NFS 2163 Second half of the semester
1/153
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
154 Terms
What factors in body water volume
body size, body composition, gender, age, intake and output
More muscle mass and lower fat is associated with
higher water content in the body compared to lower with more fat
Body water distribution
Total body water is split into extra and intracellular fluid
there is more water in the intracellular fluid
extracellular is split into plasma-in the blood and interstitial-in between cells
fluid is constantly moving from one compartment to the other due to the presence of solutes
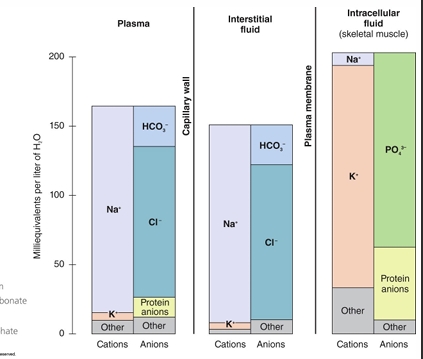
Electrolyte distribution
concentration gradient between ECF and ICF created by anions and cations
constant pressure for sodium to leak into cells and for potassium to leak out
Sodium-potassium pump maintains gradient and prevents fluid shifts under normal conditions
How does fluid shift between compartments
Hydrostatic pressure and osmotic pressure and osmolarity
Hydrostatic pressure
pressure exerted by fluid
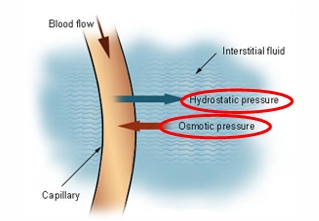
Osmotic pressure
“Pulling force” required of a solution to prevent a net movement of a solvent across a semi-permeable membrane, measured by osmolarity
Osmolarity
measures the total concentration of all dissolved solute particles (electrolytes, glucose, urea) within a liter of solution
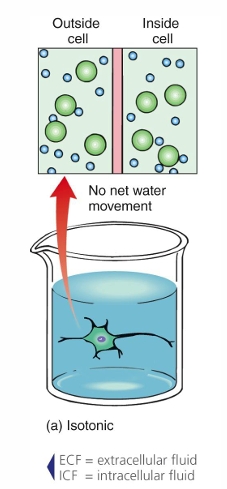
Tonicity- Isotonic
Osmolarity of ECF and ICF are the same
No osmotic pressure so no net movement of fluid
No effect on cell
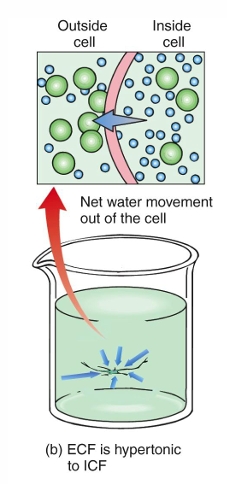
Tonicity- Hypertonic
osmolarity of the ECF is greater than the ICF
Osmotic pressure causes fluid to move out of the cell into the ECF
Cell shrinks
ICLICKER: When the ECF is hypotonic, which statement best describes how the osmolarity compares to the ICF?
The osmolarity of the ECF is less than the osmolarity of the ICF
ICLICKER: When the ECF becomes hypotonic, which direction would fluid movement occur?
Fluid would move from the ECF into the ICF
ICLICKER: When the ECF is hypotonic, what effect would this have on the size of the cell?
The cell would swell
Tonicity- Hypotonic
Osmolarity of the ICF is greater than the osmolarity of the ECF
Osmotic pressure moves fluid from the ECF into the ICF
Cell swells
What are sources of fluid input
beverages, food, aerobic metabolism
What are sources of fluid loss?
Sweat, respiration, urine
Insensible losses: ventilation and nonsweat diffusion
Sensible losses: feces, urine, sweat
Euhydration
achieving fluid balance, equal osmolarity, isotonic, no fluid shift, no effect on cells
Hyperhydration
greater ICF to ECF for osmolarity, hypotonic, Fluid shifts into the cell ECF→ICF, swell of the cell
Hypohydration related to dehydration
greater ECF to ICF for osmolarity, hypertonic, fluid shifts out of the cell ICF→ECF, shrink of the cell
ICLICKER: What is the primary source of sodium in the average American’s diet?
Processed foods
Sodium intake and excretion
UL for sodium is 2,300mg
Sodium is lost in urine, feces and sweat
Kidneys regulate sodium resorption and excretion
Training increases sodium reabsorption from sweat glands
Sodium concentration of an individual athletes sweat isn’t consistet
Acclimation to exercising in hot conditions results in more efficient sodium reabsorption over time
Higher sweat rates increase sodium concentration of sweat because sweat moves through the ducts faster and there is less time for sodium to be reabsorbed
Sweat testing can provide feedback about sweat rate and sweat composition
Maybe beneficial for “salty sweaters” and ultra-endurance athletes
Sodium for weight loss?
We don’t know what salt will do when it comes to weight loss and for your health
more salt=increased thirst=increased fluid intake=increased urine output
Study on Russian cosmonauts calls this into question
unexpected outcome was weight loss
subsequent study on mice found high-salt diet required 25% more Kcal
Potassium intake and excretion
Potassium intake
AI=4700mg/day
Potassium losses in sweat are typically small and inconsequential
odium is the primary electrolyte lost in sweat, with chloride being lost in similar amounts
Potassium losses are small and do not need to be replaced other than extenuating circumstances
Under normal conditions fluid balance is achieved through
consuming excess water
excreting excess water in the urine
kidneys reabsorb or excrete electrolytes as needed
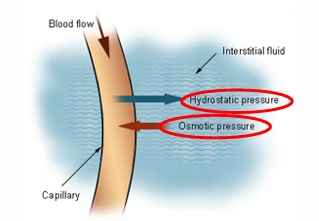
ICLICKER: What causes a decrease in plasma volume at the onset of exercise?
Hydrostatic pressure
Exercise and fluid balance
exercise challenges fluid homeostasis
Hydrostatic pressure forces fluid out of the plasma at the onset of exercise Amount of loss depends on exercise intensity
ICLICKER: Which statement regarding sweat and thermoregulation is correct?
Water evaporates from the surface of the skin, thereby cooling the body
As little as 2% dehydration can impair cognitive function and physical performance
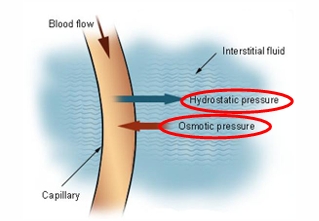
ICLICKER: When athletes lose a high volume of water through sweat, what is the impact on the tonicity of blood and muscle cells?
Blood plasma is hypertonic compared to muscle cells, causing muscle cells to shrink
Hypovolemia
loss of blood volume
Impact of hypohydration on athletic performancee
blood flow to working muscles is reduced, ability to delivery oxygen and nutrients reduced
ability to clear CO2 and waste products reduced
Decrease in VO2 max
Hypovolemia and Hyperthermia
Hyperthermia
abnormally high body temperature
ICLICKER: What determines how much we sweat?
How hot it is, intensity of exercise, amount of hydration you have yourself, illness, humidity
Regular exercise trains the body’s thermoregulation system
Water vapor in the air impedes sweat from evaporating from skin
Degree of acclimation, exercise intensity, environmental temperature, clothing/equipment
If you are well trained, then you are more likely to sweat more because your body is used to it
ICLICKER: What is the most common cause of exercise-associated muscle cramping (EAMC)?
Dehydration
Electrolyte imbalance
None of the above
None of the above
these differ from heat cramps
cause is not fully understood, but most likely due to muscle fatigue/overload
Heat cramps
Total body cramping when exercising in the heat is associated with losses of fluid and sodium
Assessing hydration status
Tracking pre and post exercise weights is more accurate
1 L of water lost = ~1kg (2.2lbs)
Not recommended for people with disordered eating
Thirst is a better indicator of hydration status than urine color, immediate alert for water need
Hypothalamus monitors blood volume and sodium osmolarity
Urine color is affected by factors other than fluid intake, reflects longer-term fluid balance
Daily hydration assessment
every morning athletes assess their thirst, urine color, body weight compared to previous morning
Pre-gaming sodium before an event
multi-day loading leads to 95%+ of sodium being excreted
Goal prior to exercise is to be adequately hydrated and consume carbohydrate if appropriate
~5-10mL/Kg 2-4 hrs before
ICLICKER: According to the American College of Sports Medicine, what is the recommendation for fluid intake during exercise?
Develop and individualized hydration plan that factors in sweat rate
Replacing more than 70% of fluid losses can result in hyponatremia
Sweat rates vary widely (~0.5-2.0L/hr), so athletes should adjust intake based on their own sweat loss
Individualized plan for hydration
Availability/access
Sweat rate and composition of sweat
Duration of exercise
Exercise intensity
Clothing and environmental conditions
Potential risk of Hypponatremmia
Hyponatremia
abnormally low concentration of sodium in the blood
Consuming excess water can result in coma or death
high sweat rate combined with high water intake causes fluid shift from ECF to ICF
Brain cells swell leading to neurological symptoms, seizures, coma and even death
Studies show endurance athletes are more likely to be
overhydrated than to be dehydrated
Hydration replenishment after training
Restore lost body water to achieve euhydration
Replace sodium and other electrolytes lost
Incorporate carbohydrate and protein for recovery when appropriate
General guidelines: 1.5L/Kg of body weight loss
Sports drink tonicity
Hypertonic, ideal for replenishment after exercise, not recommended for consumption during exercise because higher tonicity can cause digestive issues
Isotonic, ideal for hydration during endurance exercise
Hypotonic, ideal for rapid hydration/rehydration, not ideal for providing energy during exercise or replenishing glycogen after
Caffeine induced diuresis is
small
females are more susceptible to effects
exercise negates any diuretic effect
Coconut water
studies show it is no more hydrating than water
potassium and sodium content make it an inferior choice to sports drinks
Sports drinks aren’t necessary for all workouts
water is sufficient for most workouts lasting <90 minutes
Micronutrients and health
needed in small amounts, essential nutrients, both play critical roles in the body
Vitamins
organic susceptible to heat, air and acid
Minerals
inorganic, resilient to heat, air and acid
ICLICKER: Vitamin toxicities are most likely to occur with
Fat soluble vitamins
Water soluble vitamins
found in the watery portions of foods, cannot be stored in the body, CB
Fat soluble vitamins
require fat to be absorbed, stored in the liver and fat tissue, ADEK
Functionality of vitamins
energy metabolism, red blood cell formation, antioxidants, growth and developments
How much do we need of vitamins
RDA or AI- may differ based on gender and age
Tolerable Upper Intake Level (UL)- only established for 8 vitamins
The average American diet and vitamins
energy intake and nutrient density play major roles in who falls short
Athletes who consume inadequate calories are at an increased risk for deficiencies
D and E come up short the most
ICLICKER: At what point will and individual exhibit medical symptoms of a deficiency
When there is a clinical deficiency with general symptoms like fatigue and gastrointestinal distress
Clinical deficiencies were common until the mid-1900s
Fortification and enrichment
Athletes may have mild or subclinical deficiencies that impair performance
Can’t I just get tested for a deficiency
Blood levels are not indicative of storage or functionality
Testing metabolites is possible for some vitamins
A dietary assessment to determine average daily intake is the most accurate method
Too much vitamins
toxicities take months or years to develop, non-specific medical signs and symptoms, toxicities in the US are rare, mega-dosing with vitamin supplements is most common cause of toxicity
ICLICKER: Which vitamins increase energy levels
Fat soluble
B
C
None of the above
None of the above
Because there is no calories in vitamins then there is technically no energy coming from them, if the body already has enough through a normal diet then the supplement will not impact energy levels if they take a supplement
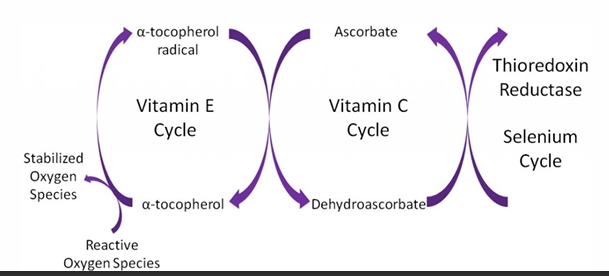
Antioxidants and free radicals
Free radical= molecules with one or more unpaired electron
Reactive oxygen species (ROS)= subset of free radicals
When exercising we release free radicals
Balance between production of ROS and clearance is key
Antioxidant systems rely on vitamins to neutralize ROS
ICLICKER: Which is a potential result of athletes mega-dosing with antioxidant supplements?
Impaired adaptation to training
Training enhances body’s antioxidant defense systems
Antioxidants at high doses impair adaptations to training and may act as pro-oxidants
Macrominerals
Microminerals
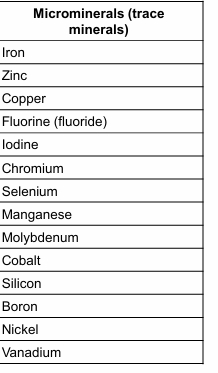
How much is enough of minerals
RDA or AI, established for 15-21 minerals, amount varies greatly but all are important, UL established for 16 minerals
Do athletes need more minerals
Factors that could increase need, Decreased absorption from GI tract, Increased loss in sweat or urine, Increased utilization due to the stress of exercise, Increased need associated with large muscle gains and maintenance, Effect of exercise is small, a healthy diet should meet needs
Americans tend to be deficient in calcium and magnesium
ICLICKER: How does the body respond when stores of a particular mineral become too low
By increasing absorption of that mineral
Mineral absorption and excretion is well regulated
In general mineral absorption is low to moderate, excretion is low
Homeostasis is maintained by adjusting absorption and excretion
If storage is high, absorption decreases and excretion increases
If storage is low, absorption increases and excretion decreases
Certain minerals compete for absorption
Excessive intake of one mineral may result in the deficiency of another
Anti-nutrients
chemically active substances in plant foods reducing their availability
Bind to nutrients thereby preventing their digestion and utilization by the body
Phytic acid, oxalate, insoluble fiber
ICLICKER: How does insoluble fiber act as an anti-nutrient
Faster transit time of food in the digestive tract
Bone health and minerals
Peak bone mass- PBM greatest amount of bone an individual can attain
Reached in late teens to early 20s
Bone is dynamic tissue going through the processes of growth, modeling, and remodeling
two primary concerns for athletes- stress fractures, and osteopenia/osteoporosis
ICLICKER: What is the biggest determinant of an individual peak bone mass
Genetics 60%
body weight, type of sport/training, energy availability, protein intake, vitamin d intake, calcium intake, loss of sodium and calcium in sweat, and hormones are the rest of it
ICLICKER: What is a health or performance consequence of a clinical iron deficiency
Reduction in VO2 max and decrease in endurance capacity
Erythrocytes
red blood cells transport O2 and CO2
Hemoglobin and myoglobin are
critical for O2 transport and storage
Effects of subclinical iron deficiency
aren’t known
Clinical deficiency of iron
VO2 max decreases 10-50% and endurance capacity is reduced
Diets low in heme iron
increase risk of deficiency
Should athletes use mineral supplements
If you eat a balanced diet then no, unless you have dietary restrictions then talk to your doctor about supplementation
Steps in diet planning
assessment, goal setting, action plan, evaluation and reassessment
Dietary assessment
Age, height, weight, gender, body composition (if available), RMR
Food recall (3-7 days), avg: energy intake, macro and micronutrient intake, and fluid intake (brand, portion size)
Type of activity, duration, frequency, intensity, based on current training cycle
Food allergies/intolerances, dietary restrictions, food likes/dislikes, food access, culinary abilities, food budget, medications/supplements
Goal setting
At least one goal in each area: athletic performance, weight and body composition, health
Action plan (dietary prescription)
individualized meal plan with an appropriate amount of calories, carbs, protein and fat
Calculations based on biometrics and information obtained in the interview
Proper amount, timing and distribution across the day of protein, carbs and fat
Emphasis on nutrient-dense foods
Supplement recommendations if appropriate
Factors in food preferences, budget, dining habits, etc
Evaluation and reassessment
Are goals being met?
Are calorie and macronutrient goals still appropriate?
Consider training periodization
Nutrition periodization = the creation of a nutrition plan to support training that has been divided into distinct periods of time
just recommendations based on mesocycle
ICLICKER: How are athlete’s macronutrient needs most accurately determined?
Using grams per kilogram of body weight
ICLICKER: The number of calories needed to maintain energy balance after the macronutrient recommendation are met is known as
Discretionary calories
Caffeine
CNS stimulant, blocks adenosine which blocks what makes you sleepy, releases calcium into muscles, muscle strength more impacted, 2+ reps on average for bench press, sleep disruptions, higher HR, major complications at 1200mg, 400mg symptoms, marketed to youth, differing amounts of caffeine in different bevs
Cannabidiol (CBD)
hemp cannabis (not THC), indirect effects like helping with sleep and pain tolerance, in drops foods and ointment, relieve stress, legal, higher doses may contain THC which is illegal, don’t buy under the table, could show up on drug tests if it contains trace amounts of THC
Platelet rich plasma therapy
patients own blood, injected into injury site, 1-3 injections, meant to accelerate healing, experimental, expensive, can vary in efficiency, no big safety concerns, discomfort pain or bruising, gray area: not regulated by a committee
Tart cherries
organic, recovery through muscle soreness, sleep, inflammation, free radicals neutralized with antioxidants, endurance, long distance, polyphenols: help produce antioxidants, blocks inflammation pathways, have natural melatonin, tryptophan= building blocks of melatonin, blocks muscle adaptation if too much, great around big events, gummies powder juice, periodization week to 5 days before, not much research, no major safety issues, can have similar effect as NSAIDs, tummy problems
Beet root
root vegetable, antioxidants, folate, potassium, vitamin C, high vasodilation properties, cardiac endurance, increased muscle contraction, mitochondrial efficiency improved, 1.5-2.5 hrs before activity, good for endurance vs short distance, moderate athletes will have more impact than advanced athletes, some risk of nitrate problems
Beta alanine
Amino acid your body makes, meat, stored in muscles, delays muscle burn, mid distance, small performance benefit, temporary tingly feeling on skin, low risk of problems
Sodium bicarbonate
baking soda, hydrogels during activity carb mix, body already makes it as a buffer for H ions, no benefit for short seconds to 8 min, no evidence for endurance athletes, GI distress, possibly can gut train for it, safety? Salt goes over sodium UL and could lead to problems like seizures, bad/banned for horses
Coconut water
young green coconuts, potassium (most prevalent), sodium, calcium, replace electrolytes, hydrates same as water, does worse than other sports drinks, 2oz for fluid of 1lb of loss, rehydration, low in sugar, high potassium (bad for people with kidney problems), good for taste, lyte hydration, no sports benefits, child labor, deforestation, plastic problems
Blood doping
high blood cell count, endurance athletes, inject themselves with hormone, inject more O2 efficient blood, blood cells live longer an prevent apoptosis, transfusion but more population in injections, UNSAFE with infection or heart attack, banned by Olympic Committee, hard to detect in small amounts, used to help increase VO2 max, very effective for endurance athletes but it is unfair
Ketones
compound developed by liver with lack of carbs, back up fuel for muscles and brain, ketogenic diet breaks down fat, increased cognitive focus, performance (endurance), uses fat already in body, inconclusive findings, not ton of information on supplementation, dependent on individual
Gatorade
Sports drink, enhances hydration, maintains blood volume, energy because of carbs, improve endurance, mental focus, better for long endurance, glucose/sucrose mix, 60+min exercise, not legal concern, marketing for all activities not just endurance, some stomach problems
Creatine
naturally occurring in skeletal and cardiac muscle, meat and fish, high intensity exercise like powerlifting, loading and maintenance phases, stay hydrated, PCr stores phosphates for when ADP needs another to make ATP, generally safe, rare events linked to excessive consumption or dehydration, good for recovery and rigorous training
What are seven macrominerals
calcium, phosphorus, magnesium, sodium, potassium, chloride, sulfur