Anesthesia Final Info
1/144
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
145 Terms
What are the 4 stages of anesthesia?
Stage 1: administer induction drug to loss of consciousness
Stage 2: excitement stage (hope to avoid)
stage 3: surgical anesthesia (we focus here)
stage 4: extreme CNS depression (try to avoid this)
What are the 5 standards that we monitor the most?
CNS
oxygenation
ventilation
circulation
temperature
What is the objective of monitoring CNS depression?
adequate depth to prevent patient awareness and movement while minimizing adverse effects of anesthetic agents.
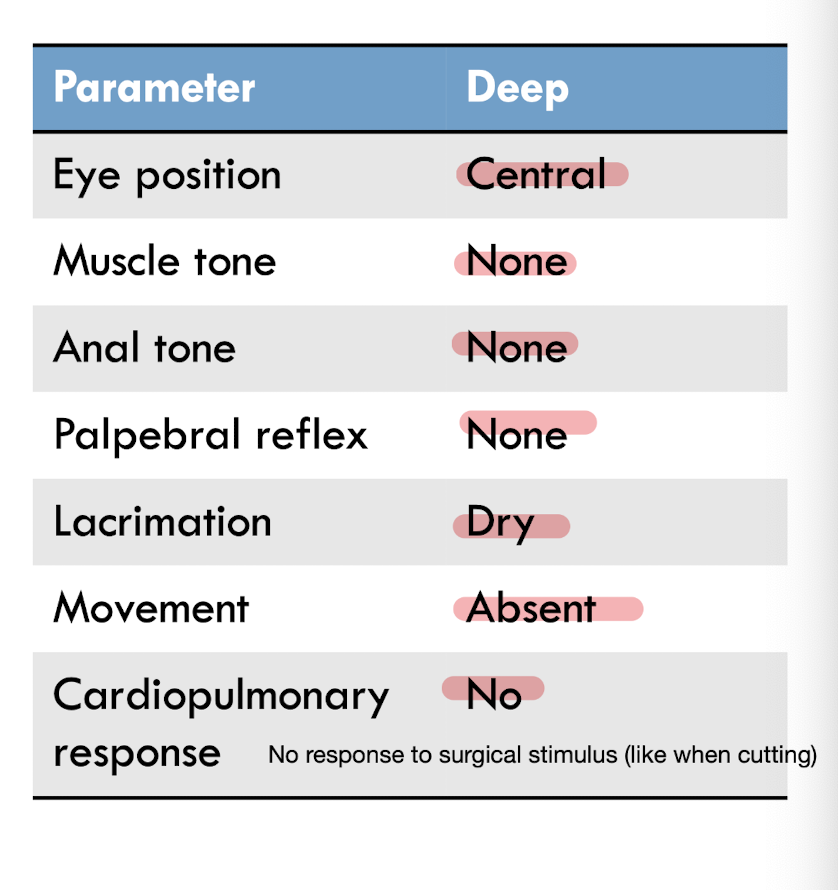
What do you see when in light, medium and deep plane in the context of eye position, muscle tone, anal tone, palpebral reflex, cornea lacrimation, movement in response to stimuli, and cardiopulmonary variations in response to stimulus?
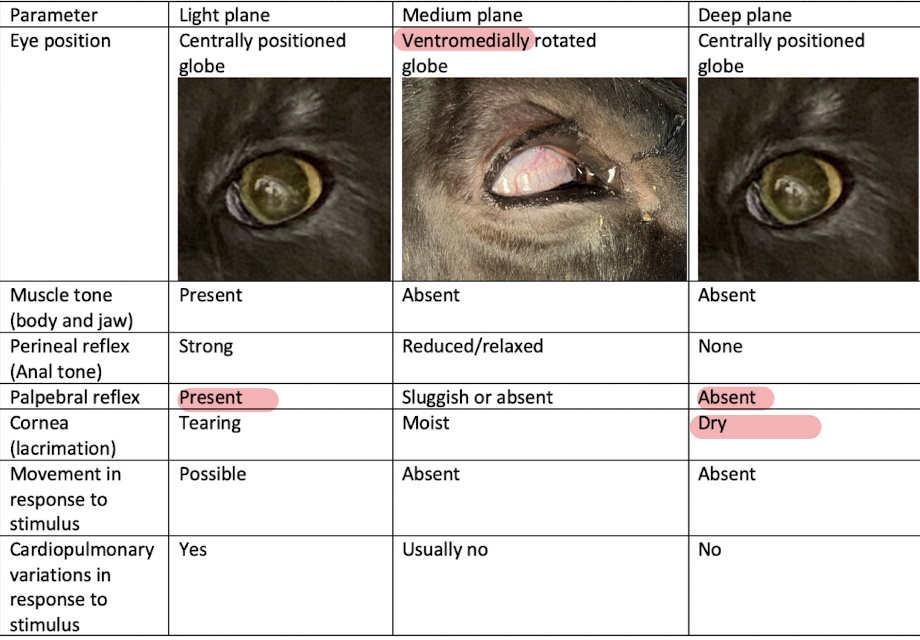
There was no palpebral reflex, absent muscle tone, central positioned eye, not moving in response to stimulation (steady HR).
What stage and level of anesthesia?
stage 3, deep
What is an advanced monitoring technique for CNS depression?
inspired and expired inhalant concentrations
What is the objective of monitoring oxygenation? What are the two minimum recommendations?
ensure adequate oxygenation of the blood and to enable rapid recognition of hypoxemia.
MM colour and pulse oximetry
What does pulse oximetry measure?
percent saturation of hemoglobin with oxygen (SpO2)
How does pulse oximetry work?
Clip has a transmitter and a receiver side. Clip over non pigmented tissue (usually tongue). Transmitter transmits two wave forms, a visible red and an infrared light. Red light is absorbed by hemoglobin. How much light passes through? It will tell us a percentage.
Also senses pulsatile flow—> pulse rate
What does the heights of the waves in a pulse oximetry graph tell us?
tells us about the volume of the pulses.
Tall wave=pulses are strong with high volume.
Narrow or flat graph=vasoconstriction or poor perfusion.
If breathing 100%, SpO2 should always be above __%.
95
What are three advanced methods of monitoring oxygenation?
arterial blood gas analysis
inspired oxygen concentrations
co-oximetry
What is the objective of monitoring ventilation? What are the minimum requirements?
to ensure adequate ventilation and to enable rapid recognition of hypocarbia and hypercarbia
resp rate, estimated tidal volume, pulmonary auscultation,
capnography
How does mainstream capnography work? How does side stream work?
Mainstream: sensor is built in—> shows end tidal CO2 reading (want between 35 and 45**).
Mainstream has sensor built into adapter while side stream draws a sample out and analyzes it.
Must scavenge gases from side stream was the sample has some waste inhalant
In capnography, what does the trough show?
trough is inspire (peak is expire)
What is normal end tidal CO2?
35-45mmHg
What does a CO2 >45mmHg tell us? What about <35mmHg?
hypoventilation
hyperventilation (not common)
What is the normal fraction of inspired CO2?
0 mmHg because the anesthetic machine should prevent all rebreathing of CO2
What are two advanced recommendations for monitoring ventilation?
arterial blood gas analysis
spirometry
What are the minimum requirements for monitoring circulation?
peripheral pulses, heart sounds, MM colour, cap refill time
ECG
noninvasive blood pressure
What are you feeling when you feel a pulse?
we feel the difference between systolic and diastolic pressure but not numbers—> (150/90 feels the same as 120/60). Look if the rhythm is in sync, regular or irregular, etc.
What does a cap refill >2 seconds indicate?
hypoperfusion
What does an ECG tell us?
Does NOT tell us if the heart is actually beating just tells us if the electrical portion of the heart is normal.
What is the normal HR ranges for dog? Cats? Horses? Cattle?
60-140
120-220
30-40
60-80
How does oscillometric non invasive bloop pressure work?
Oscillometric method: like what they do at shoppers. Cuff inflates, feel it slowly deflate and can feel pulse.
put cuff around limb or tail, inflates until blood flow is occluded. Slowly deflate. When pulses return, the pulses push against cuff and sense the oscillations in the cuff. Run them and generate a systolic and diastolic pressure and mean arterial blood pressure and pulse rate
width of this cuff is about 40% of the circumference of the limb
limitations: moving animals can impact readings, works only for regular rhythms not arrhythmias
How does the doppler non invasive BP work?
Doppler: choose cuff the same way as oscillometric (40% of circumference). Shave a spot over peripheral a. Attach doppler probe. The speaker allows you to hear pulse. Inflate until you dont hear pulse anymore then deflate. Watch the pressure and if you hear the pulse again then that is the systolic pressure.
limitations: takes a bit more skill, done manually (can’t set and forget)
good thing is you can hear the pulse rate which is helpful to pick up arrhythmias
What does the doppler measure? When is it considered hypotensive?
systolic BP
<90mmHg
What is normal systolic BP? What is normal mean arterial BP? When is it considered hypotension?
100-140; <90 is hypotensive
70-120mmHg; <60 is SA and <70. in LA
What is gold standard for measuring BP?
Invasive BP via arterial BP through the auricular vein
What is normal temp range in general?
37-39*C
How do you recognize excessive anesthetic depth?
physical signs
How do you treat excessive depth?
decrease depth by reducing vaporizer and decreasing dose of injectables
oxygen supplementation, ventilation, etc
How do you recognize inadequate depth?
physical signs
How do you treat inadequate depth of anesthesia?
increase depth by increasing vaporizer (slower) and administer dose of injectables (way faster)
What is the definition of bradycardia in dogs? cats? horses?
<60
<90
<20
2 reasons why we worry about bradycardia?
reduce CO
reduced oxygen delivery to tissues
What are the two components of cardiac output?
heart rate and stroke volume
What are 5 causes of bradycardia?
increase in vagal tone (things that stretch GIT)
hypertension (reflex decrease in HR, seen with alpha 2s and dex)
hypoxemia
hypothermia
electrolyte abnormalities (high potassium and calcium)
3 ways to treat bradycardia?
consider an anticholinergic if due to increased vagal tone (atropine or glycopyrrolate)
address electrolyte abnormalities
address hypothermia
Why do we worry about tachycardia? (3)
reduction in ventricular filling
reduction in CO
reduced oxygen delivery to tissues
What is the definition of tachycardia in dogs? cats? horses?
>190
>220
>60
8 causes of tachycardia?
pain/insufficient depth
hypotension
hypoxemia
hypercapnia
drugs
hyperthermia
hypokalemia
concurrent diseases
NOTE: many different causes so treat the underlying cause
Why do we worry about hypotension (2)?
reduction in tissue perfusion
reduced oxygen delivery to tissues
What is the definition of hypotension in SA? LA? Systolic?
<60mmHg
<70mmHg
<90mmHg
What are the two main determinants of mean arteriole pressure?
cardiac output and systemic vascular resistance
Where there is a reduction in systemic vascular resistance, think vasodilation so we treat with vasoconstriction
What are 6 ways to treat hypotension?
assess depth
assess HR
assess volume (may need fluids)
increase cardiac contractility (positive ionotropes like dopamine and dobutamine)
increase systemic vascular resistance (epi or Nor which cause vasoconstriction)
5 reasons why we worry about hypoventilation?
acidemia
hypoxemia
increase in cerebral blood flow
CNS depression
death
What is the definition of hypoventilation?
ETCO2 or PaCO2 >45mmHg
NOTE: mild hypoventilation is tolerated in healthy patients
2 ways to diagnose hypoventilation?
capnography
arterial blood gas analysis (PaCO2)
What is the formula for minute ventilation?
resp rate x tidal volume
6 causes of hypoventilation?
anesthetic drugs (inhalants are dose dependent)
CNS disease
abdominal distension
positioning
thoracic injury
equipment malfunction
Two ways to treat hypoventilation?
reduce vaporizer
start positive pressure
work on underlying issue too
What is the definition of hypoxemia when breathing room air? 100% oxygen?
<90%, <60mmHg
<95%, <200mmHg
3 reasons why we worry about hypoxemia?
lactic acidosis
organ damage
death
Two ways to diagnose hypoxemia?
pulse oximetry
arterial blood gas analysis
5 causes of hypoxemia? Which one is most common?
ventilation/perfusion mismatch
hypoventilation
low fraction inspired oxygen
diffusion impairment (ex: thickened alveoli bc fibrosis)
right to left shunt
How do you treat hypoxemia if caused by low fraction inspired oxygen (FIO2) or hypoventilation? (3)
intubate
provide 100% oxygen
institute positive pressure ventilation
What are the two types of ventilation/perfusion mismatch?
alveoli is not ventilated but blood is perfused
ventilated alveoli but not perfused (ex: thromboembolism)
Define hypothermia? How do you diagnose?
temp <36*C
rectal or esophageal thermometer
6 reasons why we care if the patient is hypothermic?
wound infection
impaired blood clotting
arrhythmias
decreased metabolic rate
metabolic acidosis
death
4 causes of hypothermia?
convection (losing heat from cold air surrounding the patient)
conduction (loss of heat to surfaces)
radiation (loss of heat to other things in the room that they aren’t in contact with)
evaporation (ex: open abdomen)
How do you treat hypothermia? (4)
minimize surgery and anesthesia time
minimize prep
passive warming
active warming
What is the definition of a prolonged recovery in SA? LA?
>30 min
>60 min to stand in equines
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
Does she need to be sedated? If so what would you use?
yes— alpha 2 agonist like dexmedetomidine
NOTE: acepromazine is for mild sedation and is irreversible. Benzodiazepines provide minimal and variable sedation and potential for paradoxical excitement. Neither have any analgesic effect.
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
Does she need an opioid and what would you use?
yes, and a full mu agonist like hydromorphone
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
Does she need to be anesthetized? What could you use?
yes
propofol; ketamine and diazepam; and alfaxolone would all be appropriate
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
How would you maintain anesthesia?
A) not needed. Induction dose of alfaxalone will be sufficient
B)constant rate infusion of propofol
C)isoflurane using a rebreathing system
D)sevoflurane using a non-rebreathing system
D
Note size of animal for non-rebreathing system
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
What supportive care will Peggy need?
A) none. Peggy’s a healthy cat
B) subQ fluids at 5ml/kg/h
C)Thermoregulatory support with forced warm air
D)intravenous fluids and thermoregulatory suppory with a circuating warm water blanket
D
Peggy: 8 month old, intact female DSH, 3.5kg, presented for an OHE and extraction of fractured canine tooth.
What is your peri-operative analgesic plan?
A) one more dose of opioid analgesic
B)one dose of NSAID
C)opioid and NSAID that continues based on pain scoring
D) local blocks of the abdominal incision and infraoribital nerve. Opioid and NSAID that continues based on pain scoring.
D
During a canine tooth extraction you auscultate a heart rate of 80bpm and there was a systolic blood pressure of 85mmHg. What problems does this dog have? How would you treat these issues?
bradycardia and hypotension
administer an anticholinergic
Spike is a 3 yo Yorkie weighing 3.2kg presented for evaluation of goose honk cough. He needs a tracheoscopy, bronchoscopy, and bronchoalveolar lavage (BAL) as you suspect a collapsing trachea. Does Spike need to be sedated? What would you use?
yes, use acepromazine and an alpha 2 agonist (dexmedetomidine)
Spike is a 3 yo Yorkie weighing 3.2kg presented for evaluation of goose honk cough. He needs a tracheoscopy, bronchoscopy, and bronchoalveolar lavage (BAL) as you suspect a collapsing trachea.
Does he need analgesia? If so, what would you use?
yes, and I would use a mixed agonist/antagonist (butorphanol)
Spike is a 3 yo Yorkie weighing 3.2kg presented for evaluation of goose honk cough. He needs a tracheoscopy, bronchoscopy, and bronchoalveolar lavage (BAL) as you suspect a collapsing trachea.
Does he need to be anesthetized? How would you induce anesthesia?
yes, propofol
Spike is a 3 yo Yorkie weighing 3.2kg presented for evaluation of goose honk cough. He needs a tracheoscopy, bronchoscopy, and bronchoalveolar lavage (BAL) as you suspect a collapsing trachea.
How will you maintain anesthesia?
A) not needed
B)constant rate infusion of propofol
C)constant rate infusion of ketamine and diazepam
D) sevoflurane using a re-breathing system
B
Spike is a 3 yo Yorkie weighing 3.2kg presented for evaluation of goose honk cough. He needs a tracheoscopy, bronchoscopy, and bronchoalveolar lavage (BAL) as you suspect a collapsing trachea.
When monitoring, you notice that he has a pulse ox reading of 88%, heart rate of 130bpm, and MAP of 87mmHg. What problems does he have? How would you treat?
hypoxemia
intubate and administer 100% oxygen through a NRB system
What is the resting heart rate of equines? What is a common cardiovascular finding in them?
28-44beats/min
intermittent 2nd degree AV blocks
True or false:
Equines are obligate nasal breathers
true
Why are there higher mortality rates in equines compared to SA? (5)
recumbency
CV function is depressed leading to hypotension and then post-anesthetic myopathy and poor recovery
impaired ventilation with muscle relaxation causing profound atelectasis
positioning can cause myopathy and neuropathy
nature of horses (prey animals)
Should horses be fasted before anesthesia?
no, and keep easy access to water is important
Before elective equine procedures, what bloodwork should be done?
PCV and TP
What are the 5 general risks for anesthesia?
4H1B
hypotension
hypoxemia
hypoventilation
hypothermia
bradycardia
What are 6 species specific risks of anesthesia in horses?
myopathy/neuropathy
poor recovery
safety of personnel
upper resp obstruction
ventilation/perfusion mismatch
post op ileus/colic
What is the most commonly used sedation in equines?
alpha 2 agonist like xylazine
could also use acepromazine if anxious/nervous (avoid in sick horses)
What is one side effect of acepromazine unique in horses?
persistent priapism which is a concern in breeding stallions
What is a good analgesic to use after sedation in horses? One potential side effect?
butorphanol
decreased GI motility—> predispose to colic
What is a good induction drug for equines?
fast bolus injection of ketamine and benzodiazepine (benzo for muscle relaxation)
Two ways to do total intravenous anesthesia in equines?
top ups but there is more swings in depth
triple drip (mixture on guaifenesin, ketamine and xylazine) which has less swings in patient depth
When performing equine anesthesia, ALWAYS have a ________ bolus drawn up and close by.
ketamine
True or false: In equines, heart rate is an indicator of arousal.
true
Is sedation required for recovery in equines?
xylazine can be used with inhalant anesthesia while injectable anesthesia often does not need sedation.
What is an important thing to watch for when extubating equine patients?
They are obligate nasal breathers and nasal edema can occur and result in upper airway obstruction.
2 things to keep in mind when anesthetizing draft horses?
they have small surface area for their size so they need a decreased sedative drug dose
higher risk for spinal cord degeneration
Does salivation production remain high in ruminants even under general anesthesia?
yes—> only difference is that they can’t swallow
Why are ruminants harder to assess pain on?
they are prey species and can mask behavioural signs of pain
What are two advantages of fasting and water deprivation in ruminants? 4 disadvantages?
decreases incidence of hypoxemia and less likely to bloat during recumbency and anesthesia
ruminal hypomotility, bradycardia (increased parasympathetic tone), regurgitation risk more likely, dehydration
What is one respiratory related thing we should watch for in small ruminants when doing a pre-op evaluation?
subclinical pulmonary disease
What are 5 species specific risks for euthanasia in ruminants?
restraint and handling risks
neuropathy, myopathy
regurgitation and excessive salivation
aspiration pneumonia
ruminal tympany (bloat)
Is atropine recommended to prevent salivary secretions in ruminants?
no, only reduces aqueous components of salivation which makes it way more thick and harder to clear.
Ruminants are very sensitive to ________ sedation.
xylazine
Two potential side effects of xylazine in ruminants? What about sheep?
ruminal hypomotility, uterine contractions
hypoxemia and pulmonary edema in sheep