wilhelm IBS + gas
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
which gender and age is IBS most prevalent in
women, 30-50yrs
t/f: patients with IBS have more GI motility both post consumption and at baseline
true
t/f: patients without IBS report more pain than pts with IBS as rectal distention increases
false. pts WITH IBS report more
IBS is a multifactorial disease with pain resulting from which types of abnormalities
- psychosocial
- motility
- sensory
- CNS processing
(ex: stress can cause chronic inflammation and pain seen in IBS)
rome IV criteria for IBS dx
1. recurrent abdominal pain at least 1 DAY PER WEEK in LAST 3 MONTHS with 2 of the following: related to defecation, change in times you poop, change in appearance of poop
2. symptoms started 6 MONTHS before dx
3. other GI diseases are excluded, with NO ALARM symptoms
what are the "alarm symptoms" that exclude an IBS diagnosis based on the rome iv criteria
ABCD WAP-> alarm sx that exclude IBS dx
1. Age= over 50
2. Bleed in GI
3. Colon cancer family hx
4. Diarrhea= fasting, nocturnal, large
5. weight loss, unexplained
6. anemia
7. pain= persistent or progressive
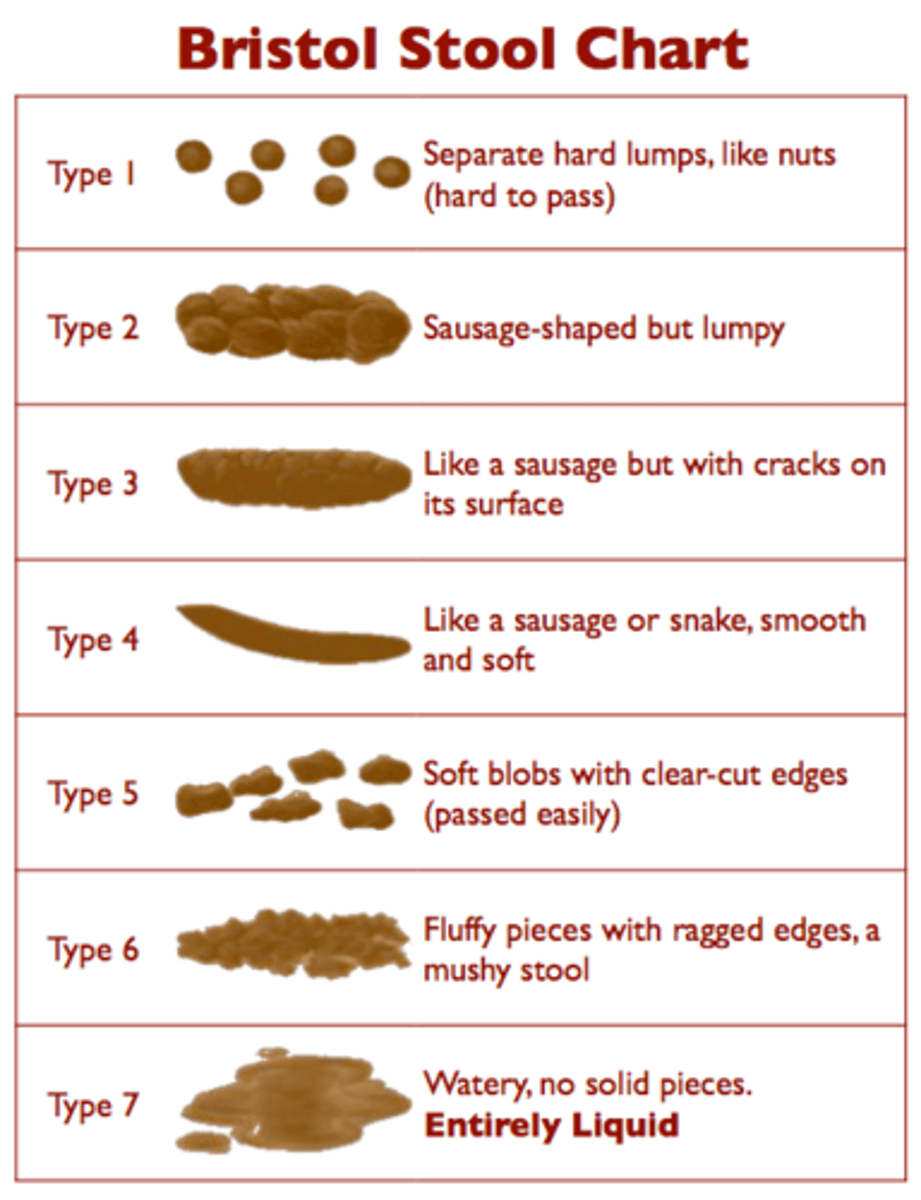
bristol stool chart
Medical aid to classify stool
types 1/2: constipation
types 3/4: ideal
types 5-7: diarrhea
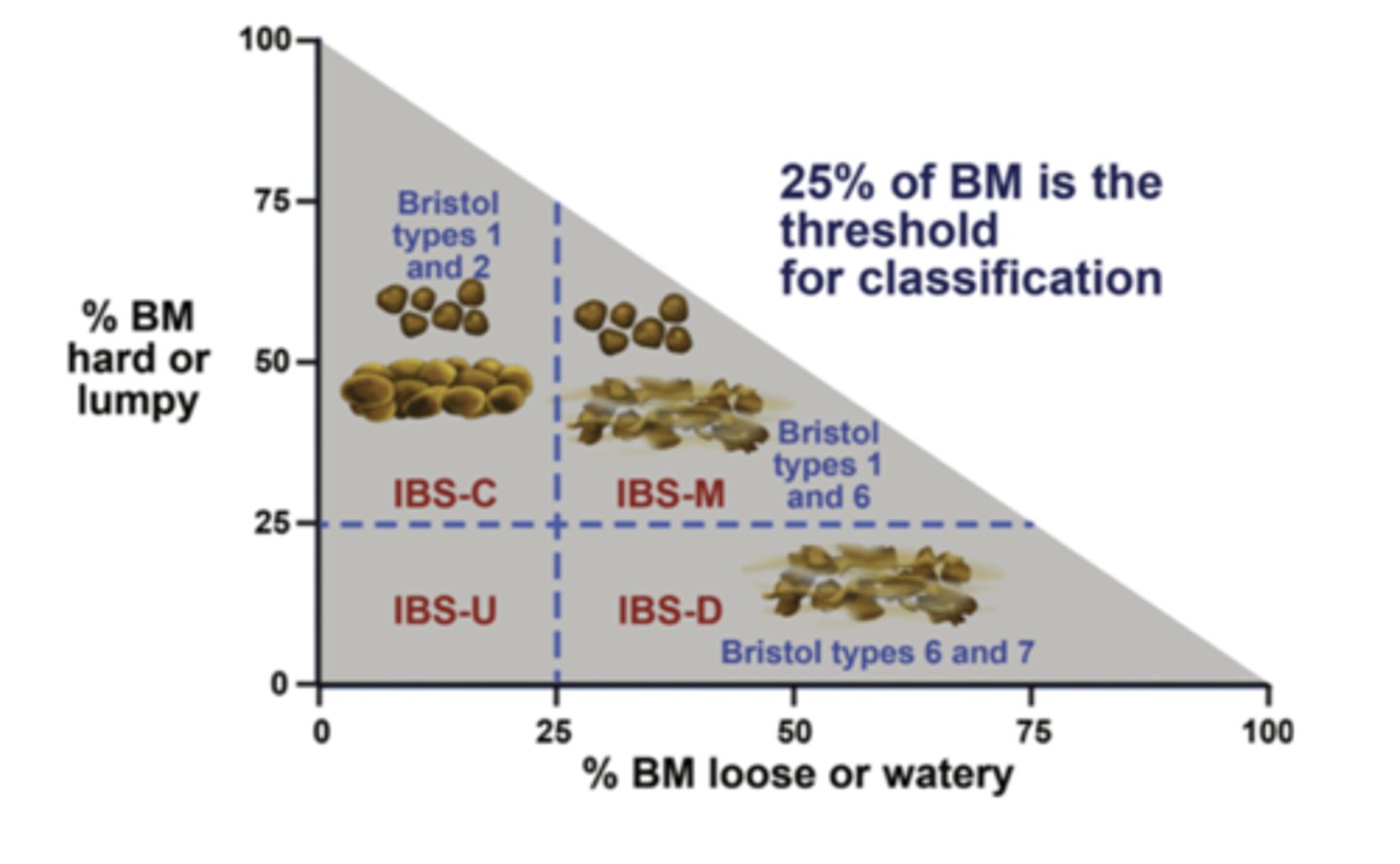
what are the 3 IBS subtypes and which bristol stool types dominate
1. IBS-C= constipation, types 1 and 2 (over 25%)
2. IBS-D= diarrhea, types 6 and 7 (over 25%)
3. IBS-M= mixed bowel habits
diarrhea is classified as >____ stools per day
more than 3 per day
constipation is classified as
less than 3 stools per week
t/f: clinical presence of IBS may be abdominal pain, diarrhea, mucus passage, and GI bleeding
false. all of them except for GI bleeding- remember thats an alarm sx!!
non-pharm diet modifications for IBS tx
1. SOLUBLE fiber: psyllium, polycarbophil
[wheat bran is insoluble and can cause gas,distention,pain]
2. eliminate gluten (see if gets better)
3. reduce FODMAPS
what are FODMAPS
Fermentable
Oligosaccharides (wheat,beans)
Disaccharides (lactose/dairy)
Monosaccharides (fruits, corn syrup)
And
Polyols (processed, sorbitol, mannitol)
-> these are carbs not digested in GI, stay and ferment
what are the 2 ways that FODMAP ingestion can be modified in IBS
1. eliminate everything and gradually add back
or
2. eliminate one at a time
what are non-pharm tx for IBS, other than diet
1. stress relief= breathing techniques, relaxation
2. physical activity
3. psychosocial/ cognitive behavioral/ hypno
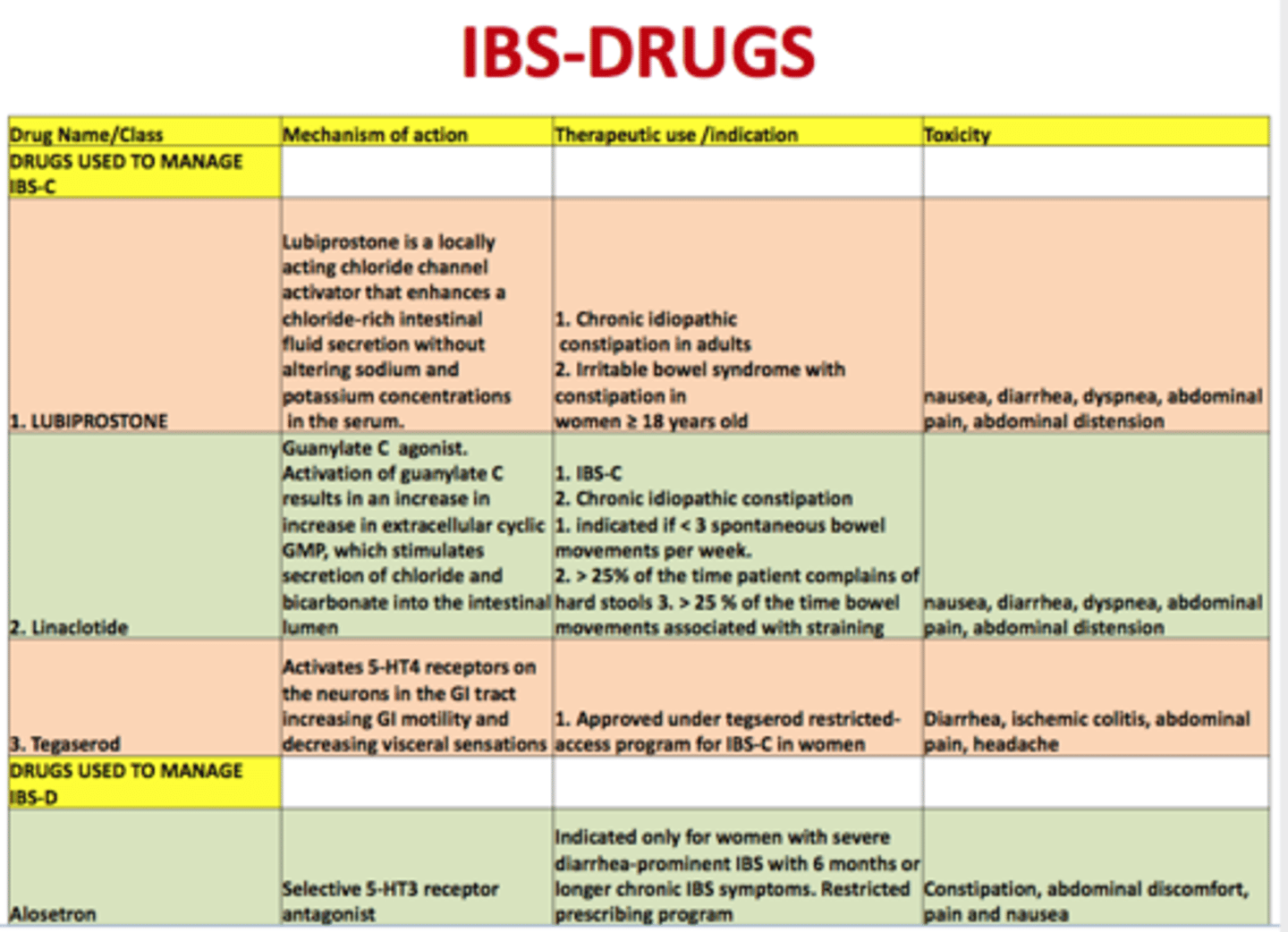
treatment for IBS-constipation (summary)
1. guanylyl cyclase c agonists: linaclotide and plecanatide
2. chloride channel activators: lubiprostone [women, bid, food]
3. sodium/H exchanger 3 inhibitor: tenapanor
4. fiber: psyllium and polycarbophil [avoid wheat/insoluble]
5. osmotic laxative: PEG (no effect on pain)
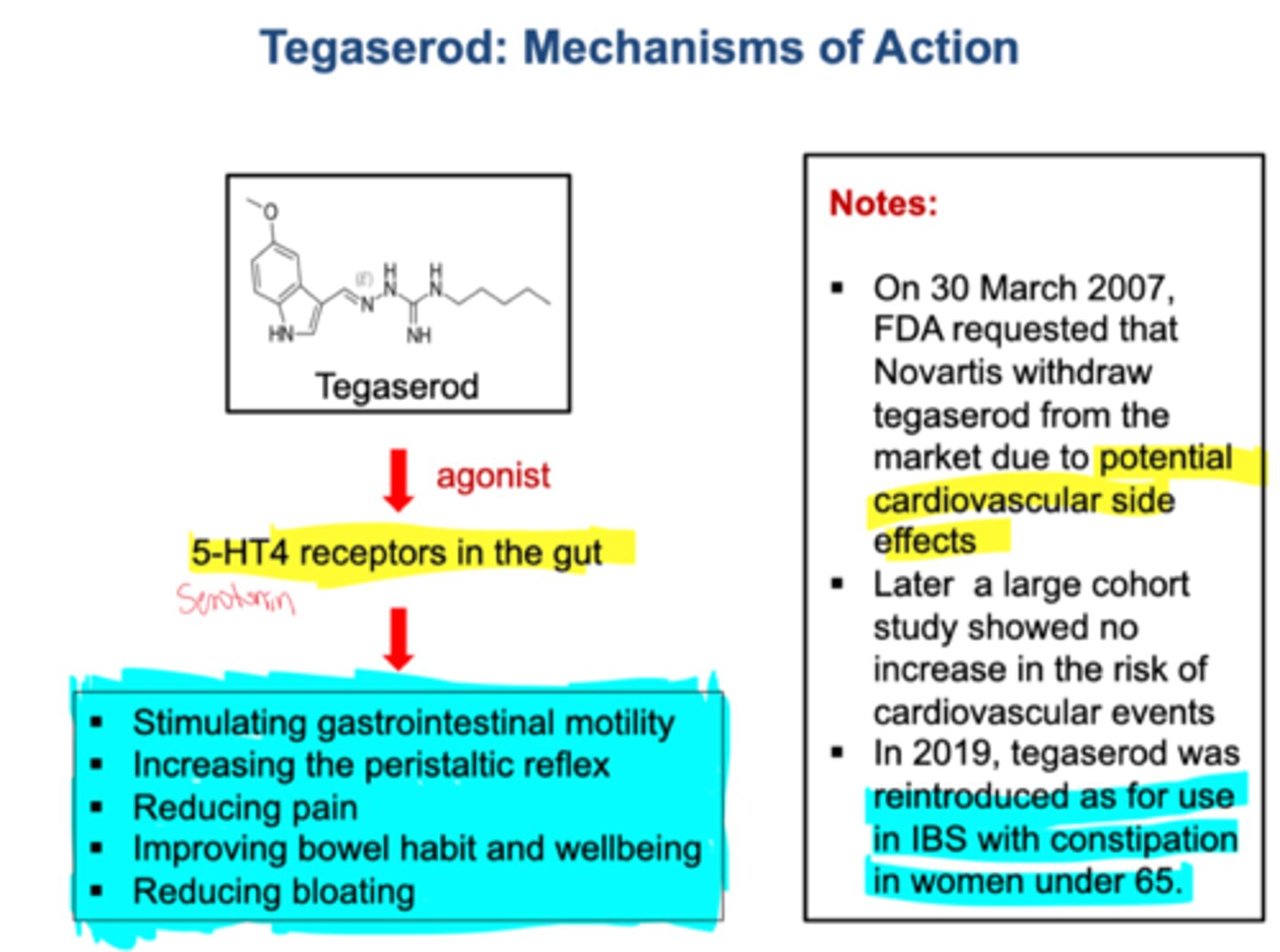
6. 5HT4 partial agonist: tegaserod [NOT AVAILABLE]
linaclotide
class/moa:
use:
guanylate cyclase C agonist
for IBS-C
plecanatide
class/moa:
use:
guanylate cyclase C agonist
for IBS-C
lubiprostone
class/moa:
use:
chloride channel activator
for IBS-C in WOMEN
BID with food
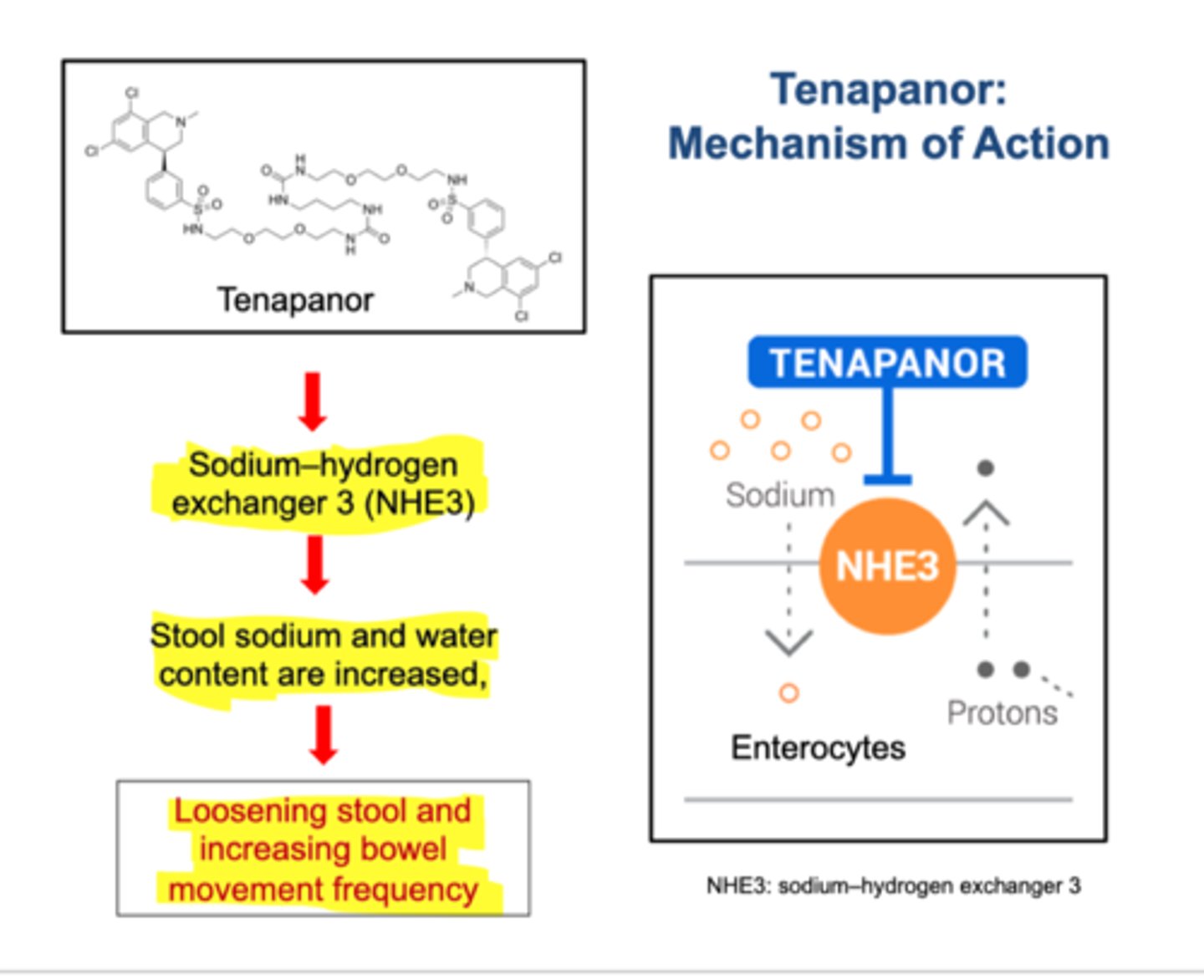
tenapanor
class/moa:
use:
sodium/hydrogen exchanger 3 inhibitor (NHE3 inhibitor)
for IBS-C
increases electrolytes and fluid in GI tract
which fibers would you recommend for IBS-C
psyllium or polycarbophil [NOT INSOLUBLES/ WHEAT BRAN]
titrate slowly
what osmotic laxative would you recommend for IBS-C
PEG-> increases stool frequency but does not help with pain
tegaserod
5ht4 partial agonist for IBS-C
NO LONGER AVAILABLE
what CAM supplement would you recommend for IBS-C?
moa?
limitations?
cascara sagrada=> stimulates colonic motility, increases propulsions
limitations: might cause pain and diarrhea, leading to fluid/electrolyte disorders
cascara sagrada
moa:
CI:
for IBS-C; stimulates colonic motility, increases propulsions
CI: intestinal obstruction, stenosis, atony, inflammation in colon
treatment for IBS-diarrhea (summary)
1. opioid agonists: loperamide
2. probiotics (balance microbiome)
3. antibiotics: rifaximin (balance microbiome)
4. opioid agonist/antagonist: eluxadoline
5. bile acid sequestrants: cholestyramine and colestipol
6. 5-HT3 antagonists: alosetron [BLACK BOX stop if constipated]
loperamide
opioid agonist
for IBS-D
does not treat pain
t/f: both probiotics and antibiotics (rifaximin) are recommended for IBS-D to balance the microbiome
true
eluxadoline moa
both an opioid agonist and antagonist that works to
1. decrease pain
2. control GI motility
cholestyramine
bile acid sequestrant
for IBS-D, bile acids increase in IBS-D which can worsen diarrhea so this is used as a control and usually combined w other drugs
colestipol
bile acid sequestrant
for IBS-D, bile acids increase in IBS-D which can worsen diarrhea so this is used as a control and usually combined w other drugs
alosetron
Serotonin 5-HT3 receptor antagonists
for IBS-D in WOMEN
BLACK BOX: stop if constipated
alosetron moa
5-HT3 receptor antagonist used for IBS-D, stops peristalsis, secretion, and sensation
what black box warning is seen with alosetron
stop immediately if constipation or ischemic colitis occurs
eluxadoline (Viberzi) contraindications
alcoholism
biliary duct obstruction
pancreatitis
severe hepatic impairment
chronic/severe constipation
t/f:eluxadoline is a strong cyp3a4 inhibitor
true
which 2 bacterial strains are most effective in IBS-D
lactobacillus and bifidobacterium
probiotics moa
-Replenish normal flora which suppresses growth of diarrhea-causing bacteria
-anti-inflammatory
- reduce visceral afferent hypersensitivity, help restore mucosa
small intestinal bacterial overgrowth (SIBO)
abnormally large numbers of bacteria present in the small intestine's proximal half
->increased gas and distention early on
in a study that compares low dose, medium dose, and high dose probiotics, which one did the worst and why?
high dose did the worst bc it never even dissolved. low and med were same
treatments for abdominal pain in IBS (summary)
1. TCAs= amitriptyline, nortriptyline, imipramine
2. SSRIs= paroxetine, sertraline, citalopram
3. smooth muscle antispasmodics= dicyclomine, hyoscyamine, peppermint oil EC
what type of IBS are TCAs used for
IBS-D
they target both pain and diarrhea
give low doses
which medication can be given for IBS pain and comorbid depression
SSRIs= paroxetine, sertraline, citalopram
(also have some promotility action)
which medications can be given for both pain and diarrhea in IBS
smooth muscle antispasmodics (dicyclomine, hyoscyamine, peppermint oil EC capsules) and TCAs (-triptylines)
TCAs
moa
when do pts benefit
reduce visceral nerve sensitivity, help w pain
efficacy w LOWER doses
pts without depression benefit in 2-4 weeks
TCAs adverse effect
anticholinergic ADEs, increase appetite, nausea, heartburn
high dose: cardiac arrhythmias, reduces seizure threshold
when are SSRIs given in IBS
pts with depression. they might also have a reduction in IBS symtpoms
-> but it is NOT generally recommended if theres no depression
peppermint oil
MOA
ADRs
moa: antispasmodic, interferes w calcium movement. reduces foaming, bloating, and gas formation
ADRs: renal failure, nephritis, increased bile production!, reduces LES pressure== may worsen reflux
which pts should avoid peppermint oil EC capsules for IBS pain tx
cholelithiasis (bc this increases bile) and GERD (bc this reduces LES pressure and worsens reflux)
oligosaccharides
diet sources:
cause of gas:
legumes/veggies
absence of alpha-galactosidase
disaccharides
diet sources:
cause of gas:
lactose: milk, ice cream, yogurt
low lactase activity
monosaccharides
diet sources:
cause of gas:
fruit, honey, veggies, soft drinks
slow intestinal transport
complex carbs
diet sources:
cause of gas:
fruit, flour, veggies, refrigerated wheat products
naturally resistant to amylase
fiber
diet sources:
cause of gas:
whole grains, veggies, fruits
absence of alpha-glucosidase
summarize tx options for gas
1. diet: omet offending foods
2. OTC: simethicone, activated charcoal, gripe water, probiotics
3. enzyme deficiency: supplements, lactase (dairy), galactosidase (beans, legumes)
when should alpha-galactosidase supplements be avoided
-diabetes-> may increase absorption of carbs and increase blood sugar
-children
simethicone
MOA:
CIs:
foaming agent, joins gas bubbles in STOMACH so its more easily belched away (no effect on intestinal gas)
DO NOT USE MORE THAN 2 WEEKS
CIs: avoid combo products w electrolytes in kidney disease!
how long can simethicone be used for
no more than 2 weeks
activated charcoal
MOA:
CIs:
reduce INTESTINAL gas (compare to simethicone which works on stomach)
CIs: do not use if decreased bowel sounds, GI obstruction, electrolyte imbalance
how can gas be treated in pediatrics? what should be avoided?
1. simethicone drops= preferred
2. lactase= children >2
3. gripe water (fennel and ginger):>2 weeks old
AVOID:
alpha-galactosidase= NOT for infants and children