Gestational Trophoblastic Disease
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Gestational Trophoblastic Disease
Molar Changes
3 types: Complete, Partial, or Coexistent
Complete Hydatidiform Mole
Most common neopasm that arises from the trophoblast
May develop into choriocarcinoma
Complete hydatidiform moles are masses that arise from either:
fertilization of a defective ovum by a single sperm
OR fertilization of one ovum by two sperm
Partial Hydatidiform Mole
Partial (Incomplete) Mole results from triploid karyotype (69 chromosomes) in about 90% of cases
Little malignant potential
Has focal and less advanced hydatidiform changes w/ slowly progressing swelling of avascular villi
some avascular villi are spared
hyperplasia of the trophoblast is focal
Potential findings of a partial hydatidiform mole includes:
abnormal fetus / fetal tissue
thick placenta
oligohydramnios
**there may be a co-existing fetus (non-viable), fetal parts or an amniotic sac
Coexistent Molar & Fetus
Rare
results from hydatidiform degeneration of twins
More likely w/ 2 placentas, coexisting fetus alive w/ normal placenta
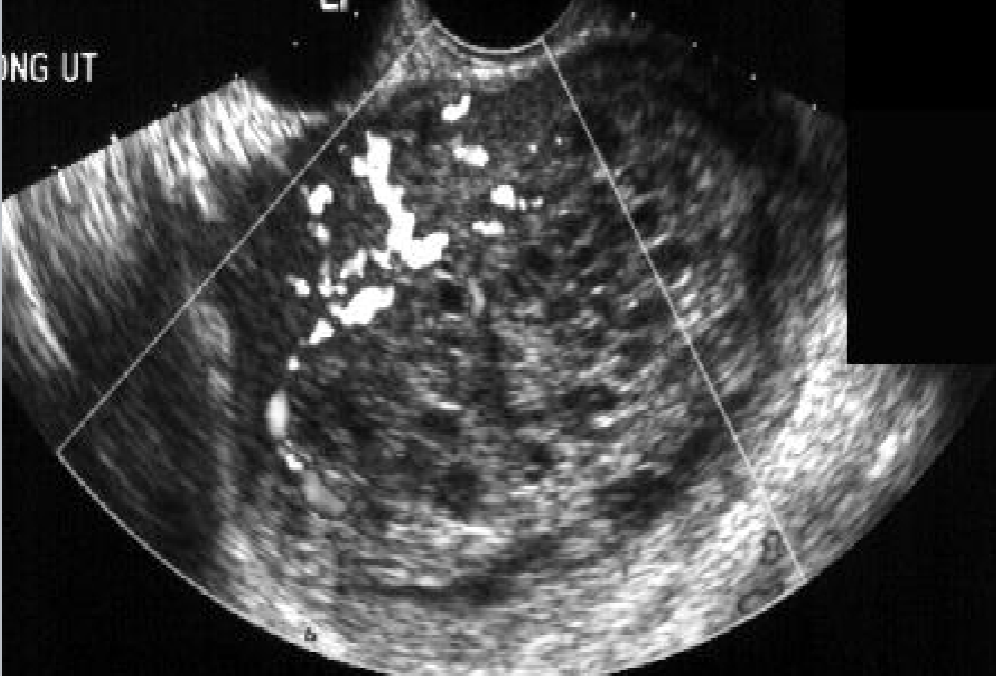
Hydatidiform Mole
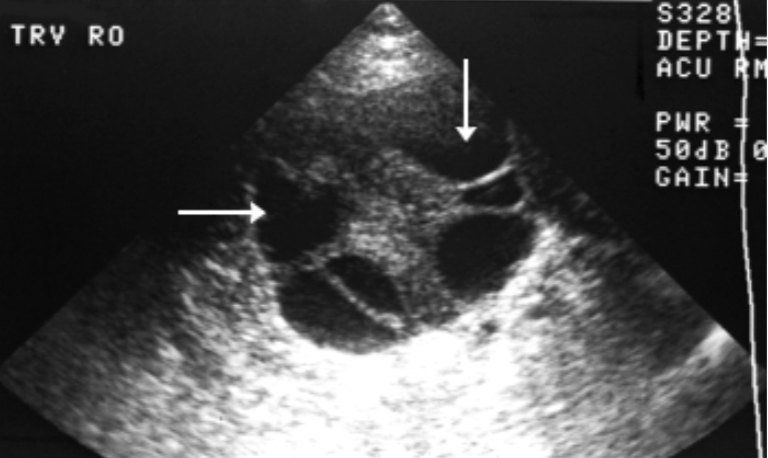
Ovarian theca lutein cysts are found in 20-35% of pt’s w/ hydatidiform moles
caused by overstimulation of ovarian tissue by large amounts of hCG secreted by the proliferating trophoblast
Theca Lutein Cysts
Bilateral
contain multiple cysts + septa
Largest when hCG production at greatest
12 - 24 weeks GA
Have potential to twist and hemorrhage, causing areas of solid echogenicity within cyst
Hydatidiform Mole Labs:
Elevated beta hCG levels
stay high or continuously rise beyond 100 days after LMP
(there is normally a decline)
Invasive Mole AKA:
Chorioadenoma Destruens
Invasive Mole
Malignant, non-metastatic trophoblastic disease
result from malignant progression of hydatidiform moles
Chorioadenoma Destruens
Excessive trophoblastic overgrowth and penetration by the trophoblastic elements, including whole villi, into the depths of the myometrium, sometimes penetrating the uterine wall and involving the peritoneum
Choriocarcinoma
most malignant form of GTD
malignant, metastatic gestational trophoblastic disease
lungs and vagina most common sites for mets
it is classified microscopically as sheets of highly malignant trophoblast of both cytotrophoblast and synctiotrophoblast elements, with no villous structures
What do choriocarcinomas arise from?
50% develop from a hydatidiform mole
50% evolve from a normal pregnancy, occur after AB, or post ectopic
What is the treatment for choriocarcinoma?
Pt is placed on Birth Control Pill for 1 year to prevent pregnancy
hCG is performed every 1-2 weeks after primary treatment until results of 3 consecutive tests are normal, then monthly for 6 months, and then every other month for 6 months
Regression should occur within 2-3 months
What is the treatment for choriocarcinoma?
Recurrence is suspected if the hCG level reaches a plateau and remains there for 3 weeks or increases over 2 weeks
Recurrent molar pregnancy confined to the pelvic region is treated with chemotherapy
Methotrexate
Actinomyocin D
Surgical intervention
hysterectomy