PHTY2101 Module 4 - Spinal Cord Injury
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
incidence of spinal cord injuries in Australia and QLD
300-400 cases Australia
80-90 cases QLD
most common causes of spinal cord injuries in QLD
68% trauma mostly surf/dive, MVA, bike, rugby
incidence declining due to seatbelts, RBTs etc
what is the most commonly injured region of spinal cord
55% are cervical, remainder equal between Tx, Lx, Sx
4 most common spinal cord levels injured and why
1. C5
2. C4
3. C6
4. T12
- most mobile parts of vertebral column
most common type of spinal cord injury
compression
how does compression of spinal cord cause neurological damage
causing inflammation which cuts of blood supply, causing necrosis and damage to spinal cord
what are 3 characterises of an upper motor neuron lesion
- injuries above the conus medullaris
- spinal cord mediated reflex are still intact
- results in spastic paralysis (unless ischaemic damage too, then more flaccid)
3 characteristics of lower motor neuron lesion
- involve cauda equina
- loses spinal cord mediated reflexes
- results in flaccid paralysis
what are mixed lesions to spinal cord
involve upper and motor lesions
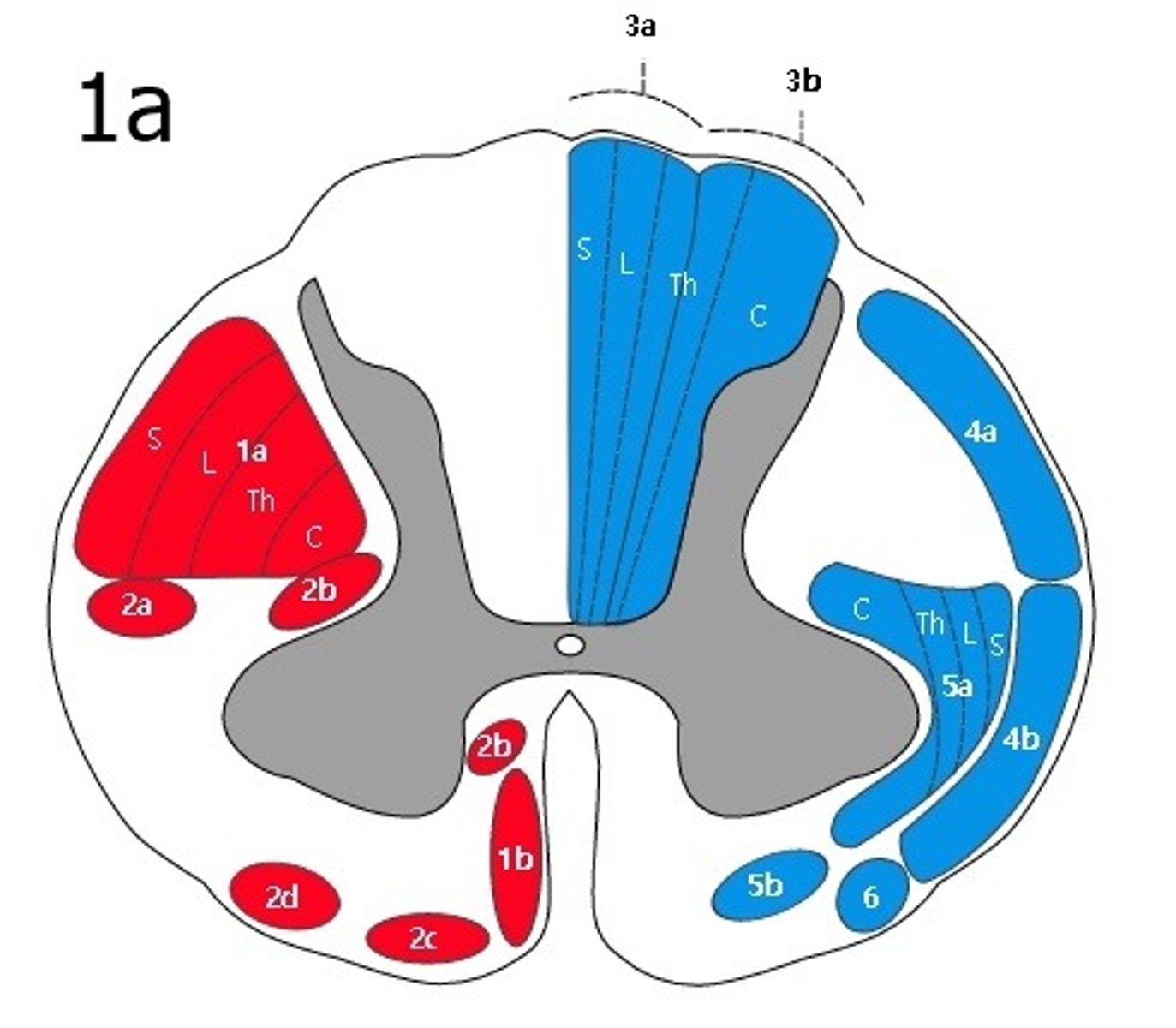
describe dorsal column tract
- what does it do
- where do fibres decussate
- light touch and proprioception
- decussate in brainstem
what does lateral spinothalamic tract do and where do fibres decussate
- pain and temperature
- decussate in spinal cord when they enter
what does anterior spinothalamic tract do and where do fibres decussate
- crude touch
- fibres decussate in spinal cord when they enter
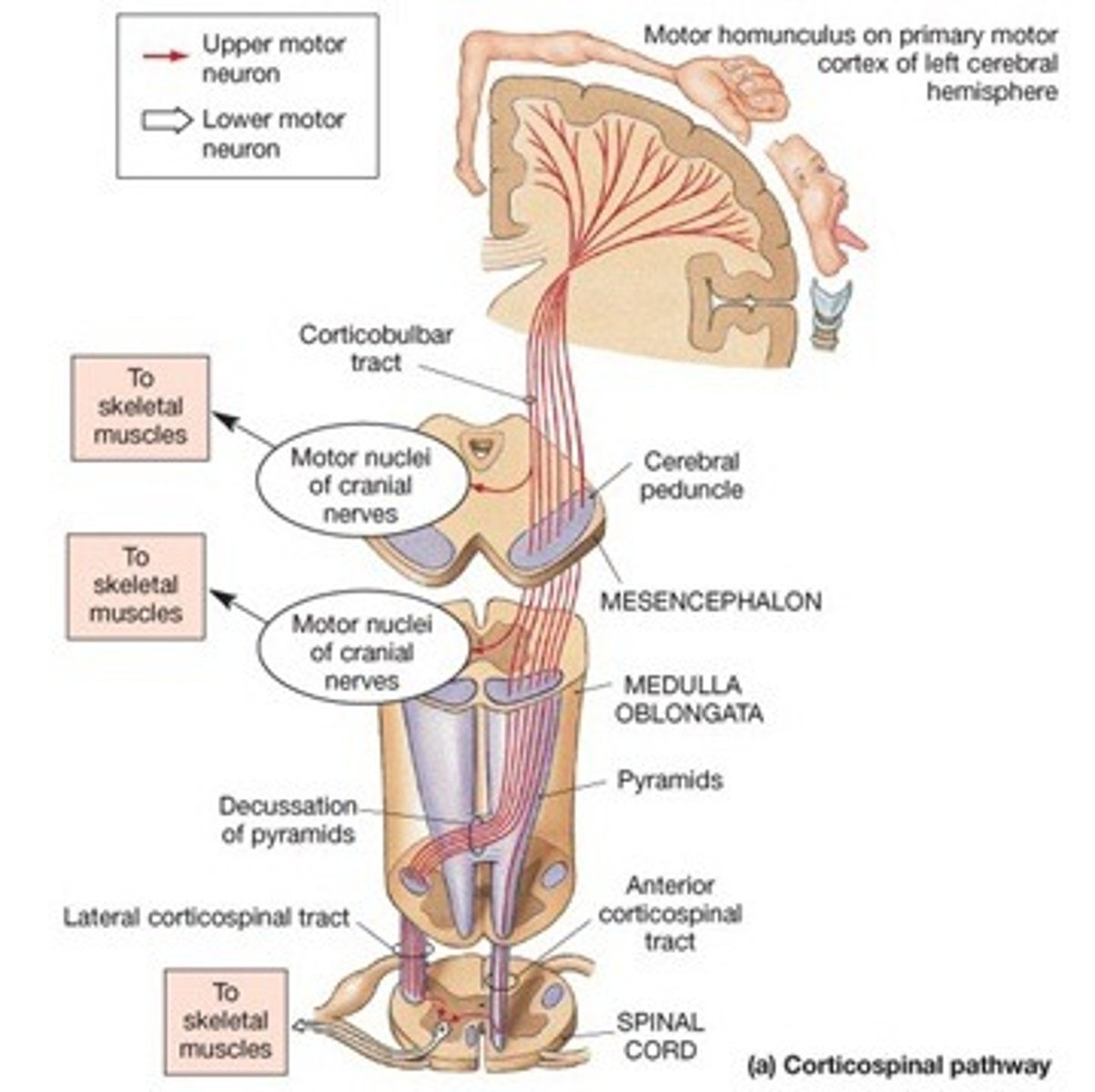
what does pyramidal tract do and where do fibres decussate
- voluntary motor control
- 85% of fibres decussate in brainstem
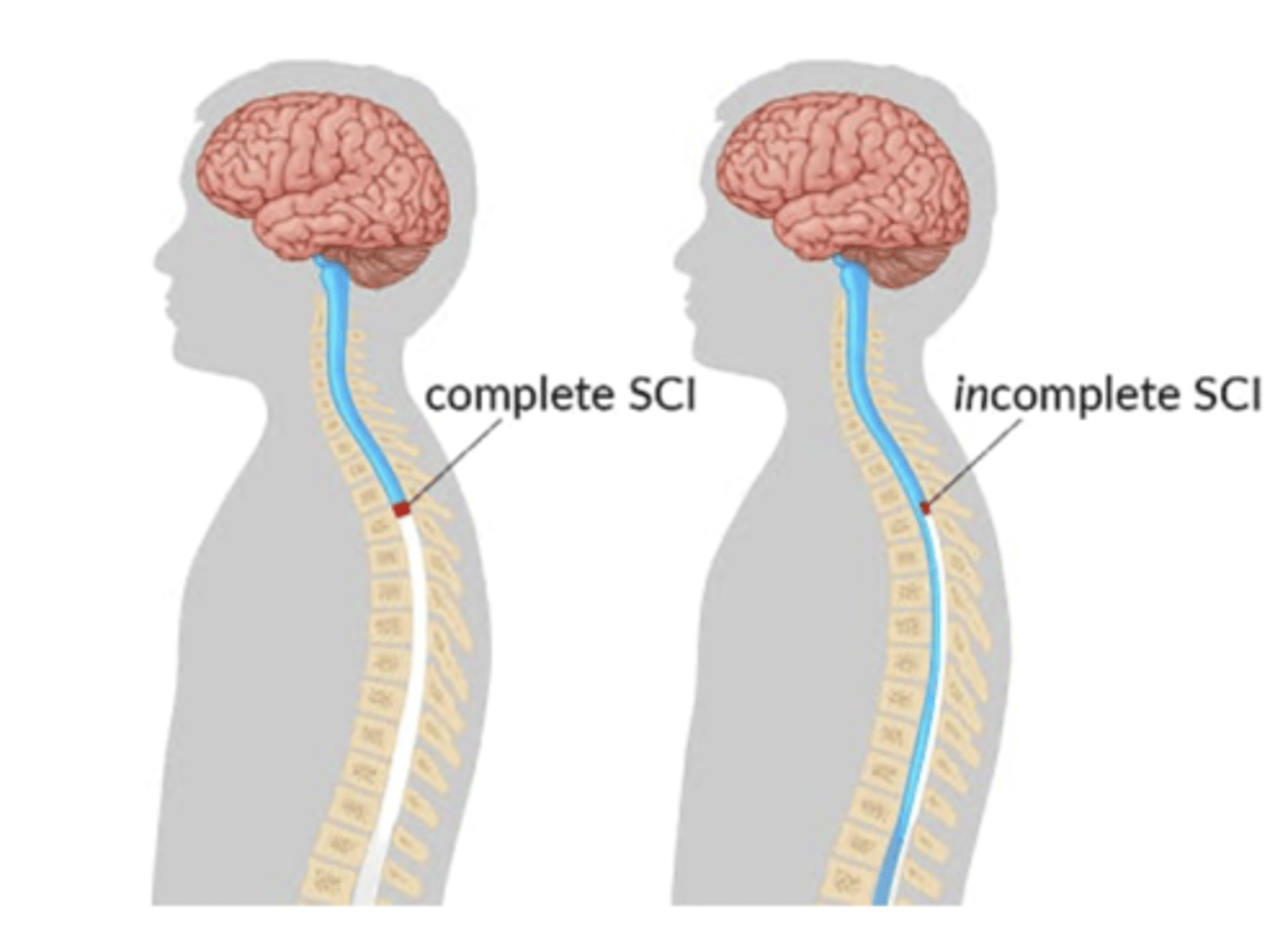
identify 4 types of incomplete spinal cord injuries
1. central cord lesion
2. sacral sparing
3. anterior cervical cord syndrome
4. Brown-Sequard Syndrome
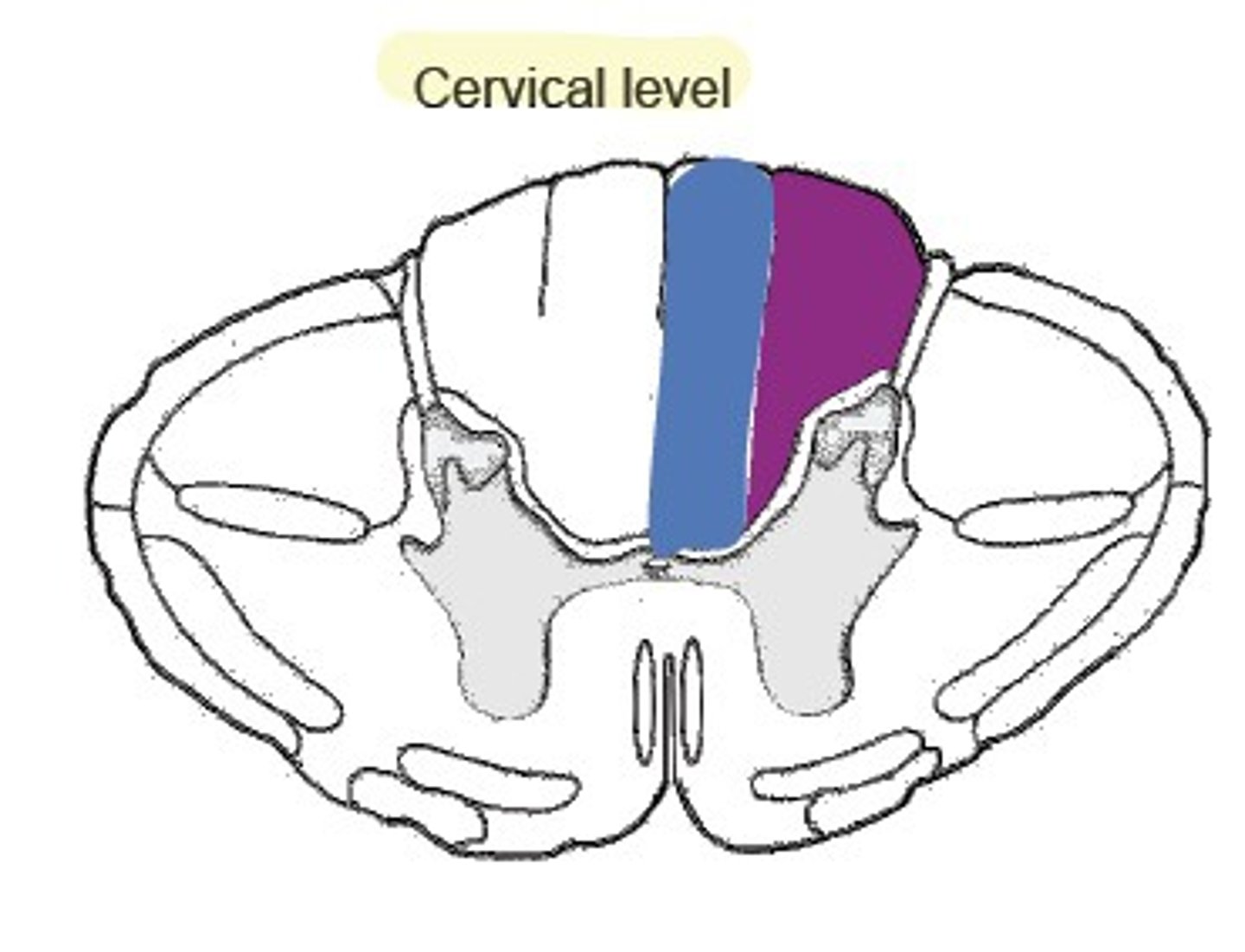
describe a central cord lesion
- typically hyperextension injury of cervical spine
- causes compression, hypoxia, haemorrhage of central grey matter of spinal cord while peripheral rim remains intact
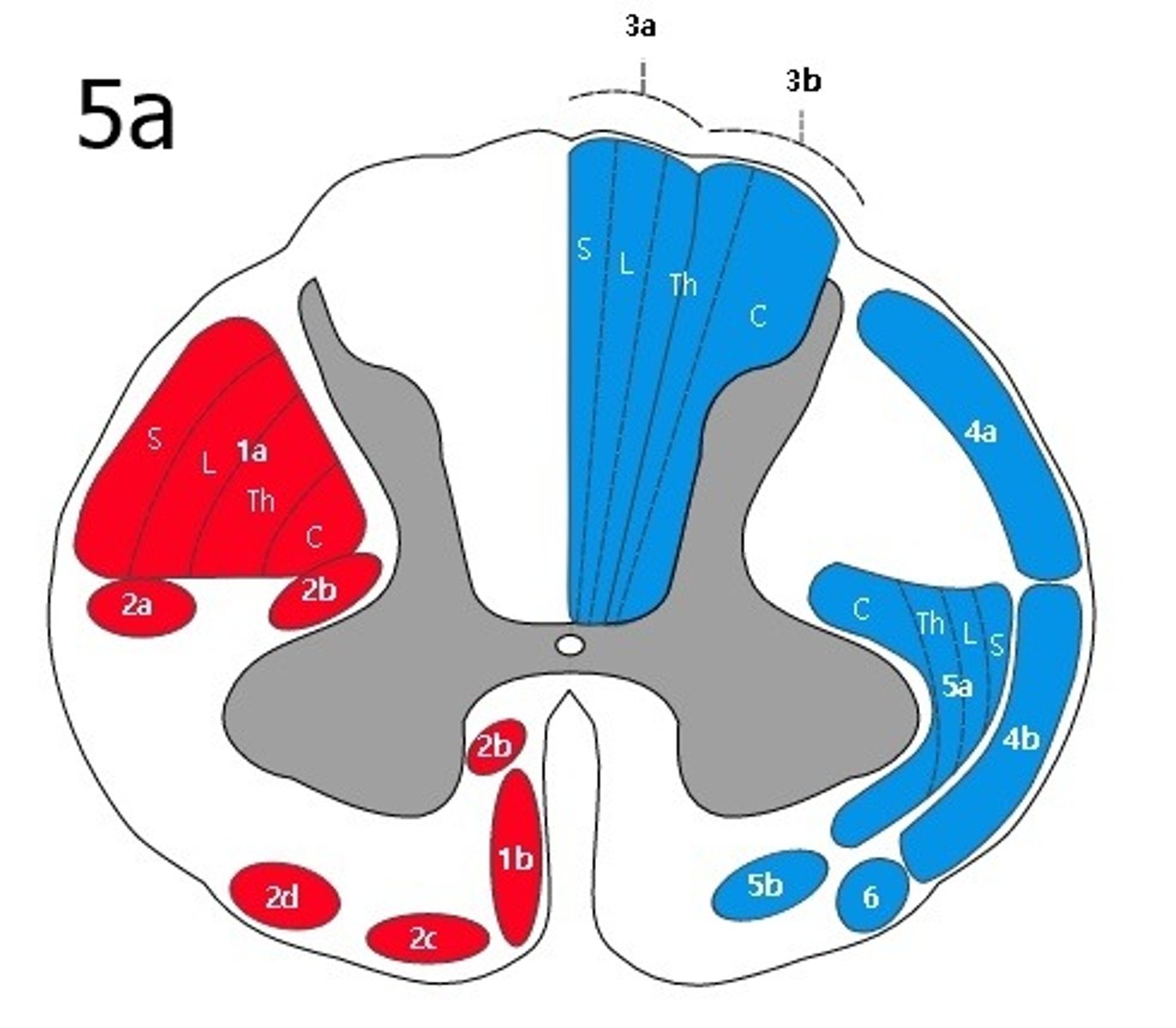
- typically severe paralysis of UL, more so than LL because cervical (UL) motor tracts are located centrally (see 1a on image)
what is sacral sparing
- only peripheral rim of spinal cord is spared, so sacral segments remain intact
- retains sacral S4-S5 sensation, voluntary anal control, bladder and bowel function, possibly toe movement
what is anterior cervical cord syndrome
- flexion injury that damages the anterior 2/3 of spinal cord
- preserves dorsal column (light touch and proprioception) but no motor function, pain, or temperature sensation below level of lesion
what is Brown-Sequard Syndrome
- A hemisection lesion of the cord usually from penetrating injury
- loss of ipsilateral motor, light touch, proprioception (decussate in brainstem)
- loss of contralateral pain and temp. (cross in spinal cord)
5 steps to a spinal cord injury timeline
1. primary injury occurs
2. inflammation, ischaemia, necrosis
3. spinal shock - flaccidity, no reflexes, systems shut down, excitotoxicity
4. cells recover -> some reflexes and tone recovery
5. neurological recovery? if any?
what is autonomic dysreflexia
- a life-threatening emergency in spinal cord injury patients
- body picks up signals of pain that it can't interpret, commonly bladder/bowel injury, ingrown toenails, pressure sores, fractures, kidneys stones, menstrual cramps
- causes a sudden hypertension
- symptoms are severe headache, nausea, nasal congestion, and bradycardia, goosebumps or blotchy skin flushing above injury level, SOB, blurred vision
how to conservatively manage an unstable vertebral column fracture
- remove debris to relieve pressure on spinal cord
- special bed to turn patient, timed with physio interventions
- skull traction to realign vertebral column
- bed rest managed with pillow, bracing, catheter
- restrictions for ROM based on level of injury
how to surgically manage a vertebral fracture
- decompression and fusion - realign vertebral column and fuse it together to reduce instability
why might a spinal cord injury patient need respiratory management
- lack of lateral expansion and function of inspiratory muscles
- inability to clear chest due to lack of force from abdominal muscles
- fatigue of respiratory muscles due to increased work of breathing
3 ways to manage respiratory problems in spinal cord injury patients
- optimal positioning for ventilation
- machines: positive pressure, hyper-inflators, cough assist
- techniques: deep inhalation holds, straws, blowing bubbles, rib springing, percussion, vibration
what does the ASIA scale measure
- sensation (light touch and pinprick) and motor function (5 key UL and LL muscles)
- looks at last spinal cord level that is normal and has grade classifications of completeness of injury
what do each of ASIA scale grades mean
A = complete = no sensory or motor function preserved in SACRAL segments S4/S5 - means patient could still be up and walking around even with 'complete' spinal cord injury
B = sensory incomplete = sensory but no motor function below injury level and sacral segments S4/S5
C = motor incomplete = motor function preserved at S4/S5 but more than half the key muscles below injury have muscle grade <3
D = motor incomplete = C but more than half key muscles below injury have muscle grade >3
E = normal
identify the 3 parts to ASIA examinatino
1. sensory exam - light touch (cotton tip)
2. sensory exam - sharp/blunt discrimination
3. motor exam - grade 10 key muscles
how is an ASIA grade determined
last level of spinal cord on each side where both sensory and motor functions were normal
+
grade scale of sensory/motor complete/incomplete
what is a zone of partial preservation
- dermatomes and myotomes below the neurological level that remain partially innervated
- i.e. lowest segment with some sensory and/or motor function
what zone of partial preservation is more likely to progress to motor incomplete injury
≥3 levels below sensory sparring
describe how spinal cord injuries are rehabilitated after hospital discharge
- transitional rehab program team generally involves physio, social worker, OT, and nurse
- goal based program lasting 6-8 weeks post discharge to allow carry-over into community
- aim to optimise quality of life and independence in ADLs
4 key parts of a physiotherapy program for rehabilitation of spinal cord injuries out of hospital
1. assessment of key impairments
2. setting agreed-upon goals to address limitations
3. identifying, developing, administering treatments
4. measuring outcomes
list some principles to a spinal cord rehabilitation program
1. variety - range of areas on different days
2. motivate - achievable goals, slowly build up range/strength
3. client re-education focus - problem-solving skills, functional re-training
4. honesty -
5. set SMART goals
how to redistribute pressure from wheelchair
1. use pressure lifts, pressure leans, tilt-in-space wheelchair
2. change positions every 20-30 mins if possible
3. cushion reduces pressure injuries, doesn't stop them
4. monitor injuries and regress back to bed at slightest sign
how are tilt tables beneficial
- gravity assisted drainage of swelling
- stretch ankles
- psychological boost
what is FES
- functional electrical stimulation
- use a current to stimulate a paralysed muscle to create a movement pattern around function