Additional Procedures (FINAL)
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
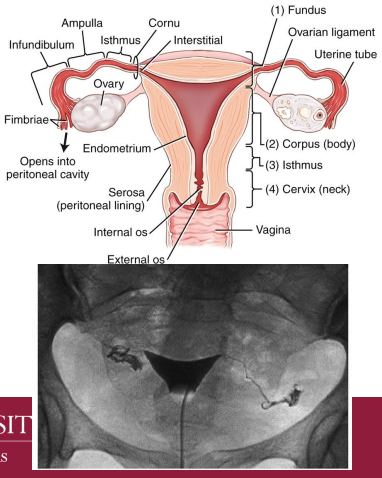
Hysterosalpingogram
The radiographic demonstration of the female reproductive tract
» Demonstrates uterine cavity and patency of uterine tubes
Indications
~ infertility: functional or structural defects
~ intrauterine pathology (ultrasound)
• endometrial polyps
• uterine fibroids
• intrauterine adhesions
~ Evaluate uterine tube after tubal ligation or
reconstructive surgery
» Contraindications
~ pregnancy
~ acute pelvic inflammatory disease (PID)
~ uterine bleeding
Hysterosalpingogram Prep
»Typically scheduled 7-10 days after onset of menstruation
»Bowel preparation
»Mild pain reliever before exam to relieve cramping
»Empty bladder
»Informed consent
»Performed in an R and F room that has ability for Trendelenburg position
»Gynecologic stirrups
Equipment
»Sterile gloves
»Sterile tray
»Sterile towels
»Speculum
»Tenaculum
»Head lamp
»Privacy screen
Contrast:
The most commonly preferred contrast is
positive, nonionic, and water soluble
Placement
»Patient is supine in lithotomy
position
»Catheter is placed into cervix
and balloon inflated to prevent
contrast from flowing out of
uterine cavity
»Contrast is injected slowly and
observed traveling through
uterus, fallopian tubes, and
spillage into peritoneal cavity
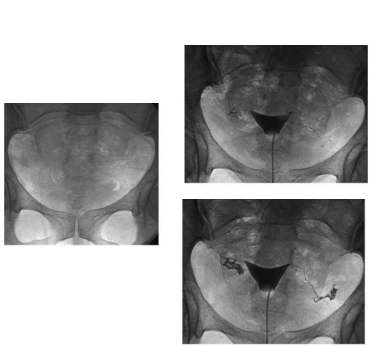
Hysterosalpingogram Imaging Routine
»AP (scout/post-contrast): CR 2” superior to the symphysis pubis
»LPO and RPO positions as requested
Swallowing Dysfunction Study (Modified Barium Swallow (MBS))
» Designed to:
~ Examine the A&P of the oral cavity and pharynx during deglutition
~ Identify disorders in movement patterns of oropharyngeal structures
~ Define treatment strategies that will eliminate aspiration and/or increase
swallowing efficiency
» Exam coordinated with a licensed
Speech Language Pathologist (SLP)
~ Patient must have been evaluated by SLP before exam
» Procedure done under fluoroscopy to evaluate difficulty swallowing (dysphagia)
Swallowing Dysfunction Study (Modified Barium Swallow (MBS)) Prep
» Varibar contrast in various
consistencies
~ Thick
~ Thin
~ Nectar
~ Honey
~ Pudding
» Cookies, crackers, diced fruit
» Paste or Barium Tablet
» Patient is given food of at least 3
different consistencies (liquid, paste
or puddinglike, and something
requiring mastication)
» Small amounts used (~1, 3, 5, 10 ml)
Technologist Role
Prepare room (tilt x-ray table to
upright position, set fluoro
console, arrange contrast and
any food)
▪ Help to position patient - either
in chair or standing upright
▪ Assist SLP and radiologist
▪ Clean up room
SLP Role
▪ Initial evaluation at bedside
▪ Administer contrast
▪ Evaluate patient
▪ Report findings in concert with
radiologist
Radiologist Role
▪ operate radiographic
equipment
▪ Document fluoro time and
report findings in concert with
SLP
▪ Video record study
Orthoroentgenography
»straight or right-angle radiography
»Performed to determine the length of long bones
»routine radiographs cannot be used for accurate measurements due
to magnification and elongation
»Comparative exam
»A ruler is taped into place on the table top
»The CR is centered directly over each joint space
»A Bell-Thompson ruler is placed under or next to the long bones
»A Bucky should be used for all exposures
»Make sure extremities are fully extended
»Make sure to use R and L markers
»Gonadal shielding can be used
»tube and Bucky are moved
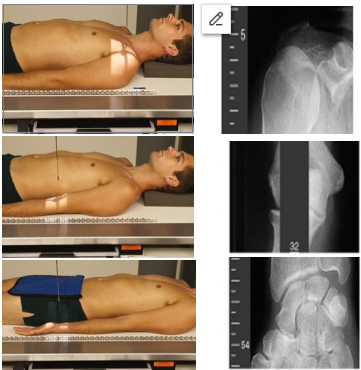
Upper limb measurement
AP shoulder
»Direct the CR to midshoulder joint
AP elbow
»Direct the CR to midelbow joint
AP wrist
»Direct the CR to midwrist joint
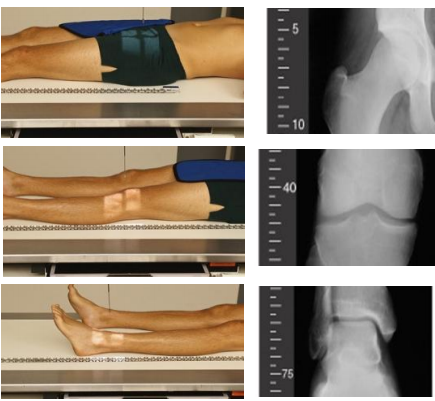
Lower limb measurement
AP hip
»Direct the CR to a level 3/4” above symphysis pubis
AP knee
»Direct the CR to a level 3/4” below apex of patella
AP ankle
»Direct the CR to level of ankle joint
Bone Age
»Single PA view of the LT hand to include the wrist and distal forearm
»Performed on children to determine normal v. abnormal “relative age” or “degree of maturation” of skeleton
»Radiologist compares radiograph against a standard of children of same chronological age
~ Greulich and Pyle (developed in the 1950s)
Soft Tissue/ Foreign Body
»Images with decreased technique to demonstrate the soft tissue structures
»Neck is most common soft tissue exam when no foreign body is suspected (see Upper Airway pg. 100)
»2 views at opposing 90-degree angles to show precise location (some exceptions)
»Technique may be reduced depending on system (DR/CR issues) and foreign material (glass v. wood v.
metal)
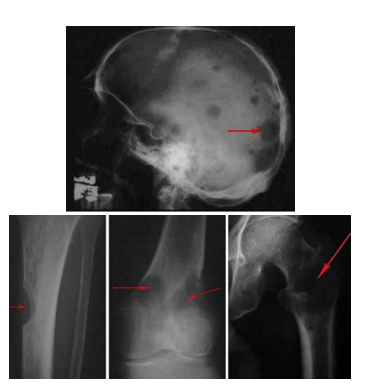
Bone Survey
Images of skeleton to
confirm presence of
certain pathologies (e.g.
multiple myeloma-cancer
of plasma cells)
Per radiologist protocol;
normally includes AP and
Lateral views of all long
bones, entire spine, skull,
and pelvis

Arthrography
»Contrast-media study of synovial
joints and related soft tissue
»Joints include the hip, knee, ankle,
shoulder, elbow, wrist, and TMJs
»Knee and shoulder are the most
common arthrograms
»MRI is most frequently used to
study the soft tissue structures of
the knee and shoulder
»MRI is also used in conjunction
with arthrography of the shoulder
and knee
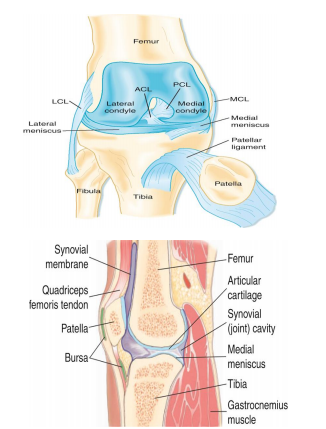
Major Structures of the Knee (6)
MCL (medial collateral ligament)
LCL (lateral collateral ligament)
ACL (anterior cruciate ligament)
PCL (posterior cruciate ligament)
Medial Meniscus
Lateral Meniscus
Knee Arthrogram
»Informed consent before procedure
»Performed in an R and F room that can perform horizontal beam radiography
»Scout AP and Lateral
»The radiologist prepares injection site (joint capsule injection via medial, lateral, anterior, or retropatellar approach)
»Synovial fluid is aspirated
»Contrast is administered
»Nine exposures are taken of the meniscus using 20º rotations of the knee
»Lateral or medial stress is applied to better visualize meniscus under fluoro
Shoulder Arthrogram
» Injection site is prepped the same way as for others
» A 2¾” to 3½” spinal needle is needed to reach the deep joint capsule
Commonly performed scout views for a shoulder arthrogram include:
AP internal/external rotation
Glenoid fossa (Grashey),
transaxillary, or bicipital groove
(Fisk) projections
Upright or Supine
Imaging sequence is then repeated post-contrast
If normal, the patient is instructed to exercise arm and the imaging sequence is repeated
Myelography
The radiography study of the spinal cord and its nerve root branches
• Largely being replaced by MRI or CT
• Some departments perform CT
• Most disk pathology of the spine occurs in the cervical and lumbar region
Contraindications
1. Blood in CSF
2. Arachnoiditis
3. Increased intracranial pressure
4. Recent LP
Post-Procedural Care
» Activity restriction
» Hydration
» Elevation of head
Myelography Prep
Informed consent before procedure
Risk of infection at injection site
Sedative/muscle relaxant for anxious patient
»The radiologist prepares injection site; then inserts the spinal needle.
»CSF fluid is collected
»Contrast is injected into the subarachnoid space
»A bandage is applied to puncture site after needle is removed
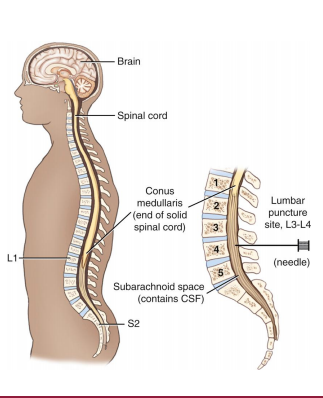
»Contrast is injected into the
subarachnoid space
»L3-4 is the most common
injection site for any myelogram
(cervical, thoracic, or lumbar)
»C1-C2 is used when lumbar area
is contraindicated – pathology or
blockage of vertebral canal
prevents flow of contrast to
thoracic or cervical regions
Equipment
»Performed in an R and F room that has ability to assume Trendelenburg position
»Shoulder braces
»Footrest
»IR with grids
» Razor
»Basin
»Prep sponges
»Sterile drapes
»Sterile gauze
» 5 ml and 20 ml syringes
» 25- and 22-guage needles
» 18-guage spinal needle
»Vial of local anesthetic
» Three test tubes
»Sterile gloves
»Antiseptic solution
» Lab requisitions – to send with CSF sample to lab
»Positioning wedge

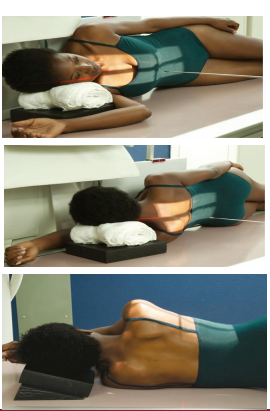
Myelography (Lumbar)
Prone and left lateral positions
» For prone – a positioning block is placed under
the abdomen to widen the interspinous spaces
» For left lateral – the patient flexes spine the to
widen the interspinous spaces
Contrast media
» Single contrast (9-15ml)
Lumbar region
Scout PA and Lateral at injection site (serves as l-spine scouts)
»Radiologist obtains fluoroscopic images
»Technologist obtains post contrast
~ Semi-upright x-table lateral
Myelography (Cervical)
Prone and upright positions
Neck is flexed to widen the interspinous spaces
Contrast media
» Single contrast (9-15ml)

Myelography (Thoracic)
Scout PA and Lateral at injection site
Scout PA and Lateral of Thoracic spine
Radiologist obtains fluoroscopic images
Technologist obtains post contrast
Right lateral decubitus
Left lateral decubitus
Right or left lateral recumbent
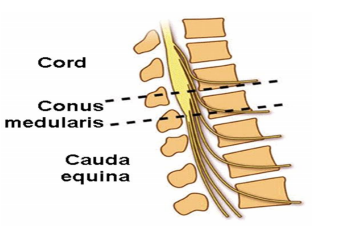
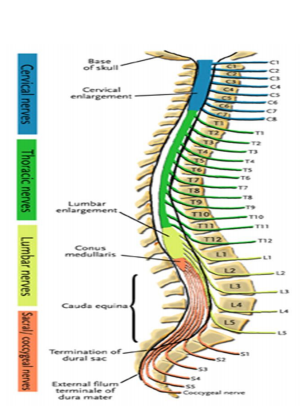
Conus medullaris
The terminal end of the spinal cord (L1-L2, can be T12-L3)
Lumbar, sacral, and coccygeal nerve roots descend from the conus medullaris, which is termed the cauda equina (horse's tail)
Normal platelet count is approximately ____
150-400k
Prothrombin Time (PT): normal time is approximately ____ for liquid portion of blood (plasma) to coagulate
11-13.5 secs
International Normalized Ratio (INR): INR was devised to standardize PT results. Times can vary if patient is on anti-coagulation therapy. Normal should be approximately
0.8 to 1.1
Warfarin: 2-3
Partial Thromboplastin Time (PTT): clotting should occur approximately between _
25-35 secs
Creatinine Value
0.6-1.5 mg/dL
BUN Value
8-25
GFR Ranges
90-60-45-30
III Procedures
» Arthrogram
~ Knee
• AP
• Lateral
~ Shoulder
• AP internal/external rotation
• Glenoid fossa (Grashey), transaxillary, or bicipital groove (Fisk)
» Myelogram
~ Cervical
• PA prone
• X-table Lateral
• X-table Swimmer’s
~ Thoracic
• PA prone
• Right lateral decubitus
• Left lateral decubitus
• Right or left lateral recumbent
~ Lumbar
• Semi-upright x-table lateral
I & II Procedures
» Hysterosalpingogram (pp. 724-726)
» Swallowing Dysfunction Study
» Long bone measurement (pp. 731)
~ Upper limb
~ Lower limb
» Bone survey
» Bone age
» Soft tissue/foreign body