ceramic indirect restoration
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Direct Restoration
Restorations that are placed directly in the mouth after tooth preparation.
Material is applied in a tooth preparation and then shaped and cured inside the tooth.
Typically used for small to moderate defects.
Indirect Restoration
Restorations that are fabricated outside the mouth (usually in a dental lab or using CAD/CAM technology).
Requires a final impression (traditional or digital) to create a customized restoration
Used for larger defects or when additional strength is required.
ceramic indirect restoration
INLAY/ONLAY
Single Crown
Fixed Partial Denture (F.P.D)
Veneers
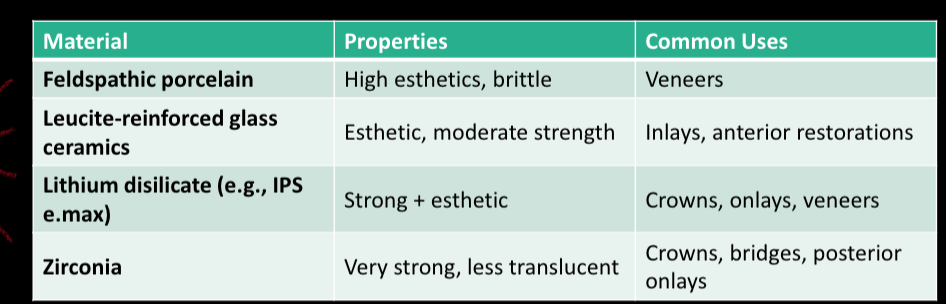
materials for indirect inlay/onlay
Porcelain/Ceramic → LEUCITE/FELDSPATHIC (anteriors)
COMPOSITE
most commonly used:
LITHIUM DISILICATE (e-Max)
Zirconia
properties of the different materials used for inlay/onlay
Indications
Esthetic areas (anterior teeth) → E. max + feldspathic
Moderate to large restorations requiring mechanical and esthetic properties → emax + zirconia
Fractured or worn dentition
Replacement of old composite/amalgam
Patients with good oral hygiene and low caries risk
Contraindications
Bruxism or heavy occlusion (relative for feldspathic)
Poor moisture control (affects bonding)
Inadequate enamel for bonding
Deep subgingival margins
Patients with high caries risk
An Inlay/Onlay can be used instead of a direct restoration for patients with
a low caries risk, when higher strength of material is needed (heavy occlusion/metal), or when superior control of contours and contacts are desired.
An inlay requires ample supporting dentin in the facial and lingual surfaces
Onlay
allows the damaged occlusal surface to be restored in the most conservative
manner, compared to a full coverage crown
Objectives of tooth preparation
Preserve Tooth Structure: Aim for minimal reduction to maintain strength and
vitality.
Ensure Adequate Thickness: Provide sufficient space for the ceramic material to
withstand occlusal forces.
Smooth Transitions: Create rounded internal line angles to reduce stress
concentration.
Appropriate Margins: Use well-defined margins suitable for the specific restoration
type.
Ceramic Inlay Restorations
Occlusal Reduction: 1.5–2.0 mm deep for sufficient ceramic thickness.
Isthmus Width: Minimum 2.0 mm for strength and resistance to fracture.
Wall Divergence: 6°–10°
Internal Angles: Rounded (no sharp internal line angles).
Cavosurface Margin: Use a butt joint or light bevel, no sharp shoulders.
Exit Angles: Avoid acute exit angles to prevent marginal chipping.
Taper: Axio-pulp lines angles rounded
Break interproximal contact. Perio probe tip will just fit between adjacent tooth and prepared CSM at facial, lingual and gingival margins. When the interproximal contact is not broken, it is difficult to capture the margin with the final impression
Ceramic onlay Restorations
Functional Cusp Reduction: 1.5–2.0 mm reduction for molars and premolars.
Non-functional Cusp: 1.0–1.5 mm if covered.
Occlusal and Proximal Boxes: Extend 1–1.5 mm into proximal surfaces with smooth transitions.
Margin Design: Use butt joint or rounded shoulder. No feathered edges.
Axial Wall Divergence: Maintain 6°–10° taper for draw.
Avoid Sharp Margins: Sharp margins increase risk of ceramic fracture.
Internal Finish: All line angles rounded and smooth.
Ceramic Inlay preparation
Evaluate occlusal contacts relationships with articulating paper
Margins of the restorations should not be at the centric contact
Rubber Dam Isolation
Outline form is usually dictated by
the existing restoration and caries
Removing existing restoration and caries.
internal outline
No undercuts: If necessary, undercuts can be blocked with composite or glass ionomer.
If the undercut leaves unsupportive enamel, the enamel must be removed and preparation design modify
Walls: Facial, lingual, mesial or distal: 6º-8º wall divergently tapered is optimum for internal adaptation and margin fit.
Over-tapering leads to thinner occlusal margins and increased margin stress as the margin approaches the cusp.
proximal box
Axio-pulpal line angle should be rounded.
Gingival wall parallel occlusal plane, no J-CSM.
No undercuts in proximal portion of walls in the box.
Proximal box (Inlay) and extension of box (onlay)
Onlay : The slopping ramp between the proximal box and the extension of box should be smooth.
Advantages of ceramic
Excellent esthetics
Biocompatibility
High strength (lithium disilicate, zirconia)
Color stability
Disadvantages of ceramic
Brittle (especially feldspathic porcelain)
Technique-sensitive bonding
Requires enamel for optimal adhesion
Higher cost compared to composites
Cementation resin based luting agents: Etchable ceramics
Hydrofluoric acid etch
Silane coupling agent
Resin adhesive cement
e.g., lithium disilicate
Cementation resin based luting agents: non-etchable ceramics
Sandblasting
MDP-containing primers
Self-adhesive or resin cements
ex: zirconia