Lecture Notes: Applied Psychology & Clinical Psychology (PSYC4130/PSYC2220)
1/46
Earn XP
Description and Tags
Vocabulary flashcards covering key terms from the lecture notes on Applied Psychology and Clinical Psychology.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
47 Terms
Applied Psychology
The professional application of psychological knowledge to solve problems associated with human behaviour and improve mental health, relationships, or social outcomes.
Clinical Psychology
A subfield focused on providing mental health services and the role of clinical psychologists. (SLIDE 19-20 ADD TXT DEFS)
Mental Health Professionals
Individuals such as general practitioners, community mental health nurses, psychiatrists, and clinical psychologists who work in mental health care.(SLIDE 21 ADD TXT DEFS)
Multidisciplinary Teams (MDTs)
Teams composed of professionals from multiple disciplines collaborating to deliver mental health care.
Mental Health Act
Legislation governing involuntary detainment for safety in mental health contexts.
Involuntary Detainment
Detaining a person against their will under mental health law to protect safety.
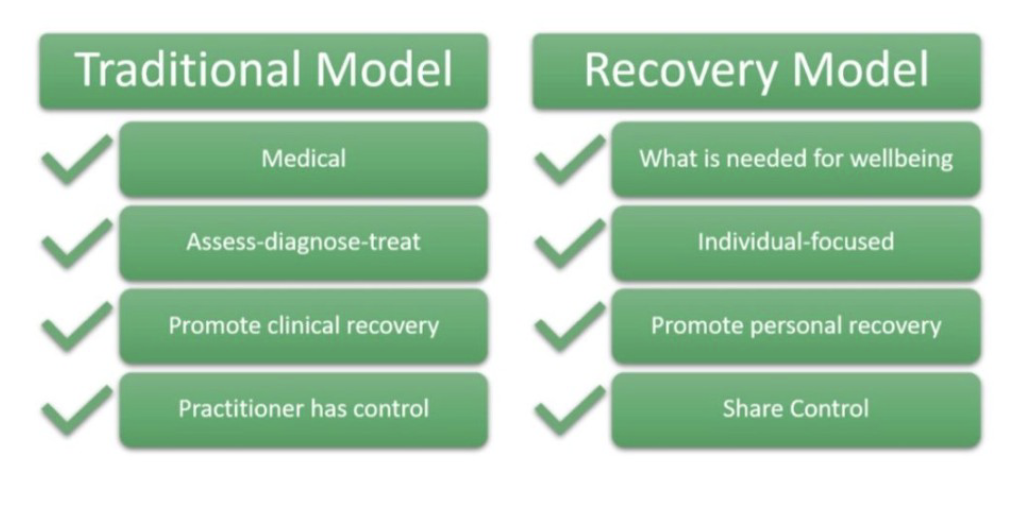
Recovery Model
An approach emphasizing an individual's journey toward wellbeing and self-determination, not just symptom remission.
Holistic model; hope, secure base, strong sense of self, etc.
Contrasts with diagnostic model
Traditional Medical Model
A model of care that emphasizes diagnosing and treating disorders, often with clinician-controlled care aimed at clinical recovery.
Traditional vs Recovery Model
Reflective Practitioner Approach
A stance of continuous self-reflection about practice, ethics, and how to better hear and respect clients.
Etiology
The study of the origins and development of mental health problems.
How are mental health problems developed and maintained?
Help us in developing interventions/preventative programs
Psychosis
A cluster of symptoms including disturbances in thought/language, sensory perception, and emotion regulation (e.g., hallucinations, delusions, withdrawal from day-to-day activities).
Schizophrenia
A heterogeneous psychotic disorder with variable symptoms influenced by biological, environmental stress factors (diathesis-stress perspective).
3 Factors of Psychosis/Schizophrenia
Biological, cognitive, developmental/social factors.
Biological Factors - Genetics
How do genetic studies explain schizophrenia?
Genes are studied to identify those linked to human disorders.
Genetic predisposition plays a role: schizophrenia can be inherited. Dependent on how closely they are related—or more specifically, how much genetic material the two share in common
Concordance studies
Research designed to investigate the probability with which family members or relatives will develop a psychological disorder depending on how much genetic material they have in common
Twin studies
Studies in which researchers compare the probability with which monozygotic and dizygotic twins both develop symptoms indicative of a psychopathology in order to assess genetic contributions to the psychopathology.
What do twin studies reveal about the genetic role in schizophrenia?
MZ (identical) twins share 100% of genes → concordance rate ~ 44%.
DZ (fraternal) twins share 50% of genes → concordance rate ~ 12%.
Shows a strong genetic influence, but rates below 100% prove environmental factors also play a role.
What are some caveats of twin studies on schizophrenia, and how are they addressed?
Concordance may be influenced by sex and social factors.
Studying offspring of twins helps clarify:
Offspring of MZ twins: 16.8% risk.
Offspring of DZ twins: 17.4% risk.
What role do brain neurotransmitters play in schizophrenia?
Neurotransmitters are chemicals that help neurons communicate with each other.
Involved in synaptic transmission.
Example: dopamine is linked to schizophrenia.
Dopamine
A brain neurotransmitter involved in movement, motivation, & reward. Impacts mood, attention, and learning.
Dopamine Hypothesis
A theory that argues that the symptoms of schizophrenia are related to excess activity of the neurotransmitter dopamine.
Antipsychotic drugs
They work by blocking dopamine receptors.
This helps reduce hallucinations, delusions, and other psychotic symptoms.
Phenothiazines
A group of antipsychotic drugs that help to alleviate the symptoms of psychosis by reducing dopamine activity.
Amphetamine psychosis
A syndrome in which high doses of amphetamines taken for a long time produce behavioural symptoms that closely resemble symptoms of psychosis.
Brain Neurotransmitters
Chemical messengers in the brain that enable neural communication (e.g., dopamine).
Cognitive Deficits in Schizophrenia
Core feature of schizophrenia.
Includes dysfunctions in working memory, attention, processing speed, visual & verbal learning.
Leads to poor reasoning, planning, abstract thinking, and problem‐solving.
Appear early in the prodromal phase and continue through illness.
Working memory decline = key precursor to relapse.
Working Memory Tests
Digit Span Task: recall increasingly long number sequences.
AX-CPT Task: respond to “X” only if it follows “A.”
People with schizophrenia perform worse than healthy controls.
Performance similar to bipolar patients with psychotic symptoms.
Reasoning Biases – Jumping to Conclusions (JTC)
Bias where decisions are made with too little evidence.
Demonstrated with the beads task: Jar A (85 red, 15 blue), Jar B (85 blue, 15 red).
People with schizophrenia often decide after 1–3 beads, showing stronger bias.
Contributes to delusional beliefs and psychotic thinking.
Factors Increasing JTC Bias
Cognitive impairments (esp. working memory deficits).
Anxiety, depression, worry → bias toward negative interpretations.
Anomalous experiences (e.g., hallucinations).
Social factors: trauma, isolation, urban stress.
These reinforce paranoia and delusions.
Cognitive Theories of Psychosis
Psychotic thinking comes from systematic cognitive biases, not random chaos.
Everyday reasoning processes become distorted.
Understanding these biases enables interventions to reduce paranoia and distress
False Belief Task / Sally-Anne Test
A test of theory of mind assessing the understanding that others can hold false beliefs.
Sociogenic hypothesis
The theory that individuals in low socio‐economic classes experience significantly more life stressors than individuals in higher socio‐economic classes.
Social-selection theory
The theory that individuals displaying psychotic symptoms will move into the lower socio‐economic classes as a result of their disorder.
Downward drift
A phenomenon in which individuals exhibiting psychotic symptoms fall to the bottom of the social ladder or even become homeless due to impairment.
Social Labelling
The theory that development and maintenance of psychotic symptoms are influenced by the diagnosis itself.
Theory of Mind
The ability to understand one’s own and other people’s mental states.
Sally-Anne False Belief Task
A method used to test whether a child has developed a ‘theory of mind’
Autism Spectrum Disorder (ASD) – Core Features
Developmental disorder marked by differences in:
Reciprocal social interaction
Communication
Flexibility of thought (difficulty in understanding the intentions and emotions of others)
Early symptoms: withdrawal, lack of communication, limited interests, difficulty learning new skills.
ASD
Appearing withdrawn
Failing to develop typical means of communication
Disinterest in surroundings
Difficulty in learning new skills
No sign of engaging or enjoying social interactions
A significant delay in development of spoken language
Lack of imagination
Empathizing-Systematizing Theory
A theory positing ASD differences in empathizing (emotional understanding) and systematizing (pattern-based thinking).
Genetic Factors in ASD
Strong familial link; higher sibling recurrence risk (2–14%).
Twin studies: MZ 60–91%, DZ 0–20%.
Heritability estimates: 64–91%.
Perinatal Factors
Birth-related factors such as prematurity and birth complications that may influence ASD risk.
Social Labelling
Stigma and negative consequences that occur when a person is labeled as mentally ill.
ASD Cognitive Factors
Executive function
Theory of mind
Empathizing-systematizing theory
Empathising–Systematising Theory
ASD linked to weak empathising but strong systematising; explains focused interests and resistance to change
Executive Functioning in ASD
Deficits in planning, problem-solving, and attentional control; impacts flexibility and social functioning.