Respiration Pt 2
1/46
Earn XP
Description and Tags
BMS 300 Unit 4 Exam
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
What is pulmonary ventilation?
The mechanical movement of air into and out of the lungs (breathing).
What is external respiration?
Gas exchange between the external environment and the blood, occurring at the alveoli.
What is internal respiration?
The absorption of oxygen and release of carbon dioxide waste by body cells.
State Boyle's Law and its equation.
Pressure is inversely proportional to volume at constant temperature. P = 1/V, or P1V1 = P2V2.
What are the two layers of the pleura and what does each cover?
Parietal pleura covers the inner thoracic wall and diaphragm. Visceral pleura covers the lungs.
What is pleuritis and what causes it?
Inflammation of the pleura, often from infections. Causes sharp, stabbing pain when breathing.
What is pleural effusion?
A buildup of fluid in the pleural cavity, often from heart failure. Causes chest pain and shortness of breath.
What pressure condition triggers inspiration?
Inspiration occurs when intrapulmonary pressure is less than atmospheric pressure.
Which muscles contract during normal inspiration and what do they do?
The diaphragm (moves inferiorly) and external intercostal muscles (lift ribs) contract to expand thoracic volume.
What is compliance in the lungs?
A measure of the ability of alveoli to expand or inflate. Increased by surfactant, negative intrapleural pressure, and tissue elasticity
What does surfactant do in the alveoli?
It reduces surface tension within the alveoli, allowing the walls to separate and making it easier to inflate.
What pressure condition triggers expiration?
Expiration occurs when intrapulmonary pressure is greater than atmospheric pressure.
How does normal (passive) expiration occur?
The diaphragm and external intercostals relax, decreasing thoracic volume and increasing pressure, pushing air out.
What muscles are used in forced expiration?
Contraction of abdominal muscles and internal intercostal muscles.
What is elastic recoil?
The ability of alveoli to return to their original shape after being stretched. Driven by surface tension and elastic fibers.
What is a pneumothorax and what happens to the lung?
Air enters the pleural cavity. Intrapleural pressure equalizes with atmospheric pressure, causing the lung to collapse (atelectasis)
In a chest puncture causing a collapsed lung, what happens to intrapleural pressure and intrapulmonary volume?
Intrapleural pressure increases (equalizes with atmosphere) and intrapulmonary volume decreases (lung collapses).
What are the three layers of the respiratory membrane?
Alveolar epithelium
Capillary endothelium
Fused basement membrane.
State Fick's Law: what is diffusion rate proportional and inversely proportional to?
Proportional to: surface area, gas diffusion coefficient, partial pressure gradient. Inversely proportional to: membrane thickness.
How does emphysema impair gas exchange?
It destroys alveolar tissue, reducing surface area for diffusion. Greater compliance and less elastic recoil — easy to inhale, hard to exhale.
How does pulmonary fibrosis impair gas exchange?
It causes thick and stiff alveolar tissue, increasing membrane thickness and making it difficult to move gases across.
How does CO2 solubility compare to O2 in plasma?
CO2 is 20 times more soluble in plasma than O2. Nitrogen is practically insoluble in plasma.
A chest puncture wound that causes a collapsed lung most likely results in _____ intrapleural pressure and _____ intrapulmonary volume
increased, decreased
The rate of oxygen diffusion across the air-blood interface is decreased in both emphysema and pulmonary fibrosis, but by different mechanisms. Emphysema decreases the _____ of the alveoli, whereas pulmonary fibrosis increases the _____ of the alveoli.
Surface area; thickness
State Henry's Law.
Gases dissolve in liquids in proportion to their partial pressures. Amount dissolved also depends on solubility.
How is oxygen transported in the blood, and what percentages apply?
98% is bound to hemoglobin (Hb). 2% is dissolved in plasma
What are the partial pressure gradients that drive O2 movement?
Alveoli (PO2=100 mmHg) → pulmonary capillaries (PO2=40 mmHg).
Systemic capillaries (PO2=100 mmHg) → tissues (PO2=40 mmHg).
How is CO2 transported from the tissues into the blood? Give the three forms and their percentages.
7% is dissolved in plasma
23% is dissolved in hemoglobin
70% is transported as bicarbonate (HCO3-)
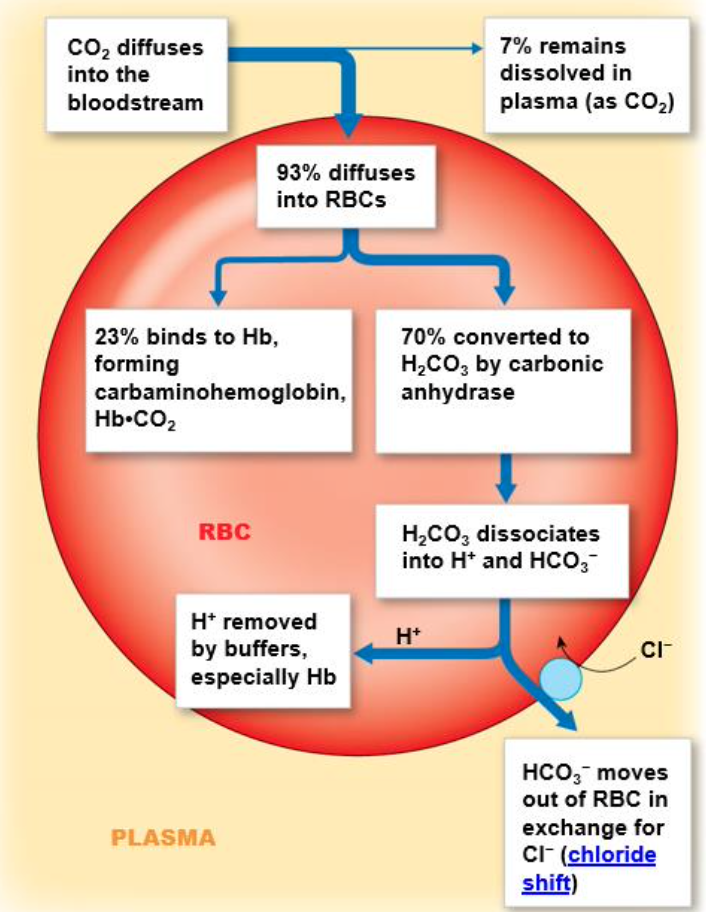
What is the chloride shift?
At the tissues, HCO3- moves out of the erythrocyte in exchange for Cl2
At the lungs, the reverse occurs — HCO3- moves back in and Cl2 moves out
What enzyme catalyzes CO2+ H2O → H2CO3, and where does this occur?
Carbonic anhydrase. The reaction occurs inside red blood cells.
What is the normal blood pH range, and what are acidosis and alkalosis?
Normal: 7.35–7.45
Acidosis: pH < 7.35 (excess H+)
Alkalosis: pH > 7.45 (too little H+)
How does the bicarbonate buffering system respond to acidosis vs. alkalosis?
Acidosis: reaction shifts left → removes H+ by forming CO2+ H2O.
Alkalosis: reaction shifts right → adds H+ by forming H2CO3 → H+ + HCO3-.
Why is the oxygen-hemoglobin dissociation curve sigmoidal?
Due to positive cooperative binding — each O2 bound causes a conformational change in Hb that makes the next O2 binding easier.
Why does fetal hemoglobin have a higher O2 affinity than adult hemoglobin?
Fetal Hb uses two alpha and two gamma chains. This higher affinity allows the fetus to 'steal' oxygen from maternal hemoglobin across the placenta.
What is myoglobin and why does it have a higher O2 affinity than hemoglobin?
Myoglobin is found in cardiac and skeletal muscle. It has only one binding site (no cooperative binding), giving it a hyperbolic curve and much higher affinity. It stores O2 for rapid use.
What causes a right shift of the O2 dissociation curve and what does it mean?
Caused by increased heat, CO2, H+, or 2,3-BPG (byproducts of metabolism/exercise).
Right shift = reduced Hb affinity for O2 = increased O2 unloading at active tissues
What causes a left shift of the O2 dissociation curve and what does it mean?
Caused by decreased temperature, CO2, H+, or 2,3-BPG.
Left shift = increased Hb affinity for O2 = decreased O2 unloading at tissues.
What is 2,3-BPG and why is it relevant?
2,3-bisphosphoglycerate is a byproduct of glycolysis. It binds hemoglobin and reduces O2 affinity, promoting a right shift and greater O2 unloading during exercise.
What is the Haldane Effect?
Deoxygenated Hb has greater affinity for CO2; oxygenated Hb has lower affinity. This promotes CO2 binding at the tissues and O2 binding at the lungs when CO2 is released
What is the Bohr Effect?
CO2 and H+ binding to hemoglobin decreases its affinity for O2 (right shift). This promotes O2 unloading at metabolically active tissues where CO2 and H+ are high.
Where does the Bohr Effect occur — systemic or pulmonary capillaries?
Systemic capillaries (at the tissues, e.g. legs, arms, abdomen). High CO2 and H+ from metabolism reduce Hb's O2 affinity, unloading more O2
What is the role of the brainstem in respiratory control?
The respiratory center in the brainstem (pons and medulla) receives input from chemoreceptors and sends efferent signals via phrenic and intercostal nerves to the diaphragm and intercostal muscles
How do central chemoreceptors work?
CO2 crosses the blood-brain barrier → carbonic anhydrase converts it to H+ in CSF → H+ binds central chemoreceptors → signals respiratory center → increased ventilation.
↑CO2 → ↑H+ → ↑ventilation.
What are peripheral chemoreceptors and where are they located?
Carotid bodies in the walls of carotid arteries (sample blood to brain) and aortic bodies in the walls of the aorta (sample blood to body).
Sense ↑CO2 or ↓O2 → increase ventilation
What is hypercapnia and how does the body respond?
Hypercapnia = increase in arterial PCO2, caused by hypoventilation (slow breathing). CO2 buildup stimulates chemoreceptors → respiration rate increases to blow off excess CO2.
What is hypocapnia and how does the body respond?
Hypocapnia = decrease in arterial PCO2, caused by hyperventilation (fast breathing). Low CO2 fails to stimulate chemoreceptors → respiration rate decreases. Can cause dizziness or loss of consciousness.
What is the primary driver of respiratory rate — CO2 or O2?
CO2 (monitored as H+) is the primary driver. Peripheral chemoreceptors do monitor O2, but O2 must drop to very low levels before triggering increased ventilation.