Complications of Pregnancy & High Risk Labor
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Hypertensive Disorders: Significance and Incidence
major cause of what
three most common types
• Common medical complications of pregnancy, occurring in 5-10% of all pregnancies
• Hypertensive disorders are a major cause of
perinatal morbidity and mortality worldwide.
• Three most common types in pregnancy:
• gestational hypertension
• preeclampsia
• chronic essential hypertension
Gestational hypertension
define
DX
resolves when
• Onset of hypertension without proteinuria or other systemic findings diagnostic for preeclampsia after week 20 of pregnancy
• Systolic BP greater than 140, diastolic BP greater than 90
• Resolves after giving birth
Preeclampsia
define
onset
when does/can it develop
• Pregnancy-specific condition in which hypertension and proteinuria develops after 20 weeks of gestation in a previously normotensive woman
• Can also develop for the first time during the postpartum period
In the absence of proteinuria, preeclampsia may be defined as hypertension along with the following: (5)
• Thrombocytopenia
• Impaired liver function
• New-onset renal insufficiency
• Pulmonary edema
• New-onset cerebral or visual disturbances
Eclampsia
define
no hx of
onset
• Onset of seizure activity or coma in a woman with preeclampsia
• No history of preexisting (seizure-related) pathology
• Women can develop eclampsia in the immediate postpartum period
• Occurs in approximately 1 in 2000 to 1 in 3448 births
• 50% of eclamptic women develop the condition while pregnant
chronic hypertension
Hypertension present before pregnancy or diagnosed before week 20 of gestation
Chronic hypertension with superimposed preeclampsia
• Women with chronic hypertension may acquire preeclampsia or eclampsia
• Can be difficult to diagnose
preeclampsia
can be caused by
common risk factors
paternal factors
theory to why it occurs
• Etiology
• Condition unique to human pregnancy; occurs in approximately 2% to 7% of healthy nulliparous pregnant women
• Common risk factors
• Multifetal gestation
• History of preeclampsia
• Chronic hypertension
• Preexisting diabetes and/or thrombophilias
• Women with limited sperm exposure with the same partner
• Paternal factors:
Men who have fathered a preeclamptic pregnancy are nearly twice as likely to father another preeclamptic pregnancy with a different woman, regardless of whether the new partner has a history of a preeclamptic pregnancy
• The cause of preeclampsia is unknown
• Current thought is that preeclampsia is caused by a complex interaction of maladaptive cardiovascular and uteroplacental responses to pregnancy
preeclampsia
pathophysiology
• Progressive disorder with placenta as the root cause
• Begins to resolve after the placenta has been expelled
• Spiral arteries in the uterus normally become larger and thicker to handle increased blood volume
• This vascular remodeling does not occur or only partially develops in women with preeclampsia and decreased placental perfusion and endothelial dysfunction result
Preeclampsia
can cause or lead to
why does this happen
Placental ischemia leads to endothelial cell dysfunction
• Generalized vasospasm leads to poor tissue perfusion in all organ systems
• Increased peripheral resistance and blood pressure (BP)
• Increased endothelial cell permeability
• Reduced kidney perfusion
• Plasma colloid osmotic pressure decreases
• Decreased liver perfusion
• Neurologic complications
• Cerebral edema
• Cerebral hemorrhage
• Central Nervous System irritability
HELLP syndrome
define
can occur in who
• Laboratory diagnosis for a variant of preeclampsia that involves hepatic dysfunction, characterized by:
• Hemolysis (H)
• Elevated liver enzymes (EL)
• Low platelets (LP)
• HELLP syndrome can develop in women who do not have hypertension or proteinuria; women with HELLP are often misdiagnosed
• Perinatal mortality rate ranges from 7.4% to 34%, with a maternal mortality rate of approximately 1%
HELLP syndrome
results from
s/s (4)
• Result of arteriolar vasospasm, endothelial cell dysfunction with fibrin deposits, and adherence of platelets in blood vessels
• The clinical presentation is often nonspecific; most women with the disorder report the following:
• History of malaise
• Influenza-like symptoms
• Epigastric or right upper quadrant abdominal pain
• Symptoms worsen at night and improve during the daytime
care management: identifying and preventing preeclampsia
medication (1)
screening
• Low-dose aspirin (81 mg daily) may help certain high-risk women
• Potential biomarkers that can identify individual women who will develop hypertension during pregnancy is ongoing
• No reliable test or screening tool has been developed
Care management
assess for what (5)
evaluate for s/s of what
s/s (4)
Assessment
• Accurate measurement of BP
• Assessment of edema, although the presence of edema is no longer included in the definition of preeclampsia
• Deep tendon reflexes (DTRs)
• Assess for hyperactive reflexes (clonus)
• Proteinuria: ideally determined by evaluation of a 24-hour urine collection.
• Although proteinuria may still be used to define preeclampsia, studies have shown little relationship between the degree of proteinuria in women with preeclampsia and pregnancy outcome
Evaluate for signs and symptoms of severe preeclampsia
• Headaches
• Epigastric pain
• Right upper quadrant abdominal pain
• Visual disturbances
Interventions: Gestational Hypertension and Preeclampsia Without Severe Features
Goals (2)
other interventions
• Because preeclampsia is a dynamic disease process, the terminology of “mild” and “severe” is no longer recommended
Goals:
• ensure maternal safety
• deliver a healthy newborn as close to term as possible
other:
• Outpatient management usually possible
• Laboratory evaluations
• Fetal evaluation
• Activity Restriction: no evidence that bedrest improves outcomes
Interventions: Gestational Hypertension and Preeclampsia with Severe Features
goal
expectant management
intrapartum care (4)
• Goals of care are to ensure maternal safety and formulate a plan for delivery
• Expectant Management
• For women at less than 37 weeks gestation
• Hospitalized; care from interprofessional team, including a perinatologist; antihypertensive meds & corticosteroids to enhance fetal lung maturity
• Intrapartum care
• Continuous FHR and uterine contraction monitoring
• Bed rest with side rails up
• Darkened environment
• Assessed for signs of placental abruptio
Interventions: Magnesium sulfate
first line treatment for what
route
dosing
effect on BP?
HIGH ALERT MEDICATION
• Medication of choice for preventing and treating seizure activity (eclampsia)
• Administered intravenously as a secondary infusion (piggyback) by a volumetric infusion pump
• Initial loading dose, then continuous maintenance dose
• Magnesium sulfate has little effect on maternal BP when administered in this fashion
• Unclear how magnesium sulfate works to prevent and treat eclamptic seizures
• High Alert Medication
other interventions
control BP
postpartum care
future health care
• Control of Blood Pressure
• Antihypertensive medications are indicated when the systolic BP exceeds 160 mm Hg or the diastolic BP exceeds 110 mm Hg
• Postpartum care
• Vital signs, DTRs, level of consciousness
• Magnesium sulfate infusion is continued after birth for seizure prophylaxis as ordered, usually for 24 hours
• Future health care
• Significant risk of developing preeclampsia in a future pregnancy (women with severe features)
• increased risk for developing chronic hypertension and cardiovascular disease later in life
• Educate clients on lifestyle changes
interventions: Eclampsia
premonitory signs (3)
can appear
immediate care (3)
stabilization
• Premonitory signs:
• persistent headache and blurred vision
• Epigastric or right upper quadrant pain
• Altered mental status
• Convulsions can also appear without warning
• Immediate care
• Ensure patent airway and client safety
• Note the time of onset and duration of the seizure
• Call for help but remain at the bedside
• Maternal stabilization after seizure
chronic hypertension: interventions
who’s more at risk
ideal management
lifestyle modifications (4)
tx for high risk women with chronic HTN
• African-American women are at higher risk than others
• Ideally the management of chronic hypertension in pregnancy begins before conception
• Encourage lifestyle modifications: smoking and alcohol cessation, exercise, weight loss
• Women with chronic hypertension are classified as either high or low risk for pregnancy complications
• Women who are high risk are managed with antihypertensive medication and frequent assessments of maternal and fetal well-being.
Hemorrhagic Disorders
NEW SECTION
Antepartal Hemorrhagic Disorders
define
causes
increases risk for (5)
• Bleeding in pregnancy jeopardizes maternal and fetal well-being
• Maternal blood loss decreases oxygen-carrying capacity and increases risk for the following conditions:
• Hypovolemia
• Anemia
• Infection
• Preterm labor
• Impaired oxygen delivery to the fetus
Antepartal Hemorrhagic Disorders
fetal risks from maternal hemorrhage (5)
hemorrhagic disorders are considered
• Fetal risks from maternal hemorrhage
• Blood loss, anemia
• Hypoxemia
• Hypoxia
• Anoxia
• Preterm birth
• Hemorrhagic disorders in pregnancy are medical emergencies
• The incidence and type of bleeding vary by trimester
• Prompt assessment and intervention by the interprofessional health care team are essential to save the lives of both the woman and her fetus
Early Pregnancy Bleeding
most common type
miscarriage (spontaneous abortion)
when do most miscarriages occur
types of miscarriages (6)
• Miscarriage (Spontaneous Abortion): a pregnancy that ends as a result of natural causes before fetal viability
• Incidence and Etiology
• Approximately 10% to 15% of pregnancies end in miscarriage
• The majority—greater than 80% of miscarriages—are early pregnancy losses, occurring before 12 weeks of gestation
• Types of miscarriage
• Threatened
• Inevitable
• Incomplete
• Complete
• Missed
• Recurrent
• Clinical Manifestations
• Recurrent (habitual) miscarriages
Early Pregnancy Bleeding: care management
assessment
initial care
follow up care
• Assessment
• pregnancy history, vital signs, type and location of pain, quantity and nature of bleeding, and emotional status, lab tests
• Initial care
• Depends on the classification of the miscarriage & signs/symptoms
• Expectant management
• Medical management: misoprostol (Cytotec)
• Surgical management: dilation and curettage (D&C)
• Psychosocial aspects of care
• Follow-up care
• Discharge teaching emphasizes the need for rest
• Address questions about attempting another pregnancy
• Follow-up phone calls; support groups
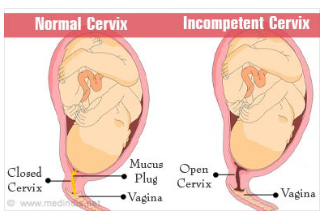
Early Pregnancy Bleeding: Cervical Insufficiency
define
can be caused by
DX
• Passive and painless dilation of the cervix during the second trimester
• May be either acquired or congenital
• Diagnosis
• Measurement of cervical length has been used as a way to diagnose cervical insufficiency
• Identify women who have cervical changes because of
impaired cervical strength before conception or in early
pregnancy rather than when they are beginning the process
of preterm labor
• Speculum/digital pelvic exams; transvaginal U/S
• abnormally short cervix – less than 25 mm
• Cervical funneling
Early Pregnancy Bleeding: Cervical insufficiency
care management
treatment of choice
follow up care
• Interprofessional Care Management
• Cerclage: treatment of choice for women with cervical insufficiency due to cervical weakness
• a suture is placed around the cervix beneath the mucosa to constrict the internal os of the cervix (McDonald technique)
• Abdominal cerclage: Suture (Mersilene tape) is placed at the junction of the lower uterine segment and the cervix
• Follow-up care
• Validity of bed rest has not been scientifically proven
• Progesterone therapy may be recommended for some women
• Watch for and report signs of preterm labor, rupture of membranes, and infection
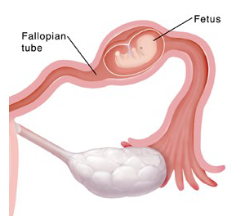
Early Pregnancy Bleeding: Ectopic pregnancy
define
s/s (3)
the fertilized ovum is implanted outside the uterine cavity; also called “tubal pregnancies”
• Clinical manifestations
• The three most classic symptoms are the following:
• 1. Abdominal pain
• 2. Delayed menses
• 3. Abnormal vaginal bleeding (spotting)
Ectopic pregnancy
DX
care management
medication
surgery
• Diagnosis
• Difficult differential diagnosis: numerous disorders share similar signs and symptoms
• Quantitative β-hCG levels and transvaginal ultrasound examination
• Discriminatory zone - a β-hCG level above which a normal intrauterine pregnancy should be visible on ultrasound
• Interprofessional Care Management
• Medical management: methotrexate
• Surgical management
• Type of surgery depends on the location and cause of the
ectopic pregnancy, the extent of tissue involvement, and
the woman’s desires regarding future fertility
• Follow-up care
Early Pregnancy Bleeding: Molar Pregnancy (Hydatidiform Mole)
define
cause
types: complete, partial
Molar Pregnancy (Hydatidiform Mole)
• Type of gestational trophoblastic disease
• Benign proliferative growth of the placental trophoblast
in which the chorionic villi develop into edematous,
cystic, avascular transparent vesicles that hang in a
grapelike cluster
• Incidence and etiology
• Occurs in 1 in 1000 pregnancies in the United States
• Cause is unknown; may be related to an ovular defect or a nutritional deficiency
• Types
• Complete: no embryonic or fetal parts
• Partial: often have embryonic or fetal parts and an amniotic sac
Molar Pregnancy (Hydatidiform Mole)
s/s (4)
DX
care management
follow up care
• Clinical manifestations
• Anemia from blood loss, excessive nausea and vomiting (hyperemesis gravidarum), and abdominal cramps
• Preeclampsia occurs in approximately 70% of women with large, rapidly growing hydatidiform moles and occurs earlier than usual in the pregnancy
• Diagnosis
• Transvaginal ultrasound and serum hCG levels
• Interprofessional Care Management:
• Most moles abort spontaneously; Suction curettage can safely be used
• Follow-up care: monitor β-hCG levels
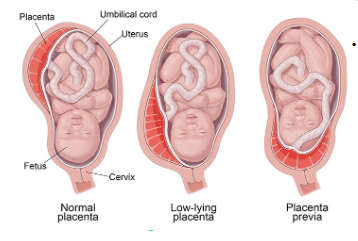
Late Pregnancy Bleeding: Placenta Previa
define
types and how their classified
risk factors (4)
• Definition: placenta implanted in lower uterine segment near or over internal cervical os
• Degree to which the internal cervical os is covered by placenta used to classify three types
• Complete placenta previa
• Marginal placenta previa
• Low-lying placenta
• Incidence and etiology
• 1 in 200 pregnancies
• Risk Factors include: Previous c-birth, advanced maternal age (more than 35 to 40 years of age), multiparity, history of prior suction curettage, living at a higher altitude and smoking
Placenta previa
s/s
DX
Abd exam findings
Maternal and fetal outcomes (3)
major complication
• Clinical manifestations
• Painless bright red vaginal bleeding during second or third trimester
• Now, most cases are diagnosed by ultrasound before significant vaginal bleeding occurs
• Abdominal examination usually reveals a soft, relaxed, nontender uterus with normal tone
• Maternal and fetal outcomes
• Major complication is hemorrhage
• Morbidly adherent placenta, an abnormally firm placental attachment
• Surgery-related trauma (most delivered by c-section)
• Preterm birth; IUGR