasing dose… from 21-35 days for mild (1-2 Gy) to no time for Lethal (> 8 Gy)
How is high dose rate data converted to low dose estimates?
DDREF of 2… Dose-rate reduction factor of 2
What is the average lifetime risk of radiation induced cancer? (per Sv)
5-6% per Sv… LOWER FOR MEN
How does lifetime risk of radiation-induced cancer change with age? Values for children and average? (% per Sv)
decreases… 15% per Sv for children, 5% for average population
Where do secondy cancers (radiation induced) occur?
non-involved organs/tissues
How does the risk of RT-induced cancer compare to uncontrolled local recurrence?
RT-induced risk < local recurrence risk
Percent of RT-induced secondary cancers in adults?
< 8%.. suggests most are due to other factors (Lifestyle or genetics)
What factors may increase risk of RT-induced secondary cancers?
age at treatment, larger treatment fields, organs within fields, radiation type
How does risk of RT-induced second cancers vary with dose?
linearly
4 Consequences of Whole-Body Radiation exposure
Prodromal symptoms
Radiation Carcinogenesis
Genetic effects
Effects on the developing embryo and fetus
What phase of damage response can be a biomarker of response to TBI/WBI?
symptomatic prodromal phase
3 tissue-specific dose-dependent radiation syndromes following TBI/WBI (Hematopoetic, GI, CNS..)
excess cancer risk appears at what whole body dose?
100 mSv
Heritable effects are only a real threat if what tissue is irradiated?
gonadal
What is most apparent effect of whole-body irradiation on an embryo/fetus?
microcephaly… small head size
What are the “Triad” of consequences? For what?
Death, growth retardation/malformations, growht disturbances w/o malformations…
all non-cancer effects on fetus/embryo
How is growth affected if radiation incident on organogenesis or fetal stage?
organogenesis - temporary growth retardation
fetal stage - permanent growth retardation
During what stage of embryonic growth will radiation kill the growth?
before or immediately after implantation
during what embryonic development phase is radiation damage most likely to cause abnormalities?
organogenesis
During which phases will prenatal death or neonatal death occur?
prenatal — pre-implantation
neonatal — organogenesis
How many IQ points are lost per Gy?
Average ~30
8-15 weeks after conception — 60 points per GY
no risk less than 8 weeks or greater than 25
The “target cell” hypothesis of radiation injury belongs to which framework? Classical or contemporary
Classical
driven by ongoing cell death AND functional changes in surviving cells describes which framework?
Contemporary
Toxicity reflects cell depletion due to direct cell killing from radiation, leading to subsequent functional deficiency …. which framework?
Classical
Kinetics and structural determinants of the tissues response to radiation deponds on … 3 things?
inherent radiosensitivity of individual cells
cellular growth kinetics of the tissue as a whole
Cellular organization within tissues (MOST IMPORTANT)
What classification describes tissue kinetics?
Michalowskis classification
What types of tissues belong to Michalowski’s classification of tissue kinetics?
H and F types
What types of tissues (Michalowskis) are early responding? Late responding ?
early — H-type (damage quickly evident)
Late — F-type (damage takes time to manifest)
T/F, functional changes take time to develop in late responding tissues?
Functional changes MAY occur immediately in late responding (F-type) tissues
Types of tissues expressing early response? late response?
hierarchical proliferative organization (e.g. skin, GI)
organ specific parenchymal cells (e.g. kidney, lung)
loss of parenchymal cells AND vascular damage is a sign of What type of tissue response?
Late responding
Loss of function is what type of tissue respsonse?
Late responding
A steep dose-response curve is associated with what type of FSU?
serial
If toxicity is caused by a high point dose, what type of FSU is it?
serial
Parallel FSUs are sensitive to toxicity if what volume is irradiated? and to how much dose?
parallel organs are sensitive to toxicity if a large volume is subject to low dose
Examples of serial and parallel FSUs…
Serial: Spinal cord, Gi tract,
Parallel: Lung, Liver, Kidney, Skin
Heat kills cells as a funciton of what metrics? With what relation? (linear, log-linear, log-log)
Time and temperature… log-linear
What temperature kills cells and how?
Above 45 C for enough time.. protein denaturization causes death by necrosis
What is most potent radiosensitizer?
Heat
What temps for anti-tumor effects in RT?
42-45 C
How does heat interact with RT induced DNA damage?
protein denaturation… NOT new DNA damage
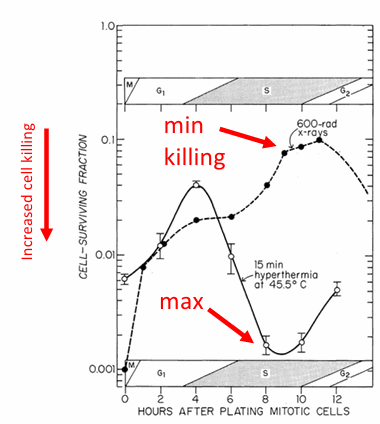
Where in cell cycle is heat most effective as a radiation sensitizer?
S phase
Is hyperthermia more effective in tumor cells or normal cells? What does this mean for therapeutic ratio?
Both… therapeutic gain comes from physiological factors
Where does therapeutic gain come from for hyperthermia?
Physiological factors
How to apply hyperthermia to target tumor?
Nanoparticles, deep heating, shallow heating…
MUST target tumor because not clear trend for HT being more effective for tumors than normal tissues
T/F Heat helps RT because it causes more DSBs
False… Heat does NOT cause DSB. Protein denaturation
How does the energy for cell inactivation compare between hyperthermia and x-rays?
far greater in hyperthermia (above 43 C)
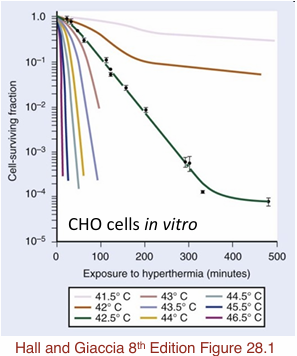
How do survival curves compare for different temperatures of hyperthermia?
43 C has a similar shape to X-ray survival curve.
Below 43 the cells develop tolerance during heating
Above 43 C — Very steeep curves.. different mechanism than x-rays
Hyperthermia alone leads to _______
reproductive cell death… (NOT DSB)
What is predominant repair pathway for RT alone? What type of damage?
NHEJ for DSB repair… (NHEJ > HRR)
Heat doesn’t enhance number of initial DNA lesions from RT, instead it does what?
Aids the conversion of sub-lethal RT lesions into lethal lesions
Chromosomal aberrations due to heat sensitivity of ____ (cellular organelle)
centriole
In terms of sensitivity/resistivity, how does S-phase compare in Radiation-induced cell killing and Heat-induced cell killing?
S-phase most sensitive in Hyperthermia
S-phase most resistant in RT
Apoptosis is a hallmark for what type of cell killing modality?
Heat-induced (HEAT ALONE)
What is main action of Heat & RT?
inhibition of repair (NHEJ) of RT-induced DNA DSBs
What effect does hypoxia have on heat/radio sensitivity?
Heat sensitive, Radioresistant… Poor vasculature so no cooling effects. Increased pH increases heat sensitivity
What effect does pH have on heat/radio sensitivity?
increased pH (acidic) increases Heat sensitivity
What time frame is most optimal for hyperthermia during RT?
20 min before, during, after (40 min total)
What is the TER for in-vivo breast cancer study for hyperthermia in mice?
~5
58 Gy compared to 12 Gy @ 50% tumor control
Thermal Gain Factor equation?
TGF = TERtumor / TERnormal tissues
When to apply heat for best TGF?
AFTER RT!! Within 6-8 hours
Most effective treatment is heat at time of RT… but best TGF after treatment because normal tissues have had time to repair
How does Quiescence affect growth fraction?
More quiescence decreases growth fraction and increases cell less → slower growth…
Queiescent is non-proliferating
What are the Cell Cycle, Potential doubling, and Volume doubling times of a typical tumor?
Cell Cycle: 2 days
Potential doubling, Tpot = 5 days
Volume doubling, TD = 60 days
What factors does Potential doubling time include?
Cell cycle time and Growth fraction → 2 days and 40%
WWhat factors are does Volume doubling time include?
Cell cycle time, Growth Fraction, Cell loss factor → 2 days, 40%, 90%
What type of gene drives cell growth? (proliferates tumors)
Oncogenes - kinases
What type of gene controls growth?
Tumor suppressors - Phosphates (PTPs)