1. adapted from quizlet: ryanef123 MMCP 8 - Liver and Bleeding (Dr. Stephens)
1/166
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
167 Terms
Case 1
Pt presents for new patient exam. Pt reports that he was recently incarcerated and is looking to get his life back on track. Pt has not seen a primary care physician since his release.
PMH: Hepatitis C
PSH: Denies
FH: NC
Med: None
Social: Denies alcohol, tobacco, history of IV drug use
ROS: Intermittent dental pain
EOE:
Well nourished
No Facial Asymmetry
Extraocular movements intact, no jaundice
(-) Proptosis
No facial masses
Trachea midline
Neck is soft with normal range of motion
No Lymphadenopathy
IOE
Soft tissue exam: Erythema and diffuse edema of gingiva
Floor of mouth is soft and flat
Tongue is free of lesions or ulcerations- no leukoplakia
Uvula midline
Dentition:
#2,5,18 gross decay- non restorable
#30 MOD caries, #4 MO caries
No mobility or calculus noted on palpation/ inspection
Hepatitis → Liver function → INR/clotting factors
five functions of the liver
Metabolism
Detoxification
Conversion of nitrogenous substances to be excreted by the kidneys
Formation of blood clotting factors
Metabolism of bilirubin
Impairment of liver function causes abnormalities in (2)
- Synthesis of coagulation factors
- Drug metabolism
Is cirrhosis reversible or irreversible?
Irreversible
Cirrhosis is associated with
jaundice, ascites, portal hypertension and significant liver dysfunction
Inflammation of the liver is known as
hepatitis
T/F: Clinical manifestations of the five forms of viral hepatitis are quite similar:
Hepatitis virus types A (HAV), B (HBV), C (HCV), D or delta (HDV), and E (HEV)
True
Which types cause most cases of viral hepatitis in the United States (3)?
Hepatitis A, B, and C
How do you determine which hepatitis someone has?
Serologic assays
With hepatitis, immune responses may be the major effectors of
injury
t/f: Hepatitis may lead to cirrhosis
true
What is characterized as an asymptomatic fulminant disease?
hepatits
ID the hepatitis phase:
Nonspecific symptoms such as fatigue, nausea, poor appetite, and vague right upper quadrant pain
Typically lasts 3 to 10 days
Preicteric phase
What would you expect to see elevated in terms of liver labs (AST/ALT, Alb, Bilirubin, PT) for a pt with hepatitis?
Elevated aminotransferase and bilirubin
ID the hepatitis phase:
Dark urine
Jaundice
Fatigue and nausea worsen
Stool color lightens
Pruritus
Followed by post icteric phase
Icteric phase
What two conditions could be present with hepatitis?
Hepatomegaly and Splenomegaly
with hepatitis there may be elevated levels of what two things
elevated aminotransferases and bilirubin
fulminant
a disease or medical condition that develops suddenly, rapidly, and with great severity or intensity; for hepatitis may need liver transplant
which form of hepatitis can be a self-limited infection aka non-fulminant?
Hepatitis A, C (*rare)
which forms of hepatitis can become fulminant?
Hep B, D (more common than B at least)
ID the type of hepatitis:
Highly contagious
Incubation period that usually is 15 to 45 days in duration
IgM anti-HAV
Self-limited infection
Does not lead to chronic infection, chronic hepatitis or cirrhosis
Vaccine available
Hepatitis A
What is the spread of hepatitis A?
primarily fecal-oral route
What is the spread of hepatitis B?
Spread by the parenteral or intimate personal contact
Most common cause of acute hepatitis in US?
Hepatitis B
1/3 of adults with hepatitis B develop
jaundice
What is Anti-HBs antibody associated with?
Hepatitis B immunity
ID the type of hepatitis:
Incubation period of 30 to 150 days
Jaundice appears in one third adults
Important cause of fulminant hepatitis
Effective vaccine available
HBIG used in certain exposures
Hep B
What causes a poorer outcome for Hep B? (3)
- Advanced age
- Female sex
- Certain strains
T/F: Most patients with hepatitis B develop chronic hepatitis
False. Only 2 - 7%
What is the third or fourth most common cause of cirrhosis in the United States
Chronic Hepatitis B
What hepatitis is an important cause of liver cancer (56% worldwide)?
Chronic hepatitis B
Which hepatitis:
Chronic liver disease
Liver failure
Hepatocellular carcinoma
Increased risk of chronic kidney disease
incubation 15-120 days
Hepatitis C
How can you diagnosis Hepatitis C?
anti-HCV in serum
What is the spread of hepatitis C?
parenteral route
Which hepatitis is the most significant infectious condition of concern to dental health care professionals
hepatitis C
ID the hepatitis type:
High potential to become a chronic liver problem
No vaccine
Has become a curable disease with the use of antiviral agents (>95%)
Achieve sustained eradication of HCV
hepatitis C
More than 60 % of Hep C cases are attributable to injection use, ____-_____% from sexual exposure
15-20%
A major complication of hepatitis C is the development of (?) hepatitis?
chronic (but fulminant is rare)
Which hepatitis has become a curable disease with the use of antiviral agents (>95%)
hepatitis C
Achieve sustained eradication of HCV; Prevent progression to cirrhosis, hepatocellular carcinoma (HCC), and decompensated liver disease requiring liver transplantation -fulminant
Which hepatitis is linked to hepatitis B?
Hepatitis D
How is Hepatitis D spread?
Parenteral or sexual spread
What is the highest risk for Hepatitis D?
Chronic Hep B
How is Hepatitis D prevented?
Prevented by preventing hepatitis B (Hep D is a unique RNA virus that required HBV for replication)
What happens if you have a combo of hep B and D?
- More severe than hepatitis B alone
- More likely to lead to fulminant hepatitis and to cause severe chronic hepatitis --> Ultimately cirrhosis
Hepatitis E is endemic in (more/less) developed areas of the world?
less
Which hepatitis tends to be more severe than other forms of epidemic jaundice?
Hepatitis E → Fatality rate of 1% to 2% & particularly high rate of acute liver failure in pregnant women
T/F: There is no known means of prevention or treatment of hepatitis E
true
Icterus aka
jaundice
What is the diagnosis?
Accumulation of bilirubin in the plasma, epithelium, and urine
Degradation product of hemoglobin
Bilirubin tends to accumulate in the plasma as a consequence of decreased liver metabolism and transport
Jaundice/ Icterus
What is characterized by massive hepatocellular destruction and a mortality rate of approximately 80%.
Fulminant Hepatitis
lab findings of hepatitis
aminotransferases/transaminases (AST/ALT): liver enzymes that act as key markers of liver cell injury (hepatocellular injury), releasing into the bloodstream when liver cells are damaged. ALT is highly specific to the liver, while AST is also found in heart, muscle, and other tissues
alkaline phosphatases: enzyme ↑ = injury
total and direct bilirubin: Total bilirubin measures all bilirubin; direct ajka conjugated bilirubin measures water-soluble bilirubin processed by the liver. High direct levels suggest liver/bile issues, while high indirect suggests blood destruction
bilirubin: yellowish substance made during the body's normal process of breaking down old red blood cells. It travels to the liver, where it is converted into a soluble form (direct) and excreted into bile before leaving the body
albumin: a vital protein produced by the liver that constitutes about half of the plasma protein, essential for maintaining oncotic pressure to keep fluid within blood vessels, transporting hormones, drugs, and nutrients throughout the body. Low levels often indicate kidney/liver disease or malnutrition, while high levels usually indicate dehydration
prothrombin time: how long blood to clot
In a pt with hepatits, would you expect prothrombin time (PT) to be increased or decreased?
Increased prothrombin time (PT)
In a pt with hepatitis, would you expect albumin levels to be increased or decreased?
Decreased
What are the most sensitive markers of acute hepatocellular injury?
Aminotransferases/ transaminases (AST / ALT)
T/F a patient who has a higher elevation in their ALT or AST has a more severe liver disease than someone who has a slightly elevated ALT / AST
False.
(Hepatocyte necrosis is NOT required for the release of aminotransferases; The degree of elevation of the aminotransferases does not correlate with the extent of liver injury)
Hepatobiliary disease leads to increased serum _______ levels through induced synthesis of the enzyme and leakage into the serum, a process mediated by ________
Alkaline phosphatase; Mediated by bile acids
Excessive alcohol consumption causes alcoholic liver disease and ultimately __________
Cirrhosis
Prolonged abuse of alcohol contributes to what three things?
- Malnutrition (folic acid deficiency)
- Anemias
- Decreased immune function
which form of alcoholic liver disease (fatty liver, alcoholic hepatitis, cirrhosis)
Fatty liver (aka hepatic steatosis)
Is fatty liver reversible or irreversible?
Completely reversible!
which form of alcoholic liver disease (fatty liver, alcoholic hepatitis, cirrhosis)
alcoholic hepatitis
Is alcoholic hepatitis reversible or irreversible, can it lead to necrosis?
May be irreversible and can lead to necrosis
which form of alcoholic liver disease (fatty liver, alcoholic hepatitis, cirrhosis)
which stage of alcoholic liver disease may be skipped?
alcoholic hepatitis
T/F: There are many conditions that can be related to alcoholic liver disease
True (see image for all!) *esophageal varices → portal vein

No dental treatment other than urgent care (absolutely necessary work) should be rendered for a patient with (BLANK) hepatitis unless the patient has attained clinical and biochemical recovery:
Isolated operatory
Aerosols should be minimized
Avoid drugs that are metabolized in the liver
Preoperative prothrombin time and bleeding time
Active (acute)
to do work you need clinical and biochemical recovery
T/F: Standard precautions during the care of all dental patients (assume everyone has hepatitis)
True
- Hep B carrier aka HBsAg positive or history of Hep C = standard precautions!!
In terms of dental management, what are the two ways we can determine current status and future risks in patients with hepatitis?
- Physician consultation
- Laboratory screening of liver function
meds metabolize in
liver
T/F: Chronic active hepatitis or impaired liver function may require changes in drug dose (Discuss with patient physician)
true
T/F certain analgesics should only be limited in persons who have end-stage liver disease
true
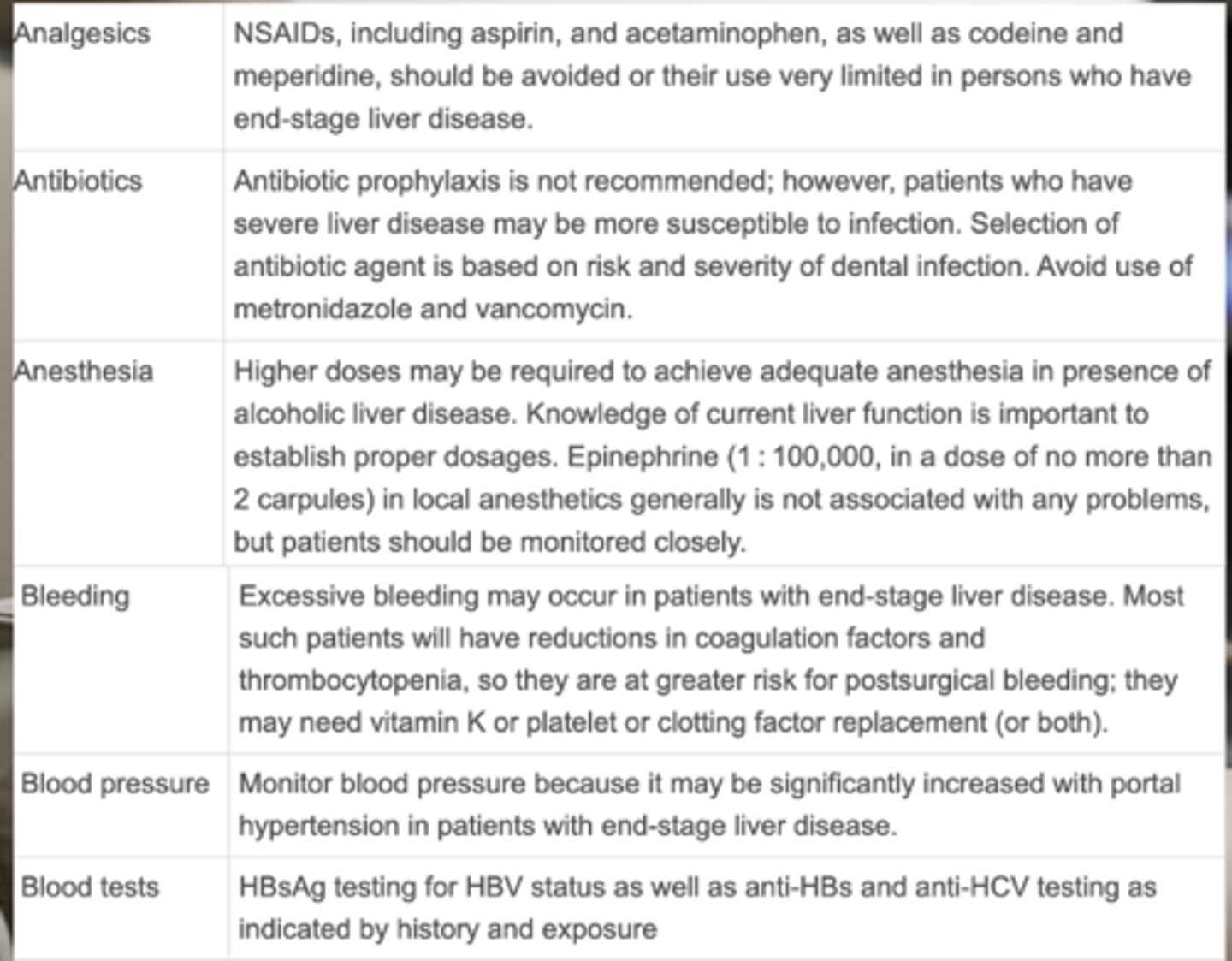
What NSAIDs should be avoided/very limited in patients with end-stage liver disease? (4)
- Aspirin
- Acetaminophen
- Codeine
- Meperidine
Is antibiotic prophylaxis recommended in patients with liver disease?
No (some patients with severe liver disease may be more susceptible)
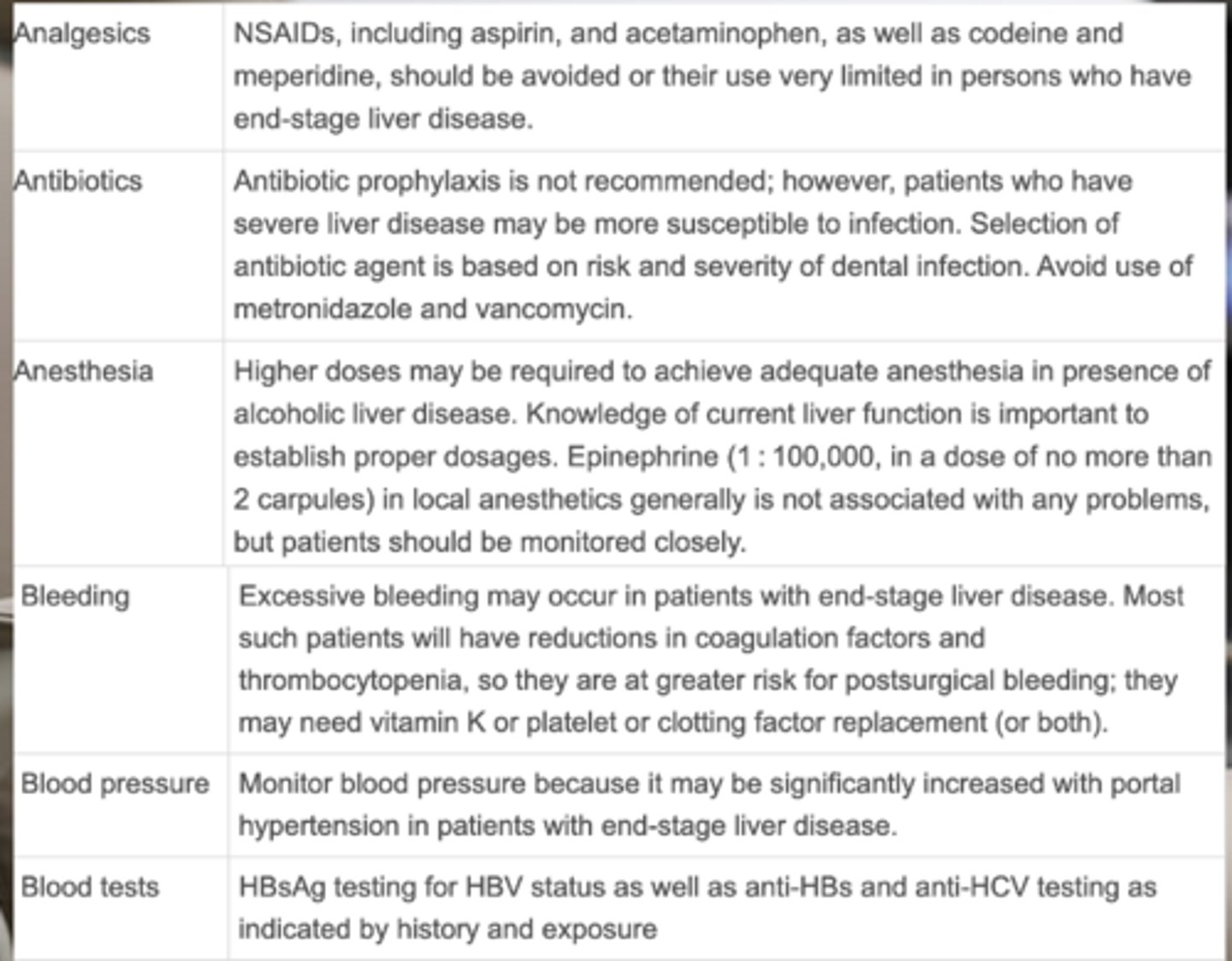
Which antibiotics should we AVOID in a patient with liver disease?
- Metronidazole
- Vancomycin
To achieve adequate anesthesia in patients with liver disease, what may be required?
higher doses
What is the recommendation for local anesthetic that is generally not associated with any problems?
1:100,000 epi, no more than 2 carpules
Which of the following is FALSE regarding considerations of bleeding for a patient with end-stage liver disease
a. Excessive bleeding may occur
b. Most patients will have decrease in coagulation factors & Thrombocytopenia
d. Lower risk for postsurgical bleeding
e. May need vitamin K or platelet or clotting factor replacement (or both)
D - GREATER risk for post surgical bleeding
Patients with end-stage liver disease may have increased blood pressure due to what?
portal hypertension
What 3 blood tests may be performed depending on history and exposure of liver disease?
- HBsAg
- Anti-HBs
- Anti-HCV
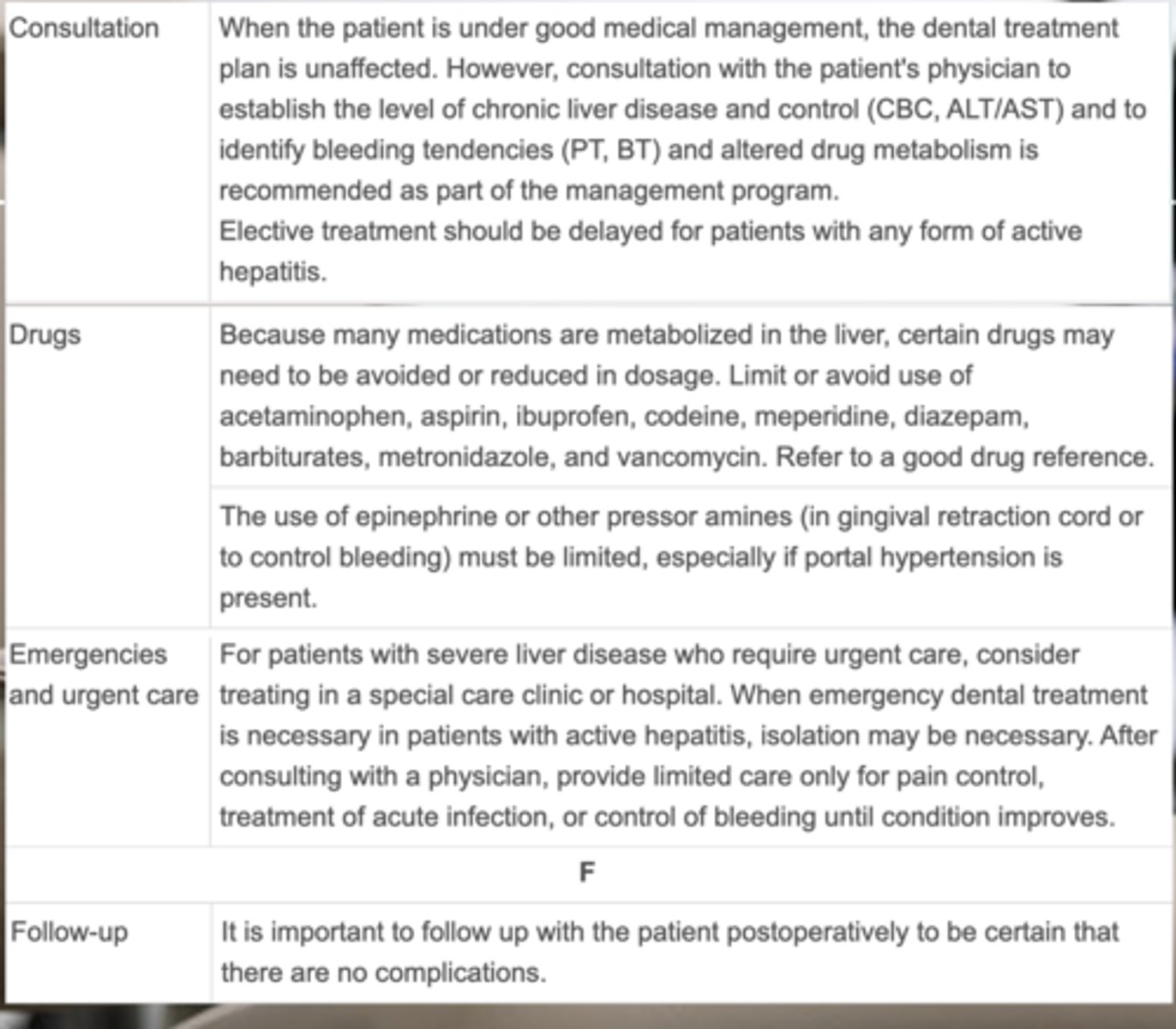
Consultations with a patient's physician for a patient with liver disease should establish (3)
- Level of chronic liver disease and control (CBC, ALT/AST)
- Identify bleeding tendencies (PT, BT)
- Altered drug metabolism
t/f: It is safe to provide elective treatment for patients with any form of active hepatitis.
FALSE - delay elective tx, urgent tx ONLY
Considerations of drugs for a patient with liver disease
- Drugs that are metabolized in the liver may need to be avoided or reduced in dosage.
- The use of epinephrine must be limited, especially if portal hypertension is present.
Drugs metabolized where should be avoided in patients with liver disease?
liver
All of the following MUST be limited or avoided in patients with liver disease. Why?:
acetaminophen
aspirin
ibuprofen
diazepam
barbiturates
metronidazole
vancomycin
they are metabolized in the liver
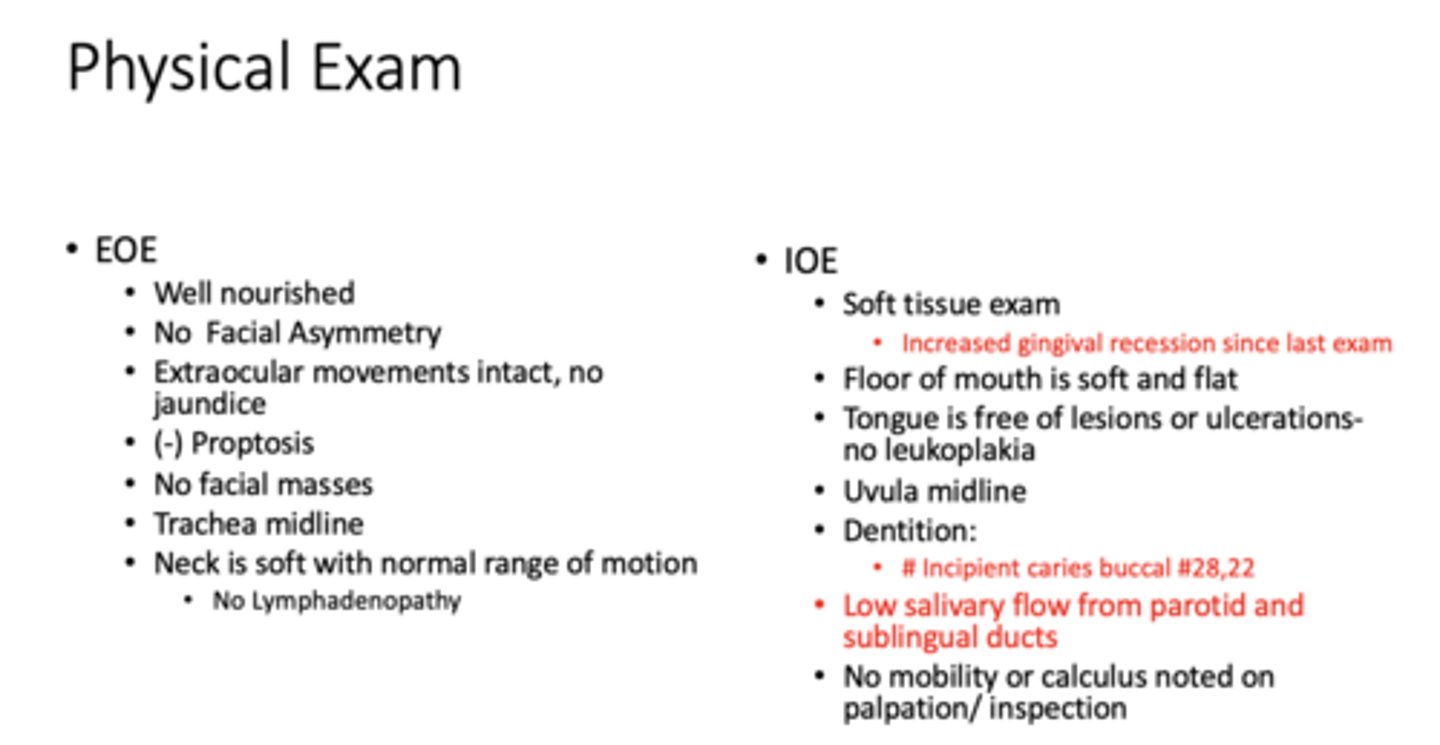
Clinical case 2:
55 year old presents continuing care. She was previously seen by another associate in your practice who has moved on to a DSO. Pt reports that she has noticed slight gingival recession since her last visit and generally feels that her previously excellent oral health is deteriorating. Pt reports that she has never had dental decay or any intervention besides routine prophy.
PMH: Depression, Von Willebrand disease
PSH: Denies
FH: NC
Med: Paxil (x 6 months) - antidepressant
Social: Denies alcohol, tobacco, rec drugs
ROS: Recent dry mouth
IOE:
Soft tissue exam: Increased gingival recession since last exam
Dentition: Incipient caries buccal #28,22
Low salivary flow from parotid and sublingual ducts (from med)
No mobility or calculus noted on palpation/ inspection
- Dry mouth
- Recession
- Caries
- Bleeding
NO NSAIDs
Bleeding is a significant feature of what condition?
advanced liver disease
Which clotting factors are vitamin K dependent?
prothrombin group II, VII, IX, X
Cirrhosis decreases liver storage and capacity for conversion of vitamin (?)
K, affecting clotting factors
T/F: Leukopenia (or leukocytosis) and anemia is often present with advanced liver disease
true
Deficiencies in clotting factors lead to elevations in (2)
- Prothrombin time
- Partial thromboplastin time
What is more common, congenital or acquired coagulopathies?
Acquired
ID the condition:
- Genetically transmitted defects in coagulation factors, platelets, or blood vessels
- Can present risk for significant bleeding
congenital coagulopathies
what are some acquired bleeding disorders?
von Willebrand disease
hemophilia A
hemophilia B
platelet function disorders - Bernard-Soulier syndrome, Glanzmann Thrombasthenia
What is the most common inherited bleeding disorder and caused by an inherited defect involving platelet adhesion?
Von Willebrand Disease (acquired bleeding disorder)
What causes Von Willebrand Disease?
Deficiency or a qualitative defect in vWF, needed to carry (bind) factor VIII and to allow platelets to adhere to surfaces
Most common form of Von Willebrand Disease
Type 1 is the most common - 70-80%
(mild/severe) Signs of Von Willebrand Disease
- History of cutaneous and mucosal bleeding
Mild
(mild/severe) Signs of Von Willebrand Disease:
VIII levels are low
Hemarthrosis and dissecting intramuscular hematomas
GI bleeding
Epistaxis - nosebleed
Menorrhagia
Severe
Lab findings for Von Willebrand Disease: aPTT (prolonged/normal/reduced)
Prolonged
Lab findings for Von Willebrand Disease: platelet count?
Slightly reduced, normal