Artificial Limbs 3
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
what are joints
joints are the areas where 2 or more bones meet (most joints are mobile, allowing the bones to move)
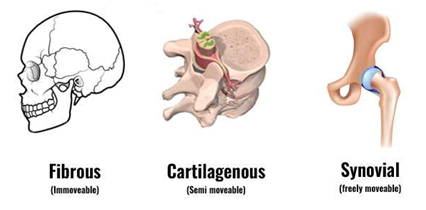
what are the 3 types of joints
synarthrosis (immovable) or fibrous
amphiarthrosis (slightly moveable) or cartilaginous
diarthrosis (freely moveable) or synovial
hip joint
a ball-and-socket joint that allows motion and gives stability needed to bear body weight (one of the most stable joints in the body)
what is the acetabulum and femur
The socket area (acetabulum) is inside the pelvis. The ball part of this joint is the top of the thighbone (femur)
what does the cartilage act as in the hip joint
the cartilage acts as a slippery coating between the ball and the socket that allows the ball to glide and rotate smoothly when the leg moves
what allows the rotational motion without any detectable translational motion
Congruity of the femoral head with the acetabulum allows the rotational motion without any detectable translational motion
what defines motion limits
The osseous anatomy of the joint & stabilizing forces of the fibrous capsule and neuromuscular anatomy defines motion limits
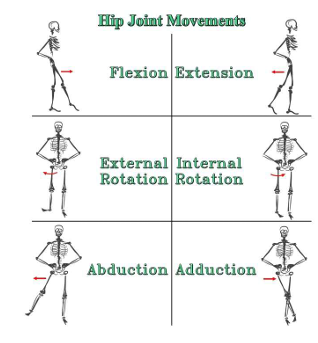
what are the degrees of flexion, extension, abduction, adduction, internal rotation, external rotation
Flexion– 120 degrees
Extension– 10 degrees
Abduction– 45 degrees
Adduction– 25 degrees
Internal Rotation– 15 degrees
External rotation– 35 degrees In
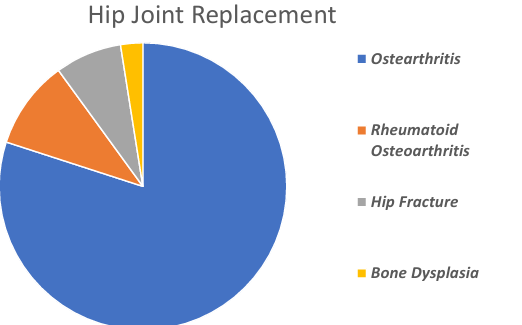
what are the 4 types of hip joint pathologies
osteoarthritis, rheumatoid arthritis, hip fracture, bone dysplasia
osteoarthritis
wear and tear arthritis
cartilage in the hip joint gradually wears away
causes: increasing age, family history, previous injury, obesity, developmental hip dysplasia
rheumatoid arthritis
autoimmune disease
causes inflammation of the synovial membrane
causes: genetics, environmental factors, hormones
hip fracture
injury
causes: older age, lifestyle, osteoporosis
bone dysplasia
when the acetabulum is too shallow to support the femoral head
congenital condition
total hip replacement surgery
The orthopaedic surgeon, upon accessing the hip joint, proceeds to extract the femoral head. They prepare the thigh bone's surface to accommodate the corresponding part of the prosthesis.
Once the articular cavity is stabilized, the surgeon readies the interior of the thigh bone to receive the prosthetic shaft
The prosthetic shaft can be affixed with or without the use of bone cement. The femoral head is affixed to the upper end of the stem
This head is positioned within acetabular component and connects directly to the liner
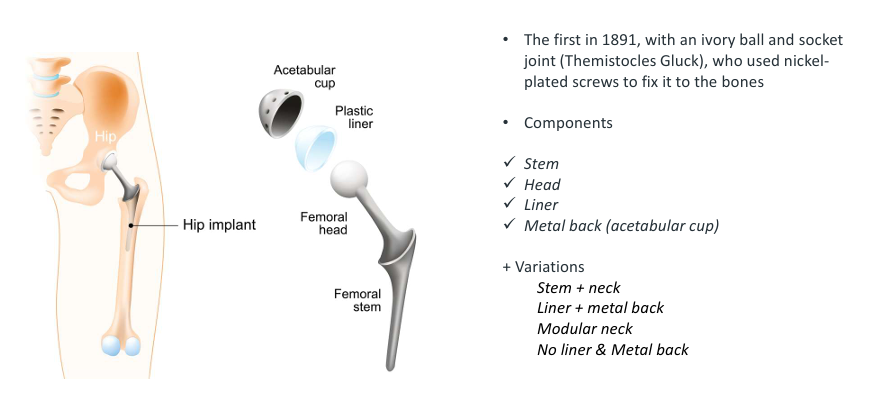
components of hip prosthesis
stem, head, liner, metal back (acetabular cup)
what can the stem be made from
stainless steel, cobaltum-chromium alloys, titanium alloys
why is stainless steel used
resistance to oxidation coupled with relative ease of machining, forming, and hardening makes stainless steel a strong candidate for material choice (however does have lower biocompatibility)
why is cobaltum-chromium alloys used
high strength, low corrosion, low wear, high Youngs modulus(however more suitable for cemented prostheses)
why are titanium alloys used
low density, high mechanical strength, excellent corrosion resistance, biocompatible (however poor wear resistance and cementless)
metal on plastic articulation (MOP)
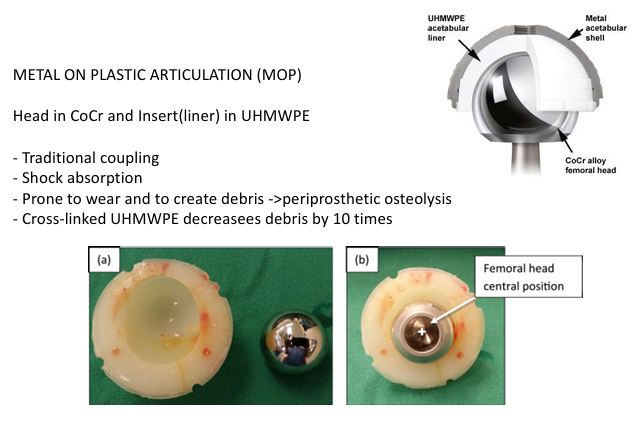
METAL ON PLASTIC ARTICULATION (MOP)
Head in CoCr and Insert(liner) in UHMWPE
Traditional coupling
Shock absorption
Prone to wear and to create debris ->periprosthetic osteolysis
Cross-linked UHMWPE decreasees debris by 10 time
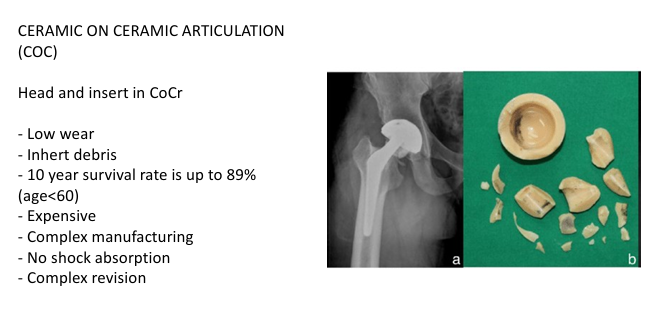
CERAMIC ON CERAMIC ARTICULATION (COC)
Head and insert in CoCr
Low wear- Inhert debris
10 year survival rate is up to 89% (age<60)
Expensive- Complex manufacturing
No shock absorption
Complex revision
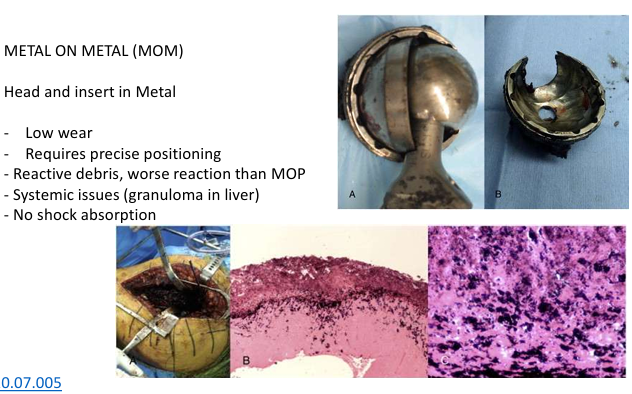
METAL ON METAL (MOM)
Head and insert in Metal
Low wear Requires precise positioning
Reactive debris, worse reaction than MOP
Systemic issues (granuloma in liver)
No shock absorption
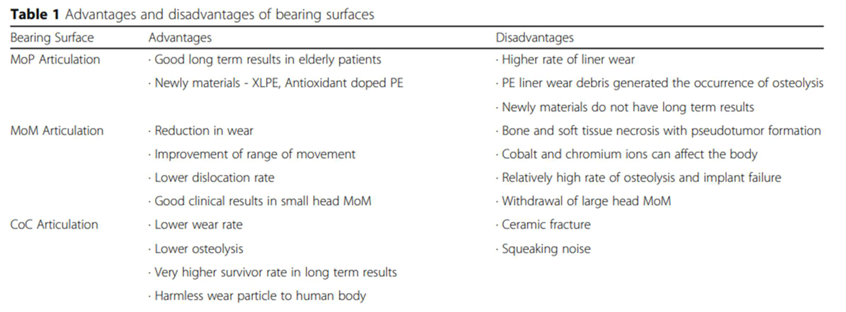
main advantages and disadvantages of bearing surfaces
see image
what is the difference of cemented vs cementless stem insertion
cemented: bone cement is used for fixing the implant to bone interface
cementless: press fit (short term), osteointegration (long term)
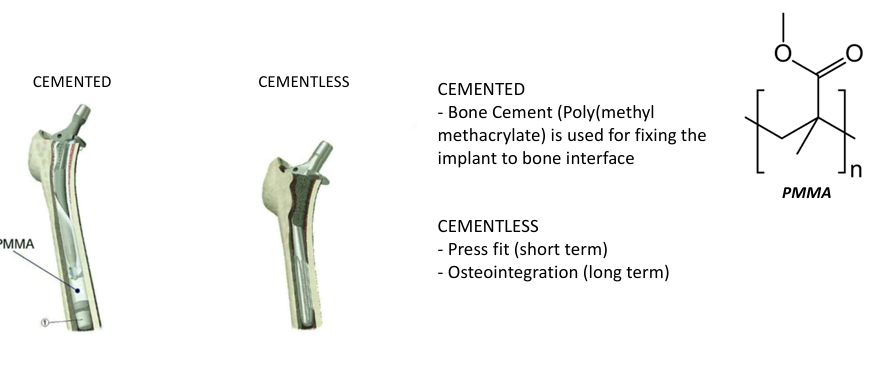
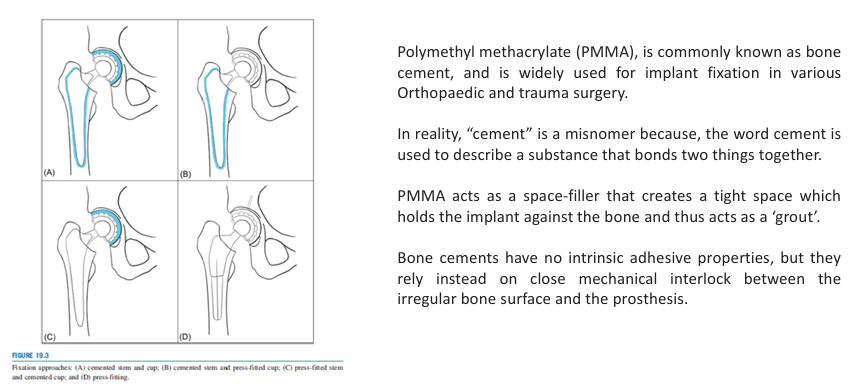
Polymethyl methacrylate (PMMA)
Polymethyl methacrylate (PMMA), is commonly known as bone cement, and is widely used for implant fixation in various Orthopaedic and trauma surgery, not really cement just substance that bonds two things together, acts as a space filler kinda like grout, not adhesive instead relies on close mechanical interlock between the irregular bone surface and the prosthesis
what are the pros of cemented stell insertion
Immediate stability
Better load distribution (if PMMA is uniformly distributed
what are the cons of cemented stem insertion
prone to long term cement fracture (due to high stress)
cement polymerisation is prone to bubbes
PMMA polymerisation is exothermal (up to 60C) which can cause bone necrosis in the first layer
large bore
what are the pros of cementless stem insertion
small bore
more stable (as per clinical evidence) if osteointegration is successful
what are the cons of cementless stem insertion
more complex procedure, very sensitive to surgical technique
what does polished surface finish do
Polished is preferred in case of cemented prostheses, since porous coating can cause fracture in the cement layer and lead to aseptic loosening
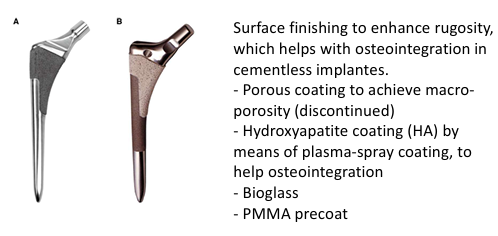
what does surface finishing enhance
Surface finishing to enhance rugosity, which helps with osteointegration in cementless implantes.
Porous coating to achieve macro porosity (discontinued)
Hydroxyapatite coating (HA) by means of plasma-spray coating, to help osteointegration
Bioglass
PMMA precoat
short term complications of hip joint replacements
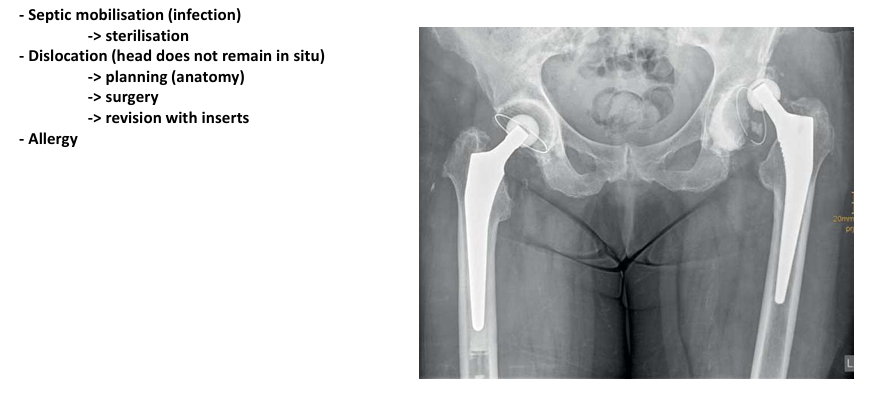
septic mobilisation
dislocation
allergy
medium term complications of hip joint replacements
structural failure
aseptic mobilisation
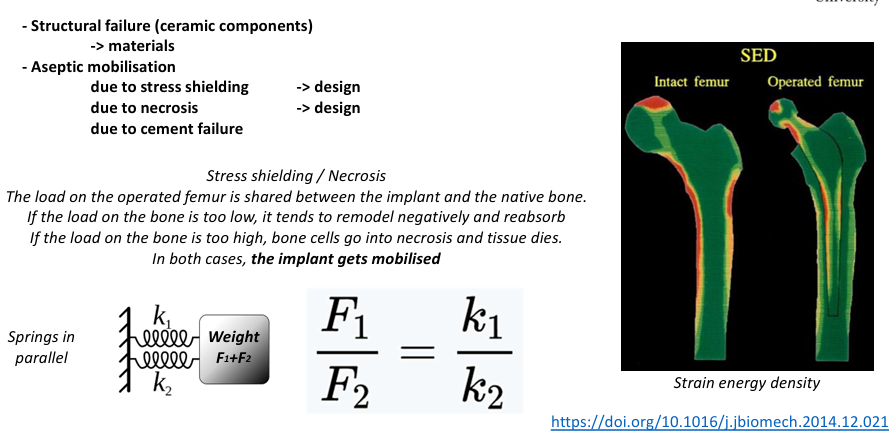
how can the implant be mobilised through stress shielding/necrosis
The load on the operated femur is shared between the implant and the native bone. If the load on the bone is too low, it tends to remodel negatively and reabsorb If the load on the bone is too high, bone cells go into necrosis and tissue dies. In both cases, the implant gets mobilised
long term complications of hip joint replacements
fatigue
osteolysis
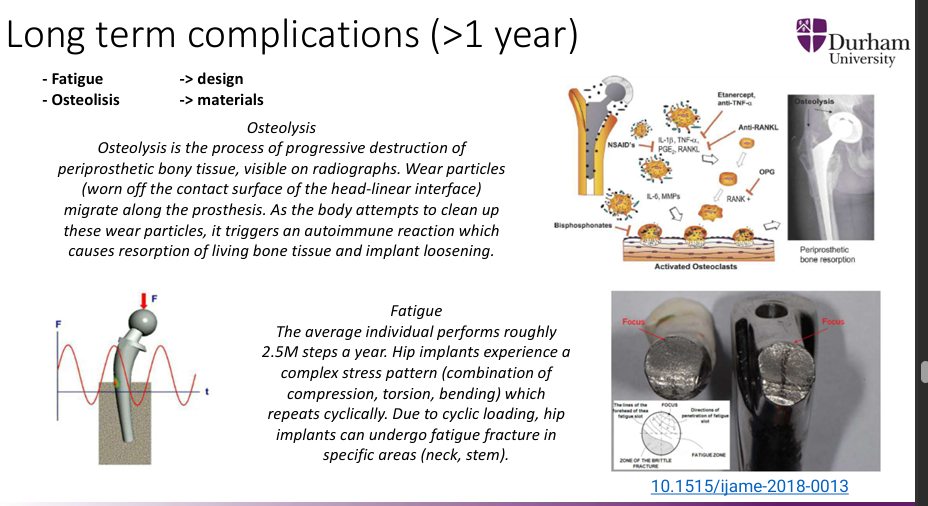
Osteolysis
Osteolysis is the process of progressive destruction of periprosthetic bony tissue, visible on radiographs. Wear particles (worn off the contact surface of the head-linear interface) migrate along the prosthesis. As the body attempts to clean up these wear particles, it triggers an autoimmune reaction which causes resorption of living bone tissue and implant loosening.
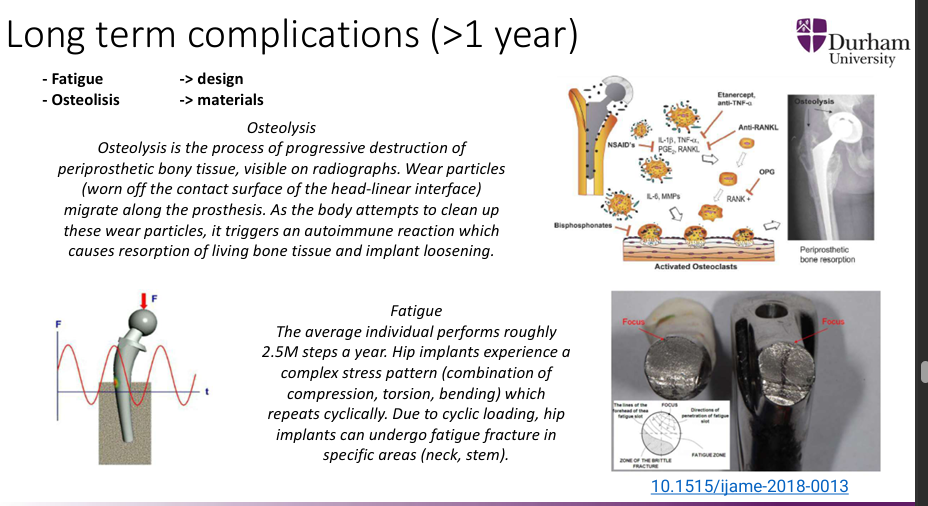
fatigue
The average individual performs roughly 2.5M steps a year. Hip implants experience a complex stress pattern (combination of compression, torsion, bending) which repeats cyclically. Due to cyclic loading, hip implants can undergo fatigue fracture in specific areas (neck, stem).

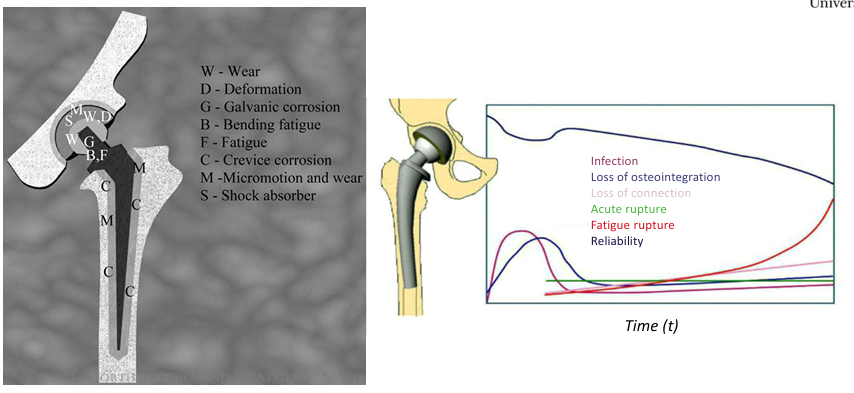
what is W,D,G,B,F,C,M.S
W=wear
D=deformation
G=Galvanic corrosion
B=bending fatigue
C=crevice corrosion
M=micromotion and wear
S=shock absorber
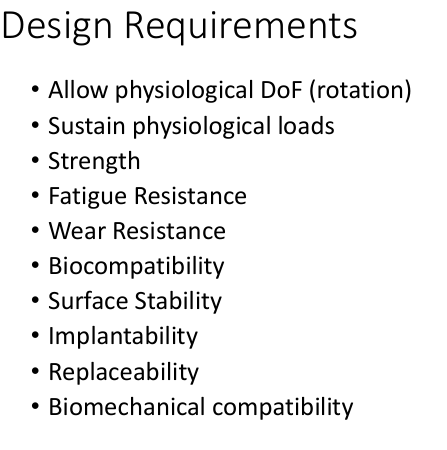
what are the design requirements for a hip joint replacement
Allow physiological DoF (rotation) (biomechanical)
Sustain physiological loads (biomechanical)
Strength (mechanical)
Fatigue Resistance (mechanical)
Wear Resistance (mechanical)
Biocompatibility (biomechanical)
Surface Stability (biomechanical)
Implantability (surgical)
Replaceability (surgical)
Biomechanical compatibility (biomechanical)
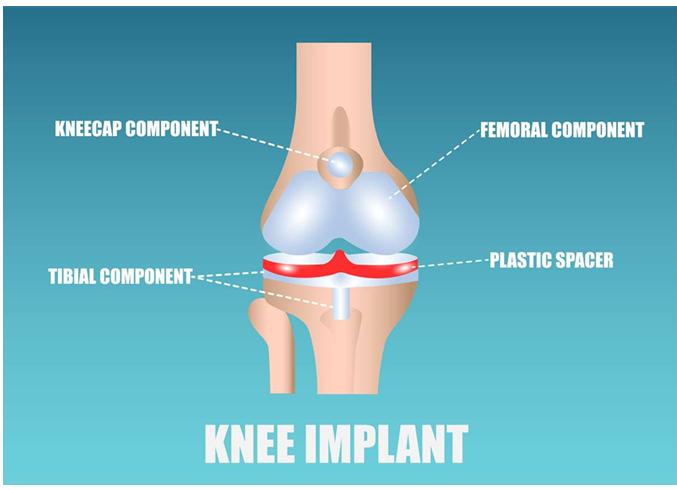
what are the components are in a knee plant
kneecap component, femoral component, tibial component, plastic spacer
what is the material of the femoral component
CoCr alloy, Ti alloy, Oxinium, ceramic
what is the material of the tibial insert
UHMWPE
what is the material of the tibial component
CoCrMo alloy, Ti alloty UHMWPE
what is the material of the patellar compoent
UHMWPE