Complex Midterm
1/57
Earn XP
Description and Tags
Modules 1-5
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
Physical Indicators of Perfusion
Brain = LOC
Body = Pulses, Cap refill, skin color + temp
Organs = Urine output
Elements of Stroke Volume
Preload
Afterload
Contractility
Preload
End diastolic volume of ventricles
CVP
Central Venous Pressure
Right heart preload
Measured via PA line PROXIMAL port and Central Line
PAOP/PAWP
Pulmonary Artery Occlusive/Wedge Pressure
Left heart preload
Measured via PA line DISTAL port with balloon inflated
Afterload
Resistance the ventricles pump against
SVR
Systemic vascular resistance
Afterload for left ventricle
PVR
Pulmonary Vascular Resistance
Afterload for right ventricle
Ejection Fraction
% of blood ejected from ventricles upon contraction
<50% HF
55-70% Healthy
4 Lumens of PA Line
Proximal
Distal
Balloon
Thermistor
PA Line - Proximal Port
Placed in Right Atrium
Measures CVP, ScvO2
PA Line - Distal Port
Placed in pulmonary artery
Measures SvO2, PAWP/PAOP with balloon inflated
PA Line - Thermistor
Measures CO via temperature changes
ScvO2
O2 saturation of upper body’s deoxygenated blood returning to heart
Upper body = brain, head, arms, neck, chest
Slightly higher number than SvO2
Measured via central line (truer read) and PA line PROXIMAL port
SvO2
O2 saturation of mixed venous return from entire body
Measured via PA line DISTAL port
Central Line measures
ScvO2
CVP
Measures of Oxygen Delivery
Cardiac Output
ABG
Hemoglobin
SaO2 (Arterial Oxygen Saturation) - 97% delivery
PaO2 (Oxygen dissolved in plasma) - 3% delivery
Healthy SaO2
95-100%
SpO2 estimates this value
Healthy PaO2
75-100 mmHg
Healthy SvO2 and ScvO2 values
ScvO2: 70-80%
SvO2: 65-75%
How do you calculate a HR using a 6 second ECG strip?
Number of QRS complexes in 6 sec strip x 10
OR
1500/small boxes btwn R waves
- 500/large boxes btwn R waves
P wave
Atrial depolarization
Impulse from SA → AV node
P-R Interval
Time for atria to depolarize and contract
.12-.2 sec (about 1 medium box)
(From beginning of P wave to downward curve of Q)
QRS Complex
Ventricular depolarization + Atrial repolarization
<.1 sec (half of a medium box)
ST Segment
Ventricular contraction
(Bottom of S to where T starts to bump up)
T Wave
Ventricular repolarization
U wave
Rare (digoxin tox or hypokalemia)
Purkinje fiber repolarization
QT Interval
<.44 sec
Shows us time for ventricles to reset
(From end of P wave to end of T wave)
QT Prolongation
Dangerous if >.5
Congential issue, meds, hypokalemia
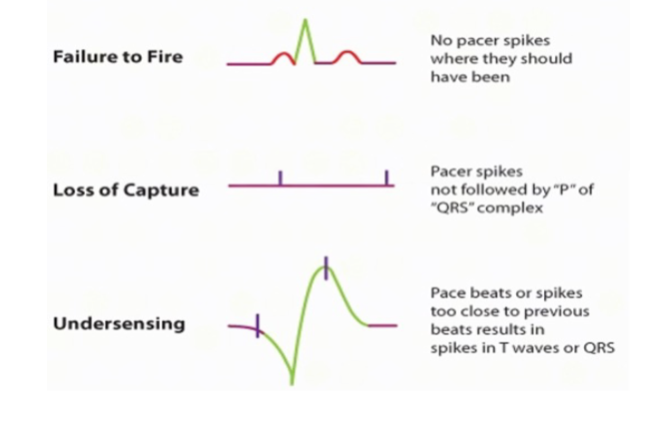
Pacing Issues
Failure to fire
Loss of capture
Undersensing
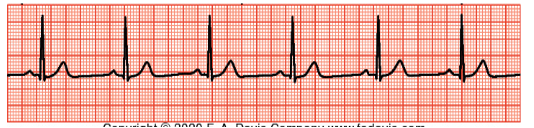
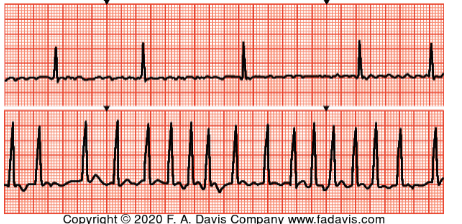
Normal Sinus

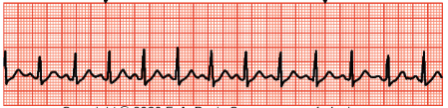
Sinus Arrhythmia
Irregular rhythm
D/t regular breathing, sleep apnea, sick sinus syndrome

Sinus Bradycardia
Rate <60 bpm
D/t hypoxia, hypothermia, meds, sleep, athletes
Treatment
Symptomatic: Atropine + treat cause (emergent), pacing (non-emergent)
Asymptomatic: Address cause, monitor
Sinus Tachycardia
Rate >100 bpm
D/t fever, compensation (anemia/hypovolemia/hypotension), PE, MI
Treatment
Treat the cause + meds (Beta Blockers, CCBs)
Tachyarrhythmias must be cardioverted
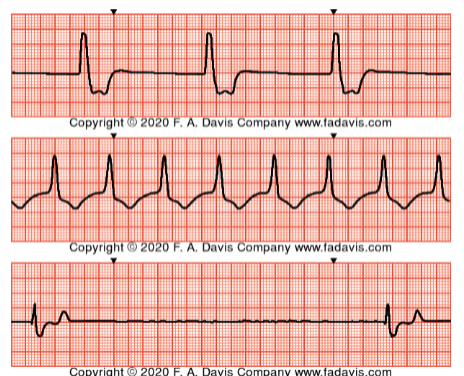
Idioventricular Rhythm
Ventricles acting as pacemaker
Slow rates typically
No P wave, wide QRS
Causes: MI, meds, toxicity, electrolytes, congenital
Treatment
Pulse: Treat cause + Pace +Atropine
Pulseless: CPR
AFib
No P waves, rates vary, no regular rhythm
Causes: aging, chronic conditions
Complications: Decreased CO, CLOTS
Treatment
Anti-coagulation, rate control, rhythm control
Severe s+s or rate → Cardiovert

Atrial Flutter
Irregular sawtooth “F” waves
Rates vary
Causes: MI, mitral valve disease, COPD
Treatment:
Anti-coagulation, rate control, rhythm control
Severe s+s or rate → Cardiovert
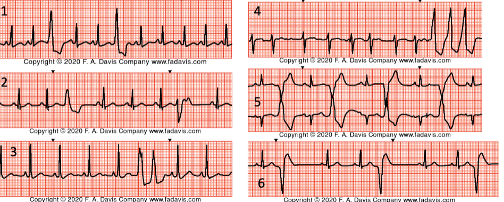
Premature Ventricular Contractions (PVCs)
Wide, irregular QRS complexes that are all unique
Multiple (3+) could be precursor to VTach
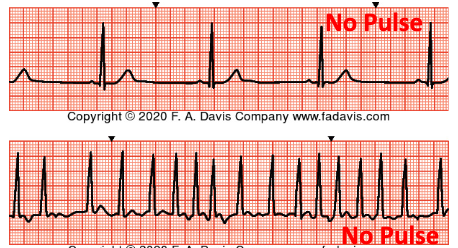
Ventricular Tachycardia (VTach)
Causes: Hs + Ts
Treatment
Pulse: Treat cause + anti-arrhythmic (amiodarone) + cardiovert
Pulseless: CPR + Defib + Epi/Amiodarone
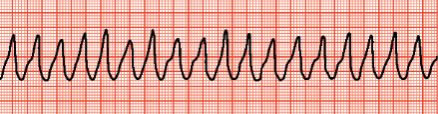
Torsade’s de Pointes
Rapid, continuously changing QRS complexes with no P waves
Treat with MAGNESIUM
Treat like VTach
Pulse: Cardiovert
Pulseless: CPR + Defib
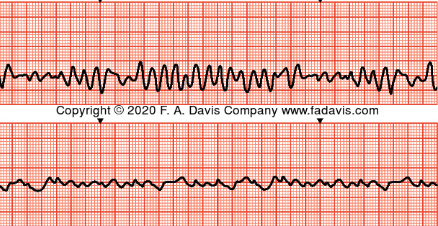
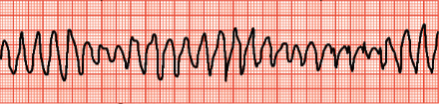
Ventricular Fibrillation (VFib)
Coarse or fine
Causes: Hs and Ts
Treat: CPR + Defib
Pulseless Electrical Activity
Treat with CPR + Epi
Push Epi Always
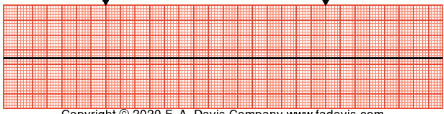
Asystole
CPR + Epi!
Hs and Ts: The H’s
Hypoxia
Hypothermia
Hypovolemia
Hydrogen ions (acidosis)
Hypo/hyperkalemia
Hs and Ts: The Ts
Tamponade
Thrombus (PE)
Thrombus (Cardiac)
Tension pneumo
Toxins
Defibrillation Rhythms
VFib
Pulseless VTach
Cardioversion Rhythms
AFib (after anti-coag)
VTach with a pulse
Unstable tachyarrhythmias
Amiodarone
Anti-arrhythmic, reduces HR
For tachyarrhythmias
Atropine
Increases HR
Bradycardias
Adenosine
Converts, slows, stops rhythms
May go into asystole - be careful!
Stages of Shock
Initial
Compensatory
Progressive
Refractory
Initial Stage of Shock
Initial insult, subtle changes in assessment
May see higher lactate
Compensatory Stage
Tachypnea (alkalosis)
Tachycardia
Decreasing BP + UO!
Subtle AMS
Narrowing pulse pressure + weaker pulses
Cool, clammy skin
Progressive Stage
Compensation fails
Blood is shunted to vital organs
Profoundly low BP
Lethargy/coma
Absent bowel sounds, anuria (organs failing d/t no perfusion)
Acidosis d/t anaerobic metabolism
Refractory Stage
Prolonged tissue hypoperfusion —> multi-system organ failure
Peripheral ischemia and necrosis
Irreversible, high mortality rate
MODS
Multiple Organ Dysfunction Syndrome
Decreased oxygen delivery to organs + higher demand
Organ dysfunction → organ death
Lungs + kidneys usually first to go
1 organ to 3+, mortality rate goes from 40% to 80-90%
Identify via anuria, respiratory failure, absent bowel sounds
Treat cause + supportive care
DIC
DIC: Disseminated Intravascular Coagulopathy Flow
Looks like…bleeding from unlikely places Labs
Treatment
|