Anaesthesia
1/450
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
451 Terms
Define anaesthesia
Dose-dependent state produced by drugs that renders the patient insensible to pain through CONTROLLED and REVERSIBLE toxicity of the CNS or nociceptor blockage → CNS depression → Less interpretation of signals
Function: Humane chemical restraint for radiography, examination, minor procedures, control of seizures, euthanasia, surgery
vs. euthanasia = Uncontrolled and irreversible CNS toxicity
ALL GA agents are excellent euthanasia agents
Compare the safety of pre-medication drugs vs. GA drugs
Pre-med (sedatives/analgesia) = High TI (10 - 50) → Safer
GA = Low TI
Injectable TI < 10 (except ketamine > 10)
Inhalant TI < 2 - 4
3 Properties required for GA (anaesthetic triad)
Narcosis = Amnesia and unconsciousness
Analgesia
Muscle relaxation (except ketamine)
Phases vs. stages of anaesthesia
Phases of anaesthesia = Process of anaesthetising a patient
Pre-anaesthetic → Recovery
Stages of anaesthesia = Progressive changes that occur during administration of GA agent which indicate anaesthetic depth
Stage I (excitation) → Stage Iv (bulbar paralysis)
5 Phases of anaesthesia
Definition
Duration
Procedures performed
Pre-Anaesthetic = Preparation of patient AND equipment
Duration: 6 - 24hr pre-induction
Procedures:
Fasting
Pre-anaesthetic assessment (history and PE)
Pre-anaesthetic drugs
Stabilisation and support
Formulate anaesthetic plan/protocol
Equipment and drug preparation (eg. equipment tray, monitoring equipment and anaesthetic circuit checks)
Pre-Medication = Provide sedatives and analgesia BEFORE induction
Duration: 30 - 60 minutes pre-induction
Procedures:
Place IV catheter
Consider clipping if patient is unstable (otherwise after induction)
Induction = Administer GA drugs to produce unconsciousness
Duration: 5 - 15 minutes
Procedures: High risk phase due to rapid loss of consciousness → Anaesthetic ABCs
Maintenance = Administer drugs to maintain anaesthesia and support the patient
Duration: Depends on procedure
Procedures: Use of dangerous drugs → Monitoring q5 minutes and interventions when necessary
Recovery = Cessation of drugs and ET extubation
Duration: Depends on drugs used and length of procedure (takes 24 - 48hr to return to normal function)
Procedures: High risk phase → Monitor q15 minutes
Hypnotic vs. dissociative GA agents
Hypnotic agents → CNS depression through agonism of GABA-A = Main inhibitory neurotransmitter in the CNS → Increased influx of Cl- into neuron → Inhibition of pain pathways and action potentials
Every GA agent except ketamine (eg. propofol, alfaxalone, thiopentone, etomidate)
Dissociative agents → CNS excitation through interaction with NMDA receptors = Main excitatory neurotransmitter in the CNS (to the point where normal consciousness and reflex messages cannot be processed)
eg. Ketamine and tiletamine
List the 3 main consequences/considerations/complications of GA
3 Hypo’s:
Hypotension (MAP = CO x SVR)
Hypoventilation (minute ventilation = RR x TV which is determined by PaCO2)
Hypothermia
Describe the TWO phases of the cardiac cycle (+ normal ratio)
Systolic = Ventricular contraction
Diastole = Relaxation of ventricles (heart refills with blood)
Myocardial perfusion via coronary artery circulation
Atrial systole at the END of diastole (empties remaining blood from A → V)
Diastole:Systole = 3:1 → Required for adequate myocardial perfusion
What is the most important determinant of tissue perfusion? (+ normal and equation)
MAP = DAP + 1/3(SAP - DAP)
MAP = 93 - 95mmHg
Closer to DAP as it lasts longer except with tachycardia → 1/3 → ½ in equation as diastole : systole = 1:1
SAP/DAP = 120/80mmHg
Why is a giraffe/elephant’s normal MAP much higher?
Relates to the position of the head above the heart → Higher MAP required for cerebral perfusion
MAP decreases as brain is lowered closer to the heart (eg. drinking water)
What is an acceptable MAP/SAP under GA? What are 3 organ effects when MAP drops below the level?
Acceptable MAP under GA > 60 - 70mmHg (SAP > 90mmHg) otherwise:
AKI (kidneys have high perfusion requirement and little regenerative capacity)
Muscle myopathy (horses) → Maintain MAP > 85mmHg
Liver/skin → NO effect (high regenerative capacity and can cope with reduced blood flow)
5 Main effects of anaesthesia on CVS
Negative chronotropy = Decrease HR
Does NOT impact CO due to compensatory increase in SC = more time for ventricular filling
Negative inotropy = Decrease contractility via myocardial depression (decreased SV)
Peripheral vasodilation (reduced SVR → reduced MAP = CO x SVR)
Hypotension during GA due to vasodilation NOT CO
Arrhythmia
Impaired homeostatic reflexes (eg. baroreceptors)
What is “dead space”? What are 3 different types?
Dead Space: "Proportion of tidal volume that is NOT available for gas exchange (ventilation but no perfusion)
Types:
Anatomical dead space = Fixed part of the airway that does NOT participate in gas exchange (aka. conducting zone)
Respiratory zone = Airway structures that participates in gas exchange (alveoli)
Conducting zone = Airway structures that do NOT participate in gas exchange → Conduit for air to travel to the respiratory zone
Alveolar dead space = Poorly perfused alveoli which cannot participate in gas exchange
Equipment dead space = Added dead space from anaesthesia equipment (eg. ET tubes and poorly functional breathing circuits)
Dead space : Alveoli ratio = 1:2
Describe the mechanism of breathing
Contraction of respiratory muscles expand thoracic cavity and abdominal organs moved caudally
Diaphragm
Intercostals
2˚ respiratory muscles of head and neck when other muscles fatigue or during respiratory failure
Lungs are fixed to the chest wall through surface tension of fluid in the pleural space
Negative pressure in airway = Air moves into alveoli
Negative pressure → Structures up stream of thorax are prone to collapse (airway obstruction prevented by cartilage/bone in nares, larynx, trachea and bronchi)
Pulmonary pump = Negative pressure causes distension of compliant blood vessels to assist blood movement → Increase venous return and CO
Passive expiration = Chest wall and lung return to normal position by elastic recoil of the lungs
NOT horses (passive phase → active phase with contraction of abdominal wall muscles)
Breathing vs. ventilation
Breathing = Physical movement chest wall and diaphragm
Ventilation = Gas exchange at the level of the alveoli defined level of CO2 in arterial blood (high PaCO2 = hypoventilation)
Patient can be breathing but NOT ventilating
Minute volume = RR x TV
#1 driver of ventilation = PaCO2 (+ pH and PaO2) → Detected by peripheral chemoreceptors and baroreceptors
Main effects of anaesthesia on respiratory system
Muscle relaxation of URT → Respiratory obstruction (esp. brachycephalics)
Nasal oedema and haemorrhage
Medullary respiratory centre depression → Reduced sensitivity to hypercapnia → hypoventilation
Higher PaCO2 required to stimulate normal ventilation
Impaired thoracic wall movement due to muscle relaxation and recumbency → Lungs squashed by organs or when dependent
V:Q mismatch due to:
GA depression of CVS → Hypotension and reduced CO → Reduced Q
Under-perfusion of upper lungs (above heart and blood pools with gravity) and under-ventilation of dependent lungs (atelectasis)
Inhibition of the hypoxic pulmonary vasoconstrictive reflex
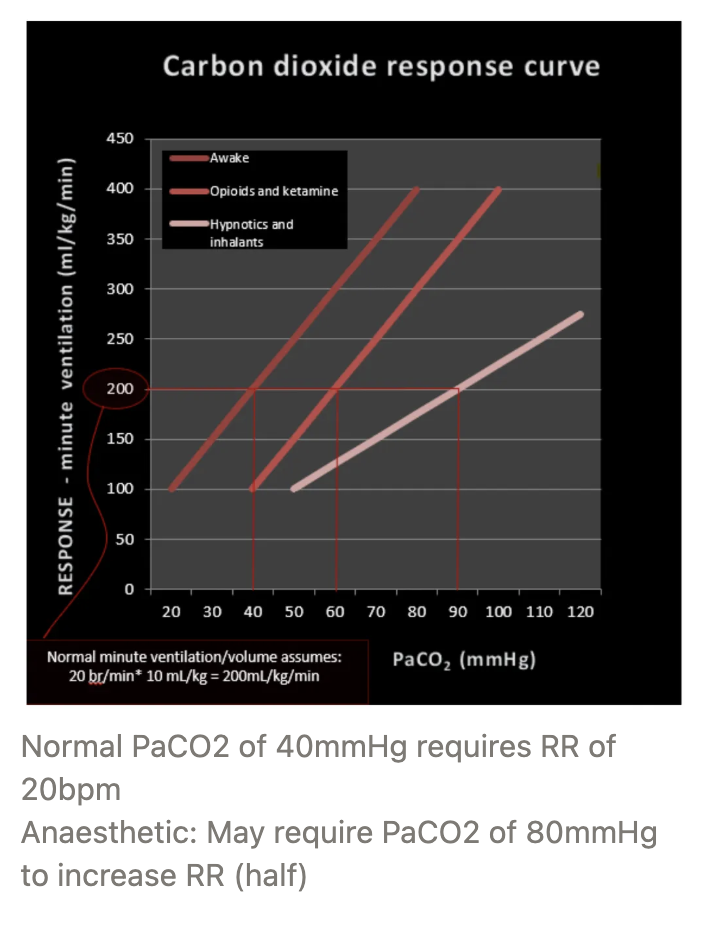
Hypoventilation (PaCO2 = and when treatment is required)
PaCO2 > 45mmHg
PaCO2 of 55 - 60mmHg = minimal consequences on pH due to carbonic acid formation (PaCO2 > 60mmHg required treatment)
PaO2 vs. SaO2 vs. FiO2
PaO2 = Arterial partial pressure of O2 (amount of O2 in arteries)
SaO2 = Arterial saturation of Hb (amount of O2 attached to Hb)
PaO2 and SaO2 does NOT have a linear relationship (oxydissociation curve) → Good SaO2 with room air
FiO2 = Fractional inspired O2
PaO2 proportional to FiO2 (PaO2 = 5 x FiO2)
3 Advantages and disadvantage of fasting during the pre-anaesthetic period
Advantages: Empty stomach →
Reduced risk of vomiting or gastroesophageal reflux (GOR)
GA patients have obtunded protective reflexes (gag reflex of larynx to seal off airway)
Reduced weight of GI → Less pressure on thorax while in dorsal recumbency → Reduced risk of respiratory embarrassment and hypoventilation
Respiratory embarrassment = Impaired breathing caused by a distended stomach against the diaphragm
More accurate assessment of small mammal weight → Appropriate dosing of drugs
Disadvantage: Prolonged fasting → Increased HCl in GI contents → Increased morbidity
Incidence and 3 potential outcomes of gastroesophageal reflux during GA
Incidence: 30 - 40%
Outcomes:
Regurgitation → Stomach contents seen coming out of mouth or nose
Treatment: Flush oesophagus immediately → Effective in reducing morbidity
Oesophagitis (fast onset of clinical signs) → Oesophageal stricture (slow onset of clinical signs)
Aspiration pneumonia → Tracheitis, stricture ± death by asphyxiation
3 Risk factors for GOR (+ examples)
Physiological
GI disease (history of nausea and vomiting)
Brachycephalics
Pregnant animals
Procedural
Fasting >6 - 12hr → More HCl → More lethal if GOR occurs
GI surgery
IVDD disease
Laryngeal paralysis → Aspiration pneumonia
Intracranial surgery
Pharmacological
Peri-op NSAIDs
Atropine
Morphine
Propofol
Fasting Duration for dogs and cats (water + food + why?)
Food = 12hr (ideally 4 - 6hr with ½ MER as wet food → faster passage through GIT but not convenient for owner)
Water = Free access until pre-medication (passes straight through GIT)
5 Indications for pre-anaesthetic drugs (+ examples)
Reduce risk of regurgitation (eg. brachycephalics → omeprazole and maropitant)
Stabilise patient with pre-existing disease
Analgesia for pre-existing pain (eg. methadone, ketamine, gabapentin for chronic pain)
Existing medications that should/should NOT be stopped
Do NOT stop exogenous steroids
Stop NSAIDs 24hr prior
Aggressive/anxious dog → Gabapentin, trazadone, melatonin
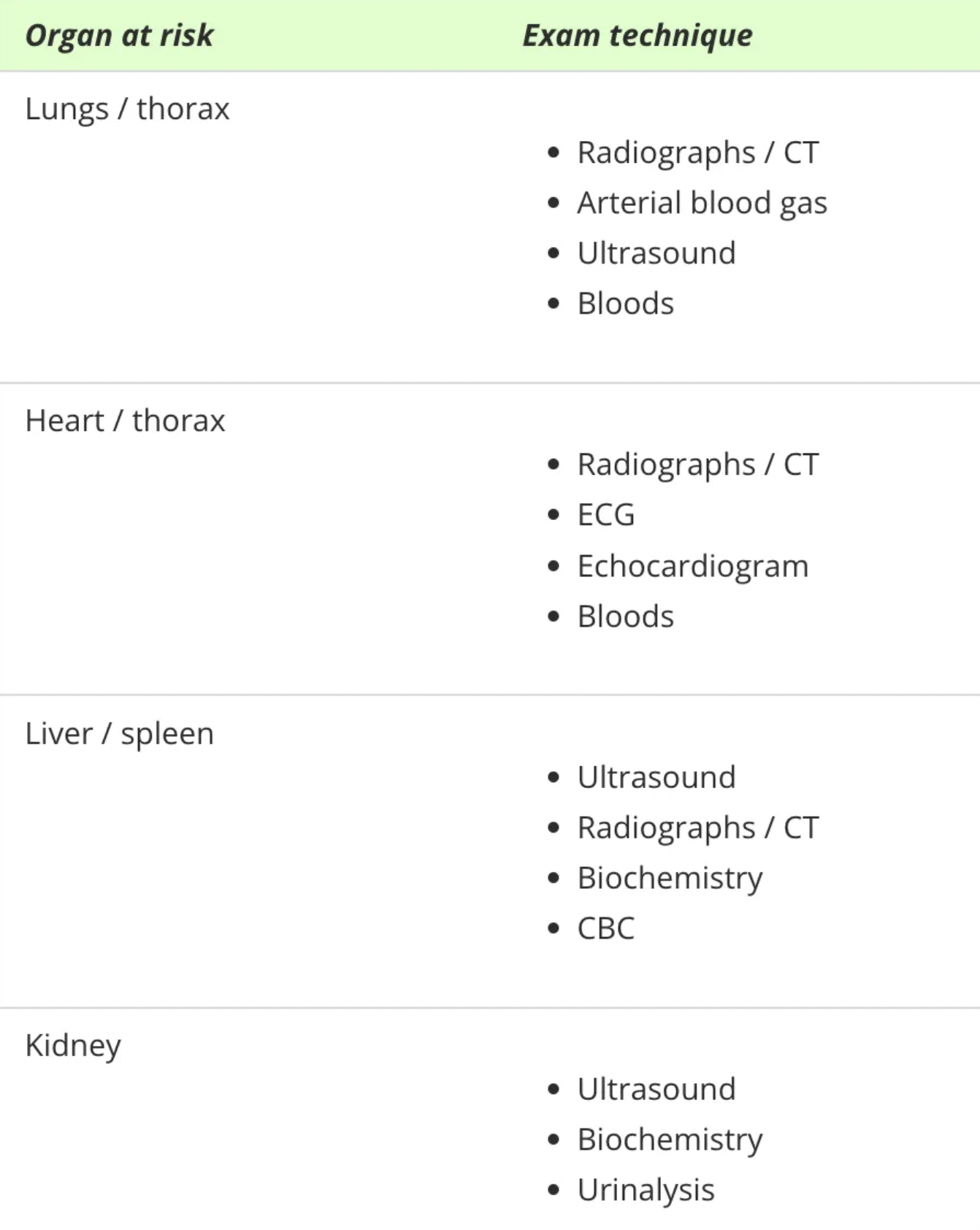
Aim and diagnostics for a pre-anaesthetic work-up
Aim: Determine patient’s ability to withstand stress of GA and surgery = Anaesthetic risk assessment (ASA grades)
Work-Up: Minimum (healthy patient)
History (complications and drugs used in previous GA events)
PE: TPR, MM, CRT, BWT, lung and heart auscultation
PCV/TPP →
Hydration status
Baseline if haemorrhage occurs
Crude estimate of protein-binding effects of drugs
Distribution of water if fluid given
± More extensive work-up for compromised patients = Young, old and sick
6 ASA Grades
Definition
Examples
Prognosis
ASA Grade | Definition | Examples | Prognosis |
I | Healthy patient with no underlying disease | Elective desexing, hip radiographs, cruciate repair | Excellent |
II | Mild systemic disturbance with no clinical signs and patient is well-compensated | Neonates, geriatric, simple fracture, brachycephalic, heart murmur ONLY (well-compensated | Good |
III | Moderate to severe systemic disturbance with mild clinical signs | Anaemia, fever, obesity, moderate renal/lung/heart disease, dehydration | Fair |
IV | Severe systemic disturbance and disease which is a constant threat to life | GDV, diaphragmatic hernia, uraemia, toxaemia, shock, severe anaemia/dehydration | Poor |
V | Moribund patient not expected to survive >24hr | Profound shock, severe trauma, MOD | Grave |
E | Emergency | Foreign body obstruction, spinal surgery | Variable |
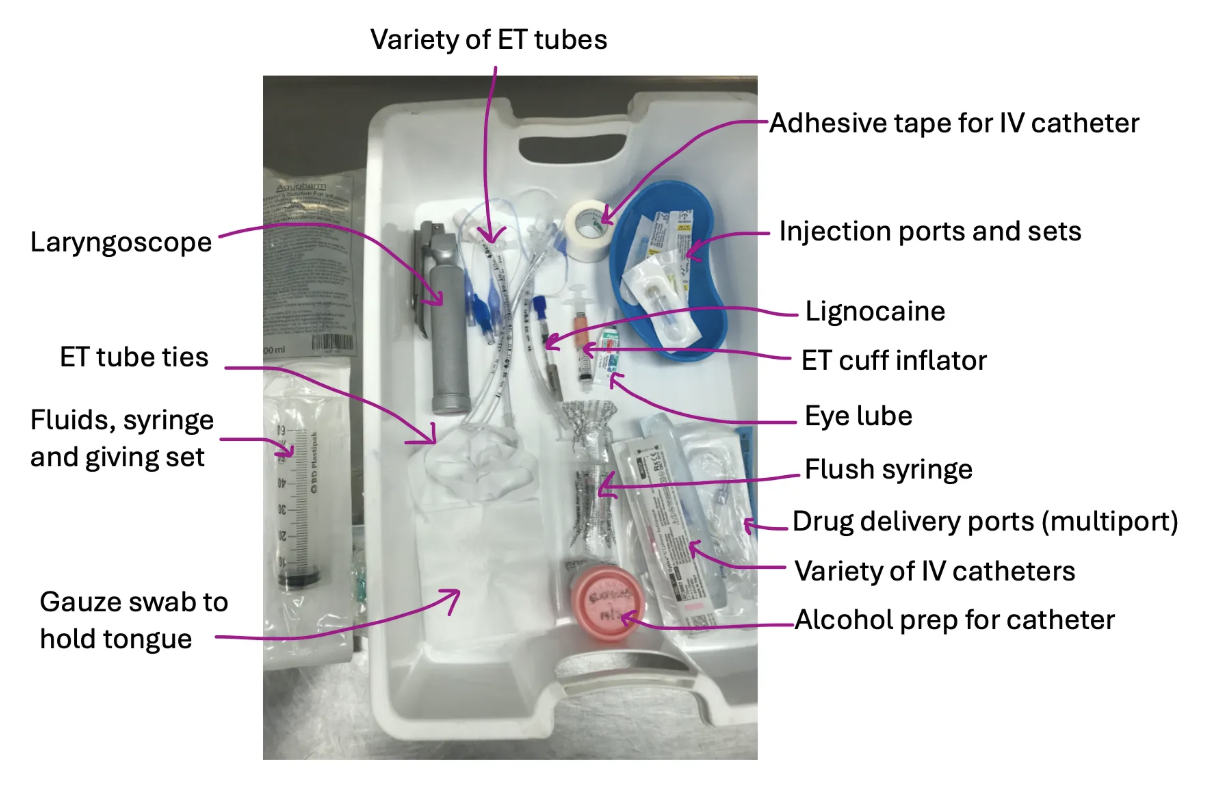
Pre-anaesthetic ABCs
Equipment
Function
Checks
A = Airway
Equipment:
Laryngoscope
ET tubes
Cuff inflator syringe
ET tube tie
Gauze swab to hold tongue
± Lignocaine (cat)
Function: Secure airway
Checks:
Attach blade of laryngoscope to check light is working
Inflate cuffs for leaks
Ensure ET tube tie is long enough
B = Breathing
Equipment:
Anaesthetic machine
Breathing circuit
Function: Assess if patient is breathing
Checks:
Machine check
Breathing system check
C = Circulation
Equipment:
IV catheters
Injection ports or T-port
Saline flush
Tape
Alcohol prep for catheter
Function: Secure IV access to induction drugs, emergency drugs and IVFT
Checks: Prime sets with saline
D = Depth and Drugs
Equipment: Drugs = Syringes, needle, drugs drawn up and labelled
Checks: Check drug calculations and correct volumes drawn up
E = Eye lube and equipment
Equipment:
Lacrilube
Pulse oximeter
ECG
Doppler/oscillometric cuff
Thermometer
Function: Protect eyes from drying out
F = Fluids
Equipment:
Fluid bag
Giving set
Function: Provide fluid for CVS support during GA-associated fluid loss
Checks: Primed line and correct fluid rates calculated
3 Factors influencing anaesthetic protocols (+ examples)
Patient factors
Signalment (species, breed, age)
Paediatric and geriatric dose rates are LOW
Juvenile (8 - 14 weeks) dose rates are HIGH
Temperament (wild patients may require 10 - 100x more sedation)
Size and conformation
Larger patients → Lower dose rates
BCS
Findings from history, PE and ancillary tests
Concurrent diseases (ASA grades)
Current medications (eg. amount of premed)
Type of procedure
Location on body
Estimated duration of procedure
Body position
Anticipated fluid loss
Anticipated pain (reduce relative dose of sedatives)
Availability of equipment and facilities
Abilities of vet/clinic (referral?)
Equipment and drug availability
Surgery or in-field?
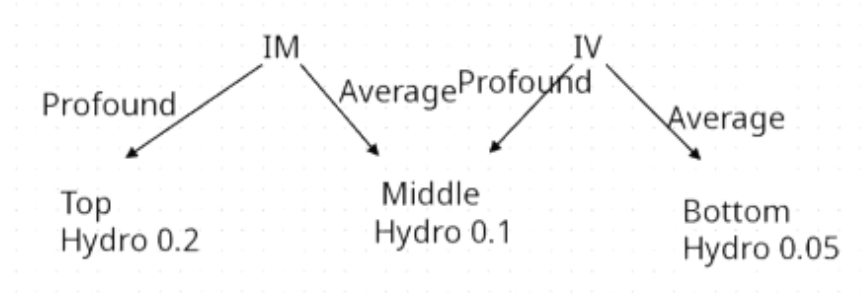
How to determine what dose rate to select?
Depends on route of administration and desired effect
Opioids
MoA
Metabolism
3 Effects
6 Example drugs
MoA: Modulation of pain via descending inhibitory pathways
Mu- or kappa-agonists which bind specific G-coupled opioid receptors within the brain and spinal cord → Mimic effect of endogenous opioids (eg. endorphines, enkephalins, dynorphines)
Metabolism: Liver (except remifentanil)
Effects:
Analgesia
Sedation (dogs) → Enhance sedative effects of other CNS depressants → Reduce dose rate of induction/maintenance agents
Less sedation in cats (euphoric ONLY)
Tolerance = Up-regulation of NMDA receptors (responsible for wind-up and central sensitisation) which bind glutamate (excitatory neurotransmitter)
Examples:
Morphine
Methadone
Buprenorphine
Butorphanol
Fentanyl
Remifentanil
Morphine
MoA
2 Unique advantages
2 Unique disadvantages
Routes of administration
Duration of action
MoA: Full mu-agonist
Advantages:
Cheap (gold standard against which all other opioids are judged)
Reliable, dose-dependent and effective analgesia for visceral AND MSK pain
Disadvantages:
IV → Drug-induced histamine release → Hypotension
Avoid in MCT surgery
Induces emesis and contraindicated for
Oesophageal FBO → Gastric rupture
Cannot open mouth (eg. lock jaw)
Difficulty protecting airways (eg. brachycephalics)
Head trauma → Increased ICP → Cerebellar herniation
Wobbler’s → Damage to cervical spine
Routes: IM, SC ± SLOW IV (care with IV histamine release)
ALSO epidural/intra-articular → 12 - 24hr duration of action (water-soluble and will stay in epidural space for long time)
Duration: 4 - 6hr IM
Methadone
MoA
4 Unique advantages
2 Unique disadvantages
Routes of administration
Duration of action
MoA: Full mu-agonist
Advantages:
Reliable, dose-dependent and effective analgesia for visceral AND MSK pain
NMDA receptor antagonist → Good for chronic pain and prevents tolerance to other opioids
Prevent neuronal plasticity associated with chronic glutamate receptor stimulation
No histamine release after IV administration → Excellent for rapid onset
Lipid-soluble = Rapid onset of action and anti-emetic (crosses BBB)
Disadvantages:
Less sedation than morphine (likely SAME sedation, but onset of action later than morphine and hence does NOT coincide with alpha-2-agonist onset of action)
$$$
Routes: IV, IM, SC
Duration: 4 - 6hr
Buprenorphine
MoA
2 Unique advantages
4 Unique disadvantages
Routes of administration
Onset
Duration of action
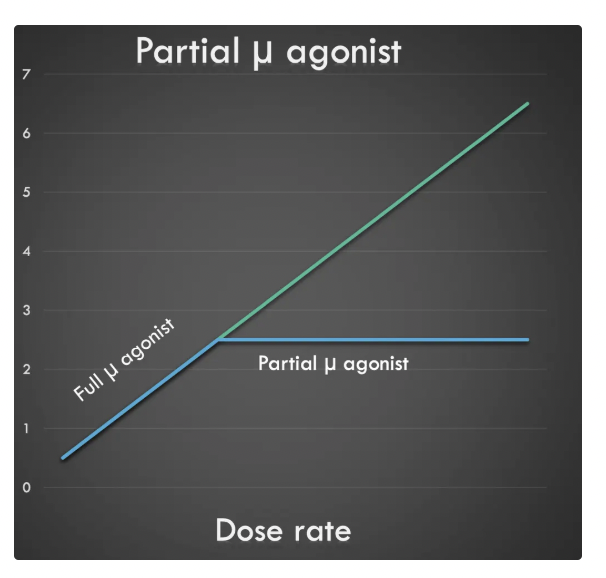
MoA: Partial mu-agonist
Advantages:
Long duration of action for analgesia
Fewer opioid-associated side effects (less respiratory depression, sedation and GI stasis)
Disadvantages:
Slow onset of action
Less effective analgesia as partial mu-agonist (ceiling effect → increased dose will no longer increase effect)
High affinity for mu-opioid receptors → Blocks effects of full mu-opioids
Limited reversal with naloxone (may require repeated administration at higher dose rates)
Routes: IV, IM, SC, buccal (cat)
Onset: 30 - 45 minutes
Duration: 6 - 8hr
Butorphanol
MoA
3 Unique advantages
4 Unique disadvantages
Routes of administration
Duration of action
MoA: Kappa-agonist and mu-antagonist
Advantages:
NOT a mu-agonist → No panting and ideal for thoracic radiography
Good sedation
Antitussive
Disadvantages:
Less effective analgesia as fewer kappa receptors (ceiling effect → increased dose will no longer increase effect)
Moderate analgesia for visceral pain but NOT orthopaedic pain
Kappa-agonists → Dysphoria = Increased movement and excitement in horses and cats
Marked bradycardia in SOME dogs
Short duration of action
Antagonism of mu-opioid receptors → Blocks effects of full mu-opioids
$$$
Routes: IV, IM, SC
Duration: 2 - 4hr
Fentanyl vs. remifentanil
Duration of action
Inducation
Fentanyl
Duration: 15 minutes
Indication: Polytrauma (bolus → CRI)
Remifentanil
Duration: 3 minutes (metabolised in blood NOT liver)
Indication: Liver disease (only opioid NOT metabolised by liver)
Avoid bolus → Bradycardia (use as CRI ONLY)
4 CNS effects of opioids
Hypothalamus → Opioids lower temperature equilibrium point in the thermoregulatory centre
Dogs pant due to activation of heat exchange mechanisms → Hypothermia
Avoid for thoracic radiographs (use butorphanol)
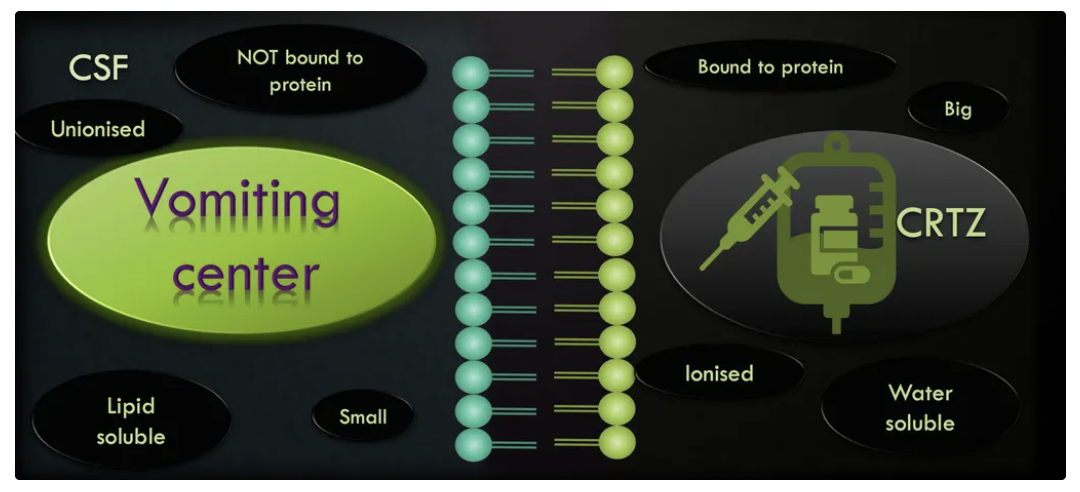
4th ventricle → Opioids cross the BBB into the emetic centre → Anti-emetic
CRTZ → Morphine cannot cross the BBB as it is water-soluble, so it binds the CRTZ to induce emesis
Morphine gradually cross the BBB due to the concentration gradient to bind the vomiting centre and become an anti-emetic (further doses of morphine have an anti-emetic effect)
Sedation = Morphine » Methadone
More profound sedation with low TP (methadone is highly protein-bound)
Respiratory effects of opioids
Dose-dependent respiratory depression
Decreased sensitivity of PaCO2 chemoreceptors → Decreased TV and RR
CVS effects of opioids
MINIMAL CVS depression with little change in MAP or cardiac contractility (safe for compromised patient) BUT induces dose-dependent bradycardia
Opioids stimulate the vagus nerve which provides parasympathetic innervation to the SA and AV node of the heart
→ Bradycardia
BUT increased ventricular filling time → Higher SV which restores CO
5 Visceral effects of opioid
Opioid receptors located on OUTSIDE of CNS (GIT, biliary tract and urinary tract) → SPHINCTER CONSTRICTORS (except oesophageal sphincter)
Dog = Miosis (cat = mydriasis → overdose)
Defaecation (anal sphincter)
Slow GI motility (pyloric sphincter → reduced gastric emptying and increased GI tone)
Urinary retention (bladder sphincter)
Increased biliary duct tension (sphincter of Oddi) → Pain with gallstones
7 Reasons to sedate a patient (+ other reasons to premed)
Sedate:
Reduce stress from excessive physical restraint and painful manipulations
Prevents injury to staff
Neuroleptic analgesia = Sedative + analgesia (opioid) → Marked synergism with enhanced sedation and analgesia than what can be achieved by either drug alone → Reduced dose rates used
More premed agents (higher TI) → Lower dose of induction/maintenance agents required (low TI)
Pre-Med:
Smooth induction and recovery periods → Rapid progression through stage I and II of anaesthesia
Pre-emptive analgesia PRIOR to nociception → Less painful recoveries with lower doses of post-op analgesic agents
Minimise adverse drug/physiological effects of other agents in the procedure
Provision of target analgesia (chronic vs. acute pain)
Tranquillisation vs. sedation vs. anxiolytic
Tranquillisation = Patient easier to handle and less stressed BUT not overtly sedated
Sedation = Calm patient but may be stressed internally if the sedative is not an axiolytic
Anxiolytic = Remove anxiety and appear like they are going to sleep
List 3 classes of sedatives (+ example drugs)
Benzodiazepine
Midazolam
Diazepam
Phenothiazine (acepromazine)
Alpha-2-adrenergic receptor agonists
Xylazine
Medetomidine
Dexmedetomidine
MoA of of benzodiazepine
Bind specific receptor sits on the subunit of GABA-A receptor = Gamma-amino-butyric acid
Activation of GABA-A receptor
Enhanced opening of Cl- channels by GABA inhibitory neurotransmitter
Increased influx of Cl- → Hyperpolarisation and resistance to neuronal excitation
5 CNS effects of benzodiazepines
Sedative (ANXIOLYTIC) = NOT useful for normal patients due to anxiolysis → Unmasks defensive and aggressive behaviour → Bizarre behaviour and paradoxical excitement in dogs/cats/horses
Good sedation in ruminants, camelids, pigs, birds, primates but NOT licensed
Excellent anticonvulsant (decreases ICP and anti-epileptic)
Seizures in patients with hepatic encephalopathy
Excellent muscle relaxant
No analgesia
Appetite stimulant
2 CVS effects of benzodiazepines
Minimal (very high TI → Safe for ASA grade 3 - 5)
Good for the very young, very old or very sick
Diazepam fast IV → Stimulates histamine release and vasodilation due to propylene glycol
Respiratory effects of benzodiazepines
Minimal (very high TI → Safe for ASA grade 3 - 5)
Good for the very young, very old or very sick
Visceral effects of benzodiazepines (liver and kidneys)
Diazepam → Hepatic necrosis in cats with pre-existing liver disease (metabolised in liver to active metabolites → Take time to dissipate from body)
Minimal renal effects
Benzodiazepine: Diazepam vs. midazolam
Solubility
Routes of administration
Diazepam
Solubility: Insoluble in water → Dissolved with propylene glycol solvent
Routes: IV, PO, transmucosal (eg. per rectum)
NOT IM/SC → Pain on injection and unreliable absorption due to propylene glycol
Not used as a premed
Slow IV to avoid haemolysis and histamine release
Midazolam
Solubility: Water-soluble → Shorter-acting and more potent than diazepam
Routes: IV, IM, SC, intra-nasal, PO
Routes of phenothiazine (acepromazine) administration
Transmucosal, IM, IV, SC, PO, transmucosal
Acepromazine high doses when PO (1 - 2mg/kg → extensive 1st pass metabolism)
7 CNS effects of phenothiazine (acepromazine) + MoA
“Anti-drug” = Histamine-, muscarinic-, serotonin-, dopamine-, alpha-1- antagonist (blocker)
Tranquillisation ONLY = Dopamine (D1 and 2) receptor blockade
Sedation when combined with opioids = Neuroleptanalgesia
NOT a good muscle relaxant (cannot give with ketamine)
Antiemetic = Dopamine (D1 and 2) receptor blockade
Antihistamine = H1 receptor blockade
Can use with MCT
Increase ICP ± increased risk of seizures (once considered to lower the seizure threshold) = Alpha-1-antagonist
No analgesia
Excessive acepromazine → Extra-pyramidal signs = Muscle tremours and spasticity
3 CVS effects of phenothiazine (acepromazine)
Antiarrhythmic = Alpha-1-adrenergic receptor ANTAGONIST in heart
Vasodilation = Alpha-1-adrenergic receptor ANTAGONIST peripherally → Reflex tachycardia
Causes hypothermia
Temporary reduction in HCT by 2 - 5% (spleen recruits RBCs) and decreased platelet aggregation
Avoid with anaemic patients and coagulopathies
Respiratory effects of phenothiazine (acepromazine)
NONE! Excellent for brachycephalic patients that cannot protect their airway (less muscle relaxation)
4 Visceral effects of phenothiazine (acepromazine) (liver + kidneys)
Metabolised in liver but NO REVERSAL available → Effects prolonged in patients with liver disease
Mild effects on kidneys through vasodilation → hypotension
Avoid in breeding stallions → Risk of priapism
Splenic enlargement (avoid with laparoscopy)
6 Example alpha-2-agonists (ranked by potency)
Least Potent:
Xylazine (LA and SA)
Detomidine (LA)
Medetomidine
Medetomidine = Racemic mixture of levomedetomidine and dexmedetomidine (optical enantiomers)
Dexmedetomidine = Active ingredient ONLY ($$$)
Most Potent:
ALSO:
Romifidine
Clonidine
Used in humans as a nasal decongestant (produces vasoconstriction of the nasal mucosal blood vessels which reduces mucus production)
Routes of alpha-2-agonists
SC, IM, IV
Epidural (vasoconstriction → prolong action of local anaesthetics)
Transmucosal gel (domosedan and sileo)
5 CNS effects of alpha-2-agonists
Sedation (can be profound) → Still can be roused
Excellent anticonvulsant (decreases ICP and anti-epileptic)
Same side effect as Cushing’s reflex = Hypertension and reflex bradycardia → Avoid for patients with high ICP
Excellent muscle relaxation
Excellent visceral analgesia (wanes prior to sedation → care with rousability due to pain)
Smooth muscle spasm in blood vessels, GIT and uterus
CVS effects of alpha-2-agonists
Prominent BRADYCARDIA at label doses (use lower dose rates than what is suggested on the bottle) ± 2nd degree AV blocks
Biphasic BP
Post-Synaptic Effect = Drug stimulates PERIPHERAL alpha-2-receptors in blood vessel walls causing intense vasoconstriction (pale MM) → Reflex bradycardia (increased BP and decreased HR)
Treatment: Reversal if severe bradycardia
Pre-Synaptic Effect = Drug stimulates CENTRAL alpha-2-receptors (crosses the BBB) → Inhibit negative feedback and release of NA from presynaptic neurons → Increased PNS with bradycardia ± vasodilation (decreased BP, CO and HR)
Xylazine causes hypotension (vs. other A2A → normotensive)
Treatment: Atropine or glycopyrrolate
2 Respiratory effects of alpha-2-agonists
Minimal effects
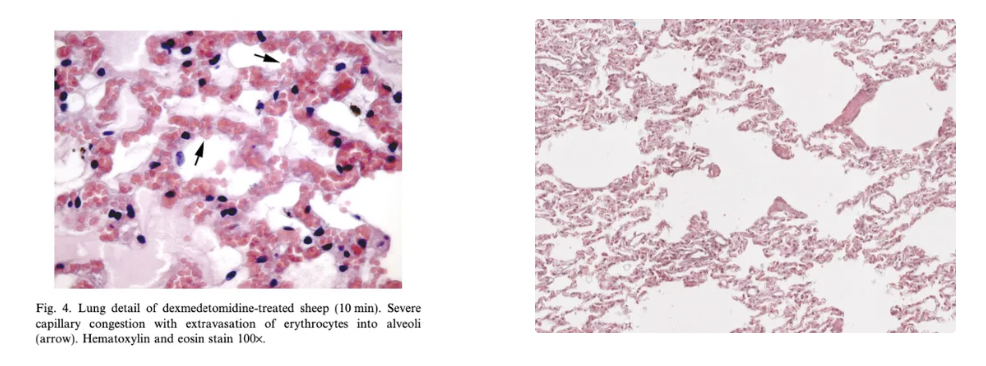
Xylazine → Respiratory distress, pulmonary oedema and hypoxaemia in ruminants (esp. goats and sheep)
MoA: Ruminants have unique pulmonary intravascular macrophages with alpha-receptors on their surface to bind xylazine → Stimulates macrophages to release cytokines which causes thickening on alveolar walls → Decreased gas exchange
Still used in ruminants due to effective sedation AND analgesia (fewer opioid receptors) and only A2A licensed (otherwise 91d WHP)
6 Visceral effects of alpha-2-agonists
Emesis in cats
Decreased GI motility
Re-narcotisation in some species = Cannot process drug, but can process reversal
Decreases GFR and increases urine production (inhibit ADH)
Dexmedetomidine is nephroprotective
Xylazine → Penile prolapse in bulls and abortion in pregnant mares/cows
Decrease pancreatic release of insulin → Hyperglycaemia
Contraindications of:
Benzodiazepines
Phenothiazines (acepromazine)
Alpha-2-agonists
Benzodiazepine:
Normal patients (young, old and healthy)
Cats with liver disease → Hepatic necrosis
Phenothiazines (Acepromazine):
Hypovolaemia or dehydration → Vasodilation (cannot divert blood to vital areas)
Liver disease (no reversal available)
Young, old and sick
mdr-1 mutants
Alpha-2-Agonists:
Cardiac disease
Nausea and emesis contraindicated in cats
Onset (IM) and duration of:
Benzodiazepines
Phenothiazines (acepromazine)
Alpha-2-agonists
Opioids
Benzodiazepine:
Onset = 10 minutes
Duration = 1hr (2 - 6hr)
Phenothiazines (acepromazine):
Onset = 30 - 45 minutes
Duration = 4 - 6hr (calm on recovery)
Alpha-2-Agonists:
Onset = 10 minutes
Duration = 1hr (higher dose → higher duration)
Xylazine = 30 minutes
Dexmedetomidine SLIGHTLY faster elimination (levomedetomidine increases the half-life of dexmedetomidine by inhibiting its metabolism)
Opioids:
Onset = 10 minutes (20 minutes for buprenorphine)
Reversals for:
Benzodiazepines
Phenothiazines (acepromazine)
Alpha-2-agonists
Opioids
Benzodiazepine → Flumazenil IV
Phenothiazines → NONE!
Alpha-2-agonists → Atipamezole IM
Same volume as sedative for dogs and ½ for cats
Opioids → Naloxone (can mini reverse patient is recovery is slow post-op; avoid full reversal of analgesia)
Onset: Fast
Duration: 30 minutes
List 4 types of premeds used (functions)
Sedatives
Benzodiazepine (midazolam ONLY)
Acepromazine
Alpha-2-agonists
Analgesia
Methadone/morphine
Butorphanol
Buprenorphine
Drugs that offset physiological/pharmacological consequences of GA/surgery
Omeprazole
Atropine
Maropitant
Antihistamines
Dissociatives
Ketamine
Tiletamine
Describe the use and MoA of premed drugs that offset physiological/pharmacological consequences of GA/surgery:
Anticholinergics = Atropine and glycopyrrolate
Antihistamines = Mepyramine
Antiemetic = Maropitant
Gastric pH modifier = Omeprazole
Anticholinergics = Atropine and glycopyrrolate
MoA: Competitive antagonist of the muscarinic acetylcholine receptors (M1 - 5) → Parasympatholytic (blocks vagal tone)
Heart = SA and AV node → Increase HR
GI = Slow GIT of LA (eg. colic horses)
Eye = Mydriasis
Lung = Bronchodilation and reduced respiratory/salivary secretions (eg. cats in laryngospasm)
Avoid in stallions → Paraphimosis
Avoid atropine in rabbits (atropinase) → Glycopyrrolate instead (fewer side effects and longer duration of action)
Indications:
Reduce ketamine-induced ptyalism (excessive salivation) and risk of laryngospasm in cats (UNCOMMON)
Offset pharmacological effects of opioid → Bradycardia
Reduce vasovagal/oculocardial reflex during ophthalmic surgery → Vagus nerve induces bradycardia
Antihistamines = Mepyramine → History of hypersensitivity reactions or MCT
Antiemetic = Maropitant → GI disease, unfasted patient, aspiration risk (eg. brachycephalics), hernia repair, prolonged GA
Gastric pH modifier = Omeprazole → Brachycephalics
Order of loss during GA (10):
Pain and memory
Consciousness
Motor coordination
Response to external stimuli
Muscle tone
Protective reflexes (eg. gag)
Autonomic functions (SNS and PNS control)
Normal control of cardiovascular and respiratory systems
Control of ventilation ending in respiratory arrest
Control of cardiovascular function resulting in cardiac arrest
It IS possible to anaesthetised but conscious (stage I = amnesia and analgesia BUT conscious)
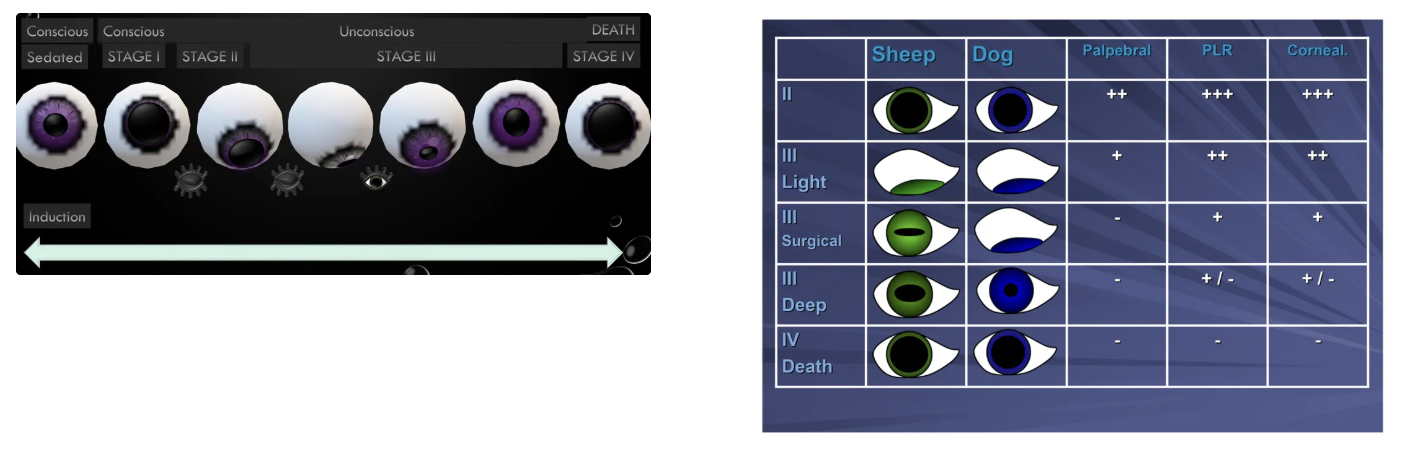
List the 4 stages and 4 planes of anaesthetic depth
Stage I = Voluntary excitation
Stage II = Involuntary excitation
Stage III = Surgical anaesthesia
Plane 1 = Light
Plane 2 = Medium
Plane 3 = Deep
Plane 4 = Very deep
Stage IV = Bulbar paralysis
Transition between stages is NOT obvious and there are species differences, anaesthetic agent differences and individual differences
4 Vital functions used to assess anaesthetic depth (+ examples and what stages they are absent)
Autonomic reflexes
Salivation
Lacrimation
Protective reflexes
Gag reflex
Cough reflex
Sneeze reflex
Corneal reflex - Sluggish stage III, plane 3 (absent by plane 4)
Indicates deeper plane than palpebral reflex
Do NOT routinely use as monitoring tool → Corneal damage
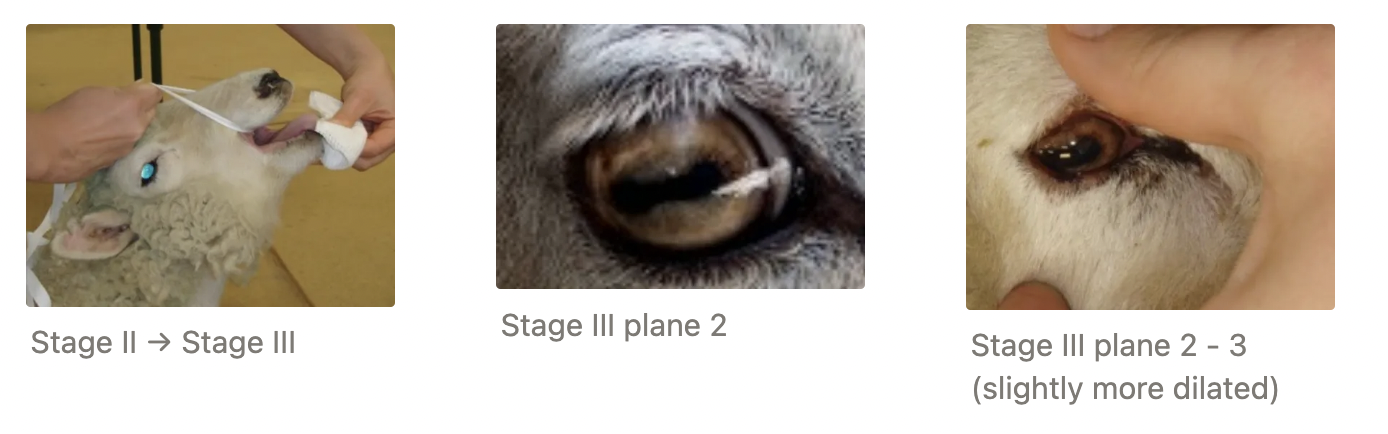
Palpebral reflex - Absent in stage III, plane 2
Lateral palpebral disappears FIRST
Good way to assess induction is progressing → intubation imminent when lateral palpebral is lost
MAY remain with ketamine → Incorrect assessment of anaesthetic depth
PLR - Absent stage III plane 3
Assess when pupils are dilated and central → Differentiate between stage II (present) and stage II, plane 3/4 (absent)
Ocular muscle tone (position and pupil size)
DOG
Stage I/II = C ± dilated (depends on lighting and premed)

Stage III, plane 1 = CV (rolling from C → VM) + dilated → constricting
Identical to stage III, plane 3 → PLR to assess

Stage III, plane 2 = VM + constricted (cannot see pupil)

Stage III, plane 3 = Stage III, plane 1 = CV (rolling VM → C) + constricted → dilating

Stage III, plane 4 and stage IV = Central and dilated

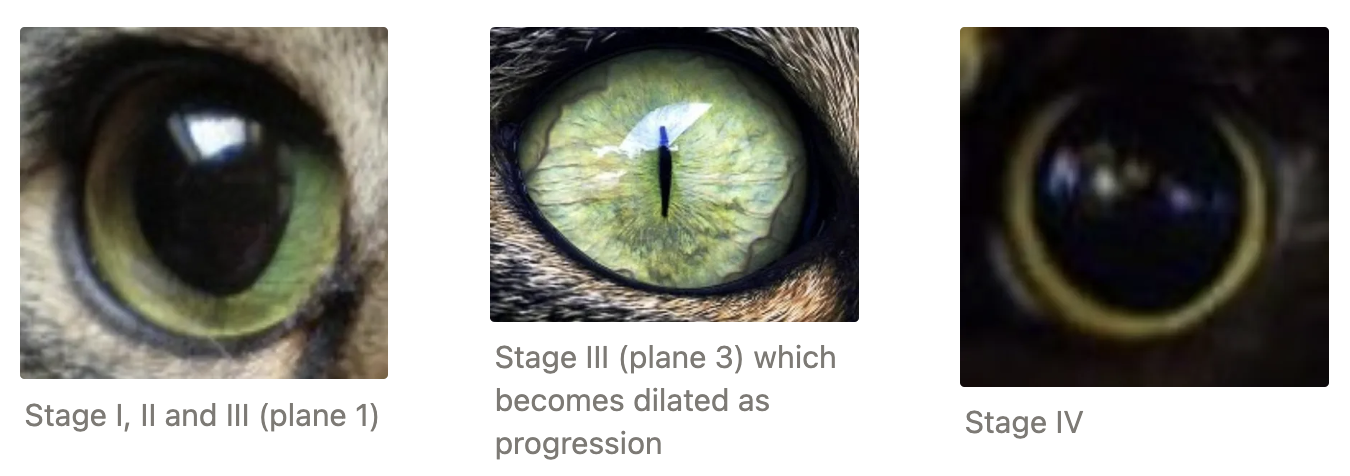
CAT:
Induction: Central and dilated due to
Stress of environment (catecholamine release)
Premeds do NOT produce profound sedation as in dogs
Mu-opioids produce mydriasis in cats
Atropine once used in cats to reduce ptyalism
Ideal: CV
Too deep: VM or central and constricted
Sheep:
Induction: Pupils dilate and move ventrally (cannot intubate until eyes are ventral)
Ideal: No palpebral, eye central and constricted (rolled V → C)
Horse:
Stage III: Central and dilated for ALL planes
Light surgical = Strong palpebral and slow nystagmus
Moderate surgical = Central, dilated with sluggish PLR
Deep surgical = Absent PLR
Skeletal muscle tone (jaw and chest)
Ruminants + horses + specific species of dogs and cats have strong intrinsic jaw tone
Menace response NOT used to assess anaesthetic depth (response to external stimulus disappears very quickly after induction = step 4)
NOT pedal withdrawal reflex (disappears immediately after induction)
Pupil size with dogs vs. cats on opioids
Dogs = Constriction (miosis)
Cats = Dilation (mydriasis)
Stage I (voluntary excitement)
Start
End
Characteristics
Cardiopulmonary
Eye position
Pupil size
Palpebral present?
Start: Induction
End: Loss of consciousness
Characteristics: Analgesia + consciousness, disorientation
± Salivation, struggling, urination, defaecation
Cardiopulmonary: Increased HR and RR (OR breath-holding)
Eye position: Central
Pupil size: Normal (cats = dilated)
Palpebral present: YES
Rapid with injectables = Stage I may not be noticed (slow with inhalants)
Stage II (involuntary excitement)
Start
End
Characteristics
Cardiopulmonary
Eye position
Pupil size
Palpebral present?
Start: Loss of consciousness
End: Loss of struggling
Characteristics: Loss of normal voluntary control and often overly responsive to pain
Exaggerated reflexes
Struggling
Laryngeal protective reflexes present
Chewing, vomiting, swallowing
Nystagmus in horses
Cardiopulmonary: Irregular breathing (breath-holding)
Eye position: Central
Pupil size: Dilating (sympathetic nervous system stimulated)
Palpebral present: YES
Responsible for dysphoria on recovery (disturbing and dangerous period as cannot be calmed by voices)
Stage III (surgical anaesthesia)
Start
End
Ideal plane
Start: Struggling stops
End: Plane 4 = Respiratory distress
Ideal: Stage III, plane 2
What is the BEST way to determine an appropriate surgical plane?
Response to surgical stimulation should be present (cardiopulmonary system is still reactive = increased HR, MAP and ventilation with surgical stimulation)
Disappears at plane 3
Stage III, PLANE 1 (light plane)
Procedures
Cardiopulmonary
Eye position
Pupil size
Palpebral
Corneal
PLR
Lacrimation
Pharyngeal and laryngeal reflexes
Muscle tone
MM and CRT
Procedures: Minor procedures or imaging
Cardiopulmonary: Decreased TV and RR, normal/rapid HR and strong pulse
Eye position: Rolling (C → V)
Pupil size: Dilating → Constricting
Palpebral: YES
Corneal: YES
PLR: YES
Lacrimation: YES
Pharyngeal and laryngeal reflexes: YES (difficult to intubate)
Muscle tone: Strong (mouth difficult to open)
MM and CRT: Pink and rapid
Stage III, PLANE 2 (medium plane)
Procedures
Cardiopulmonary
Eye position
Pupil size
Palpebral
Corneal
PLR
Lacrimation
Pharyngeal and laryngeal reflexes
Muscle tone
MM and CRT
Procedures: Surgical procedures
Cardiopulmonary: Decreased TV and RR, normal/lower HR and strong pulse
Eye position: VM (CV cat and C sheep)
Pupil size: Constricting
Palpebral: NO
Corneal: YES
PLR: YES
Lacrimation: YES
Pharyngeal and laryngeal reflexes: NO (except cat pharyngeal reflexes)
Muscle tone: Reduced (mouth easier to open)
MM and CRT: Pink and normal CRT
Stage III, PLANE 3 (deep plane)
Procedures
Cardiopulmonary
Eye position
Pupil size
Palpebral
Corneal
PLR
Lacrimation
Pharyngeal and laryngeal reflexes
Muscle tone
Procedures: Deeper than necessary
Cardiopulmonary: Decreased TV, RR, MAP, HR
Vitals do NOT increase in response to surgical stimulation
Eye position: Rolling (V → C)
Pupil size: Constricting → Dilating
Palpebral: NO
Corneal: Sluggish
PLR: Sluggish
Lacrimation: No (dry eyes)
Pharyngeal and laryngeal reflexes: NO
Muscle tone: Marked relaxation
Stage III, PLANE 3 (deep plane)
Procedures
Start
End
Cardiopulmonary
Eye position
Pupil size
Eye reflexes
Lacrimation
MM and CRT
Procedures: NEVER
Start: Paralysis of intercostal and abdominal muscles which control ventilation
End: Respiratory arrest
Cardiopulmonary: Markedly reduced MAP, weak pulse and heart sounds
Eye position: Central
Pupil size: Dilated
Eye reflexes: NONE
Lacrimation: NONE (dull and dry)
MM and CRT: Pale, blue/grey with slow CRT
Parasympathetic nervous system tone > sympathetic
Patient at risk of irreversible tissue damage due to poor perfusion and hypoxia
4 Treatments when anaesthetic plane is too deep
Immediately turn off anaesthetic agent
Patient ventilated with 100% O2
CVS supported with IV fluids
± Emergency drugs
Stage IV (bulbar paralysis)
Start
End
Cardiopulmonary
Difference between stage IV and stage III, plane 4 is that the heart no longer beats in stage IV
Start: Respiratory arrest
End: Cardiac arrest
Cardiopulmonary: No pulse, heart cannot be auscultated, jerky/irregular respiration (agonal gasping and tracheal tug)
Modern inhalants have reasonable safety margin between respiratory arrest and cardiac arrest (care with critical patients or those not closely monitored)
Steps of induction ABCs
Airway = ET intubation
Breathing = Inflate cuff and check patient is breathing
Circulation = Pulse, heart beat auscultation
Depth = Assess eyes and jaw tone to determine depth
Equipment and eye lube = Pulse oximeter, NIBP, capnograph, ECG
Fluid
List 4 injectable induction agents (+ routes of administration)
Ketamine IV
IM and SC for cats
Alfaxalone IV
IM and SC for cats (eg. aggressive cats where ketamine is contraindicated) → Slightly faster uptake than metabolism
Duration: 5 - 10 minutes (must watch patient sedate)
IV ONLY for dogs → Uptake is slower than metabolism
Propofol IV ONLY → Any drug absorbed via IM/SC is immediately metabolised
Thiopentone IV ONLY
Onset and duration of action of:
Propofol
Thiopentone
Ketamine
Propofol:
Onset = 15 - 20s
Duration = 5 - 7 minutes
Thiopentone:
Onset = 15 - 20s
Duration = 10 - 20 minutes
Ketamine:
Onset = 20 - 30s (5 - 10 minutes IM)
Duration = 10 - 15 minutes
9 Properties of the ideal anaesthetic agent
Rapid onset (seconds) → Rapid transition through excitatory stages
Predictable duration
Non-irritant if perivascular
Non-painful on injection
Non-accumulative (metabolised rapidly)
Non-allergenic
Produces physiological stability (no change in cardiopulmonary function)
Cheap
Bacteriostatic
How to administer induction agents in small animals (vs. horses)
Small Animals: Dosed to Effect
Average dose drawn up
Give ½ dose SLOWLY (except thiopentone)
Begin with 1mg/kg for propofol
Wait for effect of stage III, plane 1/2
Give ½ of remainder
Wait for effect
Administer remainder if required and appropriate stage of GA has not been reached
Draw up and administer more if required
Horse: Give ALL as excitement phase in horses is too dangerous
Alfaxalone solubility (+ 4 formulations)
Solubility: Insoluble in water
Contains cyclodextrin excipients with NO cremaphor (or alphadalone)
Formulations:
Preservatives 10mg/mL
Without preservatives (fridge) 10mg/mL
Alfaxan forte 40mg/mL (licensed for IM in cats to reduce volume required)
Historic Drug: Saffan (Althesin) = Steroidal GA agent (alfaxalone + alphadalone) in cremaphor EL
+ve: Once #1 GA agent in cats as alphadalone → Excellent analgesia
-ve: Castor oil diluent (cremaphor) → Marked histamine release in dogs
3 CNS effects of alfaxalone
Hyperaesthetic recoveries → Dysphoric (leave alone during recovery vs. propofol patients SHOULD be woken up)
Analgesia through CNS depression ONLY
Decreases ICP and anti-epileptic
2 CVS effects of alfaxalone
Minimal CVS depression (HR and BP maintained well)
Vasodilation with reflex tachycardia during induction with compromised patients (ASA IV/V)
2 Respiratory effects of alfaxalone
Minimal respiratory depression (minimal effect on the hypoxic pulmonary vasoconstrictive reflex)
Apnoea if given fast IV
Visceral effects of alfaxalone (liver + kidney)
Rapid metabolism by liver ± lungs → Multiple top-ups (TIVA) without prolonged recovery
Minimal effects on kidneys
Contraindications of alfaxalone
Large patients → $$$
Propofol solubility and 2 formulations
Solubility: Insoluble in water
Formulations: 10mg/mL
Intralipid suspension/excipient containing egg phosphatide, glycerol and soyabean oil (excellent bacterial growth medium)
Important to discard unused propofol and keep multiuse vials free of contamination to avoid inoculating patients with bacteria
Bacterial growth after 6hr of opening
Minimise pain on IV injection
Aquafol = Clear and water-soluble containing benzo-alcohol
-ve: Vehicle effect = Sudden unexplained deaths after administration due to excipient → Histamine release in dogs due to allergic reaction
Propylphenol and neutral pH → Not irritating if given perivascularly by accident
4 CNS effects of propofol
Myoclonus (muscle twitching) common → Mistaken for seizures or light plane of anaesthesia
Excellent anticonvulsant (decreases ICP and anti-epileptic)
Excellent muscle relaxant
Analgesia through CNS depression ONLY
2 CVS effects of propofol
Excellent antiarrhythmic (sympatholytic)
Dose-dependent CVS depression (decreased HR, SV, BP)
3 Respiratory effects of propofol
Minimal pulmonary depression (little effect on HPVR)
Apnoea at induction common
Cats accumulate propofol in lungs after consecutive doses
5 Visceral effects of propofol (liver + kidney)
Extra-hepatic metabolism = Metabolised by multiple sites as clearance of propofol exceeds hepatic blood flow → Ideal for liver disease
Liver 80% and lungs 20%
Non-cumulative when used as TIVA (except cats when TIVA > 30 minutes due to deficiency in glucaronidase enzyme)
Phenolic compound → Heinz body anaemia in cats when dosed with propofol on consecutive days due to RBC oxidative damage (~1 week)
White form stimulates pancreatitis
Minimal effects on kidneys (cardiac-induced damage)
Other advantage of propofol
Cheap
Contraindications of propofol
Pancreatitis
Sepsis
Chemical properties of thiopentone
Chemical: Barbiturate
Powder to reconstitute with sterile water → Lasts several days in fridge
pH = 11 → Irritating if given perivascularly (thrombophlebitis)
Treatment: Dilute 0.9% NaCl and lignocaine = Acid to neutralise alkaline solution
MUST be given IV due to high pH
4 CNS effects of thiopentone
Excellent anticonvulsant (barbiturate)
Excellent muscle relaxant
Rough recovery → Interpreted as seizures
Analgesia through CNS depression ONLY
3 CVS effects of thiopentone
Minimal CVS depression (HR and BP well-maintained)
Vasodilation and reflex tachycardia common on induction in sick patients
Arrhythmogenic in 25% of patients (not observed as ECG not present during induction)
Respiratory effects of thiopentone
Apnoea common on induction
5 Visceral effects of thiopentone (liver + kidney)
Ultra-short duration of action = Drug hits brain and is rapidly redistributed to lean tissue → fat
Highly protein-bound → Greater effect in patients with hypoalbuminaemia
Lower pH (acidosis) → More unionised drug free to cross the BBB → Greater effect
Very slow hepatic metabolism → Avoid in liver disease and TIVA due to cumulative effect
Minimal effect on kidneys