Exam 1- NSG 3130 Questions with 100% accurate solutions+ rationales 2026
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Health
State of complete physical, mental, and social well-being, not merely the absence of disease (WHO).
Wellness
Process of self-care achieved by making choices that lead to a healthy life.
Basic Human Needs Model
Maslow's hierarchy used to prioritize care; physiological needs must be met before higher-level needs.
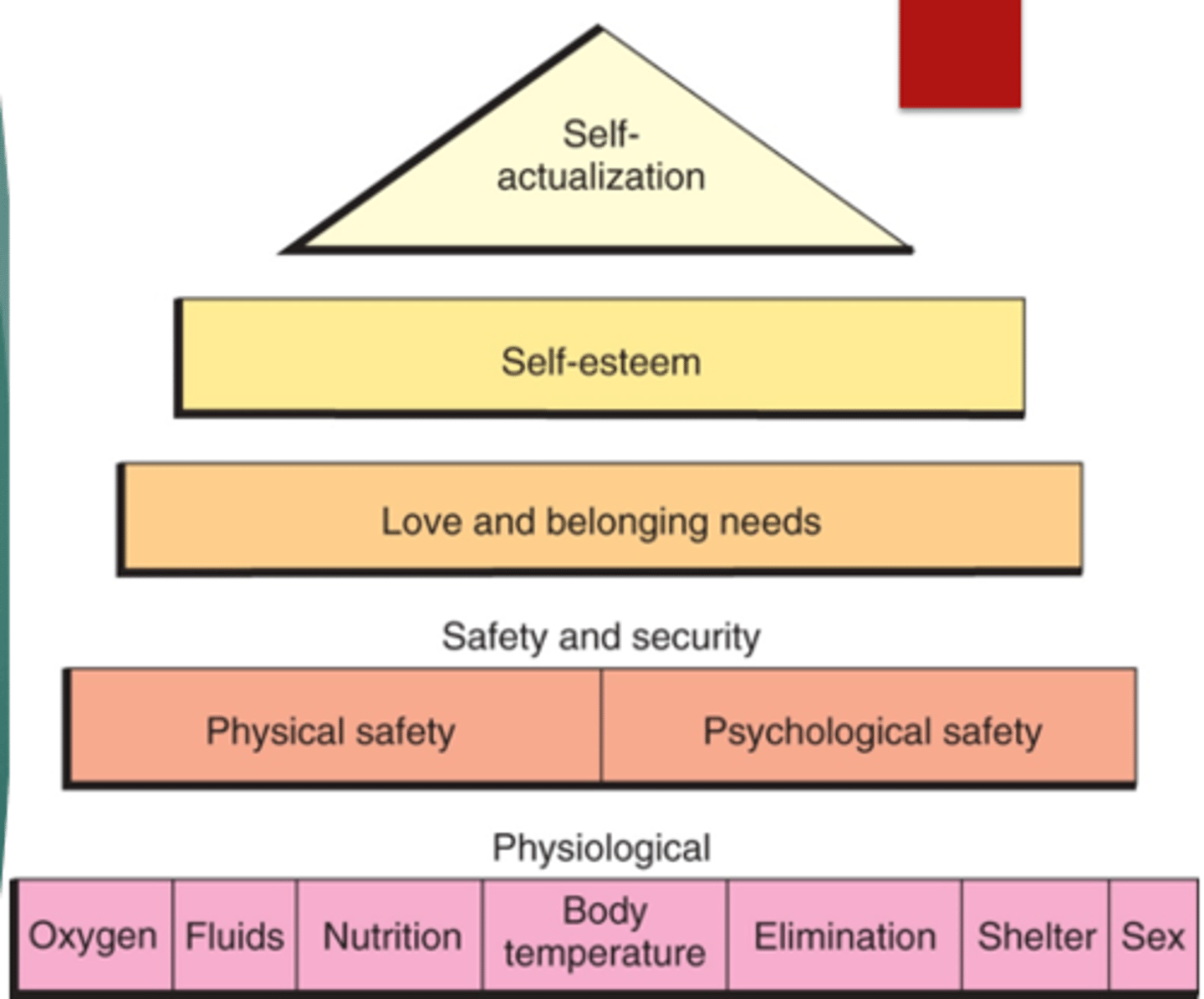
Self-Actualization
The motivation to reach one's full potential after lower-level needs are satisfied.
Health Belief Model (HBM)
Explains why people take preventive actions based on perceived susceptibility, severity, benefits, barriers, cues to action, and self-efficacy.
Health Promotion Model (HPM)
Describes health as a positive dynamic state; behavior is motivated by desire to increase well-being.
Holistic Health Model
Views the body, mind, and environment as interacting; patient is active in healing process; uses complementary therapies (e.g., yoga, art, music).
Risk Factor Reduction
Gradual improvement of health behaviors to lower disease likelihood (e.g., exercise, smoking cessation).
Nurse's Role in Health Promotion
Model healthy lifestyles, teach self-care, involve patients in health goals, and educate about prevention.
Primary Prevention
Prevents disease onset through health education, immunizations, and risk assessments.
Secondary Prevention
Early detection and treatment of disease through screenings (e.g., mammograms, BP checks).
Tertiary Prevention
Restoration and rehabilitation after illness to return to optimal function (e.g., diabetes education, rehab).
Acute Illness
Short-term, abrupt onset, <6 months, with rapid appearance of symptoms.
Chronic Illness
Long-term condition >6 months, involves ongoing care, periods of wellness and exacerbation.
Stages of Illness Model
Explains how people cope with illness: 1) symptom experience 2) sick role 3) medical contact 4) dependent role 5) recovery.
Factors Affecting Health
Age, gender, genetics, lifestyle, environment, self-concept, beliefs, culture, and access to healthcare.
Internal Variables
Biological, psychological, and cognitive factors influencing health.
External Variables
Environmental, socioeconomic, cultural, and social support influences.
Non-Adherence Management
Find reason directly from patient, explore causes, show caring, encourage healthy behavior, use aids, and allow patient freedom in choices.
Health Risk Assessment
Identifies patient risk for disease/injury in next 10 years.
Health Promotion Across the Lifespan
Children: safety; Teens: substance use, sexuality; Adults: lifestyle diseases; Older adults: falls, depression, oral health.
Homeostasis
Balance of physiological processes that maintain internal stability.
Compensation
Body mechanism to maintain balance (e.g., ↑ heart rate for low BP).
Culture
Socially transmitted beliefs, values, and ways of life.
Ethnicity
Identification with a cultural group based on shared beliefs, customs, and language.
Enculturation
Process by which individuals learn their culture from birth.
Acculturation
Cultural change resulting from first-hand contact between groups.
Transcultural Nursing
Care that considers cultural similarities and differences for culturally congruent care.
Emic Perspective
Insider's (patient's) view of their culture.
Etic Perspective
Outsider's (nurse's) objective view of the patient's culture.
Health Disparities
Differences in care and outcomes between populations (e.g., minorities, low-income, elderly).
Cultural Competence
Ability to interact effectively with people of different cultures and beliefs.
Cultural Sensitivity
Recognizing and respecting cultural differences in care.
Culturally Congruent Care
Uses cultural knowledge in meaningful and safe ways to promote health.
Cultural Self-Assessment
Nurse examines their own beliefs and biases before providing care.
Generalization
Broad assumption about a group based on patterns.
Stereotype
Fixed, often negative belief about a group.
Prejudice
Judgment or opinion formed without adequate knowledge; can lead to discrimination.
The Joint Commission (TJC)
Requires healthcare facilities to meet standards for cultural competence and effective communication.
Culturally Responsive Care
Ask permission before touch, explain procedures, and include patient beliefs in care.
Delegation
Transfer of responsibility to a competent individual for a specific task while the RN retains accountability.
RN Responsibility
RN must assess, plan, evaluate, and follow up on delegated tasks.
1st Principle of Delegation
Know state nurse practice act, policies, and scope of practice.
2nd Principle of Delegation
RN cannot delegate assessment, planning, evaluation, or accountability.
3rd Principle of Delegation
Delegate cannot re-delegate the task to another person.
5 Rights of Delegation
Task, Circumstance, Person, Direction/Communication, Supervision/Evaluation.
UAP Tasks
Vitals, I&O, bathing, feeding, ambulation, postmortem care, safety setup, simple dressings, weights, CPR.
LPN Tasks
Administer meds (not IV unless certified), wound care, NG/foley insertion, reinforce teaching, enteral feedings.
RN Tasks
Assessment, teaching, evaluation, discharge planning, blood transfusions, complex care.
Unsafe Delegation Example
UAP redelegates vital signs to student nurse — NOT permitted.
Health Care Documentation
Written/electronic record describing patient, health status, care provided, and dates.
Documentation Standards
Set by facility policy, The Joint Commission (TJC), and CMS.
Correction Errors
Draw single line, label 'error,' sign with initials; never erase or alter record.
Medical Record
Legal document containing comprehensive info about patient care.
Electronic Health Record (EHR)
Collection of data over time from multiple sources; shared across settings.
Electronic Medical Record (EMR)
Record of one episode of care (e.g., one hospital stay or visit).
Narrative Charting
Chronological documentation; may be lengthy or repetitive.
Problem-Oriented Medical Record (POMR)
Integrates all disciplines' notes; formats include PIE, APIE, SOAP, DAR, etc.
PIE Note
Problem, Intervention, Evaluation.
SOAP Note
Subjective, Objective, Assessment, Plan.
SOAPIE/SOAPIER
Adds Interventions, Evaluation, Revision.
DAR Note
Data, Action, Response.
Charting By Exception (CBE)
Only documents abnormal findings; assumes all else is normal.
Flow Sheets
Used for routine documentation (e.g., vitals, I&O, MAR, skin checks).
Kardex
Quick reference for key patient info, meds, treatments, and daily needs.
HIPAA
Protects all patient health information; written consent required for disclosure.
Hand-Off Report
Process of transferring patient-specific information to ensure continuity and safety.
SBAR/ISBAR
Communication format: (Identify) Situation, Background, Assessment, Recommendation.
Incident Report
Documents unusual events; not part of medical record.
Sentinel Event
Event causing serious harm or death; often related to communication failures.
Documentation Do's
Chart teaching, patient words in quotes, responses to interventions, and objective findings.
Documentation Don'ts
Do not leave blanks, chart before completing task, or use vague/bias language.