malignant diseases
1/52
Earn XP
Description and Tags
lecture given 6/8/2026
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
what are the general properties of malignancies?
uncontrolled growth of tissue, locally invasive, able to metastisize to lymph nodes or distant sites
*displaced teeth, loosened teeth over short time, ulceration, indurated or rolled border, exposure of underlying bone, lymphadenopathy, hemorrhage, lack of normal healing, pain and swelling, pathologic fractures
M>F, >50 yo
what are the common locations of malignancies?
tongue, floor of the mouth, tonsillar area, lip, soft palate, gingiva, may invade jaws, sarcomas of both jaws
metastatic tumors: posterior mandible and maxilla, some at apices or in follicles
what are the imaging modalities for malignancies?
intraoral- best resolution, reveals subtle changes
panoramic- quick, overall assessment, anatomical information (boundaries of maxillary sinuses)
CBCT- 3D analysis to better determine extent of tumor
PET- detects cellular metabolic activity, can be fused with MDCT for accurate localization
MRI- 3D soft tissue images showing perineural spread and involvement of lymph nodes
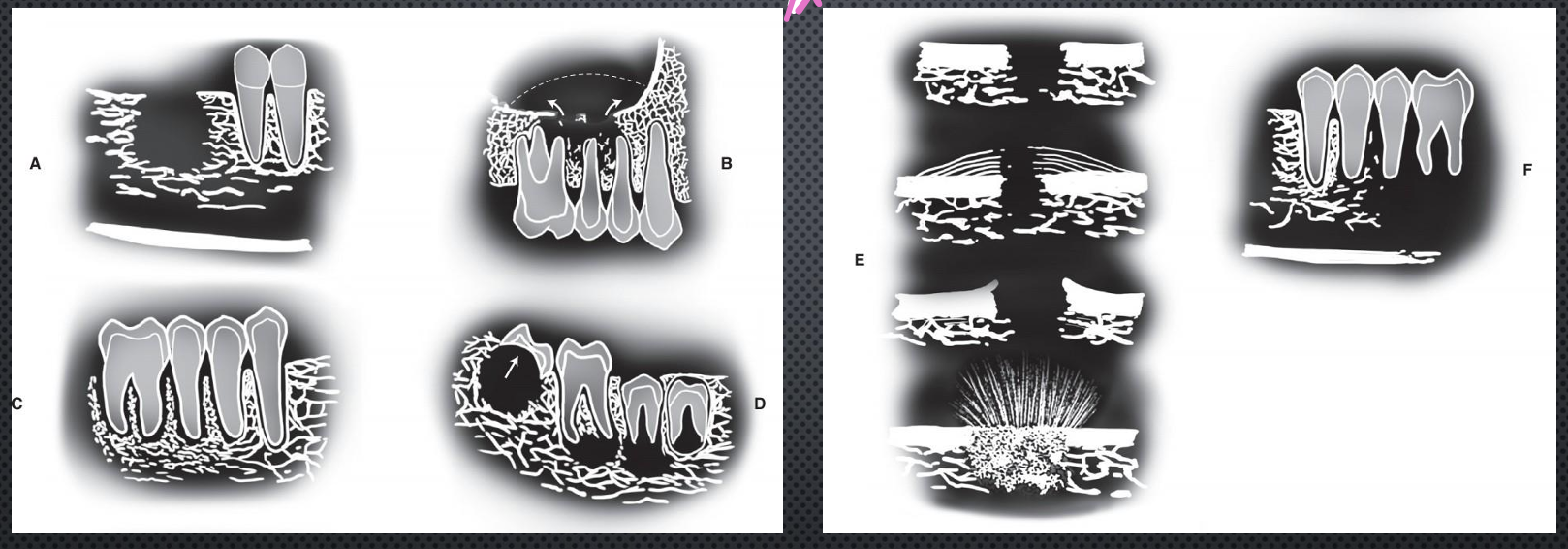
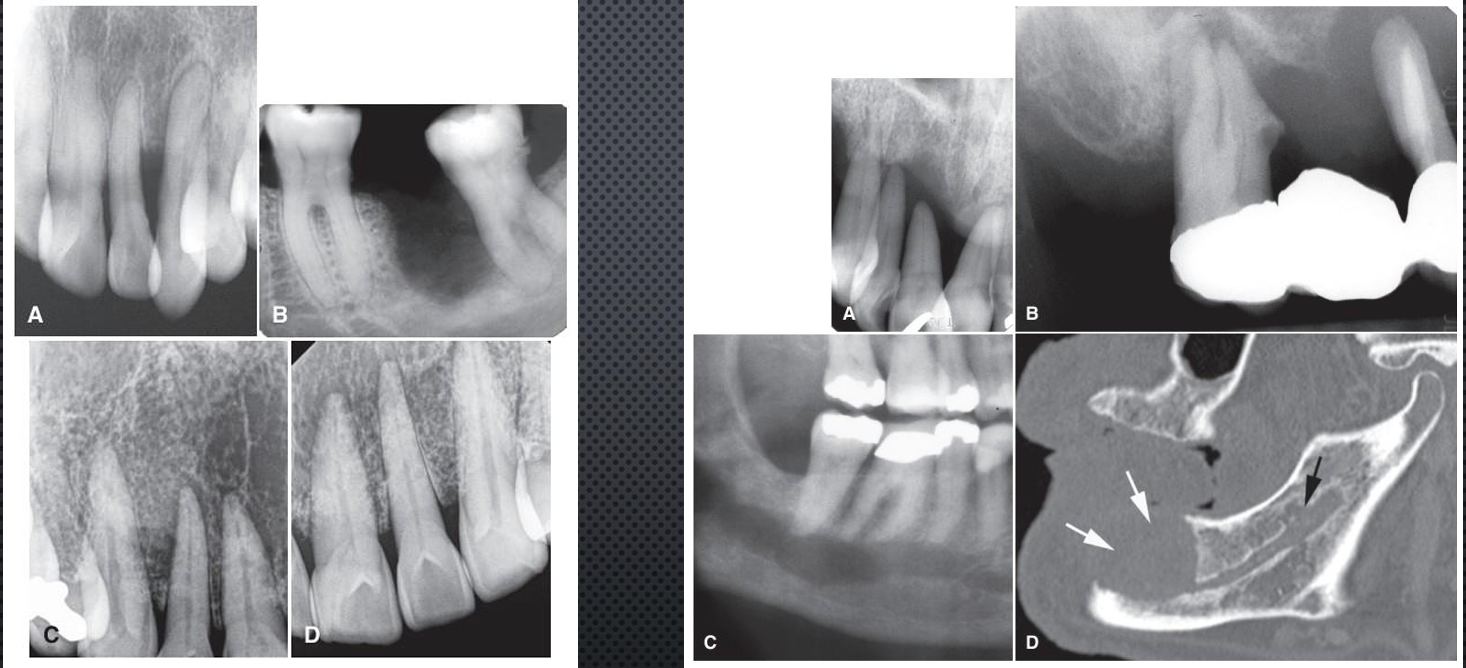
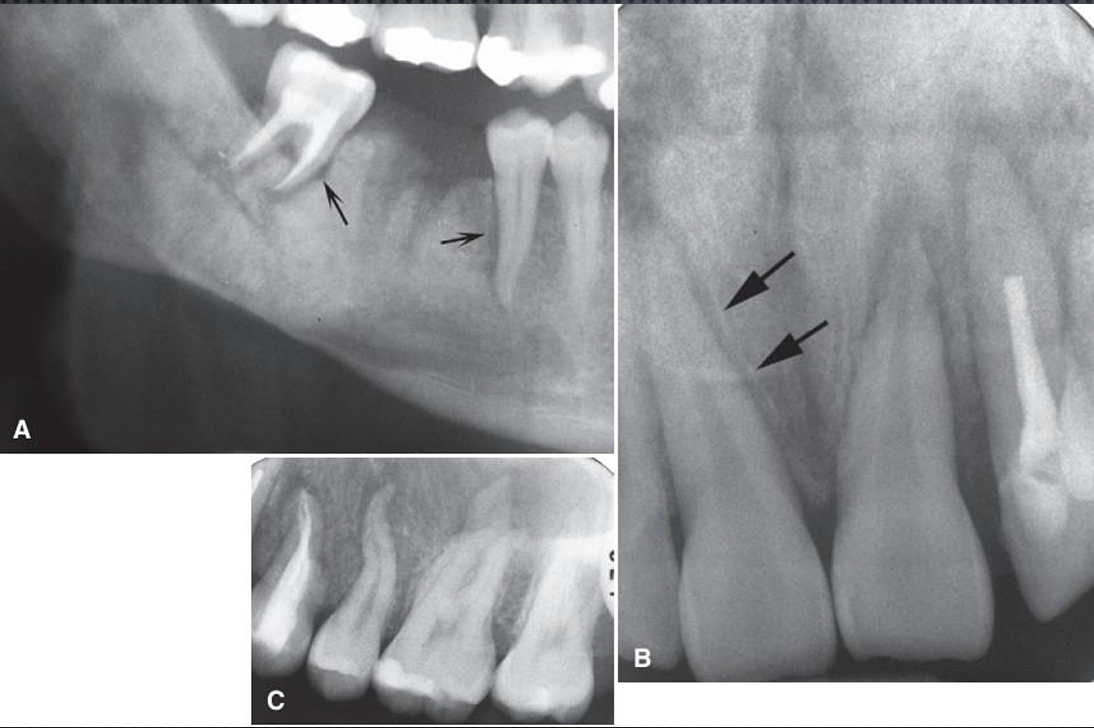
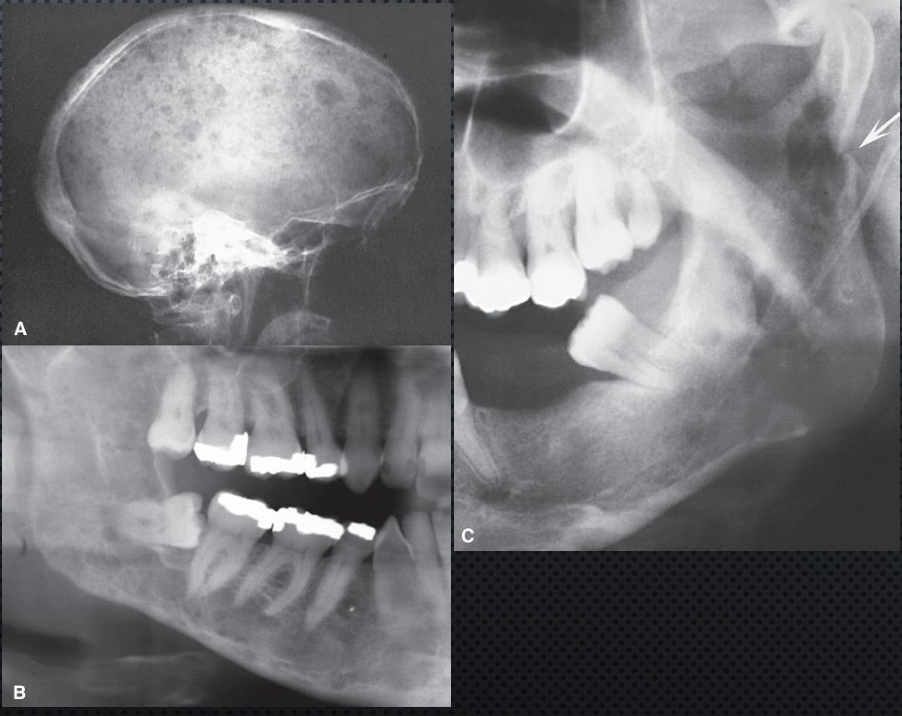
A?
ill defined invasive borders followed by bone destruction
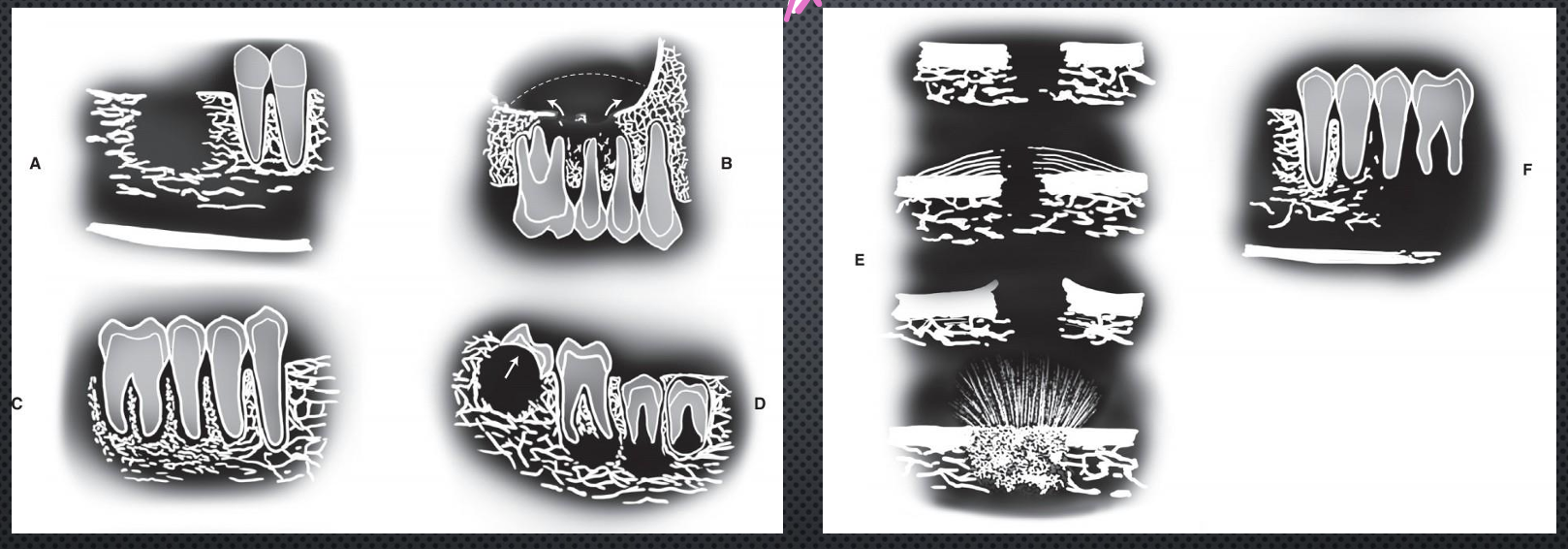
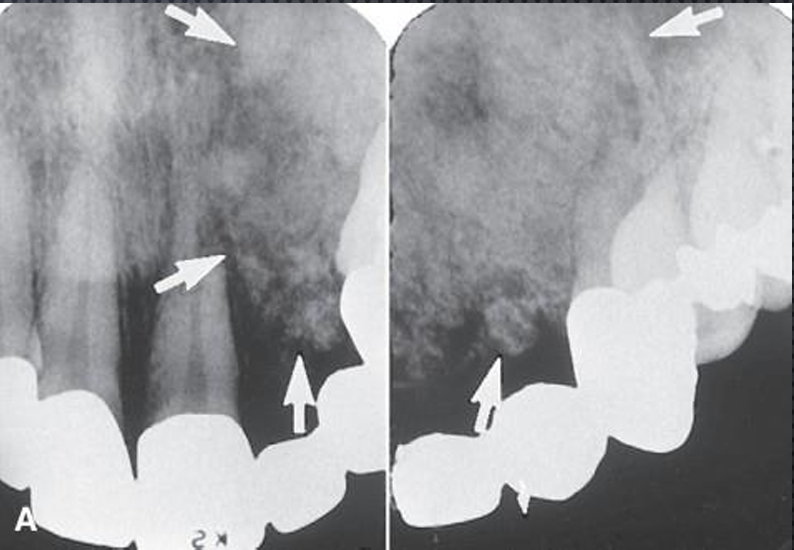
B?
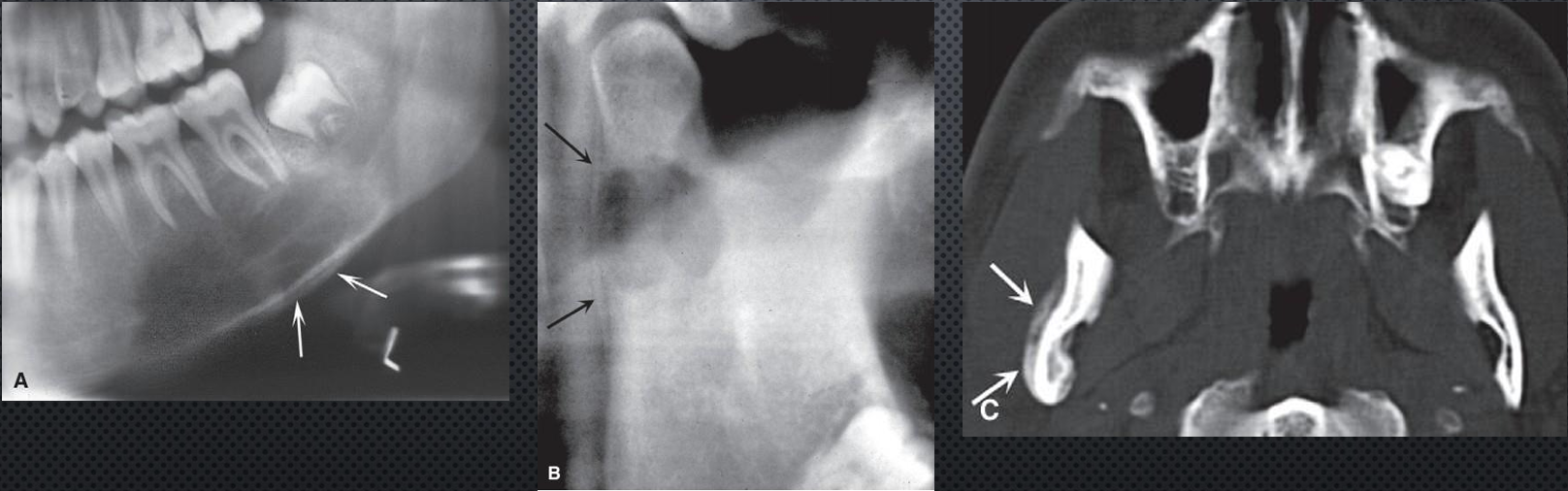
destruction of the cortical boundary (floor of the maxillary antrum) with an adjacent soft tissue mass (arrows)
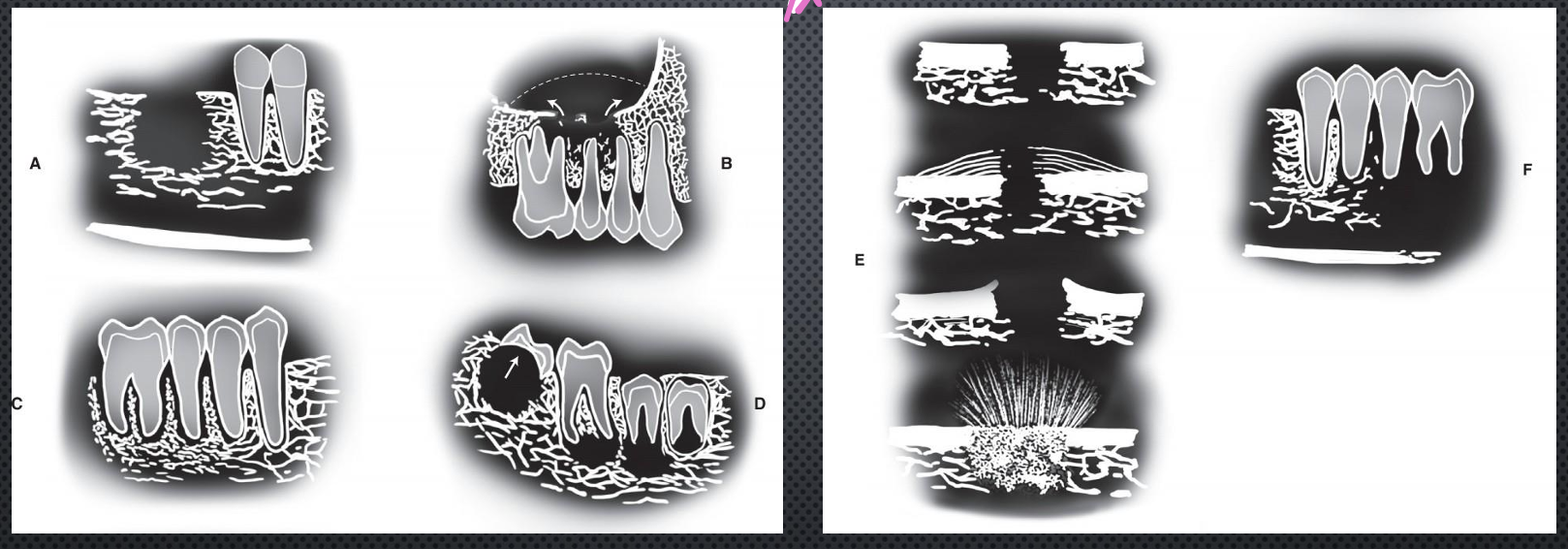
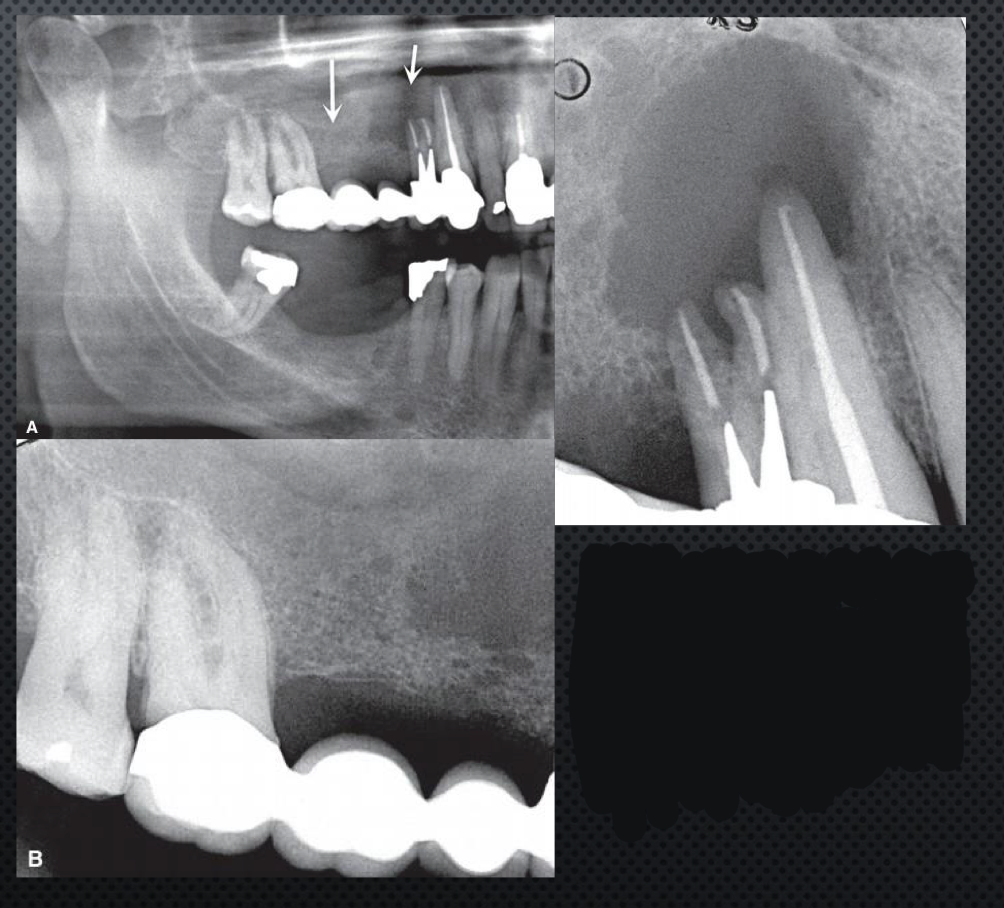
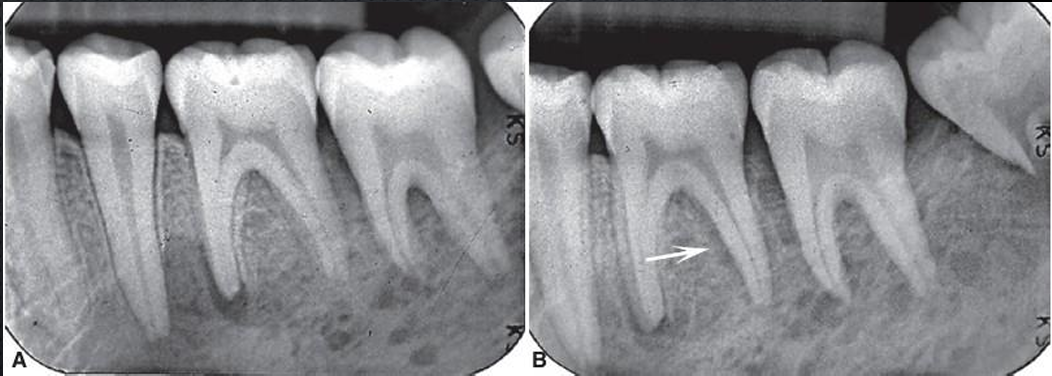
C?
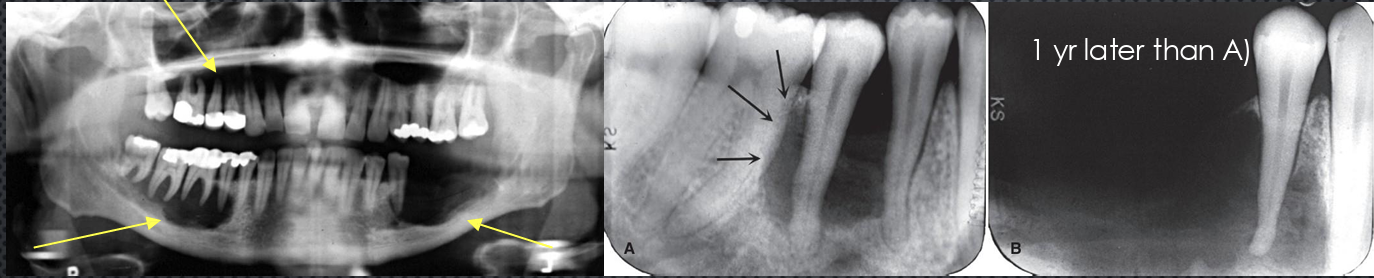
tumor invasion along the periodontal membrane space causing irregular thickening of this space
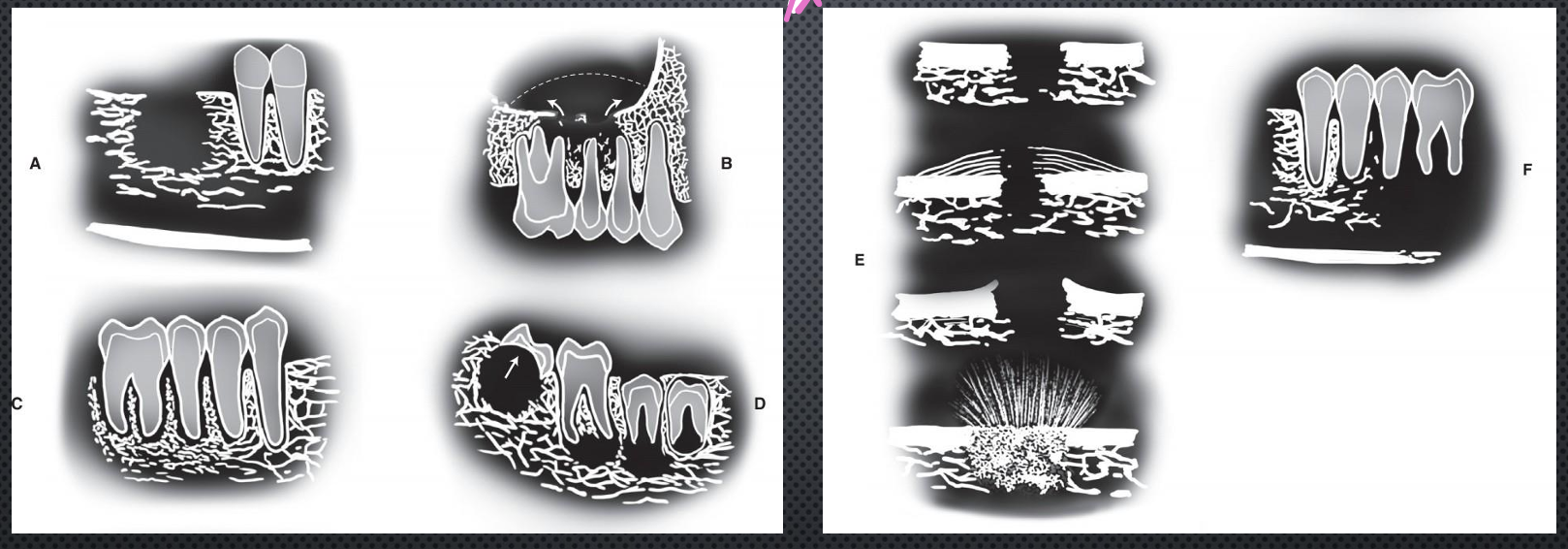
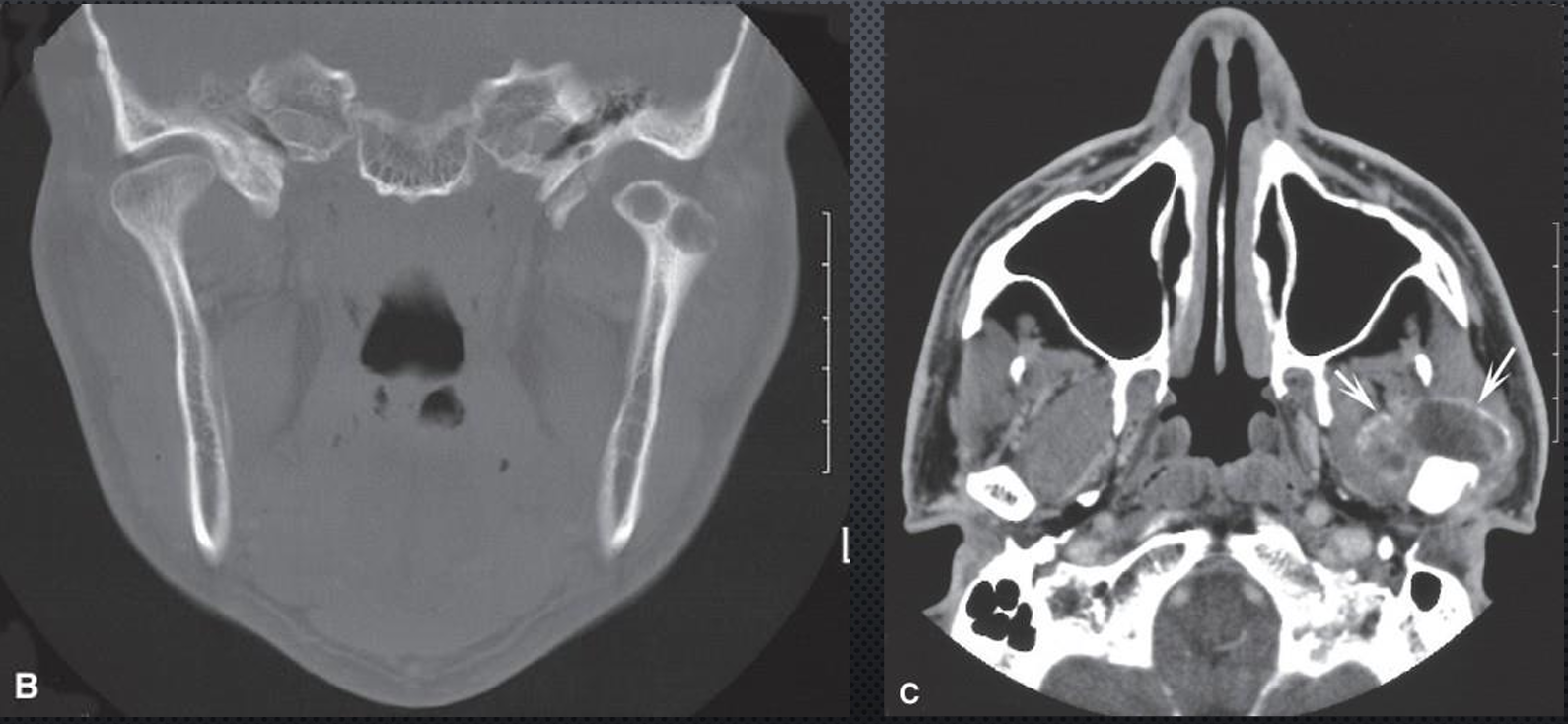
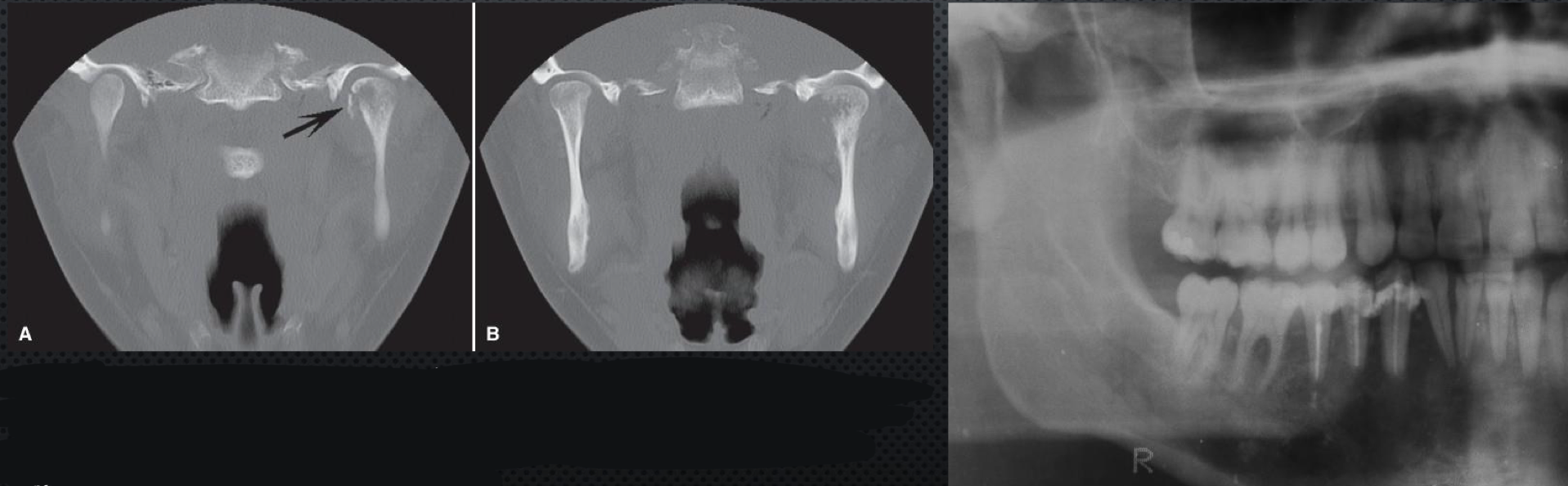
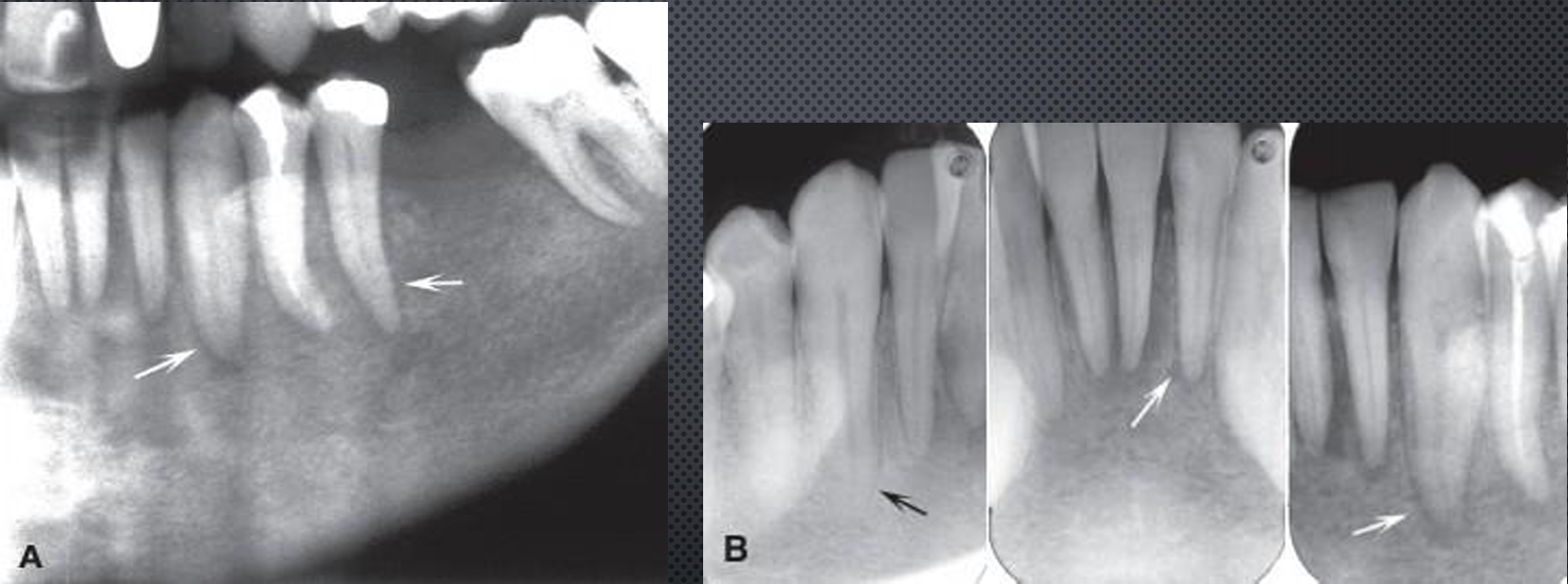
D?
multifocal lesions located at root apices and in the papilla of a developing tooth destroying the crypt cortex and displacing the developing tooth in an occlusal direction
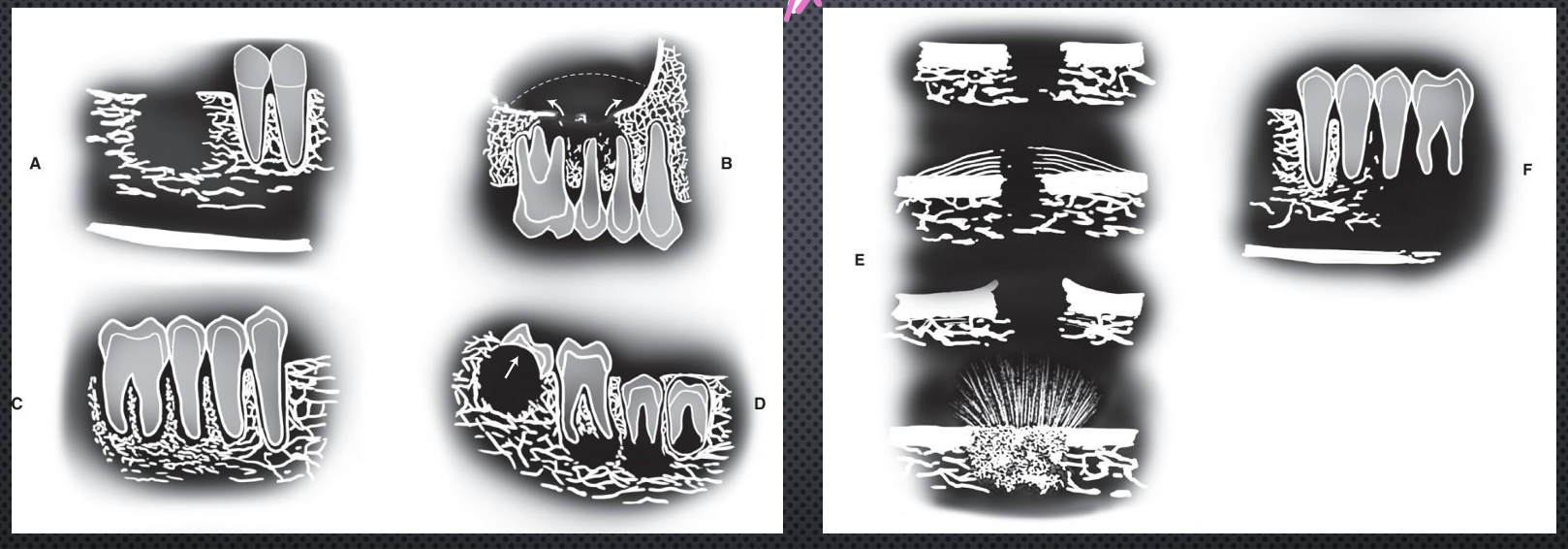
*E?
4 types of effects on the cortical bone and periosteal reaction
cortical bone destruction without periosteal reaction
laminated periosteal reaction with destruction of the cortical bone and the new periosteal bone
destruction of cortical bone with periosteal reaction at the periphery forming **Codman’s triangles
**a spiculated or sunray type of periosteal reaction
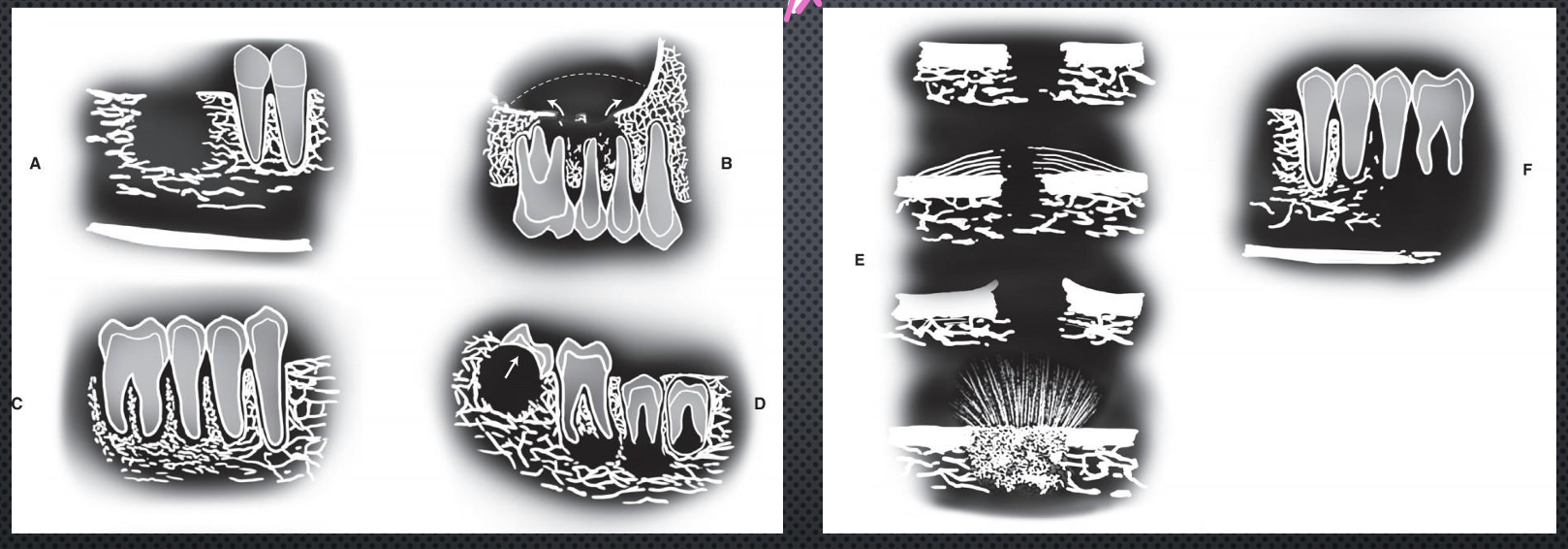
F?
bone destruction around existing teeth, producing an appearance of teeth floating in space
what are general features of malignancies on radiographs?
ill defined, irregular, non-corticated, infiltrating
radiolucent, radiopaque
rapidly destructive- destroy bone but leave teeth or resorb roots, destroy cortices, follow path of least resistance
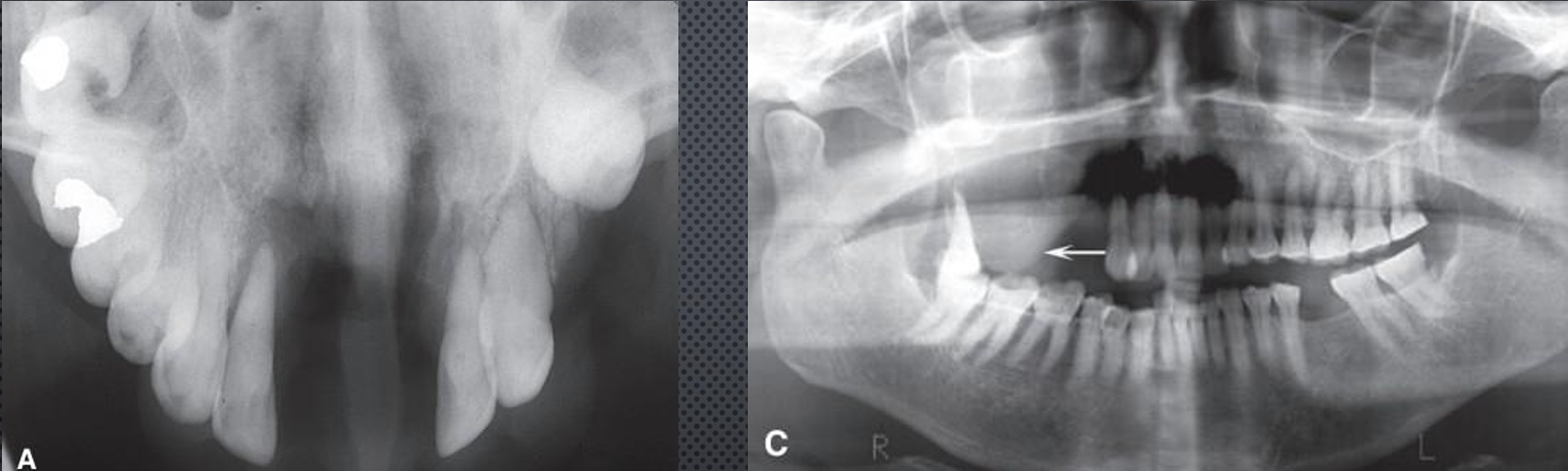
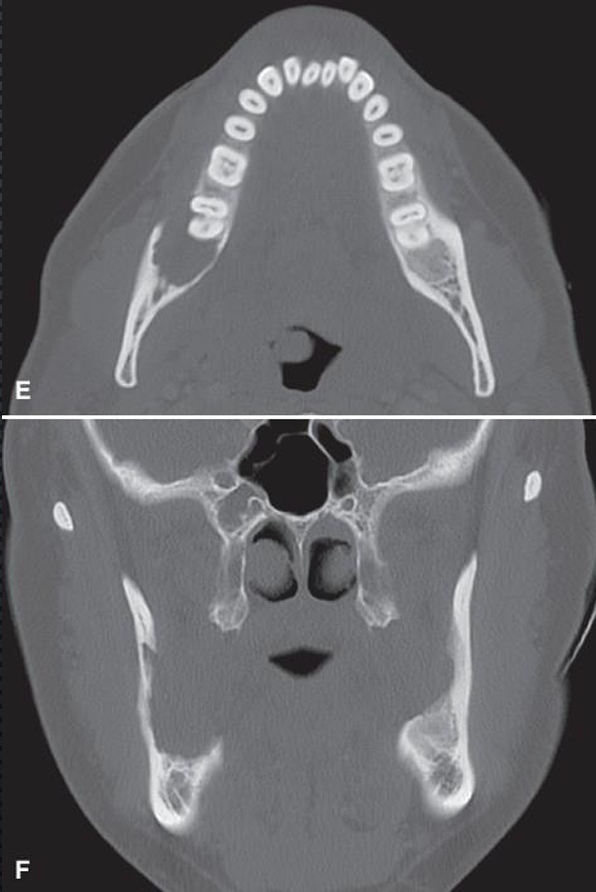
squamous cell carcinoma arising in soft tissue
arises from surface epithelium, smoking/alcohol/papilloma viruses play a role
red or white, irregular patchy lesions, variable pain, lymphadenopathy, significant weight loss, feel unwell
lateral tongue, invades bone
irregular outline, ill defined, non-corticated, sclerosis from secondary infection may occur
irregular PDL widening → teeth floating → teeth drifting, increased width and cortical destruction of mandibular canal, other cortices

squamous cell carcinoma arising in soft tissue
squamous cell carcinoma arising in the soft tissue
squamous cell carcinoma arising from soft tissue
squamous cell carcinoma arising from soft tissue
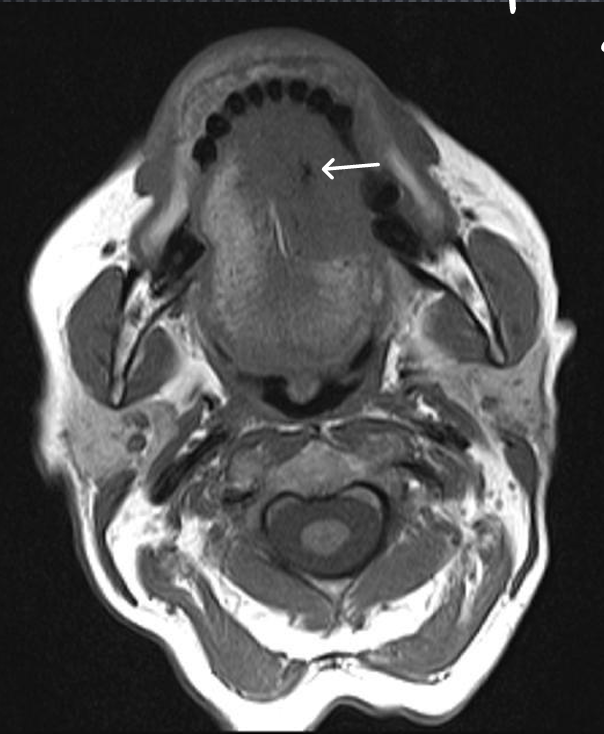
*is this T1 or T2 image, and what is the white arrow pointing to?
T1, evidence of necrosis
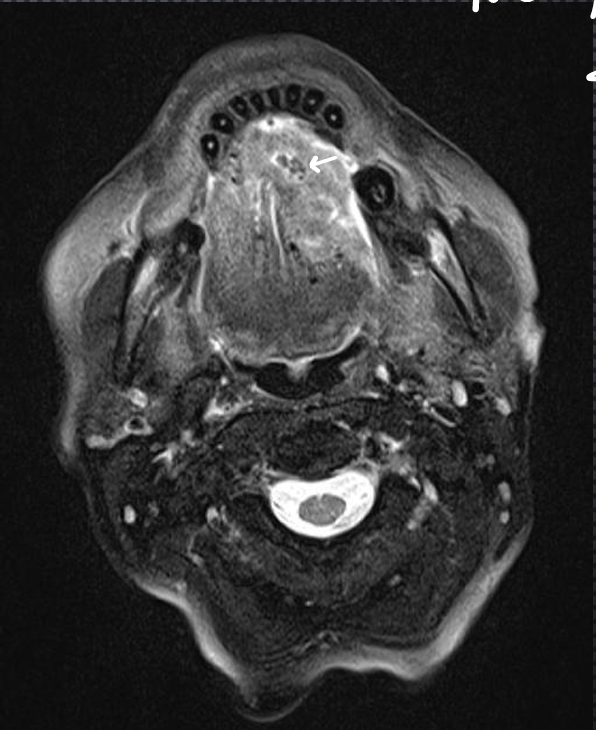
*is this T1 or T2, and what is the itty bitty white arrow pointing at?
T2, evidence of inflammation
squamous cell carcinoma arising in bone
remnants of odontogenic epithelium, no connection with surface epithelium
clinically: rare, pain, pathological fracture
M>F, 4-8th decade
imaging features: mand > max, molar region, ragged border
radiolucent
destruction of adjacent structures

squamous cell carcinoma arising in bone
squamous cell carcinoma arising in bone
squamous cell carcinoma arising in cyst
uncommon, arise from inflammatory periapical, residual, dentigerous, and odontogenic keratocystic
dull pain, swelling
imaging features: early- cystic, later turns into malignancy
mand, anterior max
characteristic of cyst and malignancy
DD: inflamed cysts show peripheral sclerosis

squamous cell carcinoma arising in a cyst
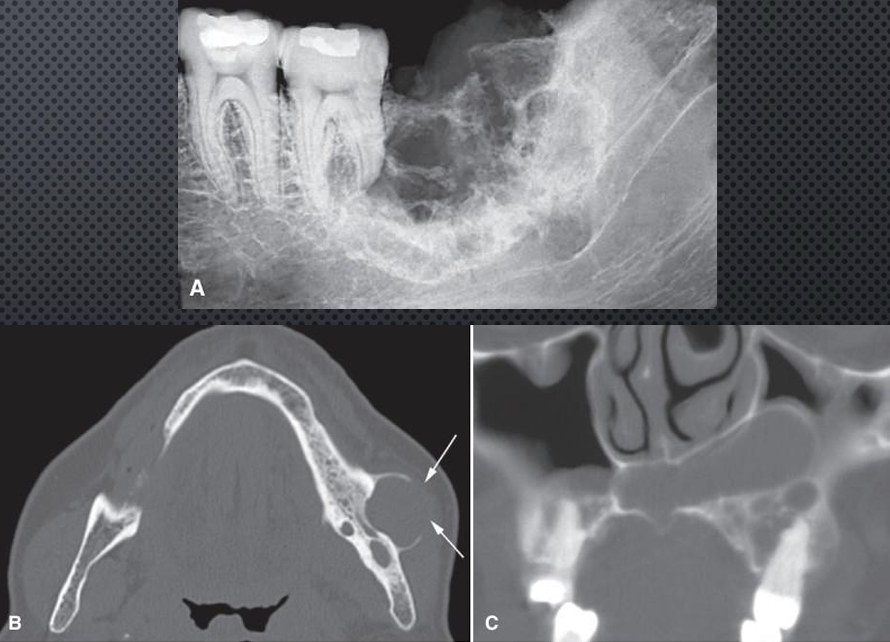
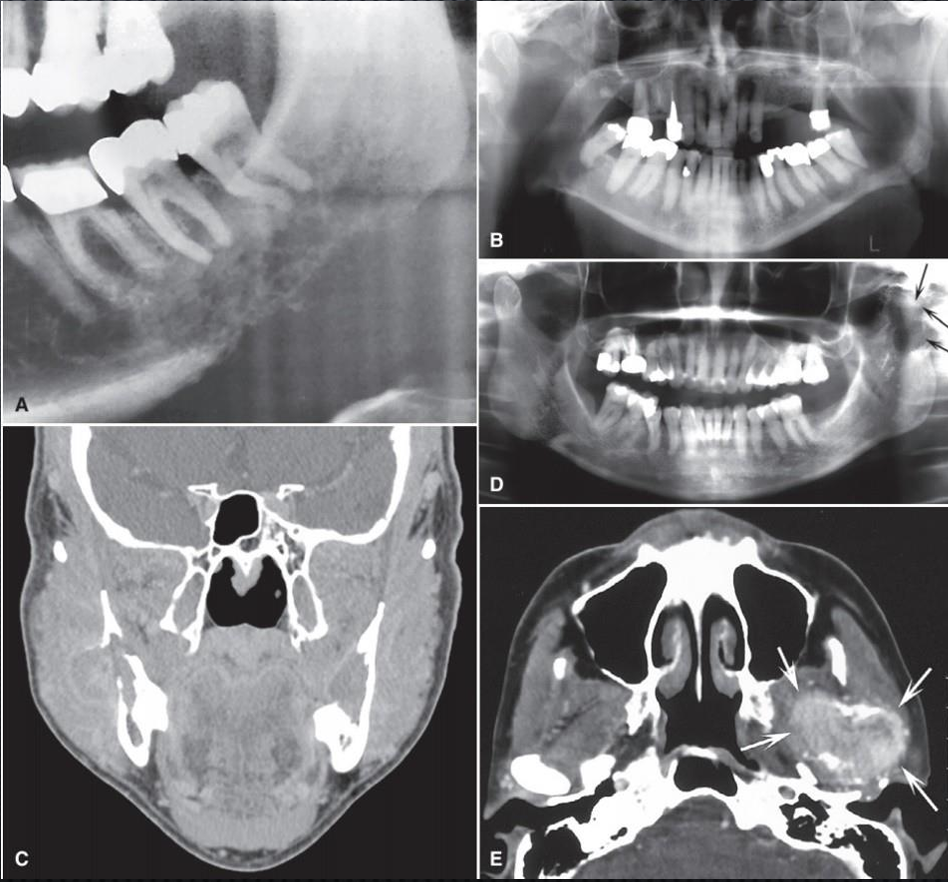
squamous cell carcinoma arising in the max sinus
risk factors: chronic sinusitis, inhaling manufacturing chemicals
african, asian, M>F, sinus symptoms
opacification of the sinus, destruction of borders
squamous cell carcinoma arising in the maxillary sinus
central mucoepidermoid carcinoma
mimic benign tumor or cyst, painless swelling, F>M
mand:max 4:1, posterior, above canal
well defined and corticated
uni or multilocular, expansile, resorbs cortices, does not affect teeth, displaces canal
DD: myxoma, CGCG
central mucoepidermoid carcinoma
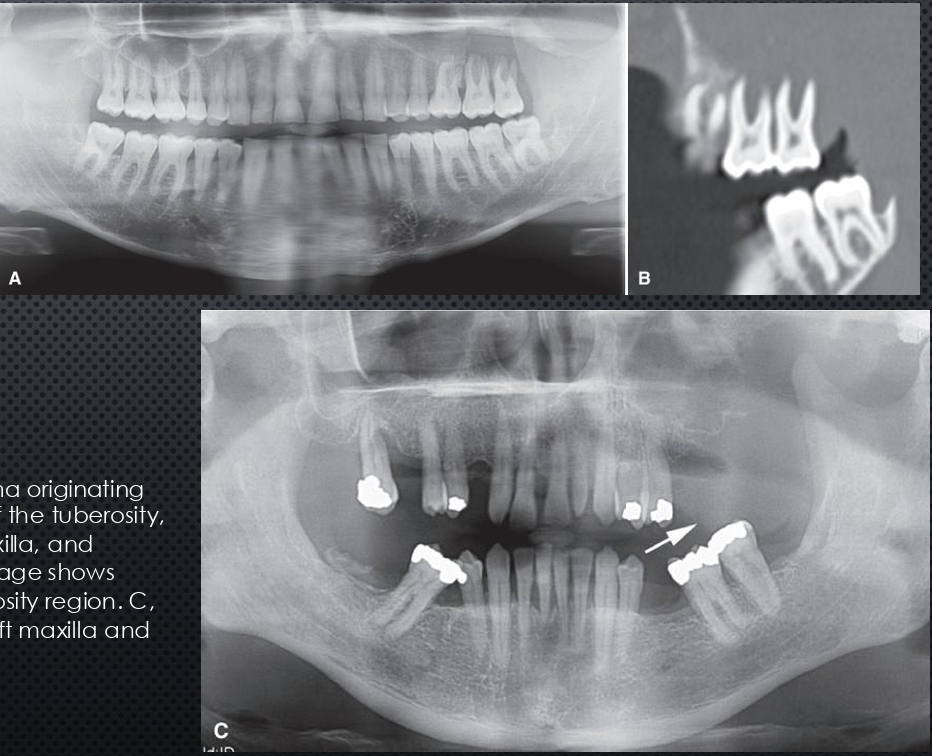
metastatic tumors
secondary malignancy, tumor spreads via blood vessels, typically carcinoma
breast 31%, lung 18%, kidney 15%, thyroid 6%, prostate 6%, colon and rectum 6%, stomach 5%, melanoma 5%, testicle/bladder/liver/ovarian/cervical
F>M 2:1, dental pain, paresthesia, bleeding
post mand, max sinus, hard palate, condyle, PDL, mimicking PARL, maybe defined, non-corticated,
breast and prostate stimulate bone formation- patchy sclerosis, may cause spiculated periosteal reaction
metastatic tumors
*
metastatic tumors
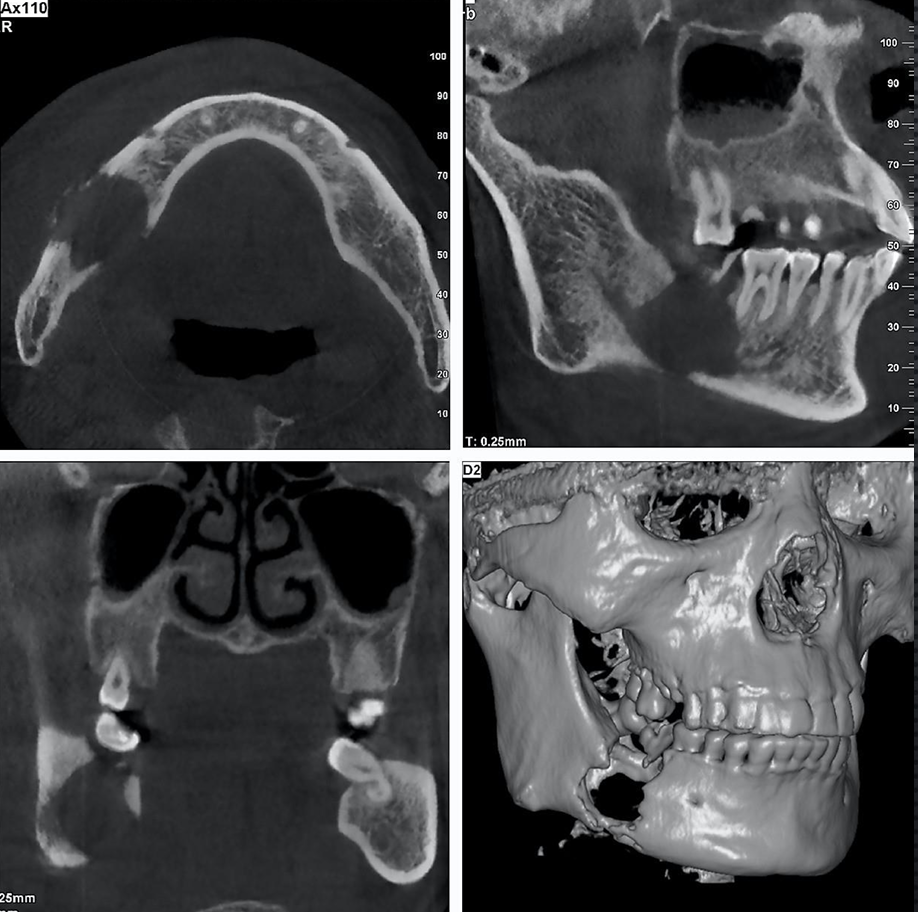
osteoscarcoma
osteoid is produced directly by tumor
M>F 2:1, peaks in 4th decade, rapid swelling, pain, tenderness
posterior mand, max, may cross midline
ill defined, radiolucent/radiopaque, periosteal reaction, destruction of cortices

*
osteoscarcoma
osteosarcoma
chondroscarcoma
slow growing malignant tumor that produces cartilage and tends to calcify
any age, more common in adults, mean age 47, M=F, long duration firm mass, near TMJ can affect joint function
mand = max, anterior, condylar head and neck, coronoid process
well defined, can be corticated, but can be ill defined, invasive, expands cortices, possibly large
mixed radiolucent/radiopaque
root resorption and displacement, widened PDL space
chrondrosarcoma
chrondrosarcoma
*ewing’s sarcoma
small round cell tumor that arises in medullary portion of bone and spread to cortex
common in second decade, age 5-30, M>F 2:1
mand > max, posterior, never corticated, ragged border, radiolucent periosteal bone formation, **codman’s triangle, destroys bone and cortices
ewing’s sarcoma
fibroscarcoma
malignant fibroblasts that produce collagen and elastin
M=F, 4th decade, enlarging mass, pain
mand premolar-molar region, ill defined, ragged
grow along bone through marrow space, sclerosis of adjacent bone, radiolucent, destroy bone and cortices

fibrosarcoma
mutliple myeloma
systemic malignancy of plasma cells, single lesions are called plasmacytoma
35-70 yo, M>F, fatigue, weight loss, bone pain, anemia
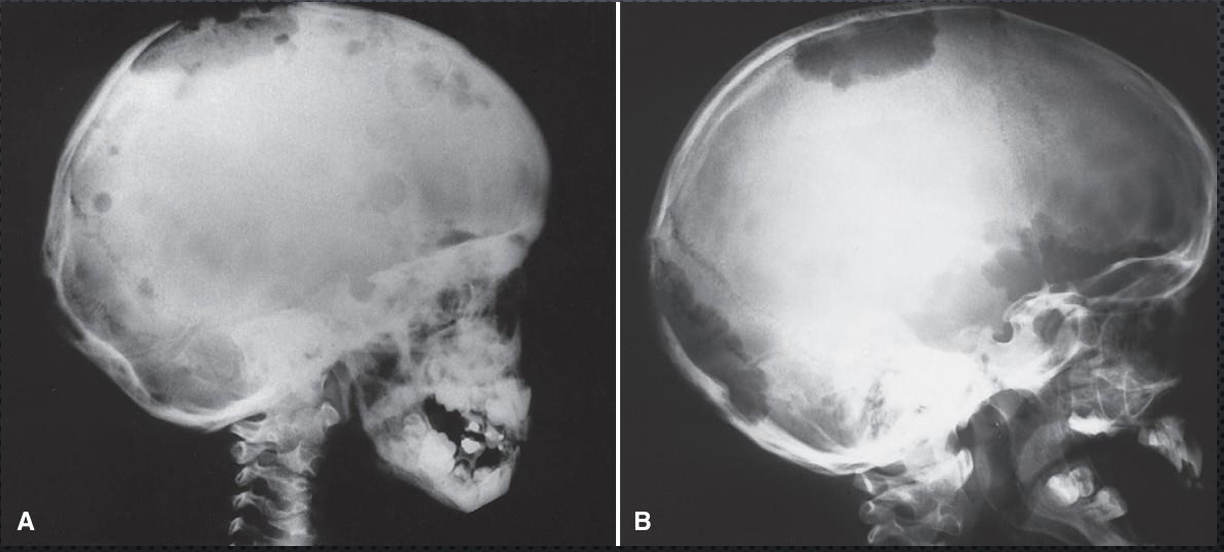
mand > max, posterior, well defined, non-corticated, **punched out, may be ragged and infiltrative, radiolucent, rarely root resorption, resorbs cortices
multiple myeloma

multiple myeloma
non-hodgkin’s lymphoma
malignant tumor of lymphatic cells, typically found in lymph nodes but can appear extranodal
all age groups, rare under 10, feeling unwell, night sweats, swelling
maxillary sinus, posterior mand and max, ill-defined, invasive, radiolucent, effacted sinus walls, soft tissue mass visible, destroys cortices, propensity to grow in PDL space, displaces developing teeth occlusally
non-hodgkin’s lymphoma
non-hodgkin’s lymphoma
leukemia
malignancy of hematopoietic stems cells
acute: bimodal (so very young or very old), feeling unwell, bone pain
seen around PA of developing teeth in children, ill defined, patchy radiolucencies that can enlarge
no expansion, teeth displaced occlusally

leukemia
leukemia
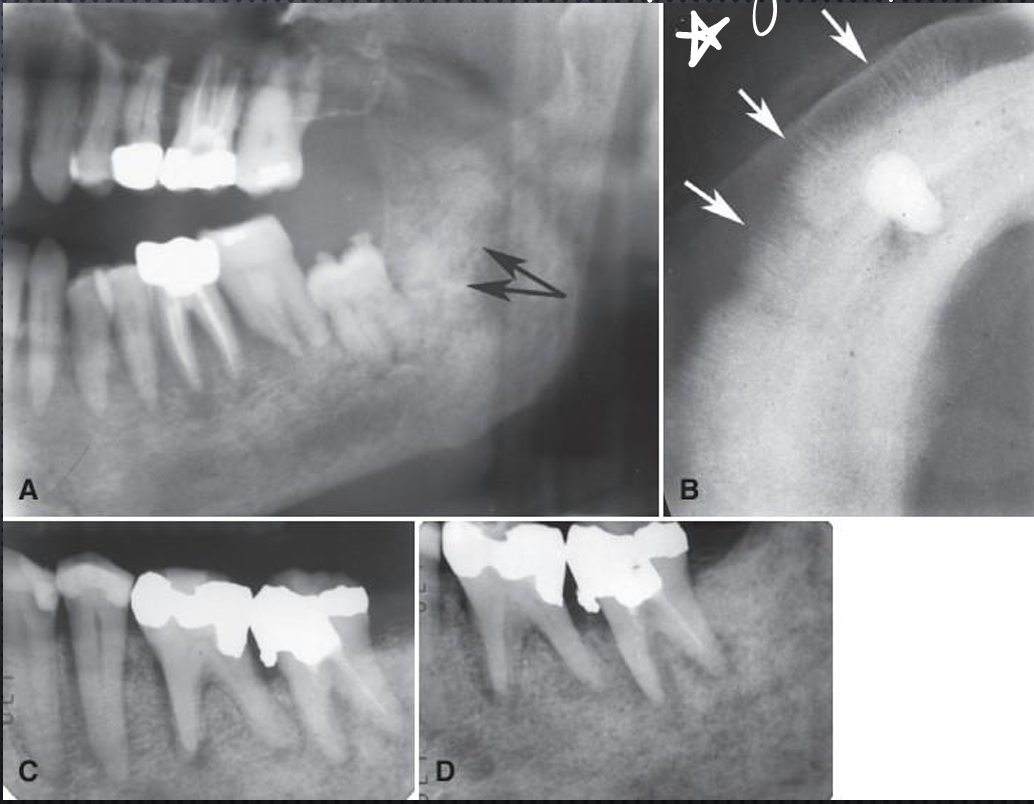
langerhan’s cell histocytosis
langerhan’s cell histocytosis
non-malignant (eosinophilic granuloma) or malignant (letterer-siwe disease and others), have neoplastic nature
older children to young adult most common, forms quickly, dull pain, bony or soft tissue swelling, bleeding, ulceration
multifocal in the alveolar bone, solitary elsewhere, mandibular ramus
moderately well-defined, non-corticated, can appear scooped out, at midroot level scooped out appearance, smooth or irregular borders, destroys bone
langerhan’s cell histocytosis
periosteal reactions from langerhan’s cell histocytosis
what are the differential diagnoses for langerhan’s cell histocytosis?
periodontal disease- PD starts at the crest of bone, LCH midroot
squamous cell carcinoma (and other malignancies)- LCH typically better defined, younger age group, periosteal reaction