New Material - Arterial Bypass Grafts, EVAR, Hemodialysis AV Fistulas, Transcranial Doppler (TCD)
1/140
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
141 Terms
Arterial Bypass Graft
Redirects flow around occluded artery via a synthetic graft or vein
Role of Sono. in Graft Mapping & Post-Graft Surveillance
Pre-surgical planning
Patency after surgery
Prevent failure
Monitoring
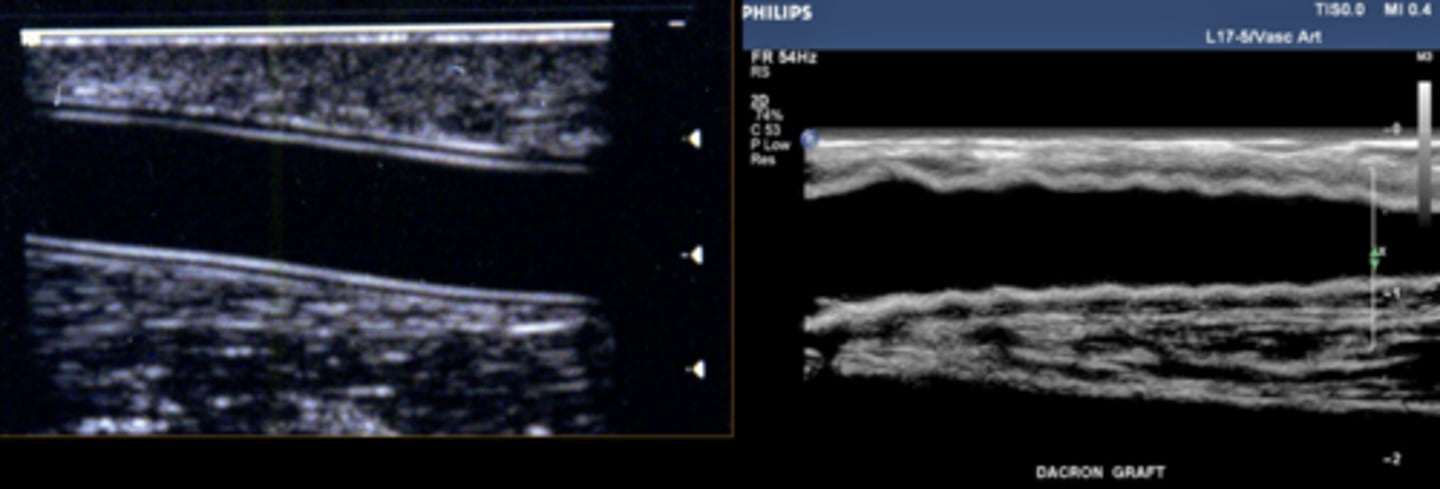
Synthetic Bypass Graft
Made of PTFE (polytetrafluoroethylene) or Dacron
Lower rates of early failure
Worse long term patency
Readily available with many sizes
Higher thrombogenicity
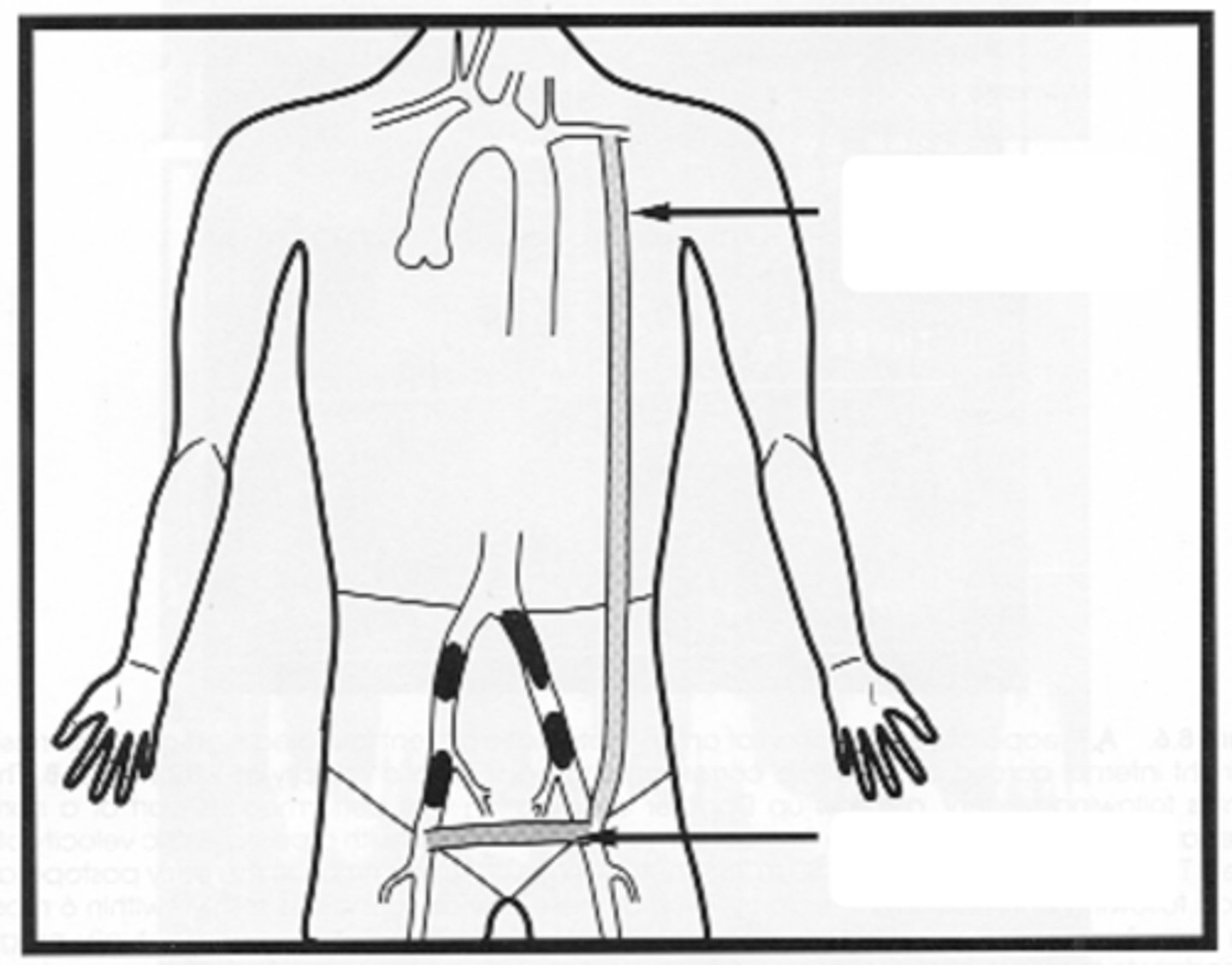
Axilla-Femoral Graft with Femoral-Femoral Bypass
Longest graft type
Femoral-femoral bypass supplies opposite leg
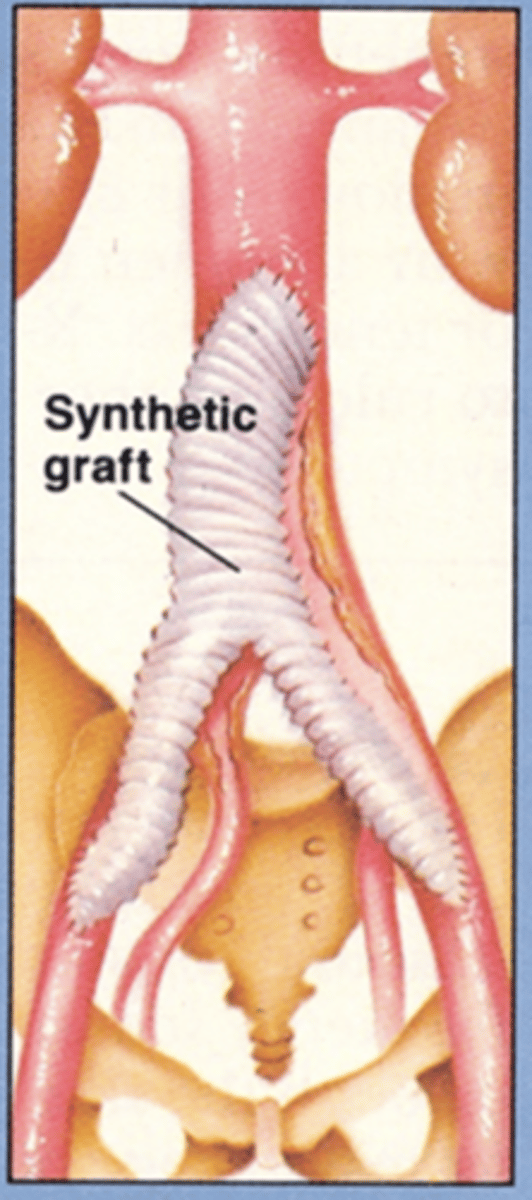
Aorto-Iliac Graft
Scars in abdomen & each groin
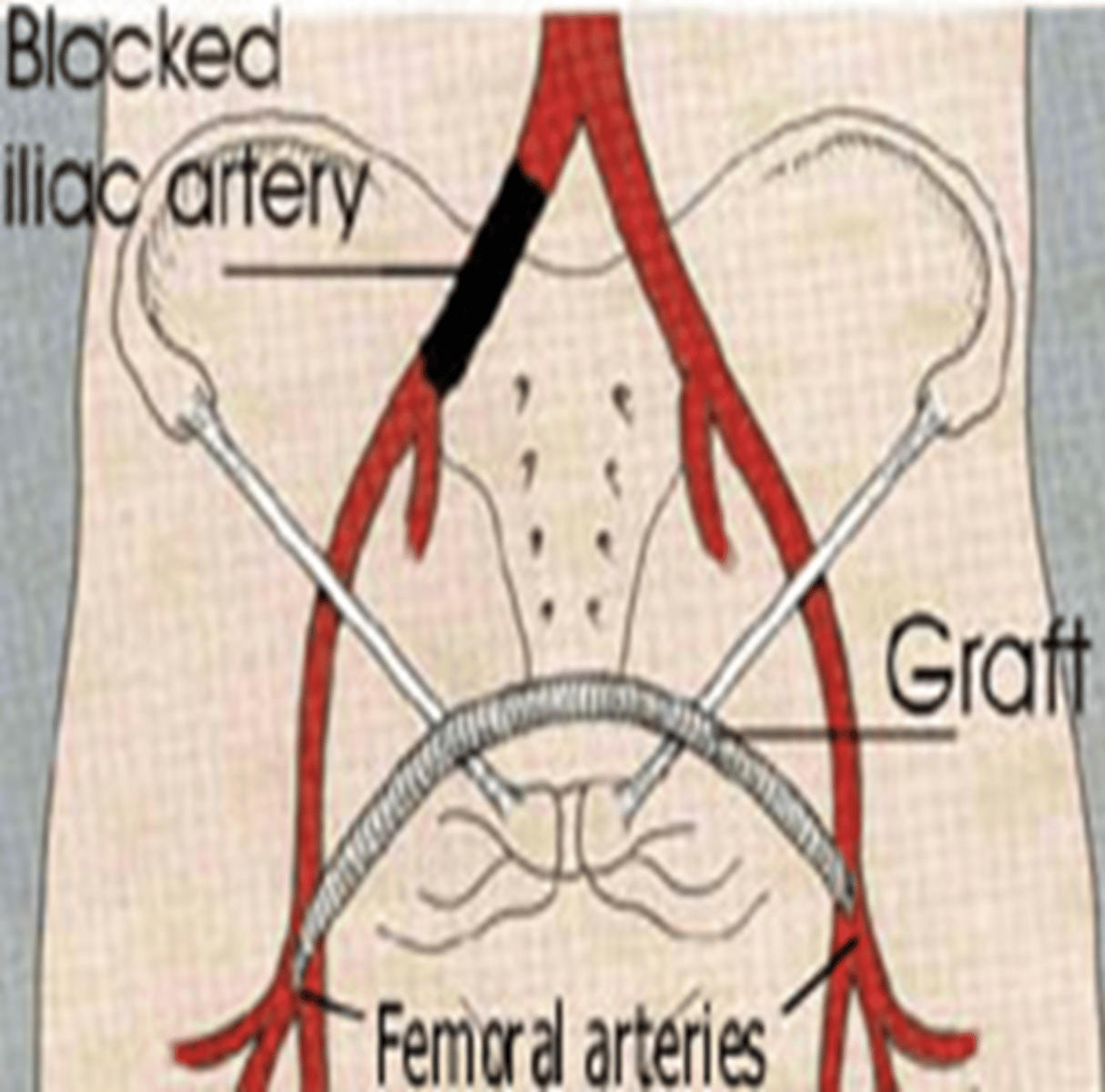
Femoral-Femoral Graft
Bypasses single iliac artery
Scar in each groin
Autogenous Vein Graft
GSV, SSV, cephalic, or basilic veins used
Higher rates of early failure
Better long term patency
In-Situ Vein Graft
Uses GSV in its native position
Venous valves removed to allow downward bloodflow
Perforators & tributaries removed
Larger proximal end connected to inflow artery
Smaller distal end connected to outflow artery
Preferred when vein diameter matches artery size at anastomosis
Reversed Vein Graft
GSV is removed & reversed -> smaller end connected to inflow, larger end connected to outflow
Perforators & tributaries removed
Venous valves do not need to be removed
Most Common Proximal Anastomosis
CFA or SFA
Distal Anastomosis
Placed below the lowest level of disease
Early Graft Failure
Within 30 days
25% of all graft failures
Technical defects - retained valve or anastomotic site issues
Compression/twisting of graft
Hypercoagulability
Thrombosis
Intermediate Graft Failure
Within 30 days to 2 years
75% of revisions are during this period
Due to myointimal hyperplasia - causes stenosis, typically at valve site
Leads to increased peak velocities at areas of stenosis
Late Graft Failure
> 2 years
Progression of atherosclerotic disease in native vessels
Changes in spectral waveform - increase rise time & decrease peak velocities
Aneurysms
Symptoms of Graft Failure
Return of pre-surgical claudication
Rest pain
Ulcers
Absent pulses
ABI < 0.15
Pre & Post-Op Graft Mapping/Surveillance Protocol
Grayscale, PSV (with angle correct), and Color of:
Inflow artery
Proximal anastomosis
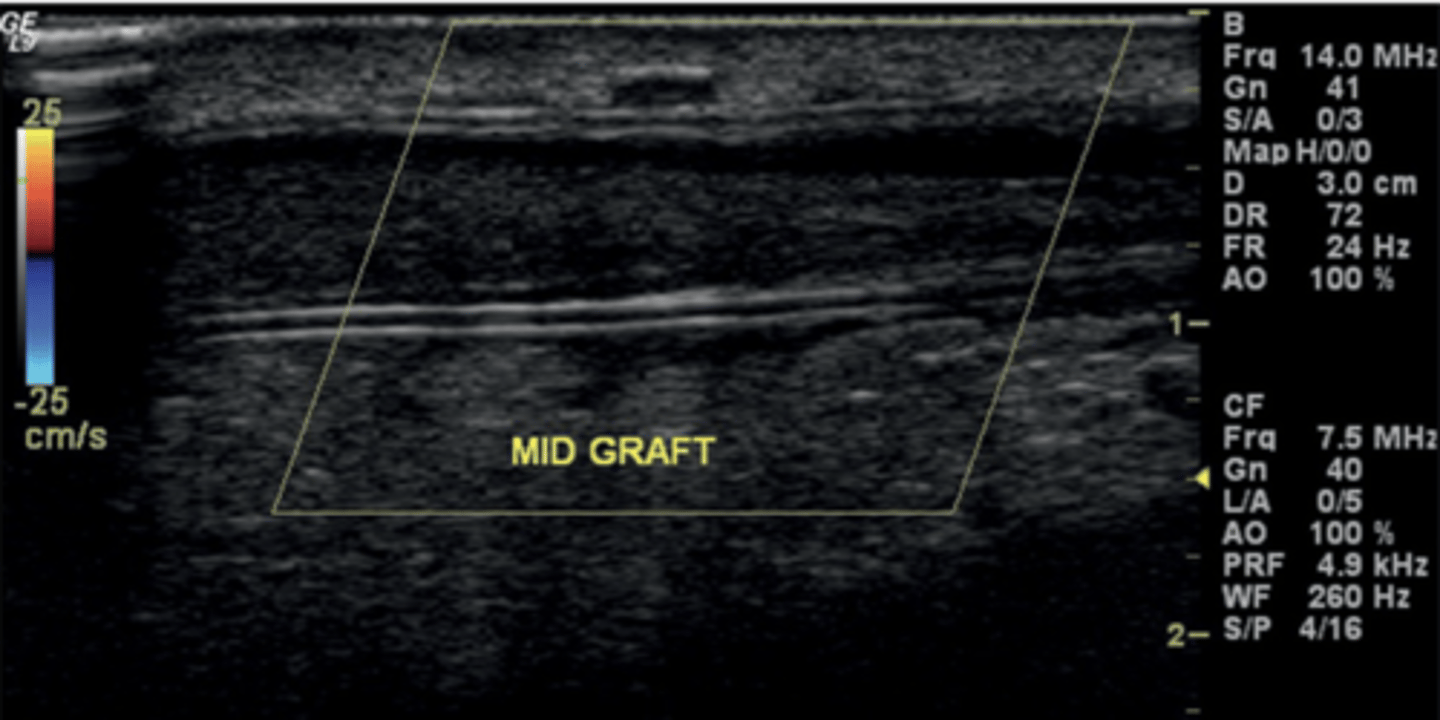
Mid-graft
Distal anastomosis
Outflow artery
Normal Graft Diameter
Minimum for any bypass = 2 mm
Preferred = 2.5-3 mm
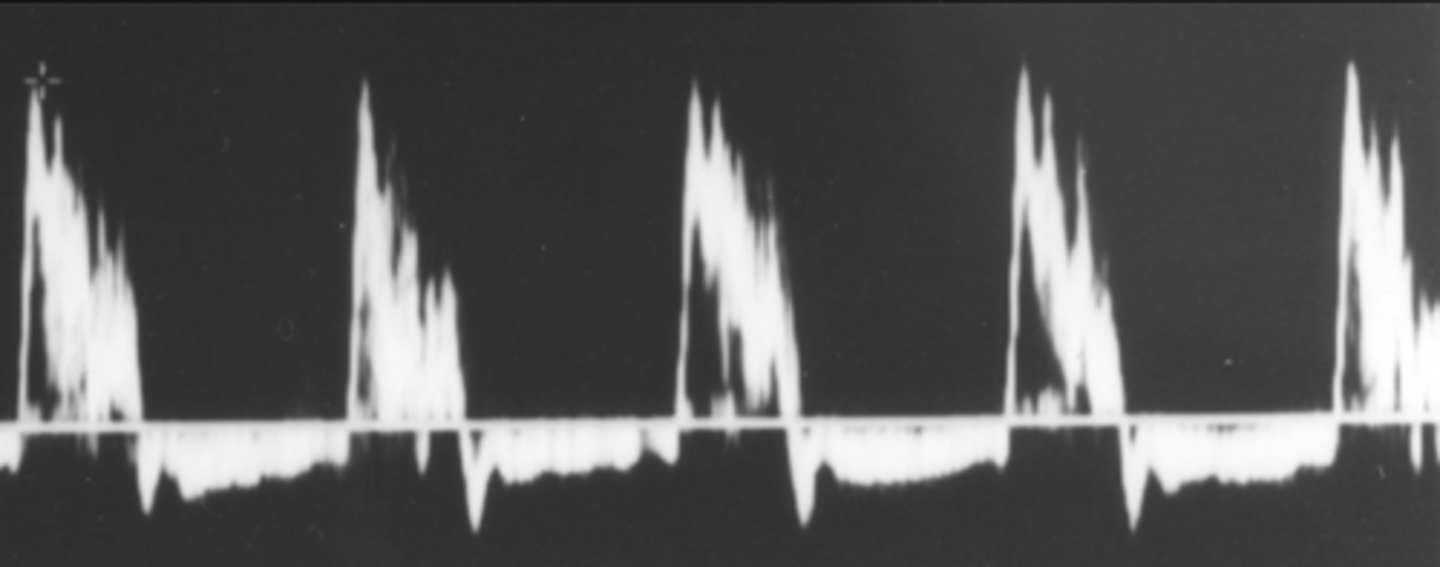
Normal Graft Spectral Appearance
Multiphasic arterial waveform
Sharp upstroke
Narrow systolic peak
Reversal of flow may not be seen early post-op
Normal Graft Velocity Ratio
< 2
Normal GFV Velocity
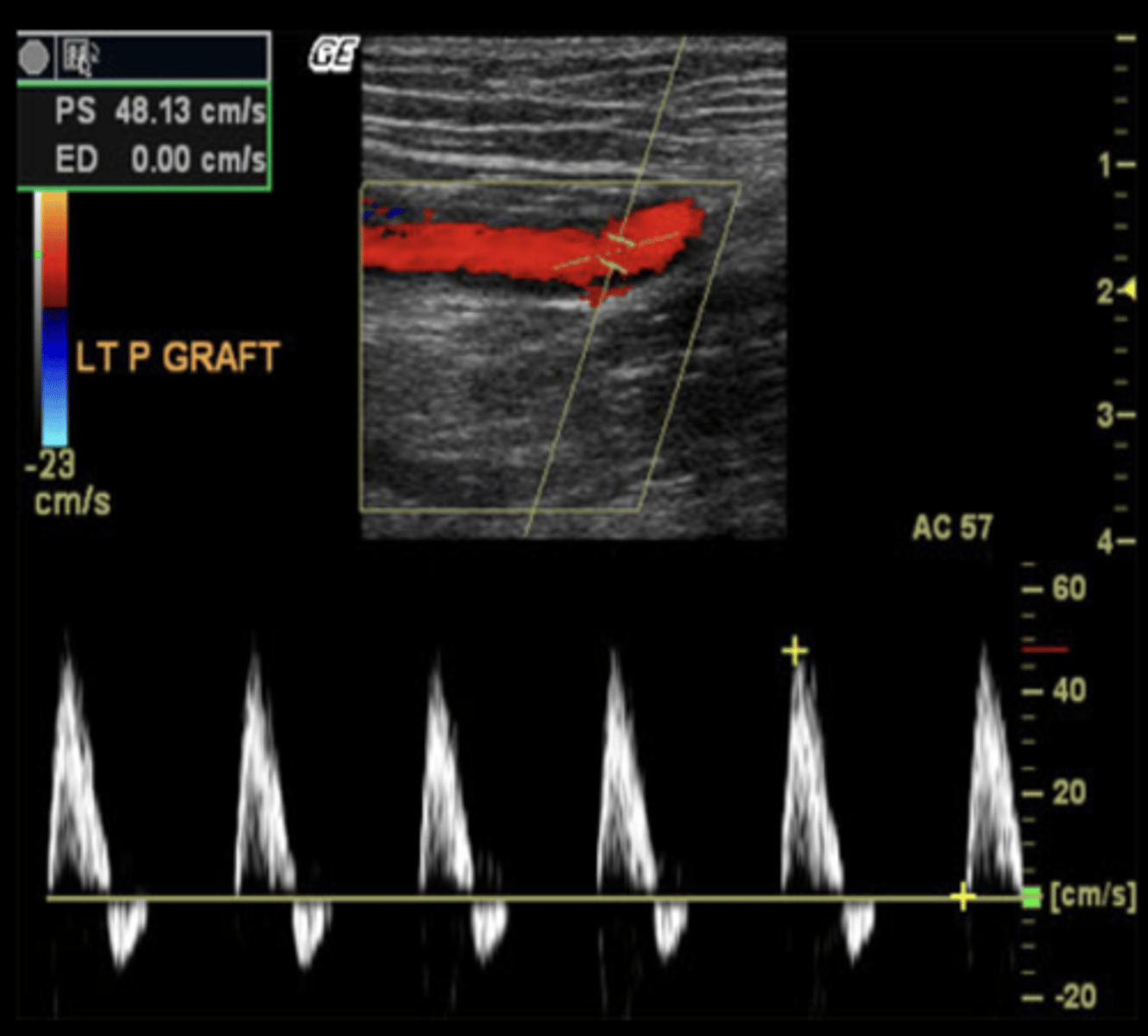
> 45 cm/sec
GFV Graft Failure Velocity
< 30 cm/sec
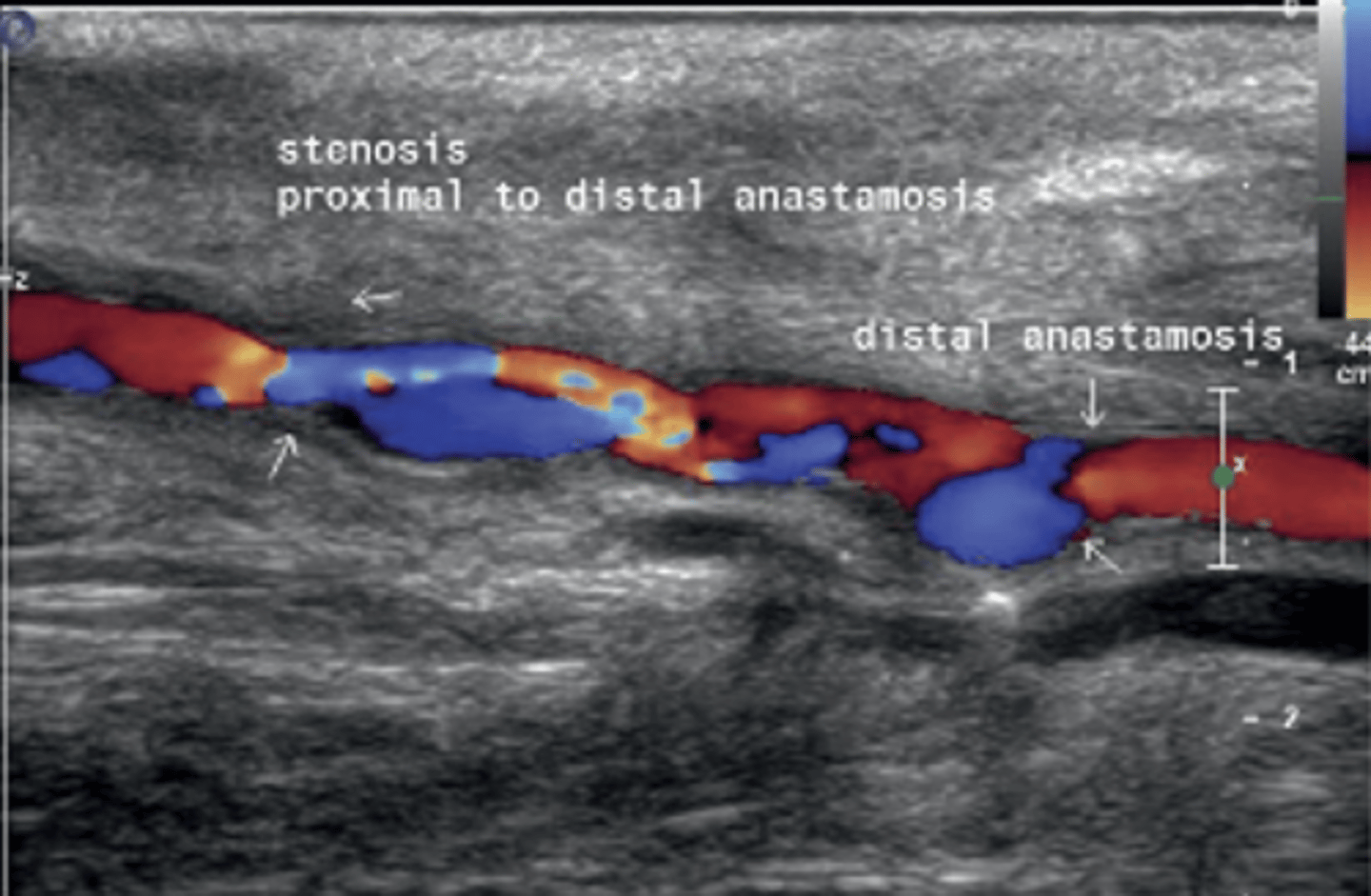
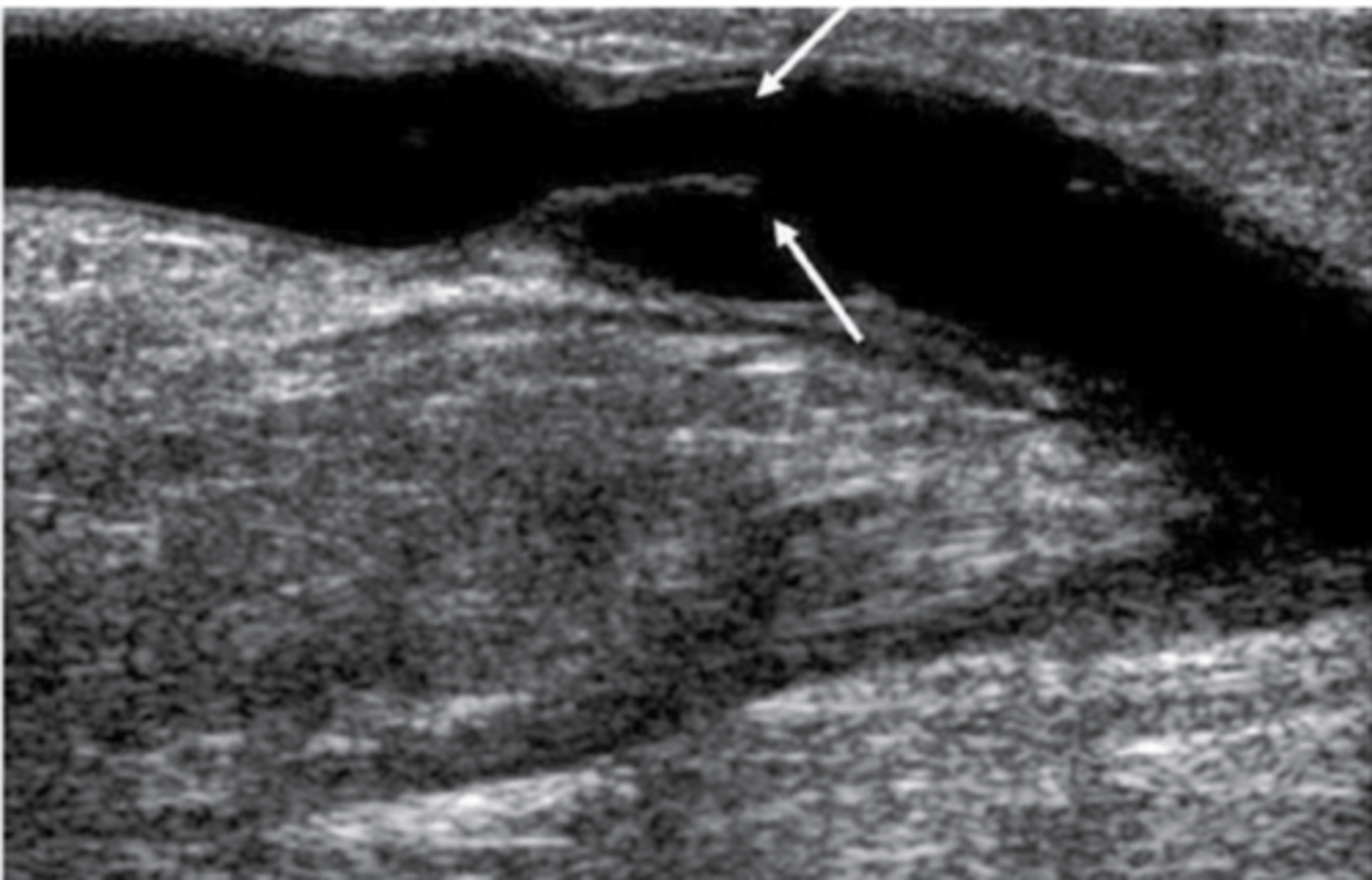
Graft Stenosis
Continuous diastolic flow with loss of diastolic reversal
Peak velocity > 180 cm/sec or < 45 cm/sec
Stenotic profile
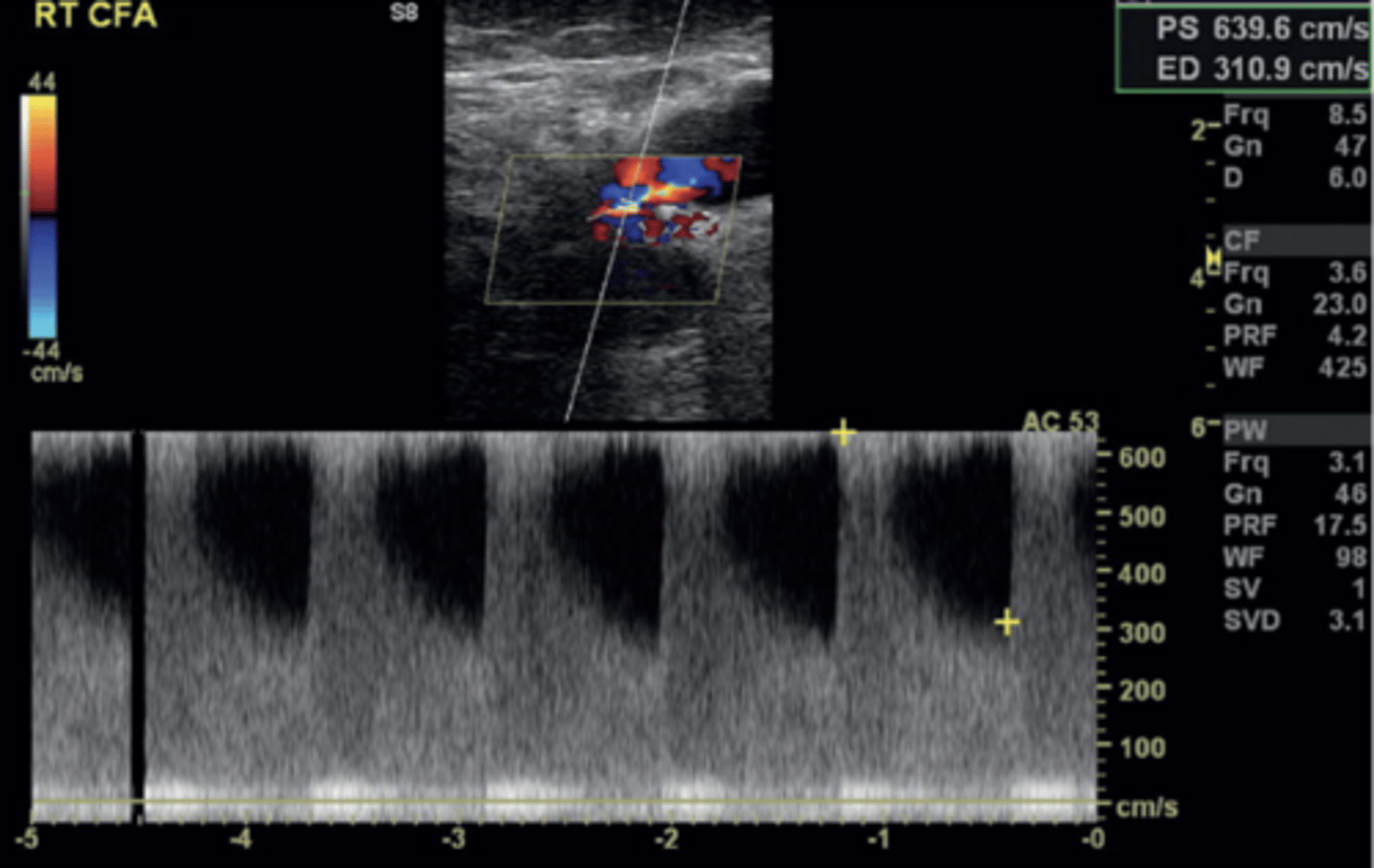
50% Graft Stenosis
PSV > 180 cm/sec
PSV ratio of 2
75% Graft Stenosis
PSV > 300 cm/sec
PSV ratio of 3.5
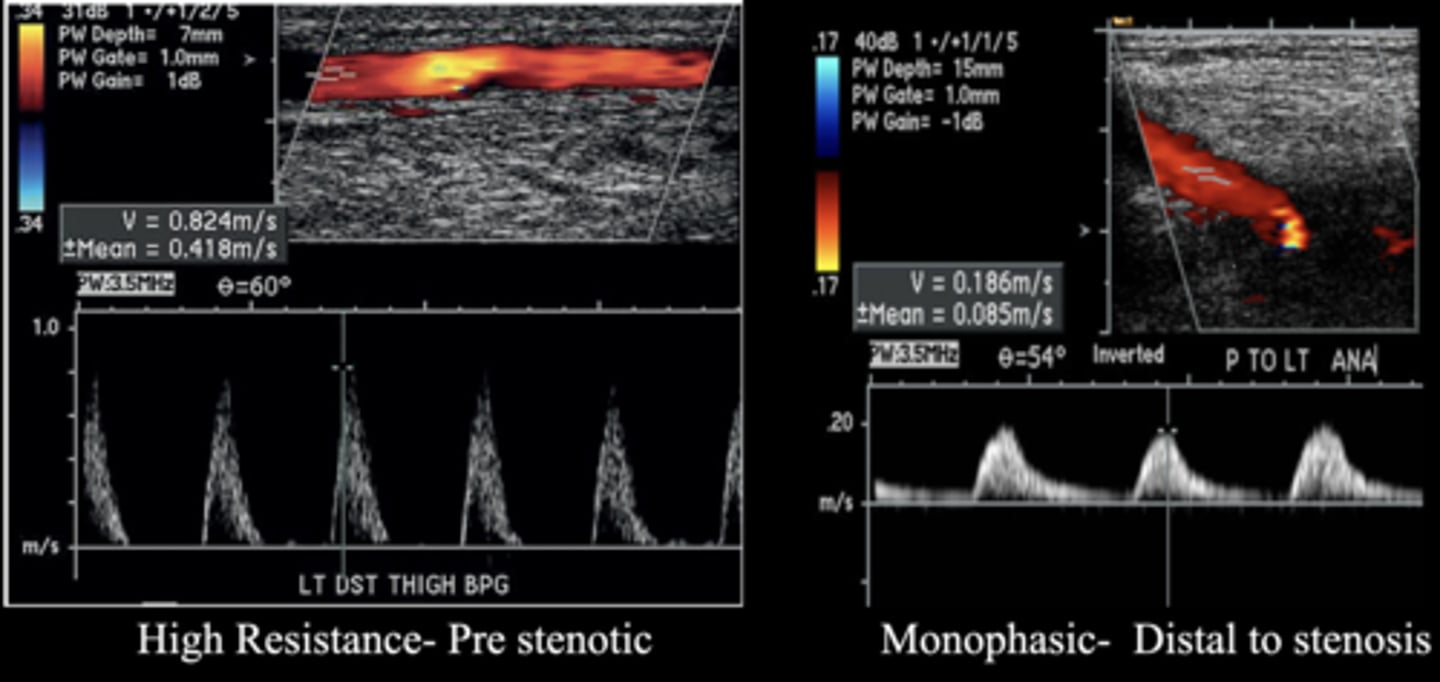
Walk Through Technique
Drag PW cursor through entire stenotic area
Record pre-stenotic, stenotic, post-stenotic, and distal to stenosis zones
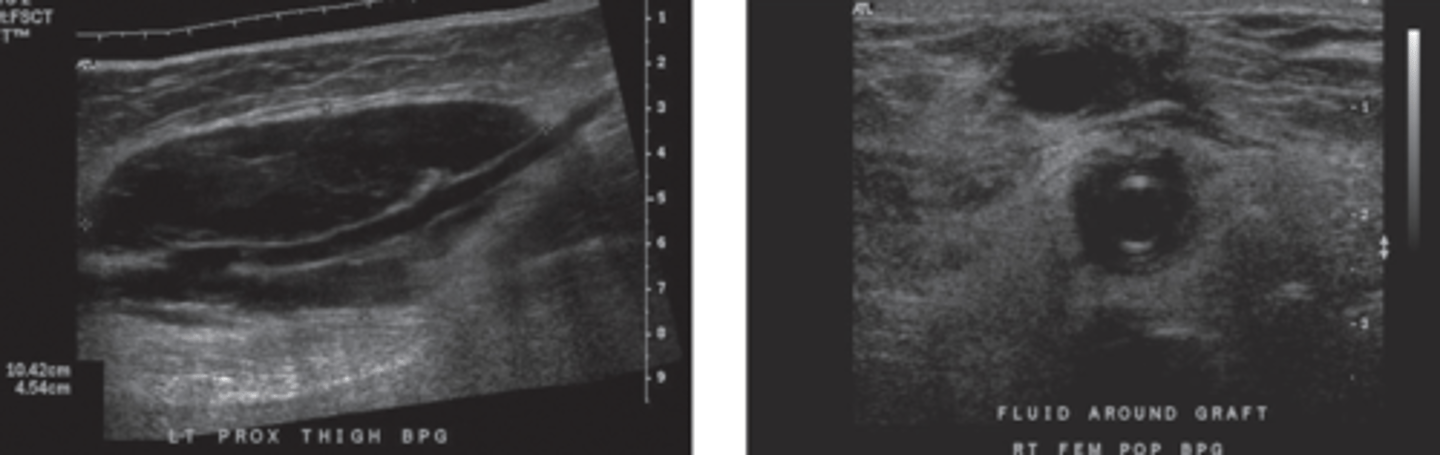
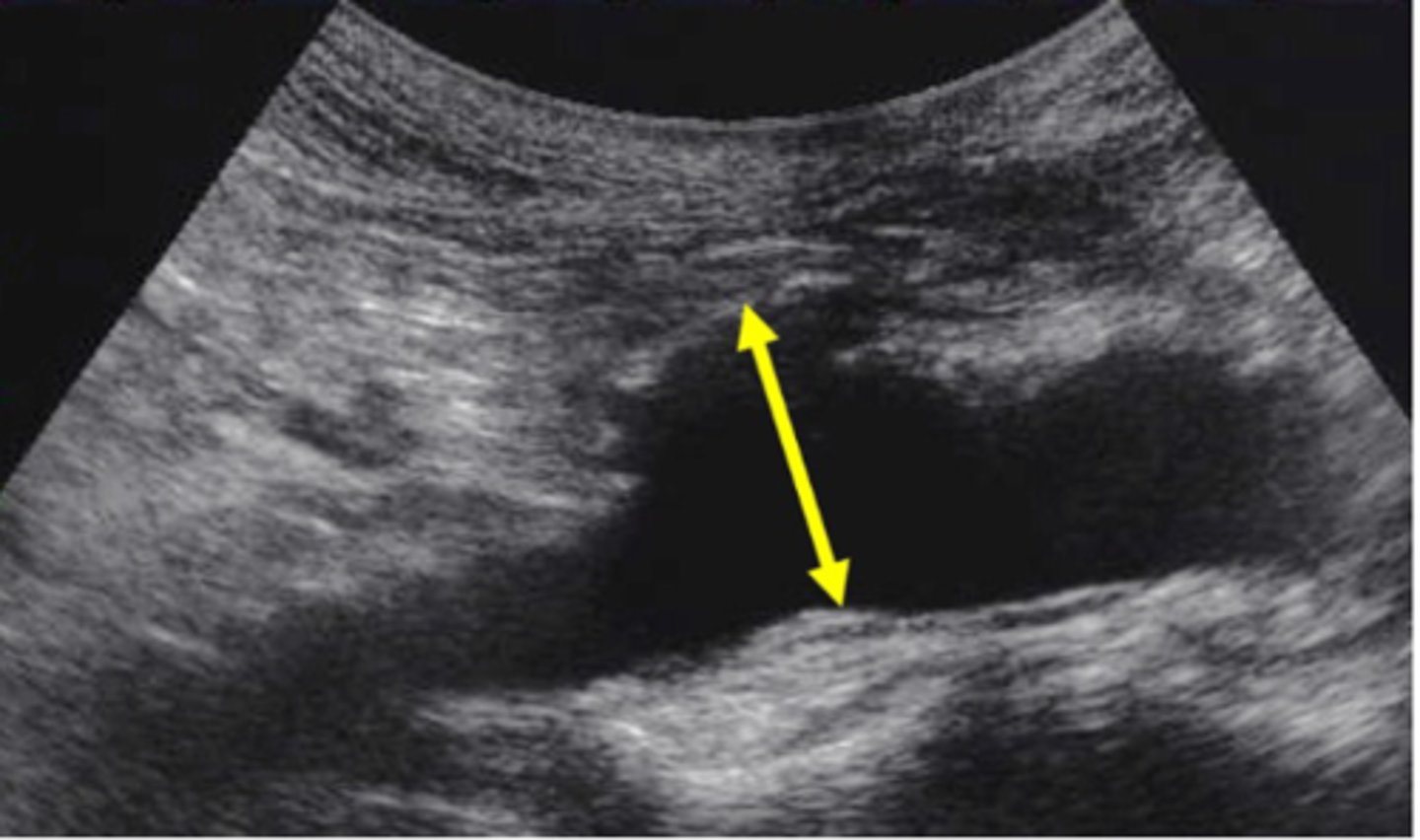
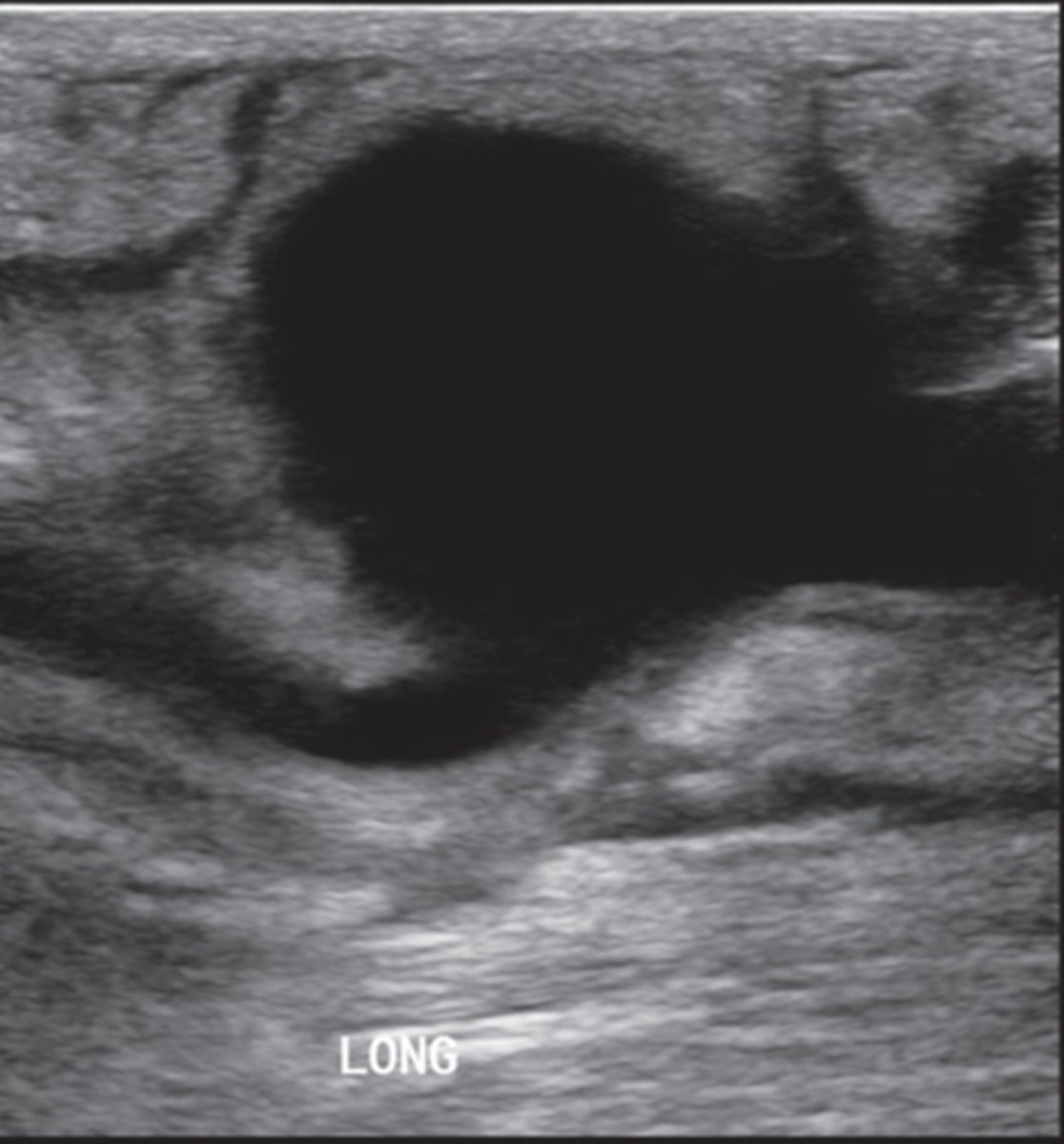
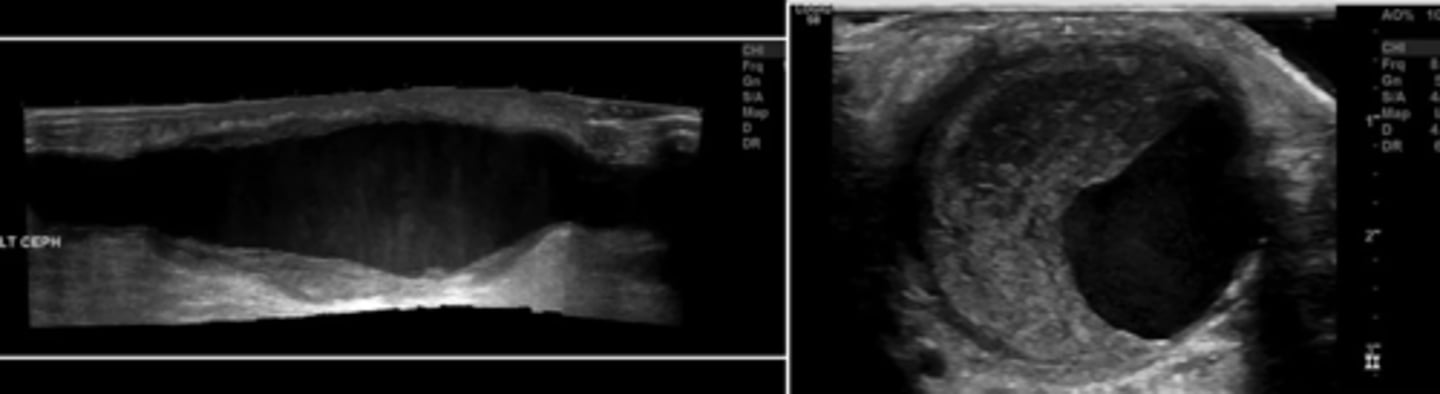
Peri Graft Fluid Collection
Fluid collections around graft
May be hematoma
Can compress graft & impact function
Can be infection
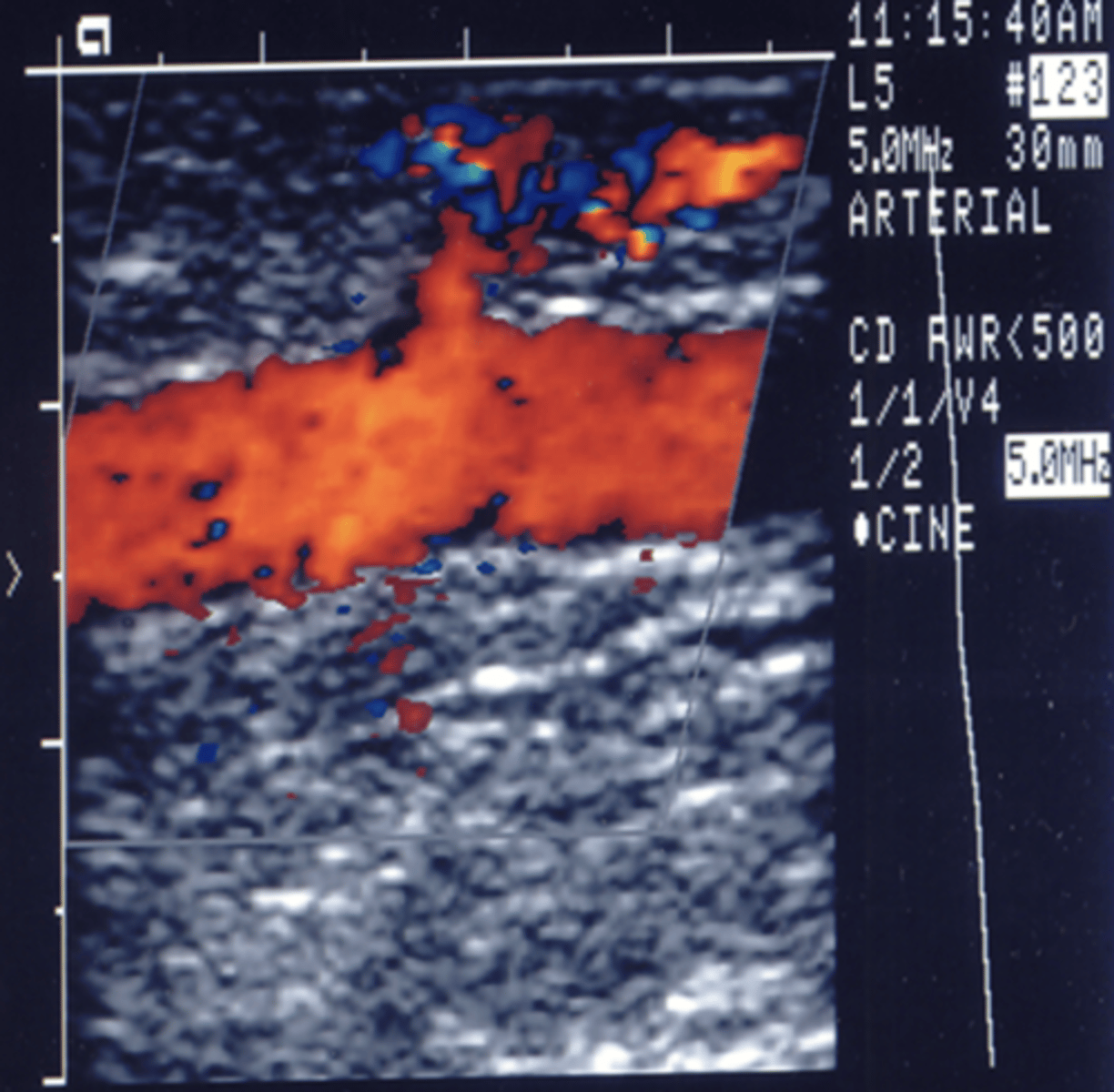
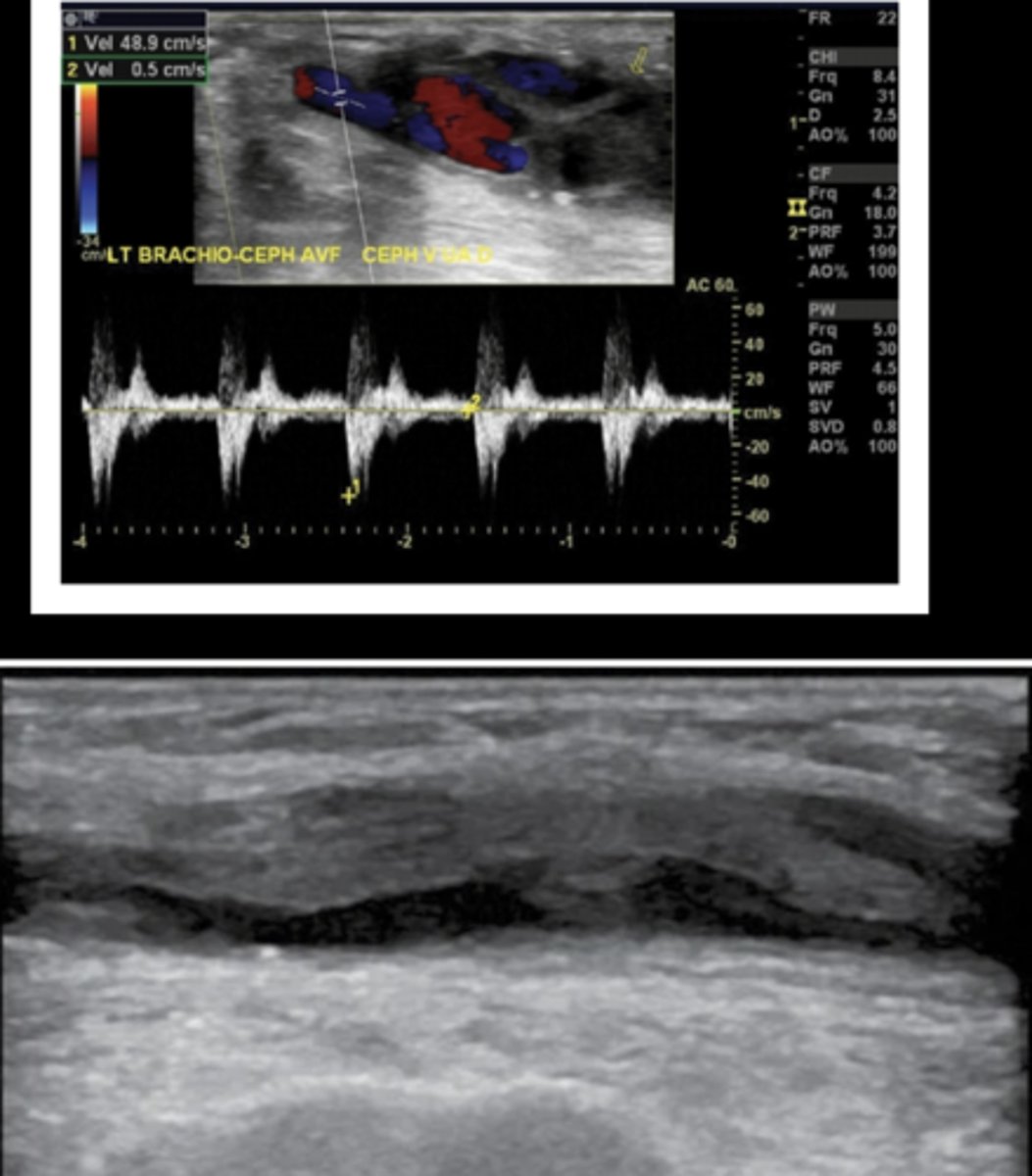
Fistula
Patent venous tributary that may communicate with deep venous system
Color flow is turbulent with aliasing
Spectral may be pulsatile or continuous
Proximal antegrade diastolic flow evident in graft
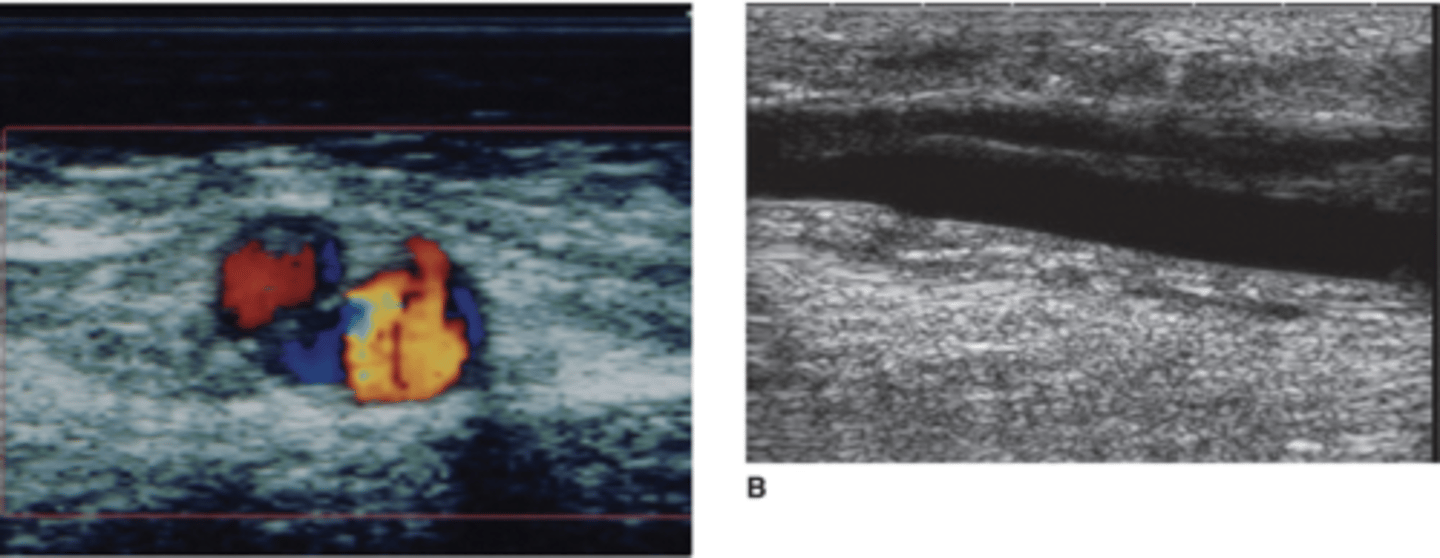
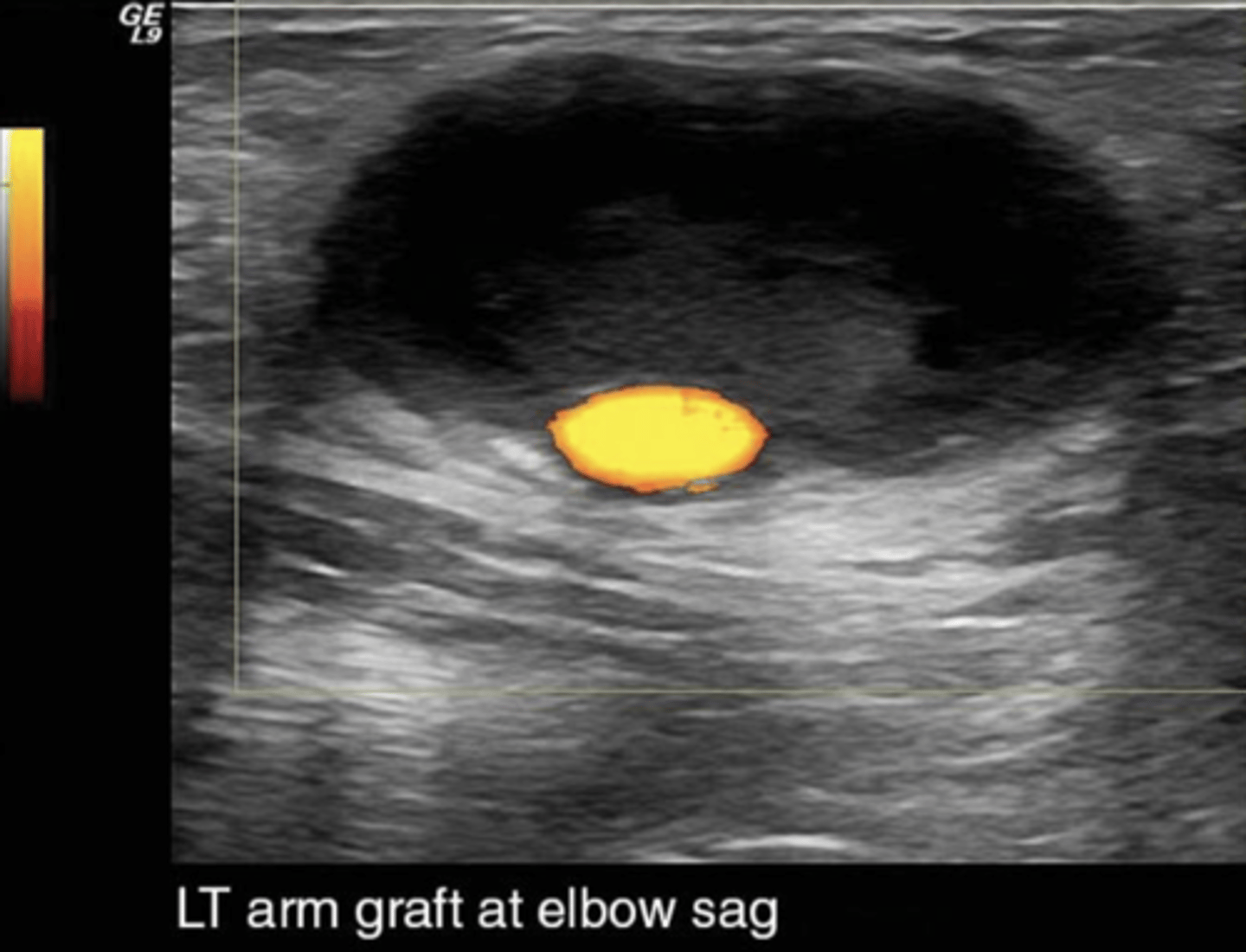
Aneurysm
Focal increase of diameter 1.5x adjacent normal vessel
Swirling color (yin/yang) & low velocity turbulent waveform
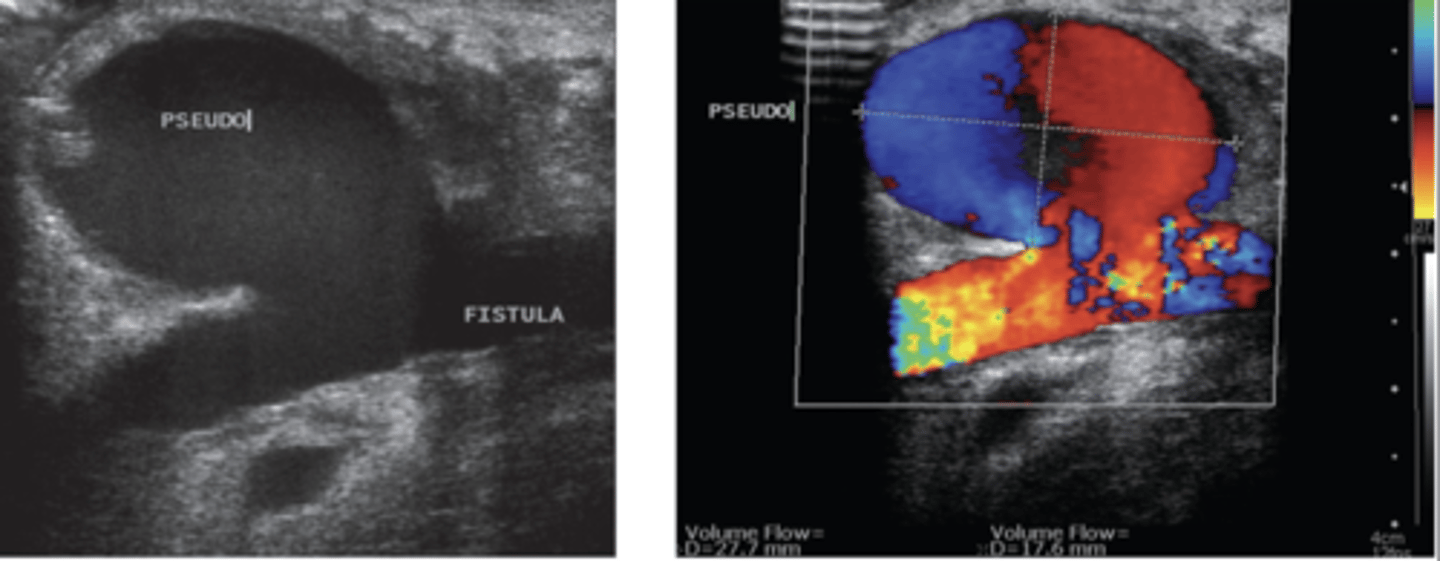
Pseudoaneurysm
Common in CFA grafts
Look for neck
To and fro flow
Dissection
Intimal flap parallel to vessel walls
Turbulent color in either lumen
Bidirectional spectral
Increased resistance
Neointimal/Myointimal Hyperplasia
Overgrowth of cells into the intimal layer
Creates narrowing and stenosis
Retained Venous Valves
Increased velocities through stenotic area at level of retained materials
Turbulent post-stenotic zone
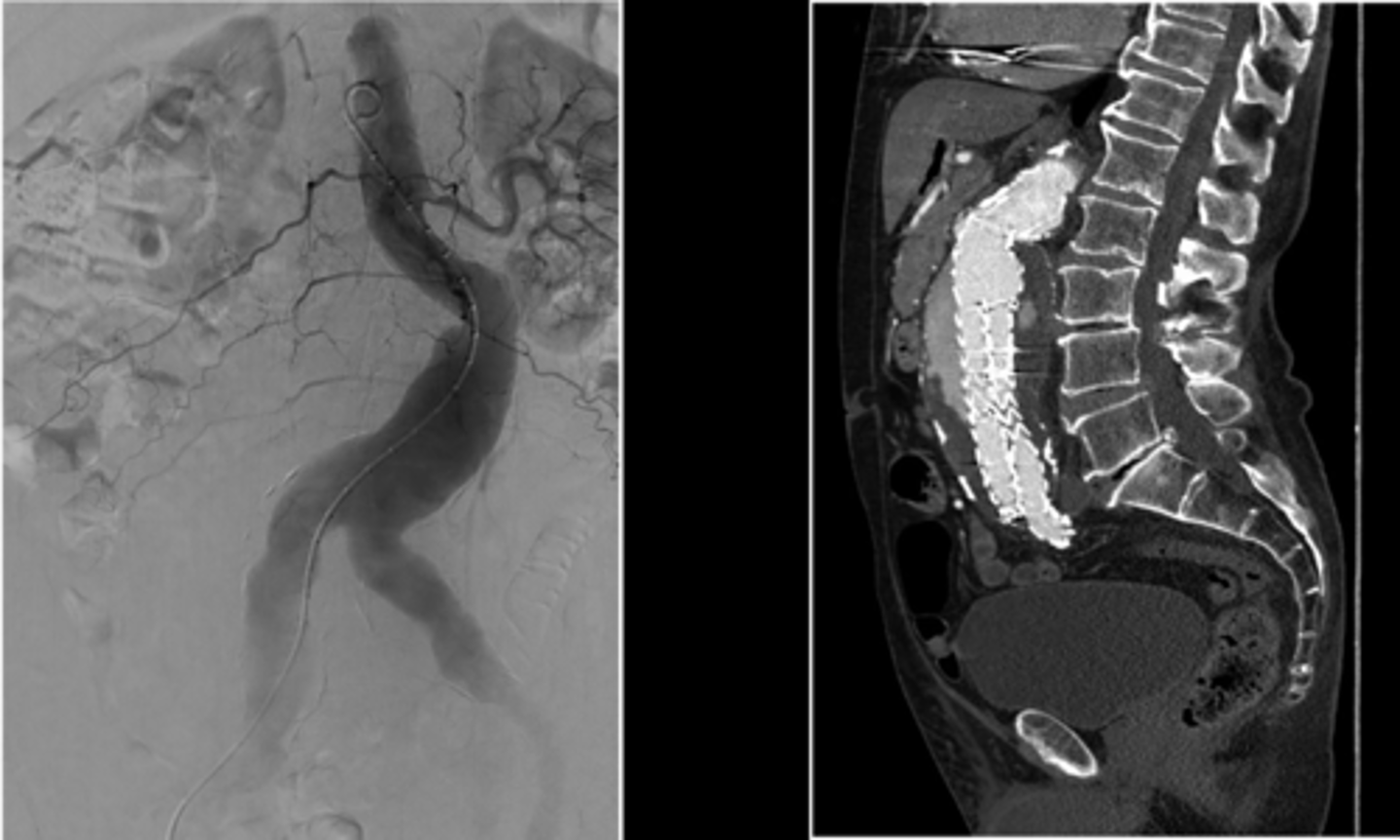
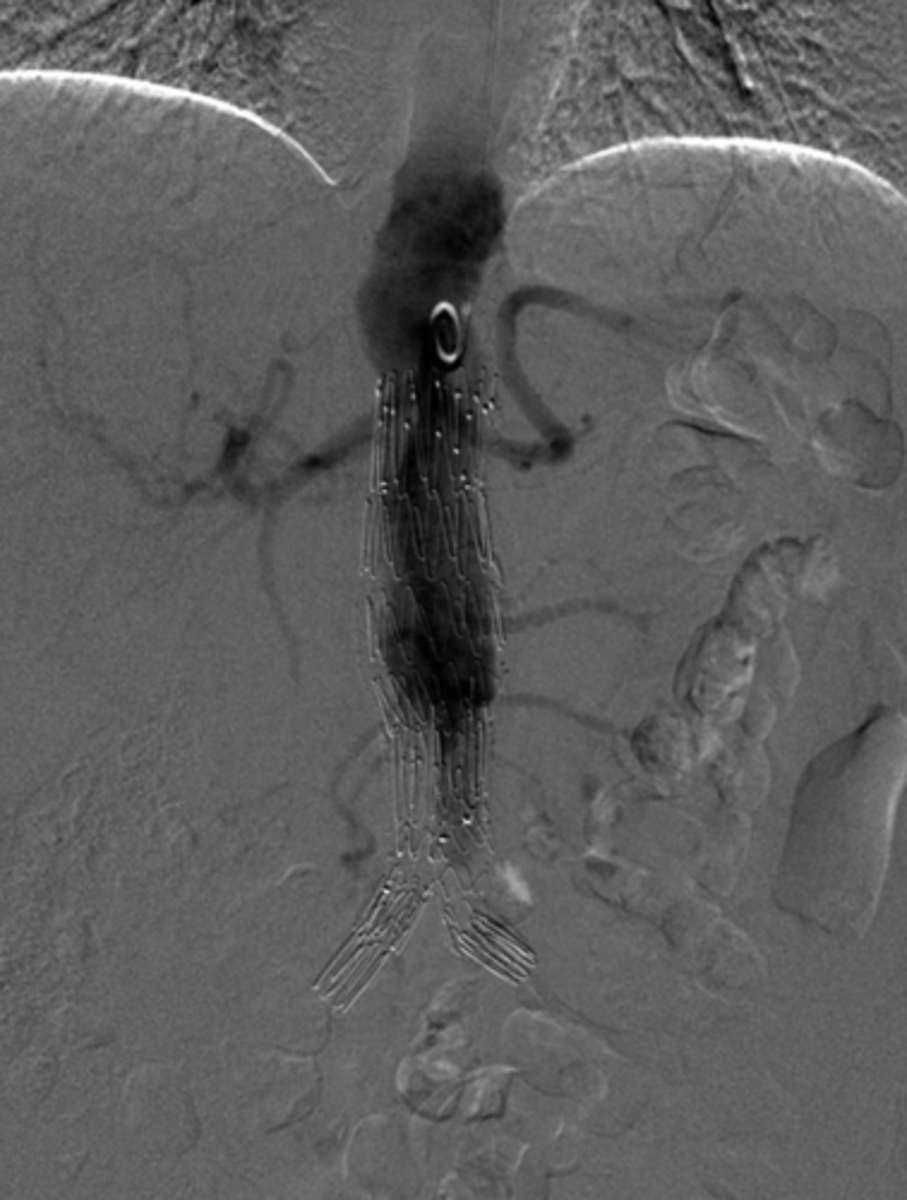
EVAR
Endovascular Aortic Aneurysm Repair
Minimally invasive procedure
Treats AAA's using a stent graft
Excludes aneurysmal sac from circulation to reduce rupture risk
Other Imaging Modalities for EAVR's
Digital subtraction angiography (DSA)
Computed tomographic angiography (CTA)
Placing an EVAR
Catheter access through CFA in groin
Device is anchored with stents in the normal aorta proximal & distal to AAA
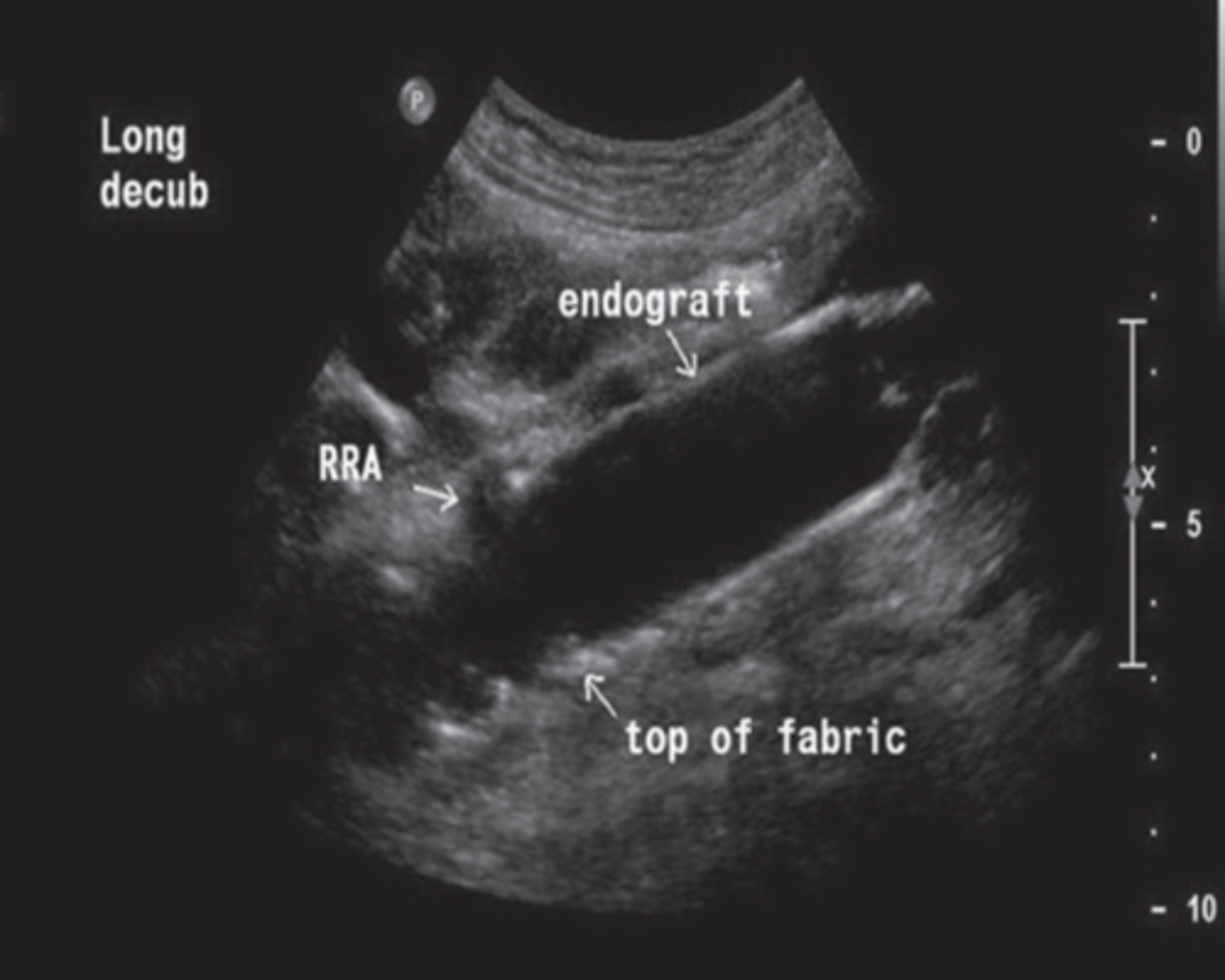
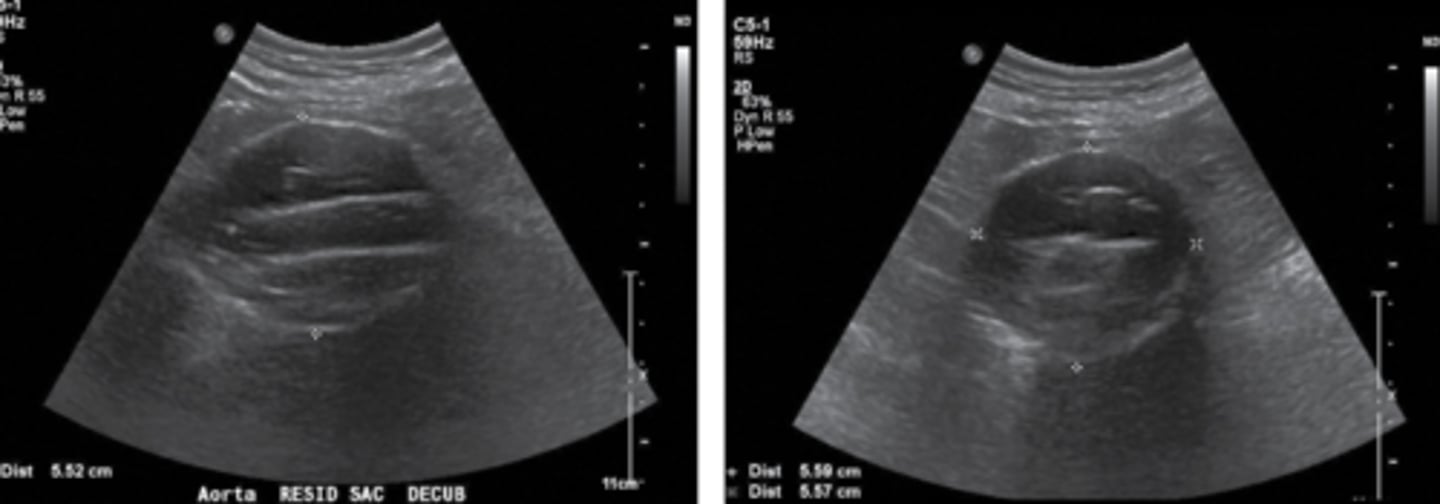
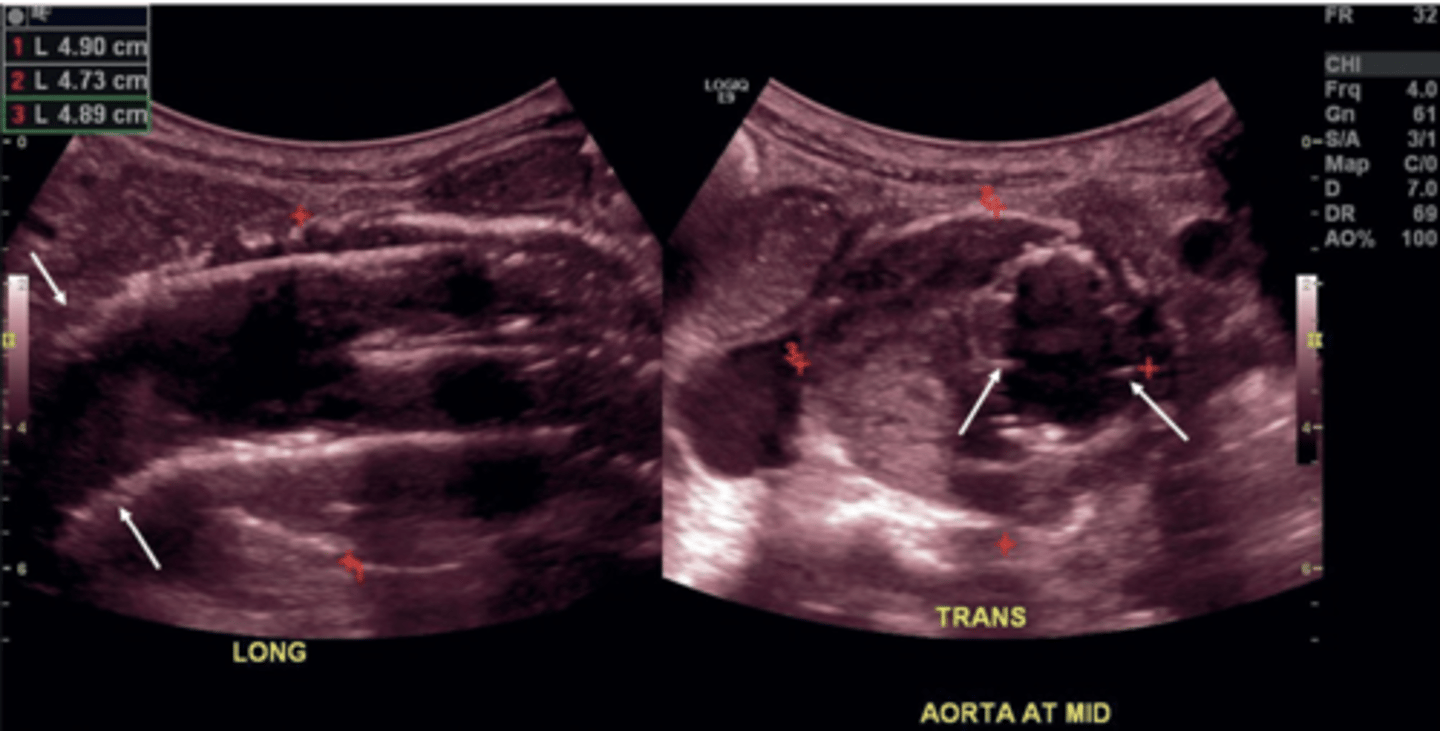
Sonographic Appearance of Residual Aneurysm
Homogenous
Heterogeneous/spongy = endoleak
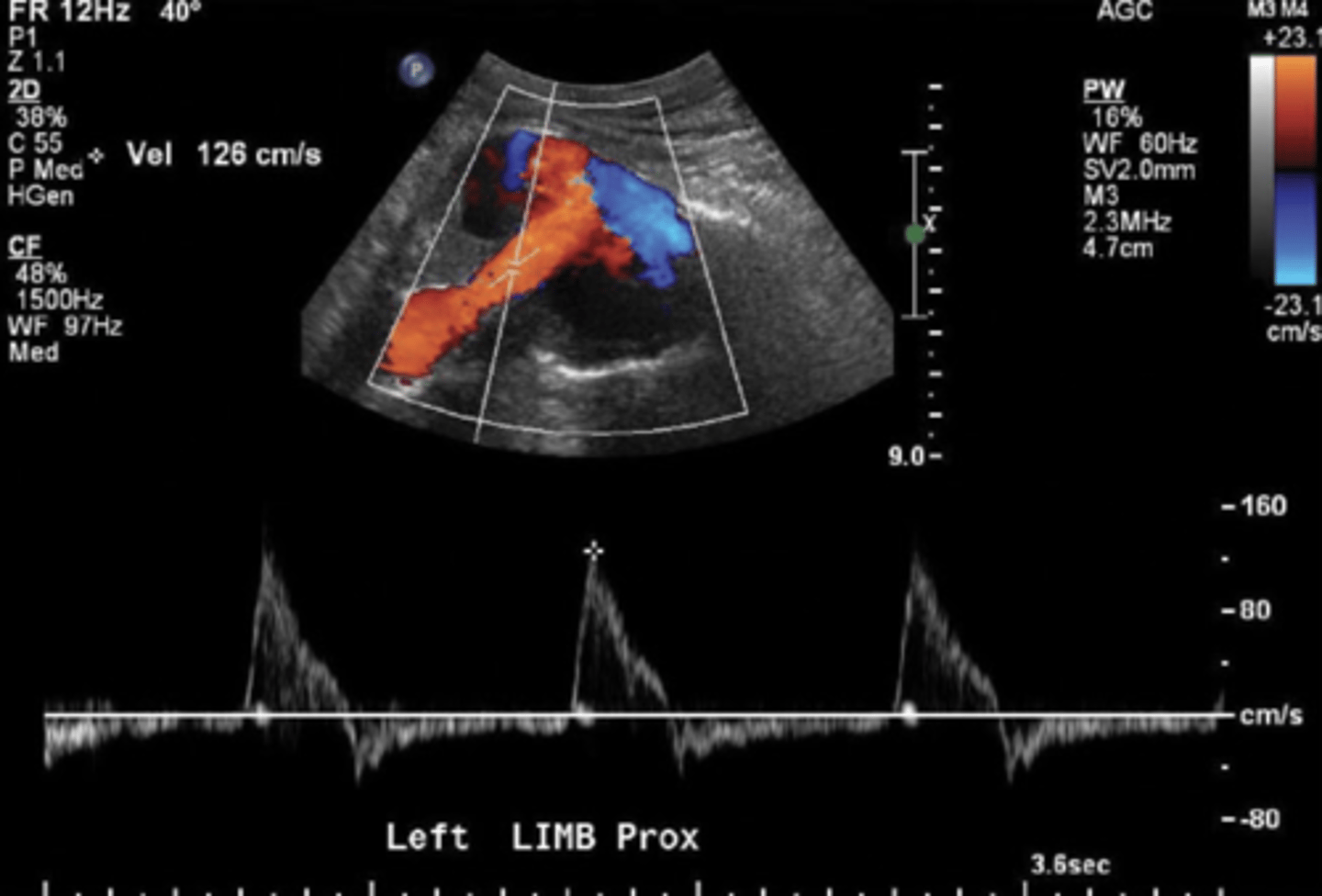
Sonographic Appearance of EVAR
Reflective (metal)
Hyperechoic proximal end
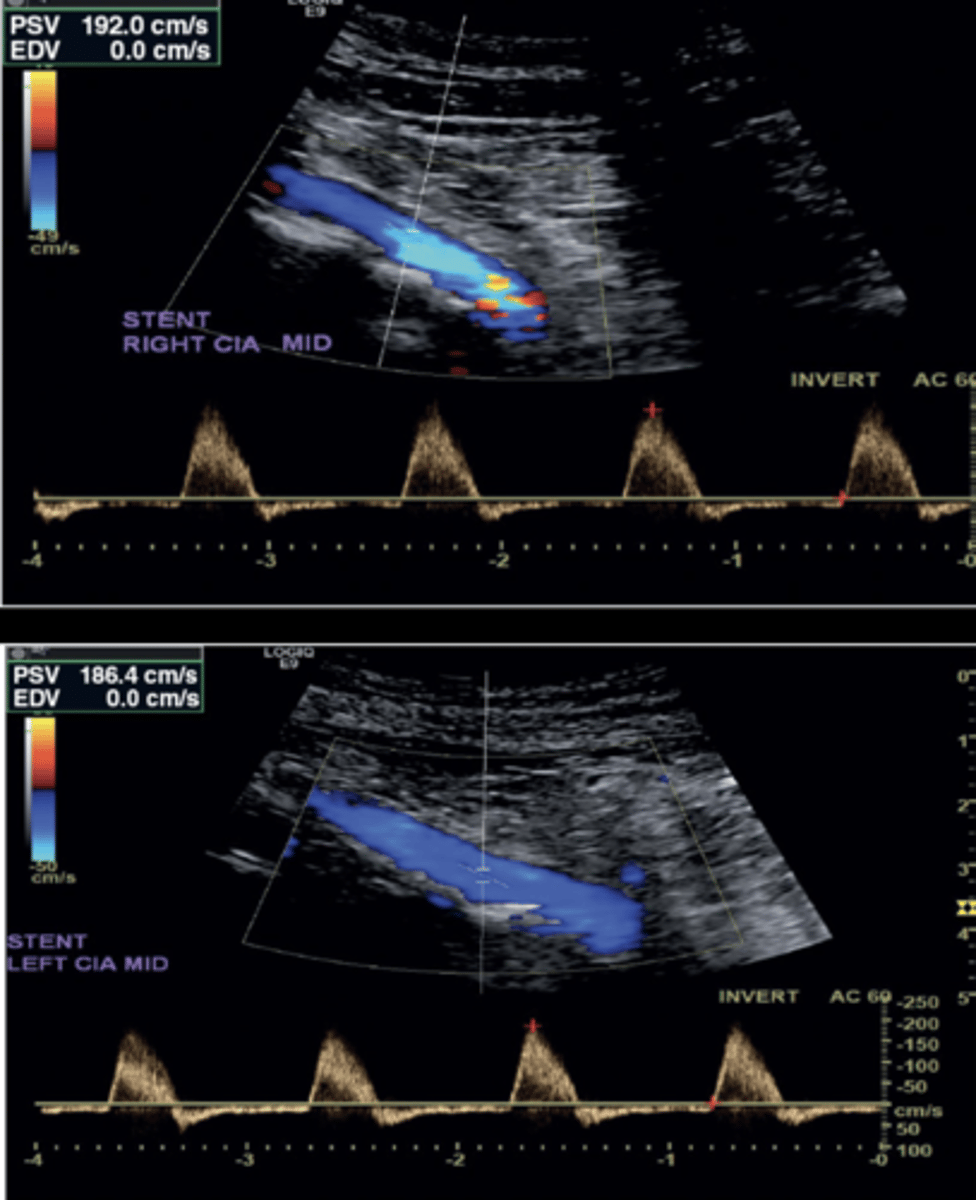
PW Waveform of EVAR
Multiphasic
Evaluate prox to, at entrance, through, at exit, and distal to graft
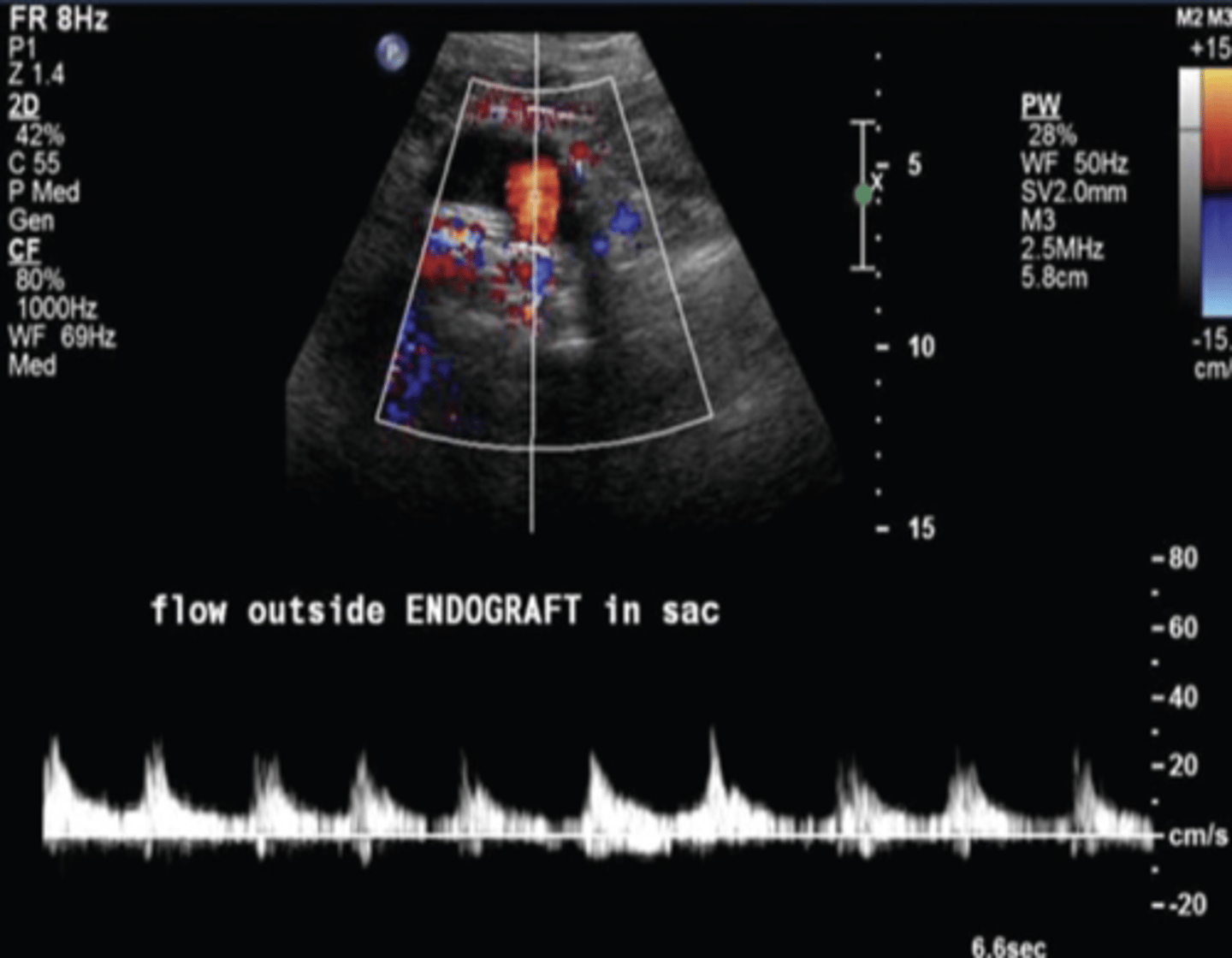
Perigraft Leaks
Arterial waveforms are different from flow within endograft
Endoleak Type 1
Inadequate seal at attachment sites
Waveforms look like that of the graft
High flow
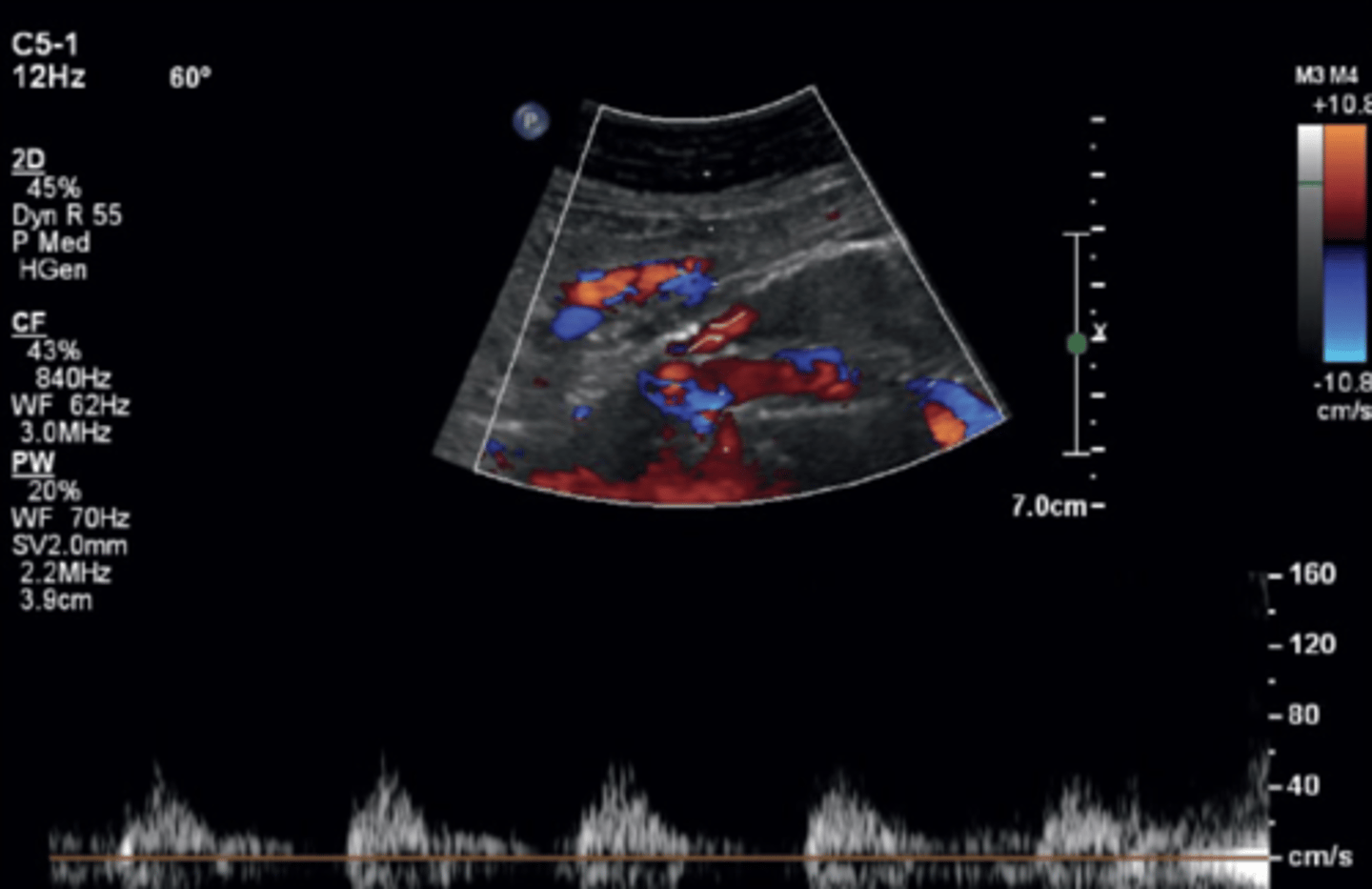
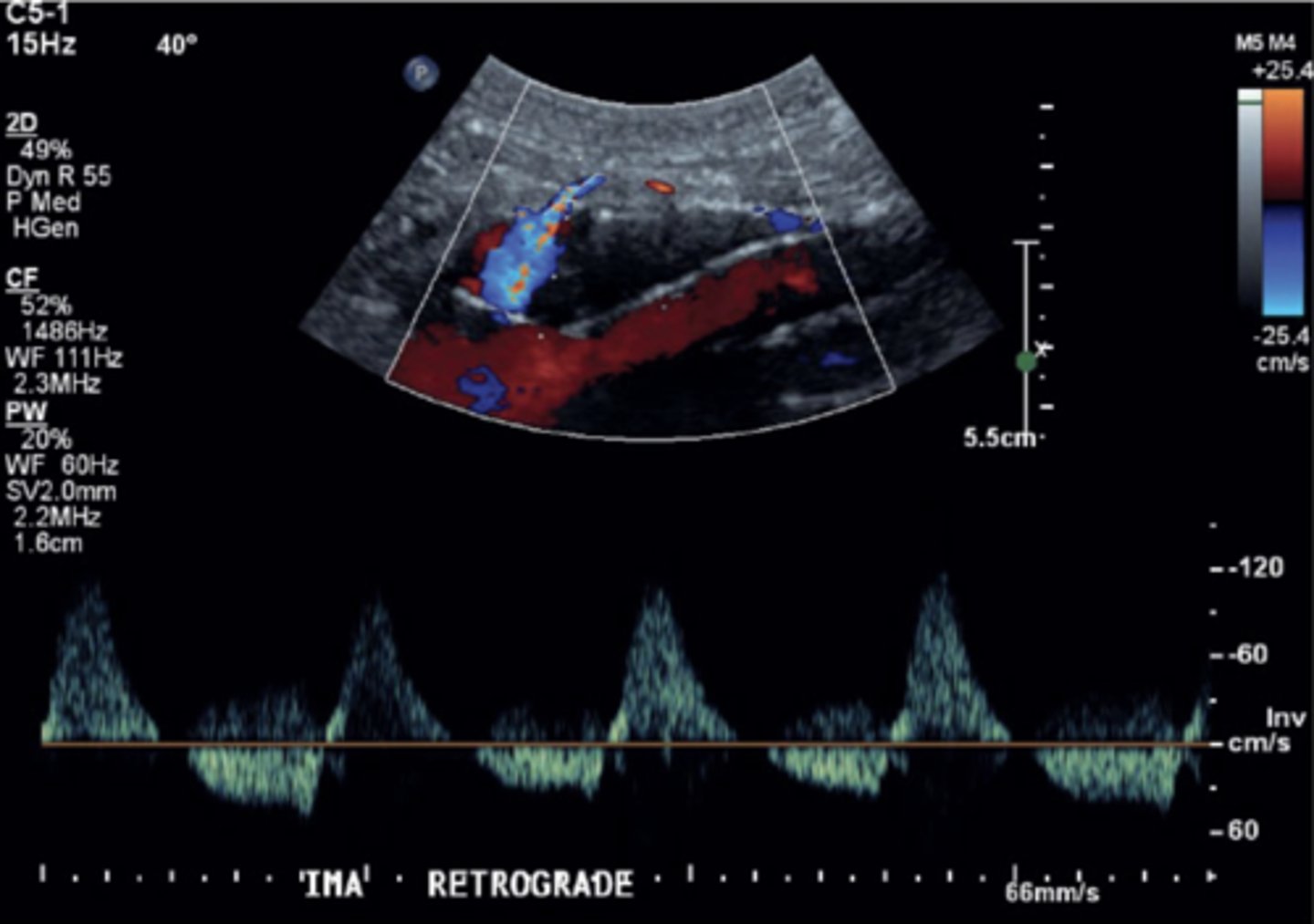
Endoleak Type 2
Leaks from branching vessel of aorta (IMA, renal A, lumbar A)
Spectral can be bidirectional, monophasic, multiphasic, slow or high flow
Endoleak Type 3
Modular disconnection of graft segments or fabric disruption (fracture)
Waveform similar to regular graft waveform
High flow
Endoleak Type 4
Blood flows through EVAR graft into aneurysm sac
Endotension (endoleak type 5)
Aneurysm continues to expand in the absence of an endoleak
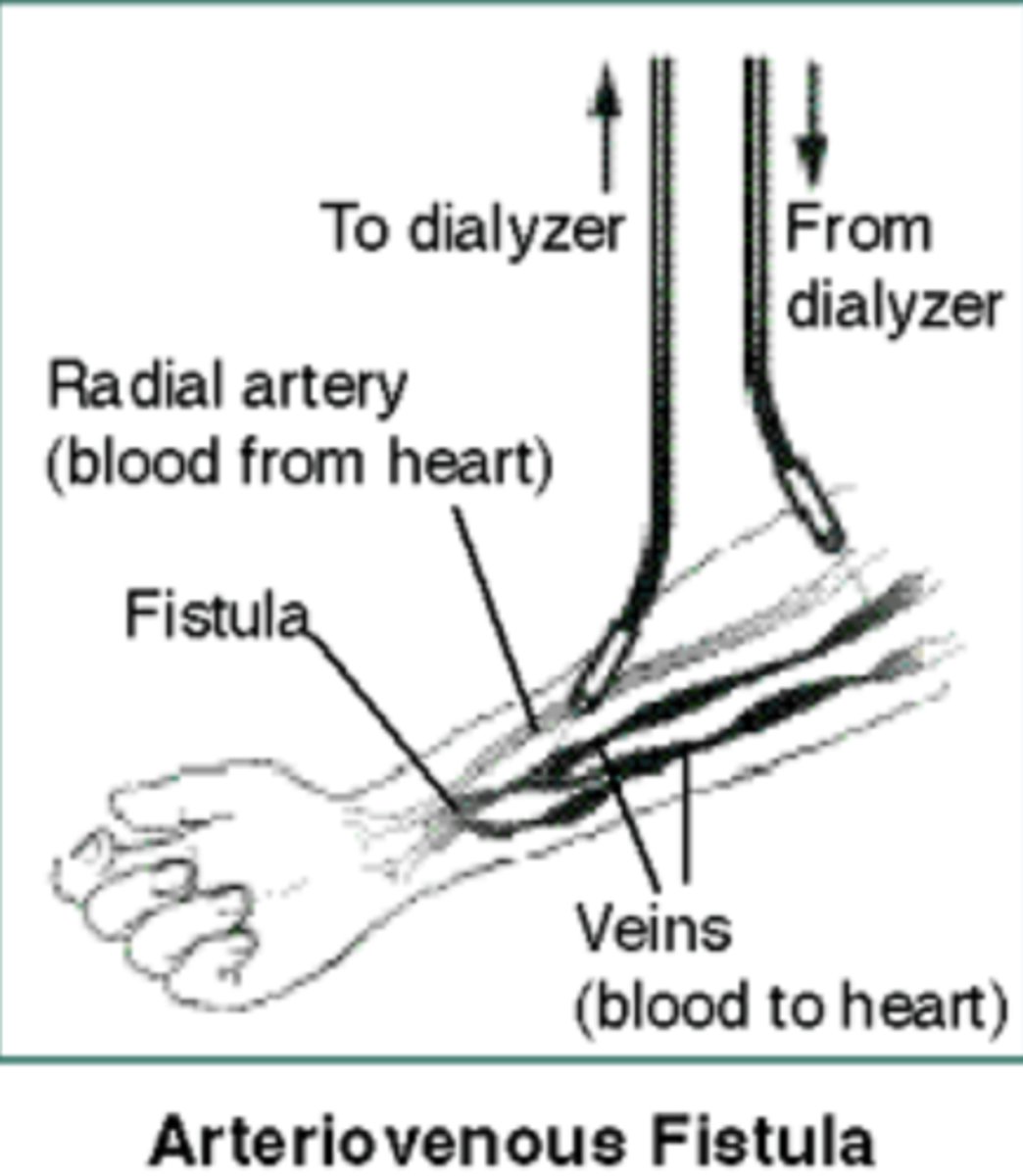
Hemodialysis AV Fistula
Anastomosis of artery & vein
Reliable, repeatable hemodialysis access with minimal complications
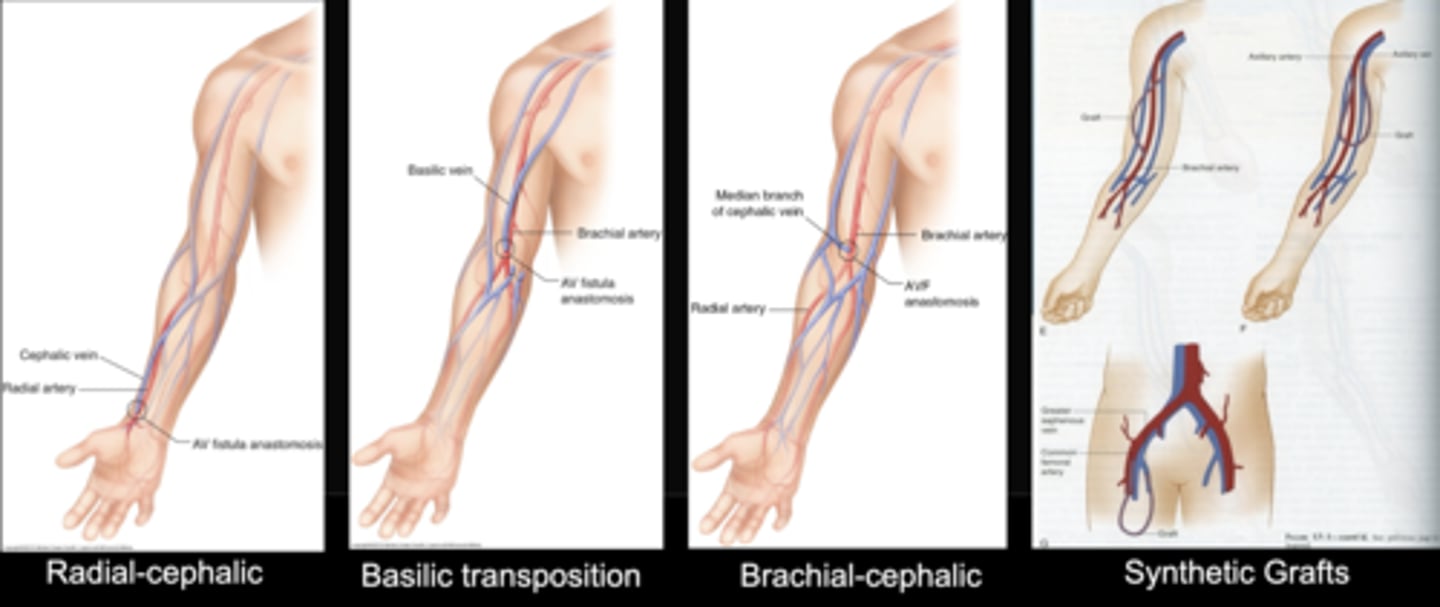
Types of Anastomoses
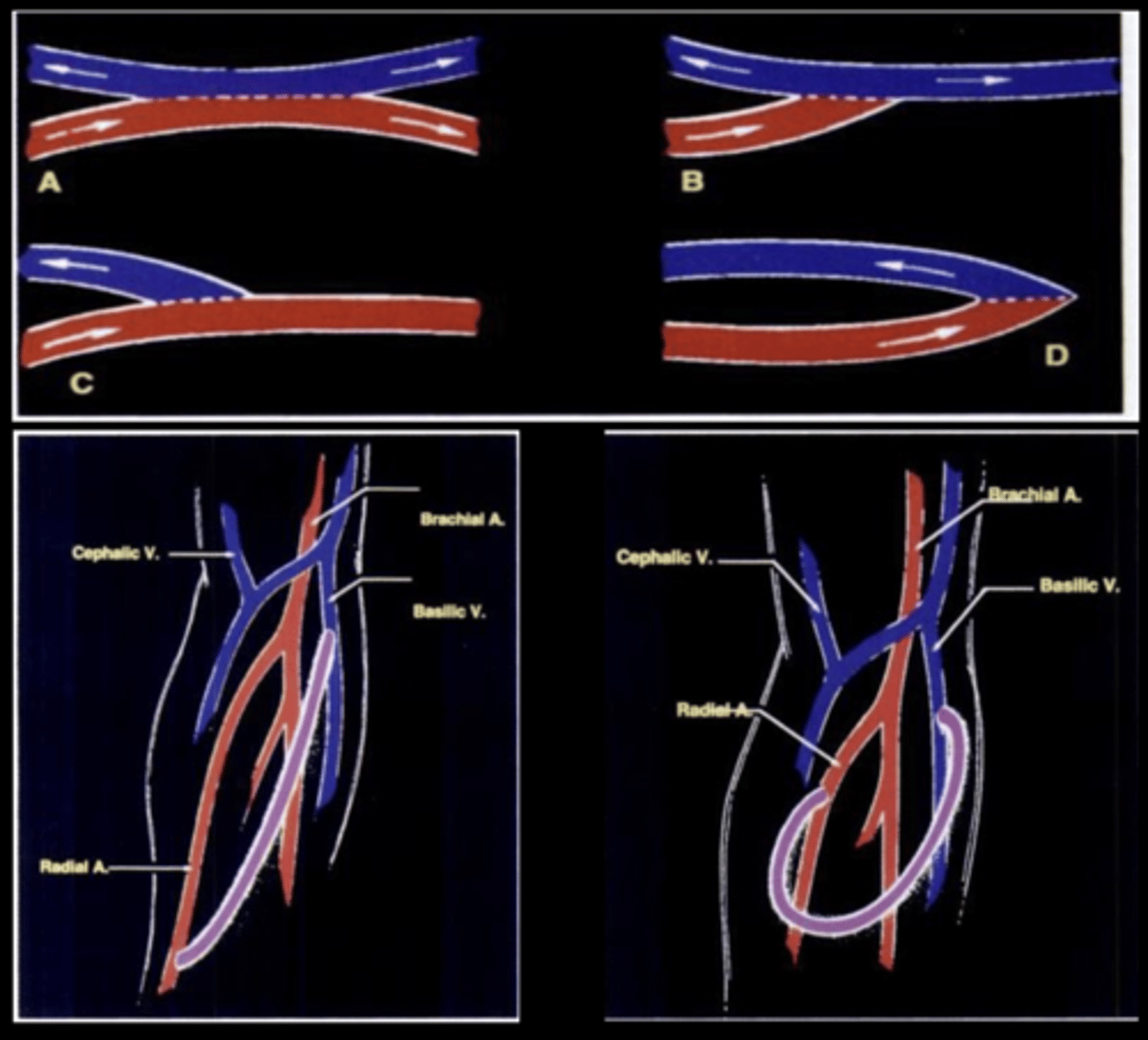
Site Preferences for AV Fistula
Non dominant forearm
Dominant forearm
Non dominant upper arm
Dominant upper arm
Lower extremity
Preferred Site for AV Fistula
As distal as possible in non-dominant arm
Why is the upper extremity preferred for AV fistulas?
Patient comfort & preference
Lower infection rates
Greater longevity
Easier to access
Patient Prep & Assessment
Keep room warm
Patient in supine/sitting position
Take bilateral blood pressures
Take pulses of brachial, radial, and ulnar arteries
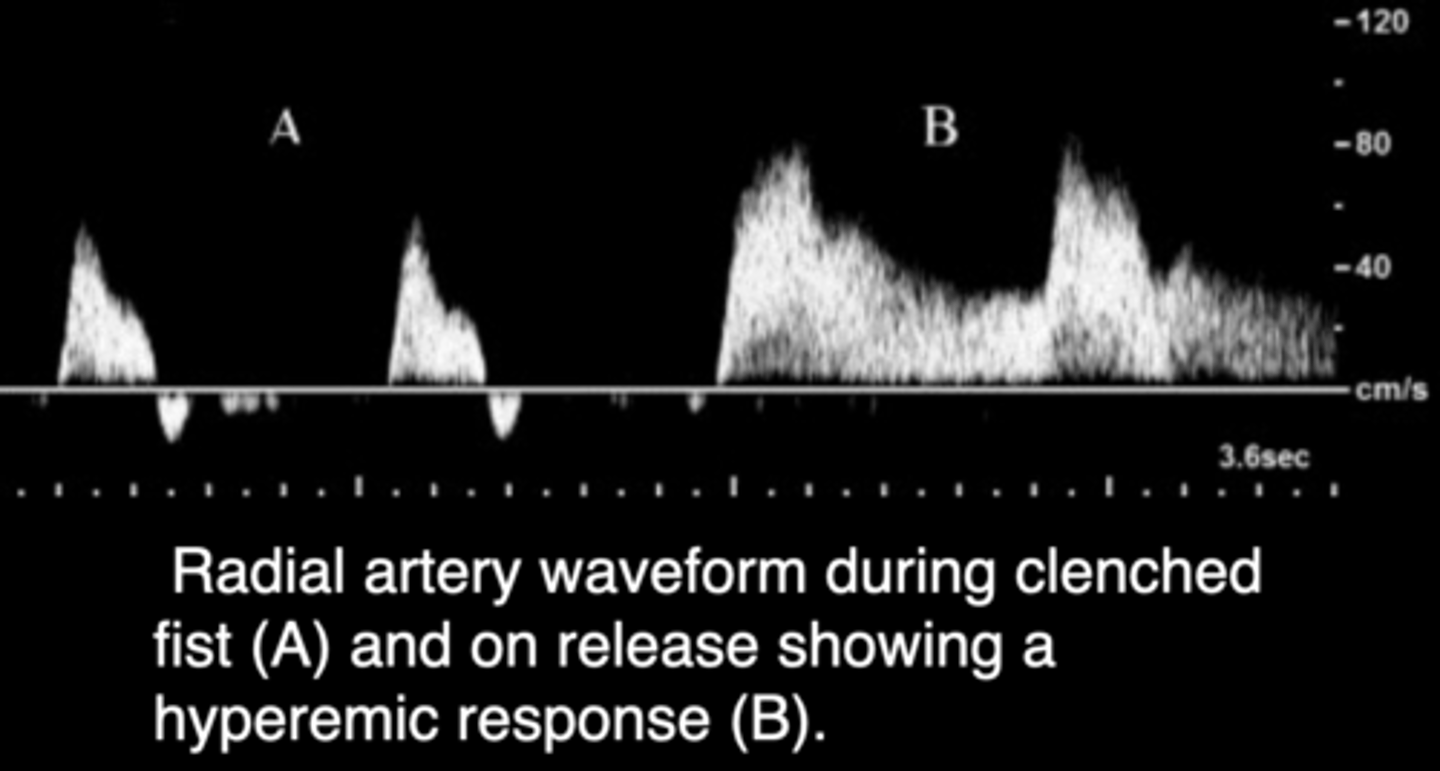
Allen Test: assesses for intact palmar arch - clenched fist - reactive hyperemia after compression indicates patency
Assess superficial veins using tourniquets
Fistula Maturation Failure
Caused by obligatory use of small/suboptimal veins
Quality of Artery
Determines capacity to dilate & accommodate increased flow
Fistula/Graft Mapping
Find suitable artery before moving onto venous system
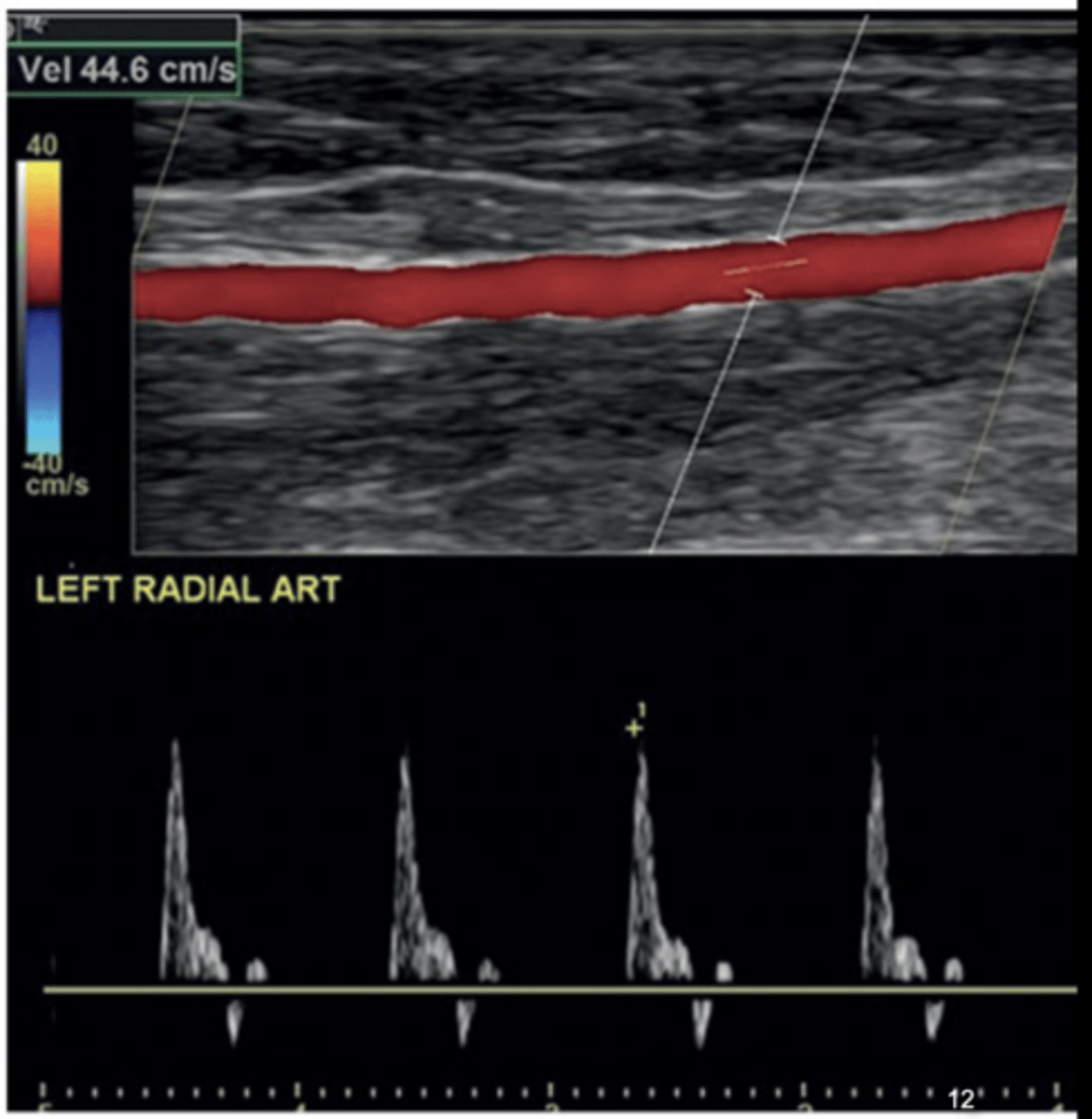
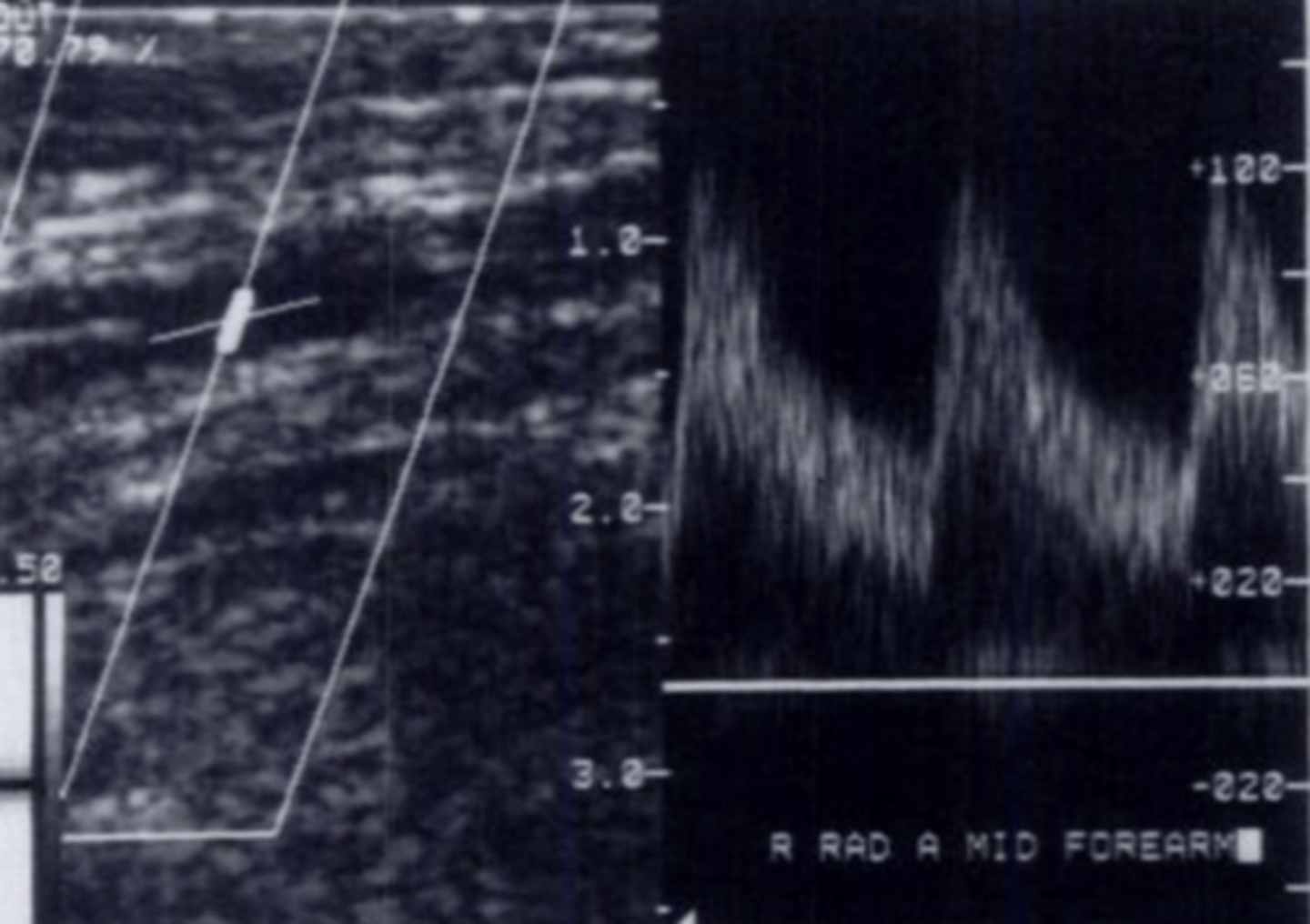
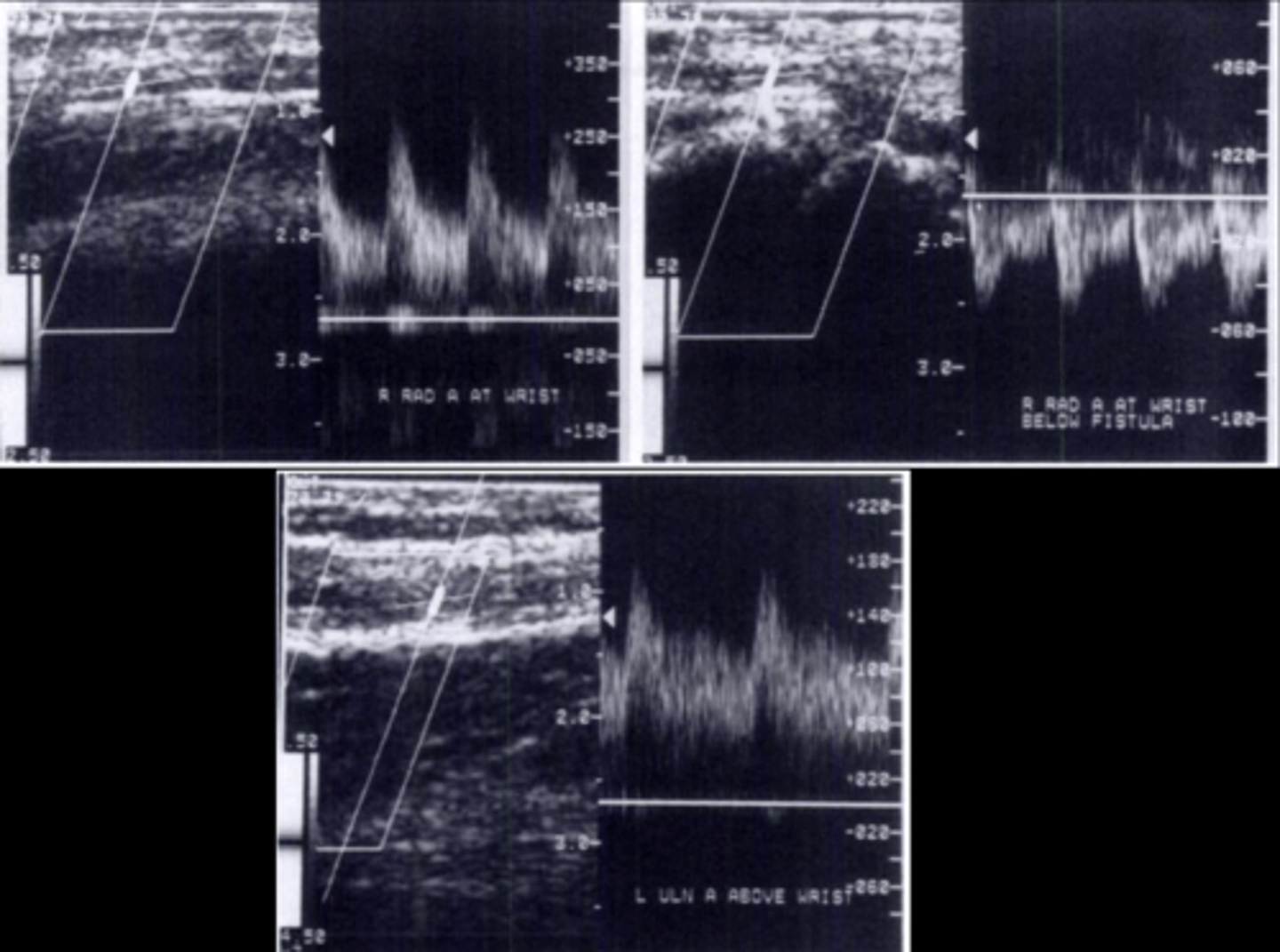
AV Fistula & Hemodialysis Graft Arterial Mapping
Start with distal forearm of non-dominant arm
Assess for plaque, thickening, stenosis, compliance
Evaluate waveform & note PSV - high resistant (rapid upstroke, sharp peak, low diastolic flow)
Arterial Diameter for Fistulas/Grafts
> 2.5 mm
AV Fistula & Hemodialysis Graft Venous Mapping
Start with superficial system of non-dominant forearm
Begin with cephalic, basilic, and median cubical veins at wrist and move proximally to axilla
Assess for thrombus, compressibility, narrowing, tributaries , scarring- central veins have respirophasicity & cardiac pulsatility
Compress & record diameter every 2 cm
Doppler with augmentation (include subclavian & IJV)
Measure vein diameter with & without tourniquet (2 tourniquets-at axillary & forearm-for 3 minutes)
Assess depth from skin surface to anterior wall of vein
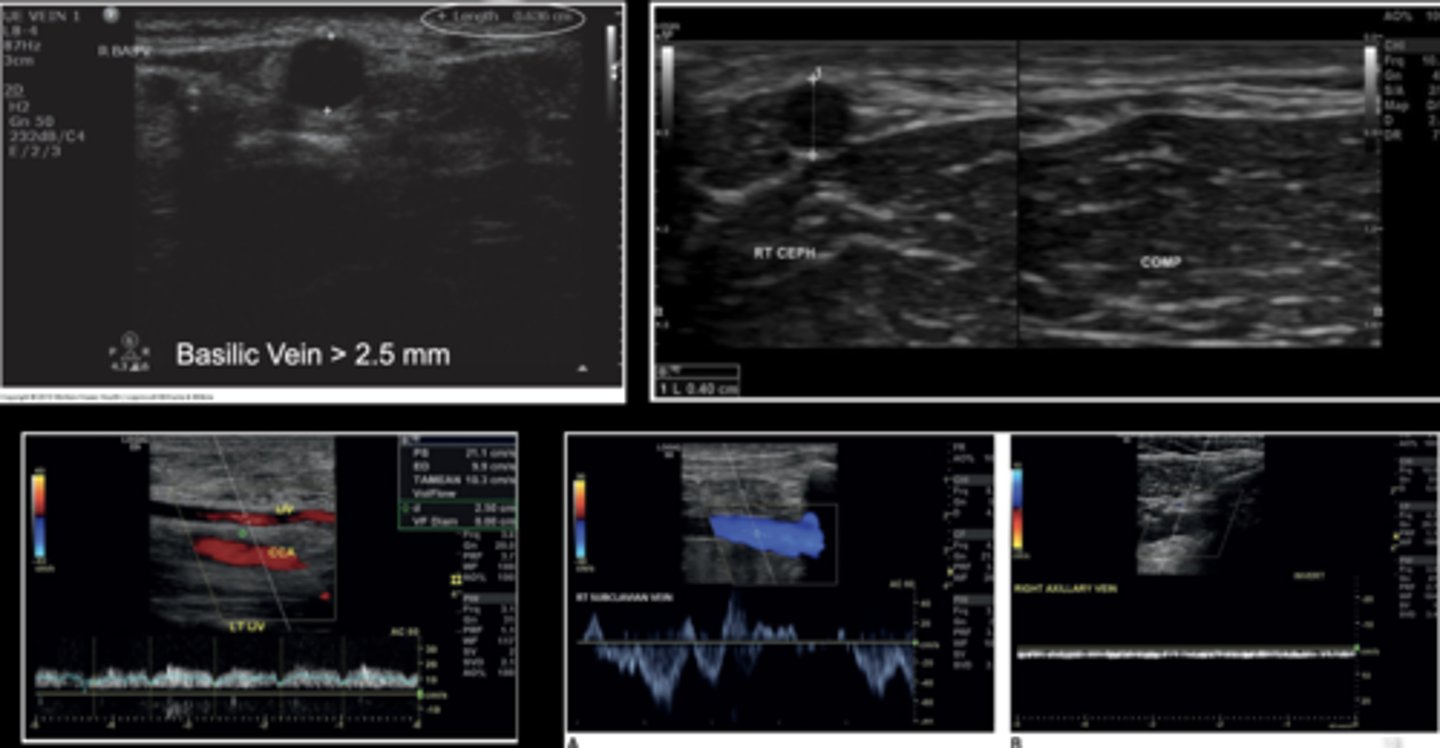
Vein Diameter for Fistulas/Grafts
> 2.5 mm
Vein Diameter for Synthetic Fistulas/Grafts
≥ 4 mm
Basilic Vein Length for Fistulas/Grafts
≥ 10 cm
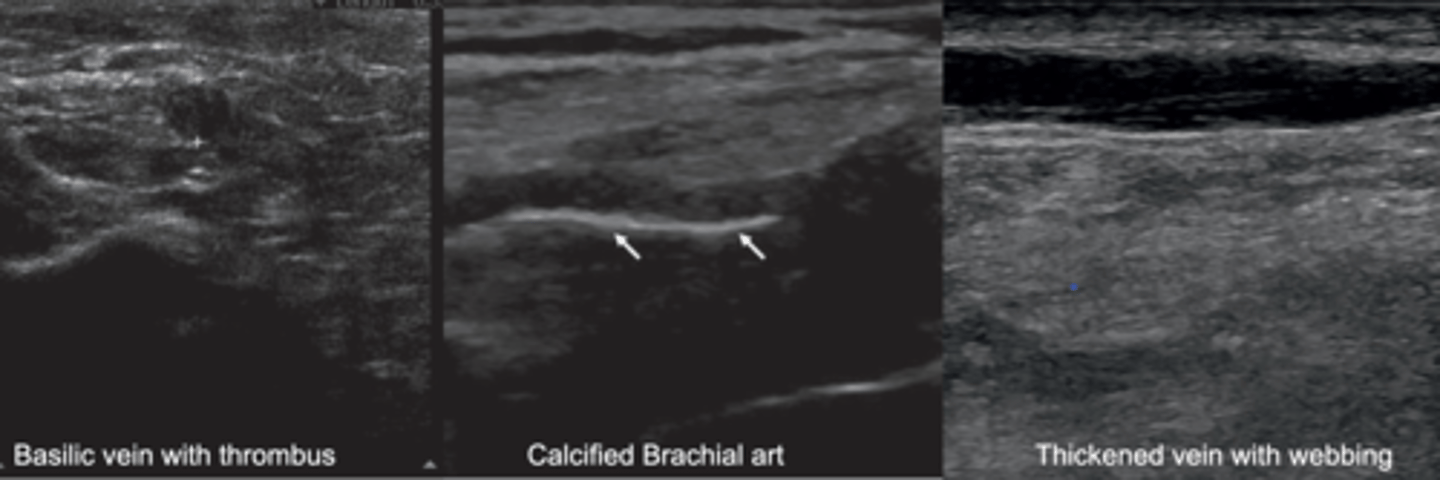
Pre-Mapping Contraindications for AV Fistula Placement
Thrombus
Calcifications
Thickened vessels
Local infection
Dressings that can't be removed
Open wounds
AV Fistula/Graft Maturity
Occurs 6 weeks - 6 months after placement
Assess 10-12 weeks after placement before hemodialysis begins
Mature AV Fistula/Graft
Drop in peripheral resistance
Can handle 6 cycles a month
Audible swishing bruit
Palpable thrill/vibration - turbulent flow at anastomosis
Large enough for two 15-gauge needles
Normal PSV for Fistula
100-400 cm/sec
Normal EDV for Fistula
60-200 cm/sec
Fistula Surveillance
Fistula diameters
Depth from skin surface
PSV's of:
- Native artery prox to anastomosis/arterial inflow
- Arterial anastomosis
- Throughout fistula - walk-through technique
- Venous outflow
Assess patency of all inflow arts/outflow veins
Arterial Side of Fistula
Low-resistant waveform
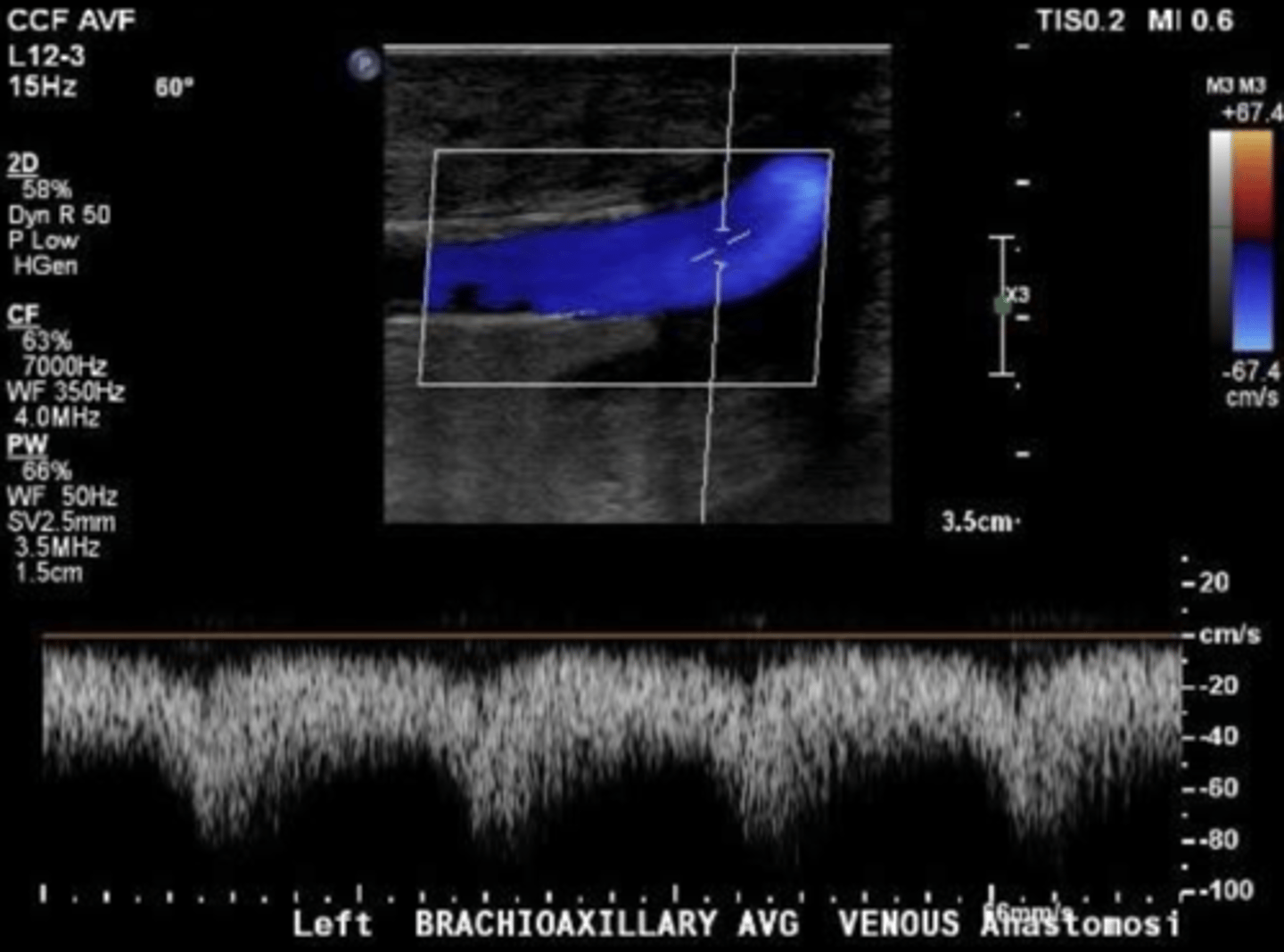
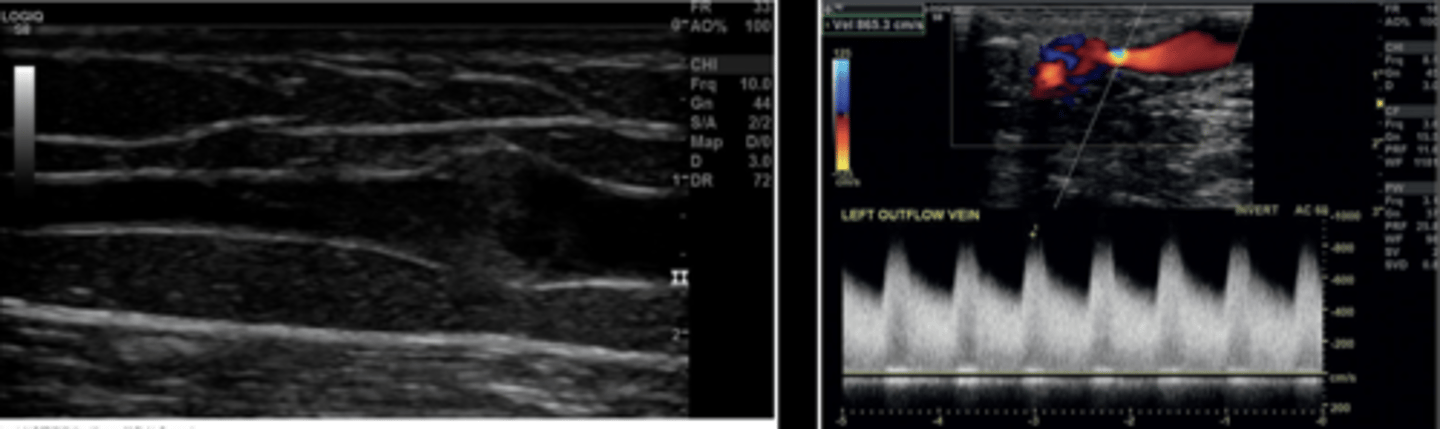
Venous Side of Fistula
High flow volume
Pulsatile prox to anastomosis
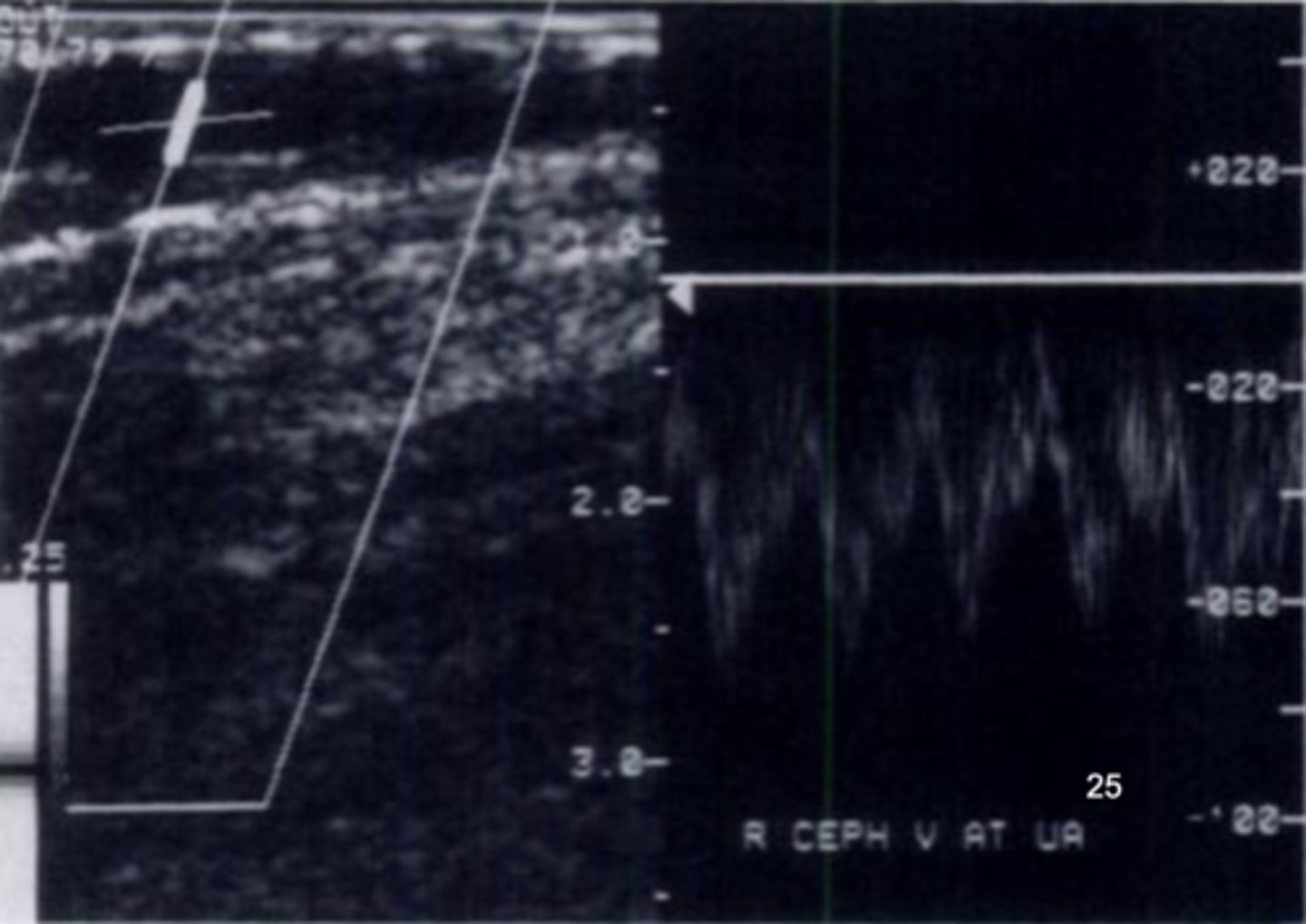
Normal Fistula Inflow Artery
Proximal to anastomosis
Low resistant - forward diastolic flow & spectral broadening
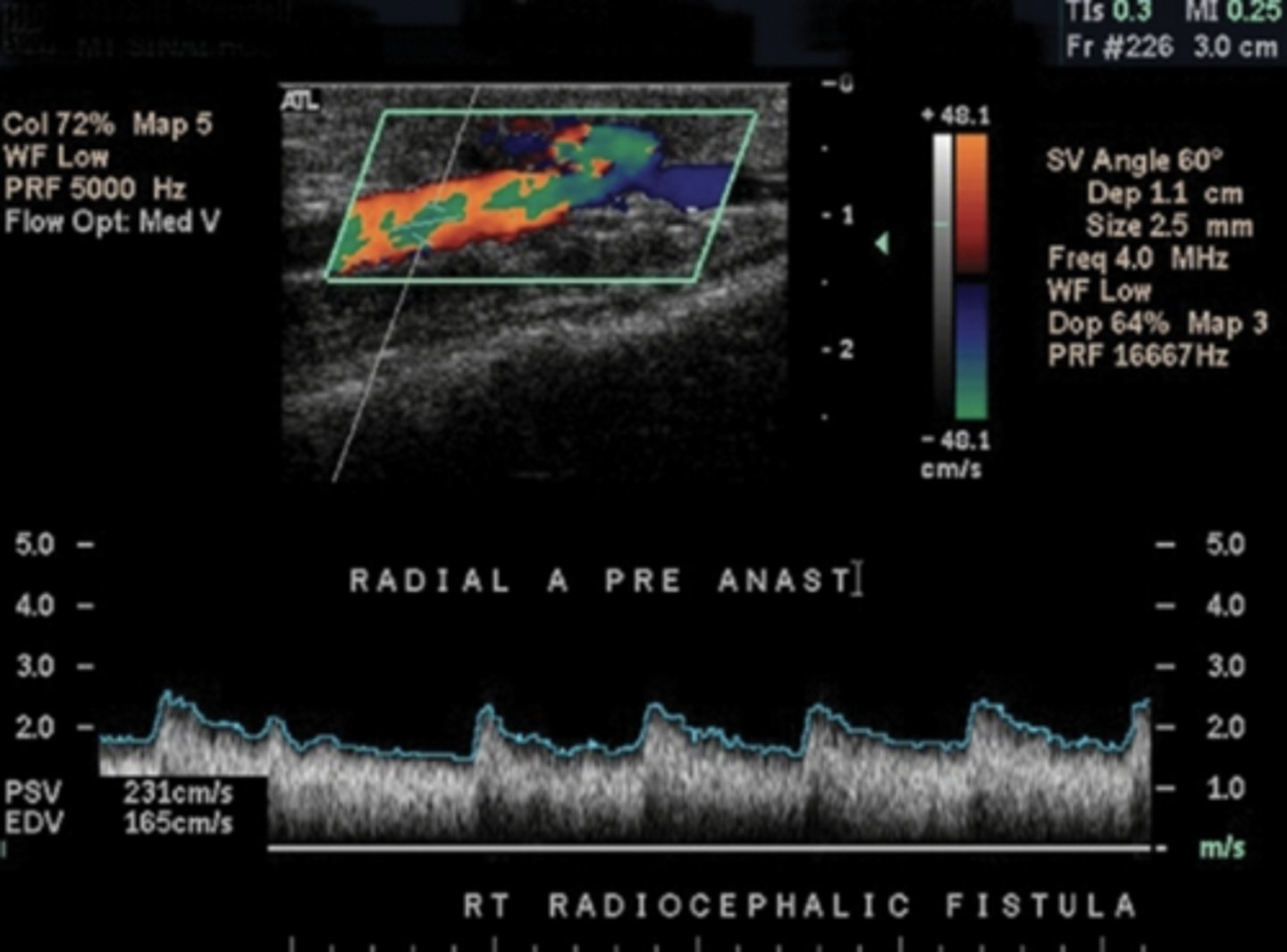
Normal Fistula Flow
1 cm below skin
Low resistant - forward diastolic flow & spectral broadening
Elevated PSV & EDV velocities
Normal Venous Outflow
Pulsatile flow
Acquiring Flow Volume of a Mature Fistula
Evaluate function at mid-fistula
Large sample volume (wide as vessel)
Measure diameter on grayscale
Use auto-tracing or trace 3-4 waveforms for mean velocity
Take at least 3 times
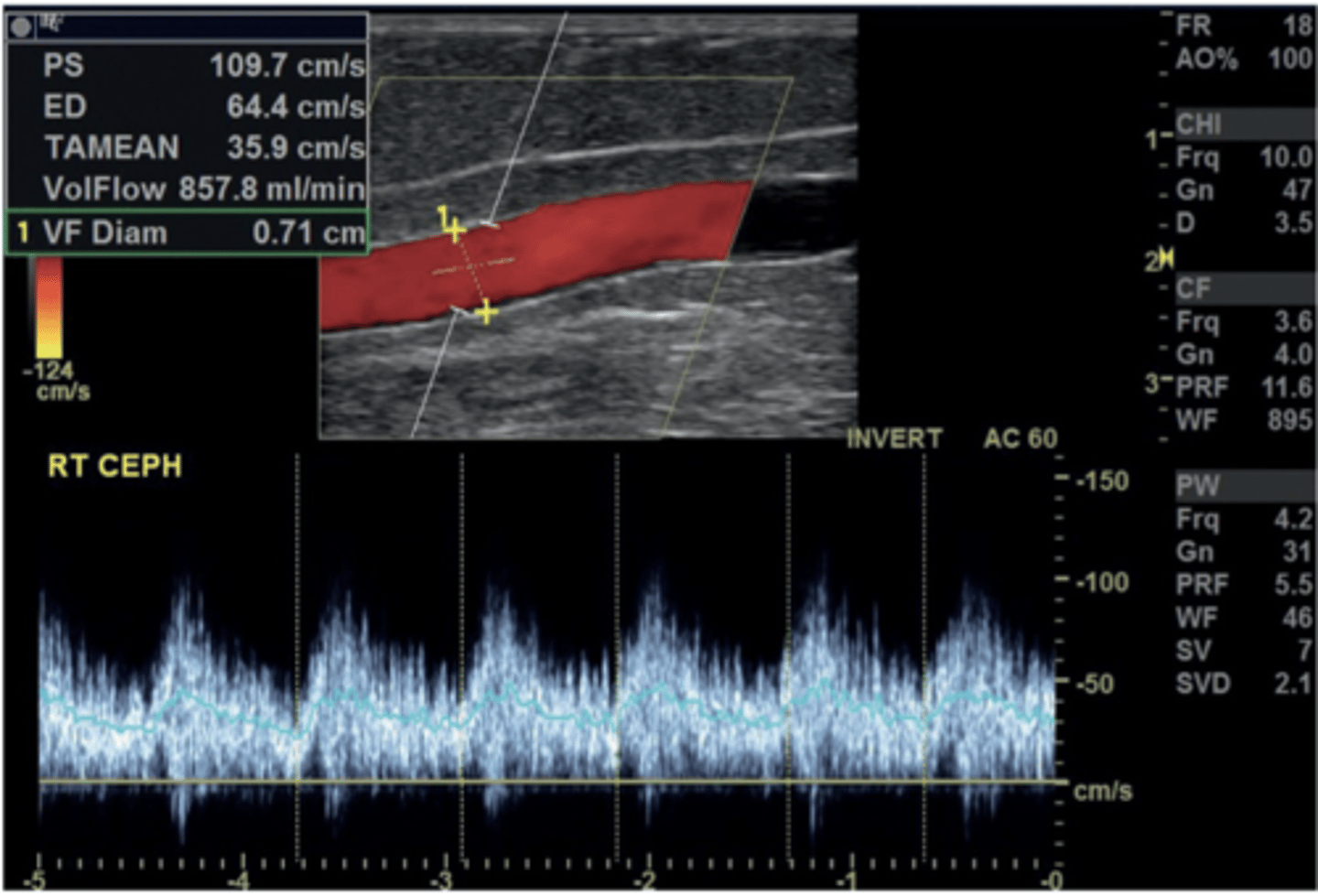
Normal Flow Volume of a Mature Fistula
> 800 ml/min
AV Fistula & Graft Complications
Immaturity
Stenosis
Occlusion
Thrombosis
Aneurysm and Pseudoaneurysm
Fluid collections
CHF
Arterial Steal Syndrome
Immature AV Fistula
Proximal hammer pulse
Minimal thrill
Lack of venous distention
Lack of high-pitched bruit
Signs of stenosis & palpable distal thickening
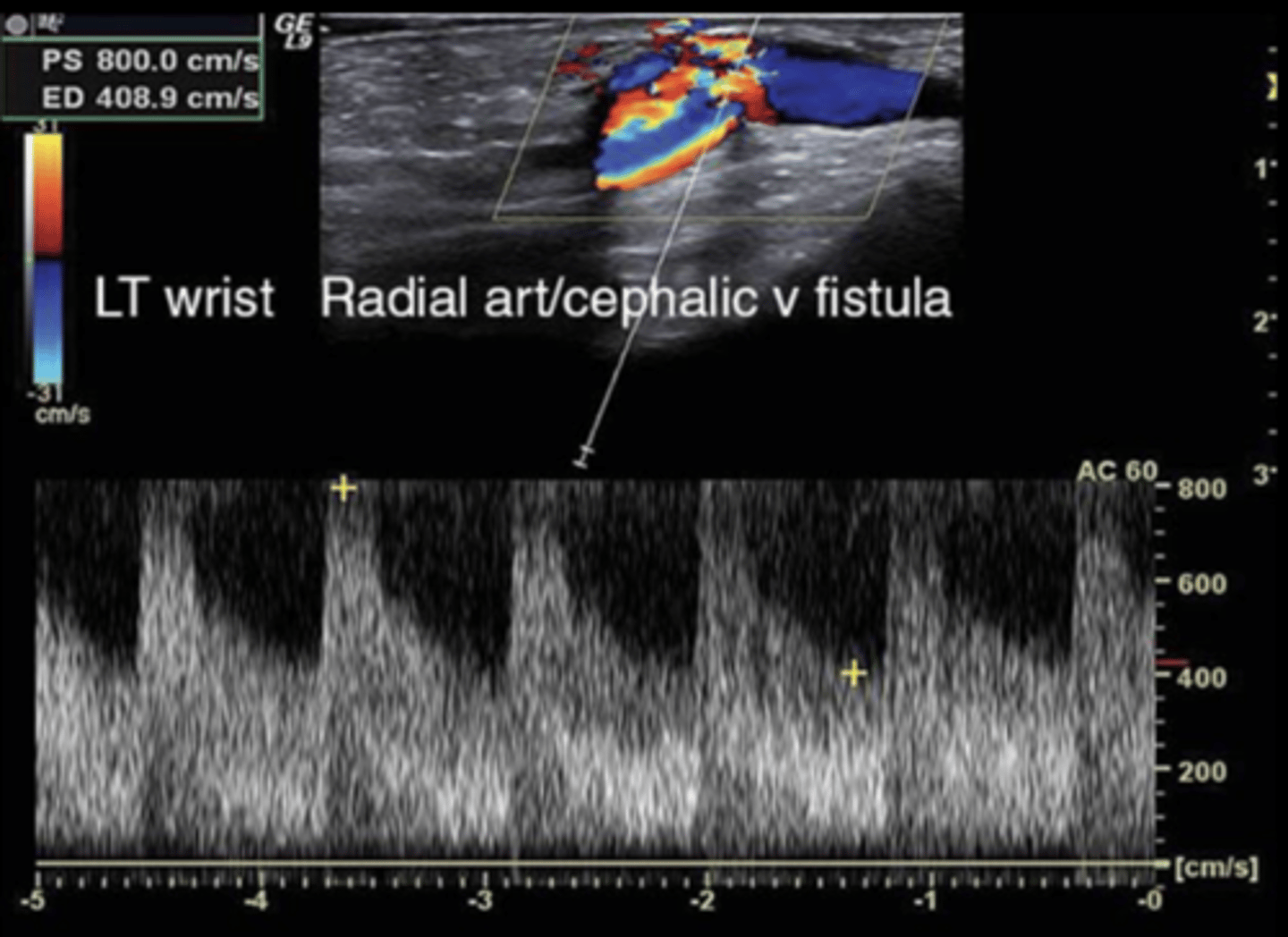
AV Fistula Stenosis
Most common in venous anastomosis & outflow vein
Echogenic intraluminal lesion
Flow reduction
Mild/Moderate Stenosis Flow Volume
500-800 ml/min
Severe Stenosis Flow Volume
< 500 ml/min
PSV of AV Fistula Stenosis
> 375 cm/sec
PSV Ratio for > 50% Stenosis on Arterial Side
> 3:1
PSV Ratio for > 50% Stenosis on Venous Side
> 2:1
AV Fistula Occlusion
Absent flow in lumen
Echogenic thrombus in lumen
Prox high-resistant flow
AV Fistula Thrombosis
To and Fro flow- inflow
Low PSV
Absence of color flow & no outflow
Echogenic material
AV Fistula Aneurysm
AV Fistula Pseudoaneurysm
AV Fistula Fluid collections
Arterial Steal Syndrome
Occurs in 75-90% of patients
Most patients are asymptomatic
Due to poor distal collateral circulation & high flow through fistula
Low-resistant outflow vein draws antegrade flow from inflow artery & steals retrograde flow from distal artery
Failing AV Fistula/Graft Interventions
Percutaneous transluminal angioplasty
Percutaneous recanalization
Interoperative branch ligation
Interoperative revision and vein interposition
DRIL procedure
DRIL Procedure
Ligation of native artery distal to dialysis access
Bypass from native artery to artery distal to ligation

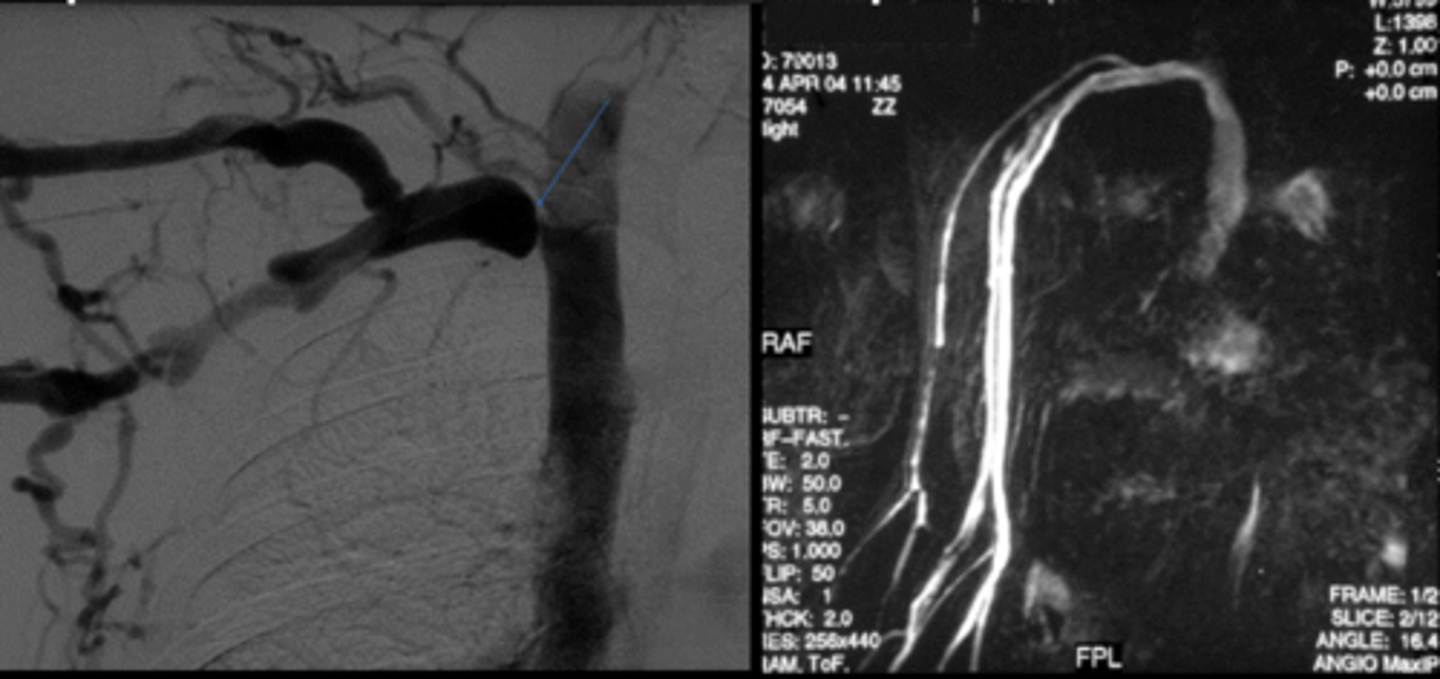
Complimentary Imaging for AV Fistula Mapping/Monitoring
Venography
Enhanced MR Venogram
Anterior Circulation of the Circle of Willis
Carotid siphon - parasellar, genu, and supraclinoid segments
ICA branches - ophthalmic & posterior communicating
MCA
Anterior cerebral - pre & post-communicating
Anterior communitating
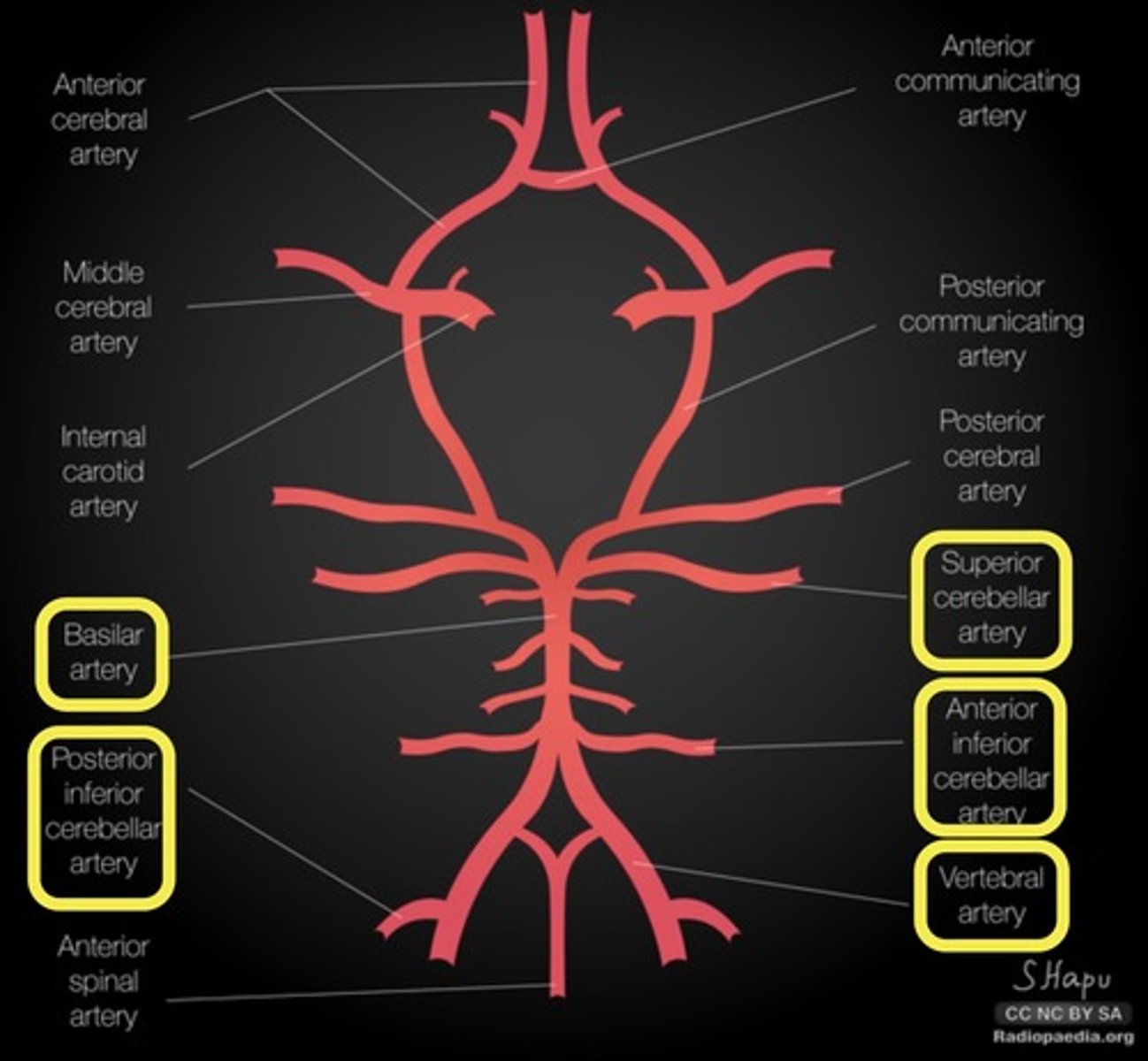
Posterior Circulation of the Circle of Willis
Vertebral
Basilar
Posterior Cerebral - pre & post-communicating
Vertebrobasilar Circulation of the Circle of Willis
Vertebral - posterior inferior cerebellar
Basilar - anterior inferior cerebellar & superior cerebellar
Common Anatomical Variants in Cranial Vessels
Hypoplasia of posterior communicating A
Hypoplasia of pre-communicating posterior cerebral A
Hypoplasia &/or Duplication of anterior communicating A
Hypoplasia of pre-communicating anterior cerebral A
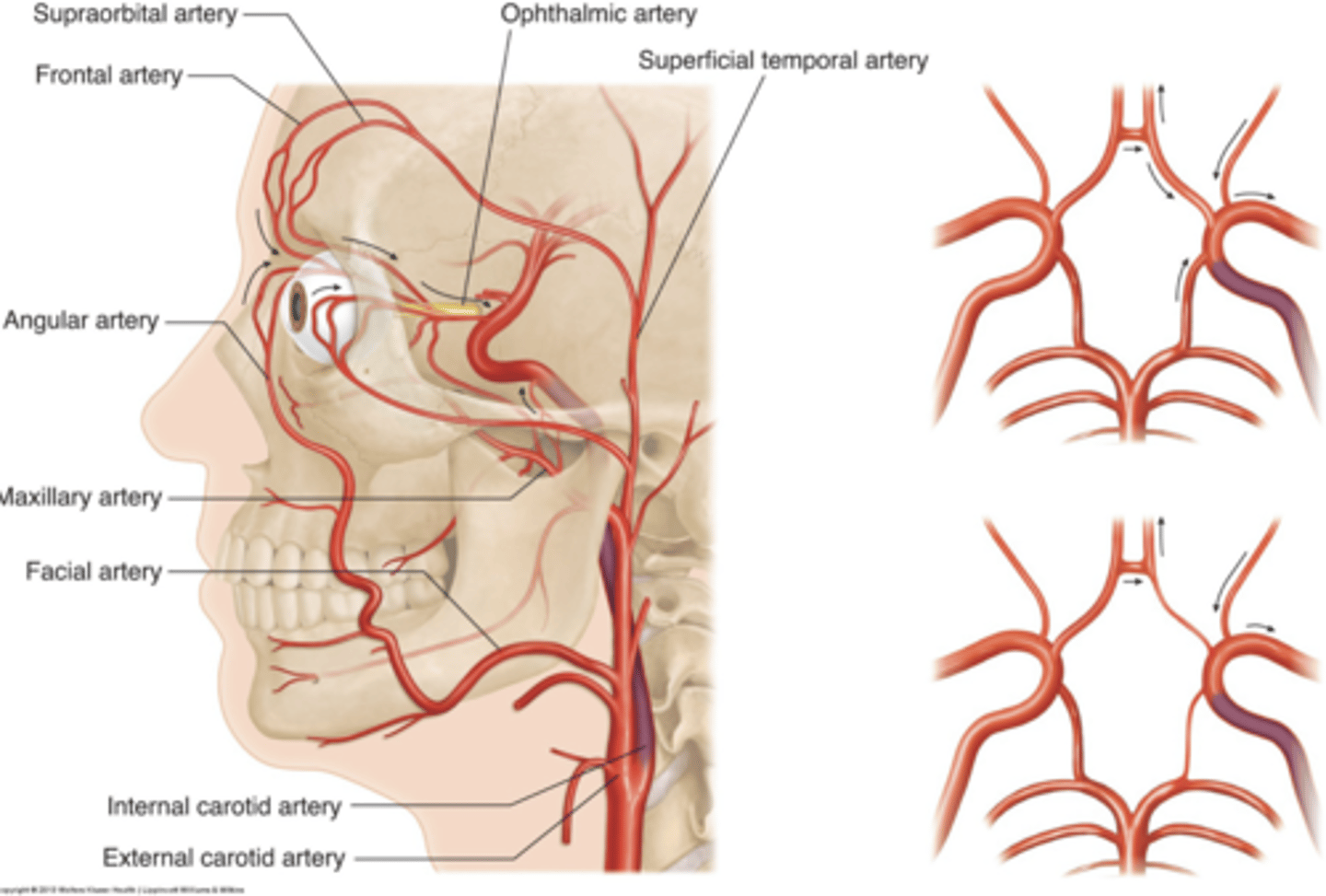
Collateral Flow Patterns of Cranial Vessels
ECA to ICA via reversed ophthalmic A
Crossover collateral via anterior communicating A
Posterior-to-anterior collateral via posterior communicating A
Disadvantages to TCD
Extracranial status
CO2 status
Intracranial pressure
Limited windows
Blind spots
Pilot error (6 month learning curve)
TCD Indications
Vasospasm - trauma or aneurysm
Vertebral basilar insufficiency
Intraoperative monitoring
Intracranial pressure
Brain death
PFO - right to left shunts
Sickle Cell
Sub arachnoid hemorrhage - head trauma, aneurysms, AVM
TCD Risk Factors
Diabetes
Hypertension
High cholesterol
Tobacco abuse
Cardiac disease or hx of heart attack
Claudication
Stroke or TIA
Previous vascular procedures - stents or bypass
TCD Relevant Patient History
Face, leg, or arm numbness, tingling, weakness
Problems speaking/understanding speech
Vision problems - blindness or double vision
Gait disturbance or leg weakness
Vertigo or fainting
Severe headaches
Equipment for Non-Imaging TDC
Dedicated non-imaging System
1-2 MHz transducer
Equipment for TDC Duplex Imaging
Ultrasound system
1-5 MHz sector transducer
