13- Clinical Try in of Dentures
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
What must you determine during the try-in of a waxed-up RPD?
The acceptability of the VDO, centric and eccentric occlusion, and appearance
In a CD/RPD, how do you evaluate the VDO?
Begin by evaluating the interocclusal distance while the mandible is in rest position and check the closest-speaking space while the pt reads aloud
Why is it unacceptable to judge the adequacy of the occlusal by intraoral inspection?
Because the denture base can move too easily on its soft tissue support and mask any errors
How can you verify centric relation with a record?
Put 2 layers of Aluwax on the maxillary posterior teeth
Patient closes into CR
Put the record back on the mounted casts
If the teeth fit do not fit perfectly into the indentations they made, CR is incorrect
Take another CR record
Repeat until it fits
Use TWO layers of Aluwax. Why not one layer?
Teeth may penetrate the wax and contact each other, causing a faulty record
What can happen if teeth touch while obtaining the record?
Base or jaw can shift and cause a faulty record. Distal extension bases can be displaced as least as easily as CD bases when excessive closing forces are applied
What is the point of getting patient approval of esthetics at the try-in?
Make sure the patient likes how it looks because once it's processed, changes are much harder
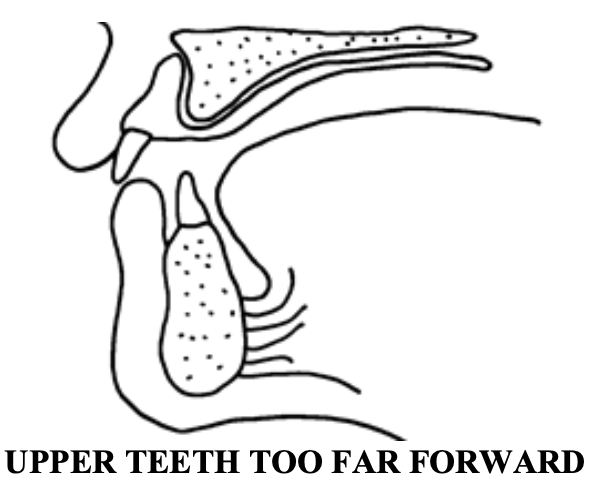
Speech problems help the doc identify tooth-positioning errors. What if the maxillary teeth are set too far forward?
Speech will be slushy, and the "S" especially difficult to enunciate because the lower incisors do not approach the upper incisors close enough to restrict the air flow and create the required hiss
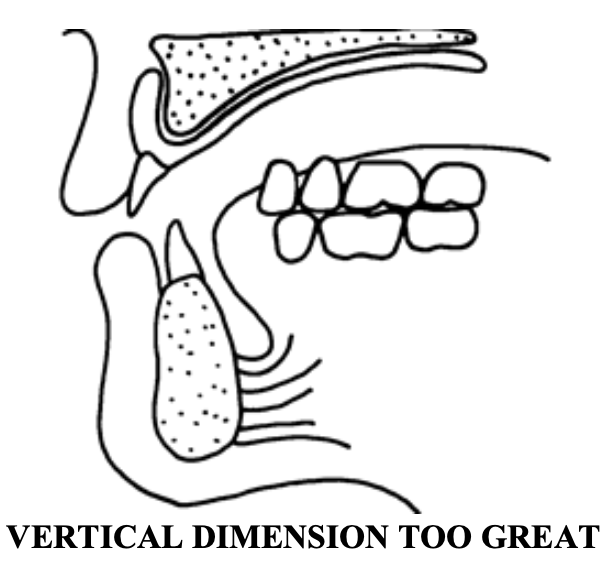
Speech problems help the doc identify tooth-positioning errors. What if the VDO is too great?
A frequent cause of this is not closing the jaws far enough when recording centric relation. S, J, Z, all become slushy because the tongue can't control airflow properly through the oversized space
What is the purpose of a remount cast?
Because the denture teeth move slightly during processing; remount the prosthesis for occlusal adjustment before/after delivery
What is the sequence for creating a remount cast?
Take an alginate impression
Put Play-Doh in areas that would lock the cast in (blockout)
Pour up tooth portion with Die-Keen (do not include distal extension areas)
Why should you avoid pouring Die-Keen in distal extension areas?
Because the remount cast is only there to support the framework and teeth during occlusal adjustment
Why is a remount cast impression not made for an immediate denture?
Because immediate dentures are remounted in the laboratory prior to delivery
If the patient is missing anterior teeth, why do you put missing teeth onto the immediate denture baseplate for the try-in
To evaluate tooth color, tooth position, and esthetics before processing
In a tooth-supported partial denture (class III) opposing natural teeth, what are you checking when you evaluate VDO and CO?
Does the patient bite the same with the RPD in as they did before?
How should you evaluate VDO and CO in class III cases?
Use articulating paper intraorally
Do you need protrusive records for class III cases?
The condylar mechanisms are arbitrarily set at 30 degrees with the occlusal plane parallel to the upper member of the articulator, so usually no. Check if working contacts look acceptable, you don’t need balancing contacts
With a distal extension RPD, how do you check VDO and CO?
The bases can be intruded into soft tissues and mask an occlusal error. So, ask the patient to close the jaws until teeth “feather touch” and evaluate occlusion at the first point of contact
In distal extension cases, it is necessary to have a protrusive record?
No, because the opposing natural teeth provide sufficient guidance and balancing is not desired. Check intraorally with articulating paper