DEENT Exam 2
1/619
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
620 Terms
The epidermis is the first ___ layers of the skin
four
What layer of the skin are you typically treating when you treat dermatitis?
epidermis
What is typically used when treating dermatitis?
topical creams and ointments
Topical medications are often the most ____ in standard tube sizes
cost-effective
Perscribed amounts are ___ to available tube sizes
rounded up
How much is a fingertip unit?
0.5g
How many fingertip units are used on the scalp?
3 (1.5g)
How many fingertip units are used on the face and neck?
2.5 (1.25g)
How many fingertip units are used on hand (front and back, including fingers)?
1 (0.5g)
How many fingertip units should be used for one arm, including the entire hand?
4 (2g)
How many fingertip units should be used for the elbows?
1 (0.5g)
How many fingertip units should be used for both soles of the feet?
1.5 (0.75g)
How many fingertip units should be used for one foot, including toes?
2 (1g)
How many fingertip units should be used for one leg, including the foot?
8 (4g)
How many fingertip units should be used for the buttocks?
4 (2g)
How many fingertip units are used for the knees?
1 (0.5g)
How many fingertip units are used for both sides of the trunk?
14 (7g)
How many fingertip units are used for one side of the trunk?
7 (3.5g)
What is the hallmark symptom of atopic dermatitis?
Pruritis
Atopic dermatitis is usually due to what?
allergen influx, especially due to broken or damaged skin barriers
Atopic dermatitis is also known as what?
eczema
Atopic dermatitis is a very ______ inflammatory skin disorder with typical morphology and age-specific patterns
common chronic or relapsing
When does atopic dermatitis often develop?
childhood
There is no __ for AD and it is not ___
there is no cure for AD and it is not contagious
Emollient therapy improves the skin barrier to block what?
the inflammatory cascade
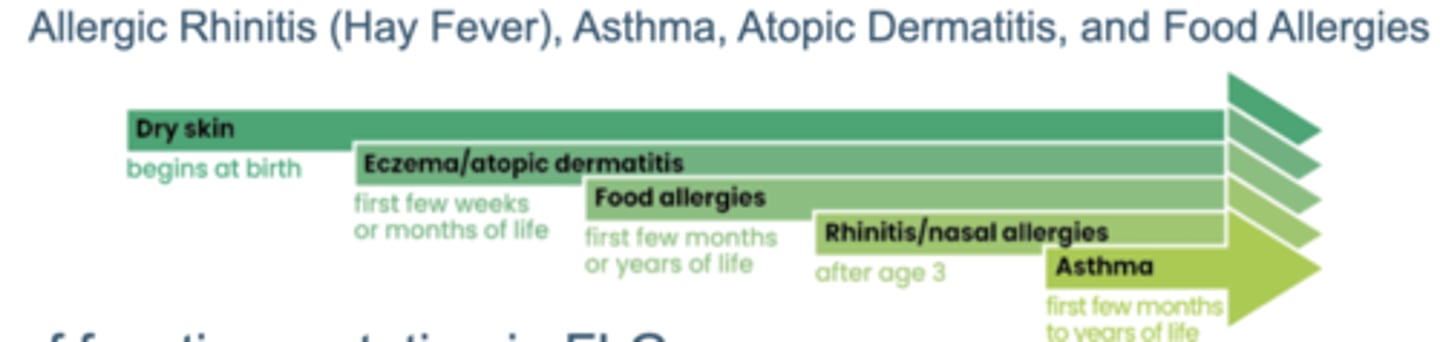
What is the atopic triad?
Allergic Rhinitis (Hay Fever), Asthma, and Atopic Dermatitis
What is the atopic march?
Refers to the natural history or typical progression of allergic diseases that often begin early in life
What puts someone at risk for AD?
personal or family history of atopic disorders
loss of function mutation of the FLG gene
living in an urban environment
smaller family size
higher level of parental education
What irritants may trigger AD?
Airborne - tobacco smoke, air pollution
Cosmetics, fragrances, astringents
Irritating soaps/scrubs/detergents
Dyes /preservatives
What allergens may trigger AD?
Food: Eggs, milk, peanuts, soy, wheat, nuts, tomato
Clothing: Wool, polyester
Aeroallergens: House dust mites, Pollens, Pet dander, Mold
What environmental factors might trigger AD?
Extreme temperatures and Low Humidity
What personal factors trigger AD?
Stress
Excessive skin washing and sanitizing
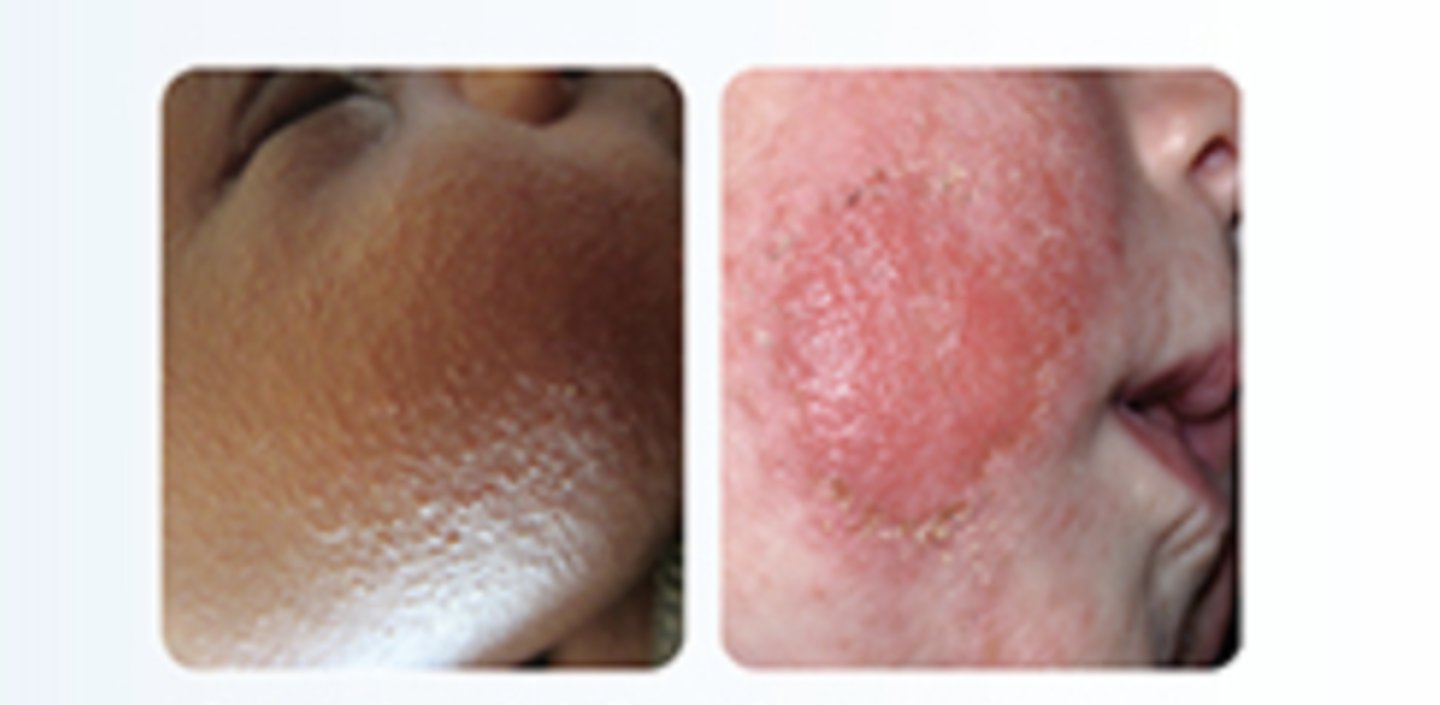
ASWQHow does AD present in infants (0-2)?
Quality/Quantity: Erythematous, popular rash that tends to ooze
Region: Face, scalp, trunk, arms, and legs
Timing: Most common onset is between 3-6 months of age
The majority have onset by age one
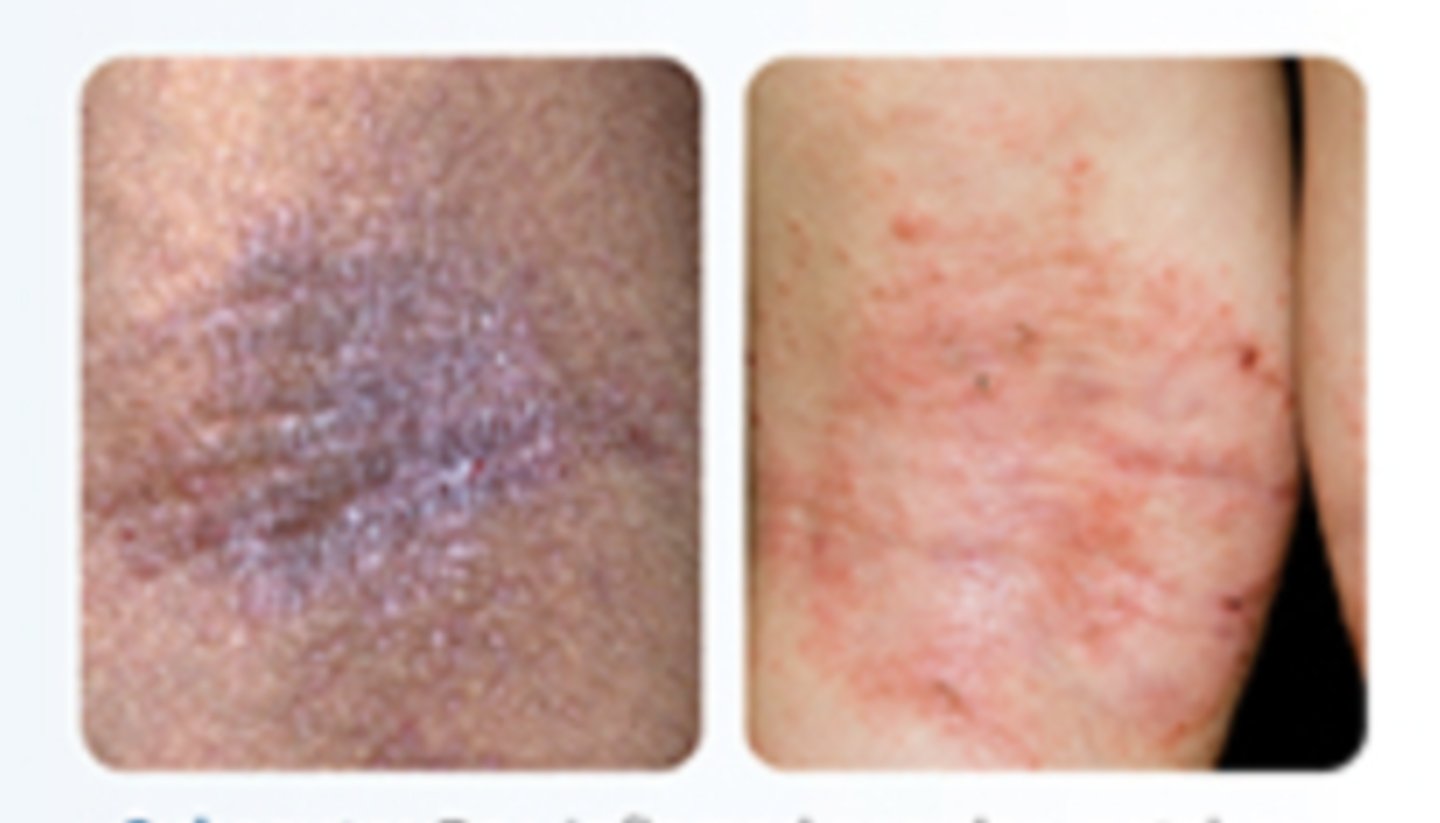
How does AD present in childhood (2-puberty years)?
Quality/Quantity: Dry, flaky, rough, cracked skin, crusting, lichenification
Region: Face, creases of the neck, elbows, wrists, knees, ankles
Timing: Up to 90% by age 5 years old
How does AD present in adulthood?
Quality/Quantity: More diffuse with underlying erythema, dry, scaly skin, lichenification
Region: Less common on the face and more common on the hands, neck, inner elbows, back of knees, and ankles Timing: May have resolution of disease by adulthood (70-90%)
What is lichenification?
Skin is dark and thick with plaque, dry, flaky skin that is clumped together. Typically seen in adult patients, but can be seen in children.
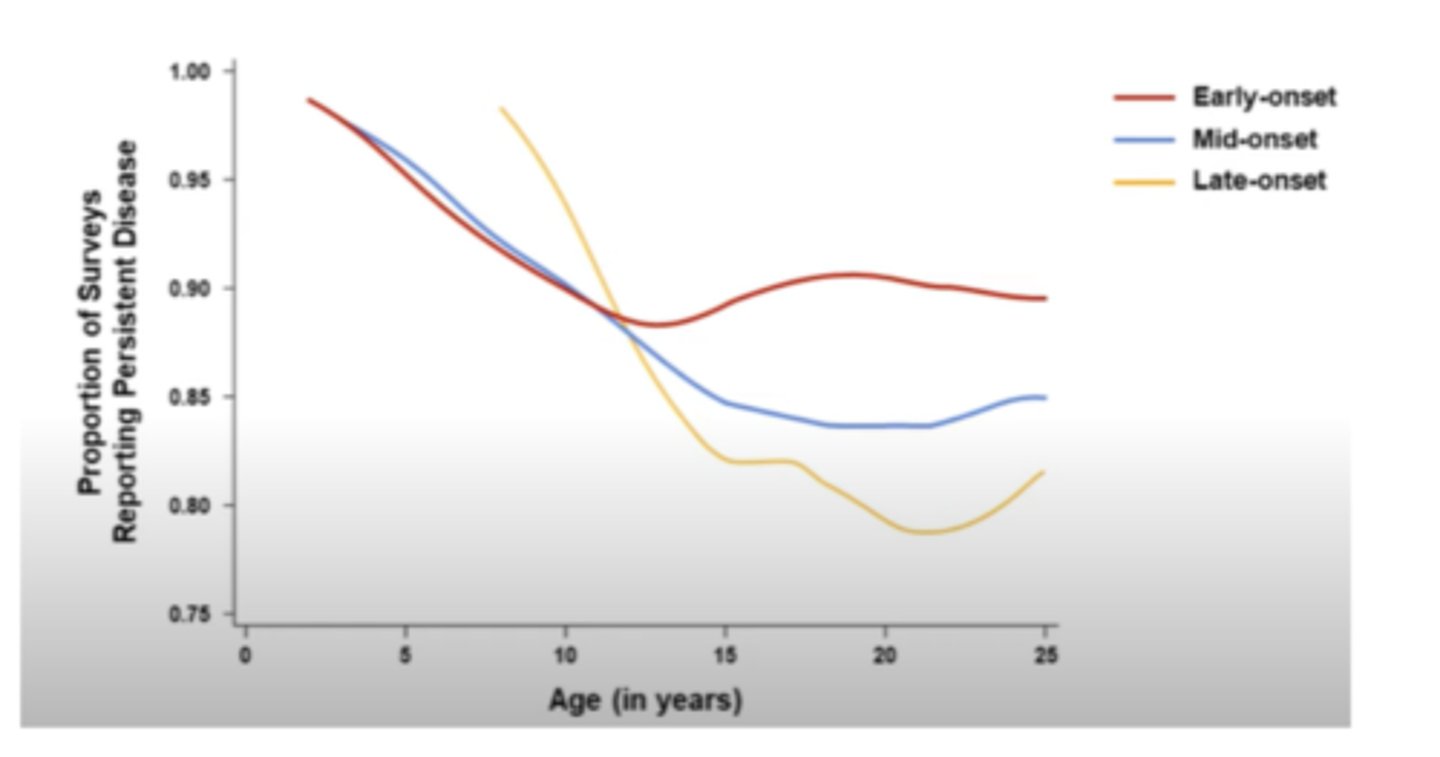
How does age of onset predict the persistence of AD?
Patients with early onset of the disease will most likely have it throughout life, and patients with late onset have decreased persistence
What is the SCORAD scale?
Clinical tool used to assess the extent and severity of AD (SCORing Atopic Dermatitis)
On the SCORAD scale what is classified as mild?
less than 25
On the SCORAD scale what is classified as moderate?
25-50
On the SCORAD scale what is classified as severe?
greater than 50
What characteristics classify a mild case of AD?
Areas of dry skin, infrequent itching (with or without small areas of redness); little impact on very day activities, sleep, and psychosocial wellbeing
What characteristics classify a moderate case of AD?
Mild characteristics with frequent itching, moderate impact on everyday activities, and sleep
What characterisitics classify a severe case of AD?
Wide-spread areas of dry skin, incessant itching, redness, thickening, bleeding, oozing, severe limitation to activities, and nightly loss of sleep
How are acute lesions characterized?
acutely inflamed papules, vesicles, exudate, and crisis
How are subacute lesions characterized?
dry and inflamed
How are chronic lesions characterized?
lichenified plaques

What are some complications associated with AD?
sleep disturbances, impact quality of life and family's quality of life, skin infections, and depression
What skin infections are associated with AD?
S. aureus
Prone to infections with herpes simplex virus
Atopic dermatitis treatment goals
Eliminate triggers
Reduce symptoms
Prevent future flare-ups
Prevent secondary infections
Minimize adverse drug reactions
Reduce trans-epidermal water loss
You shouldn't use oral or topical antibiotics over what?
large areas of skin
How do you avoid stripping off the weakened epidermis?
Use gentle cleansers and limit bath time (bath water should not be too hot or too cold)
How do you help reestablish the epidermis?
moisturize with thick emollients and maintain hydration
How do you reduce inflammation when treating AD?
Use topical medications to reduce inflammation and decrease scratching
Atopic dermatitis bathing practices
Suggest a 10-minute lukewarm bath with gentle cleansers and then pat dry gently. Patients may add oatmeal or baking soda to bath water daily. After bathing, an occlusive moisturizer should be applied to decrease moisture release.
In severe cases patients can add what to their bath water?
May add bleach (0.005% Na hypochlorite = ½ cup bleach to full tub of water) twice a week, to prevent recurrent bacterial skin infections
What is the purpose of applying occlusive moisturizers immediately after bathing?
trap moisture and strengthen the skin barrier
What non-pharmacological treatments can be used to treat AD?
bathing practices, gentle cleansers, wet wrap, soft cotton clothing, avoiding unknown triggers, and decreasing stress
What is a wet wrap?
You wrap the skin in a gauze rag to trap moisture in, but it cannot be used with calcineurin inhibitors
OTC moisturizers: Petroleum-containing
Comments: Occlusive, greasy, can be uncomfortable
Examples:
- Aquaphor: Petrolatum
- Eucerin: Petrolatum, mineral oil
- Lubriderm: Mineral oil, lanolin, petrolatum
OTC moisturizers: Ceramide-containing
Comments: creams, provides barrier
Examples:
- CeraVe: glycerin, petroleum,ceramides, hyaluronic acid, etc
- Aveeno eczema therapy: Oatmeal, ceramides
OTC moisturizers: Urea-Containing
Examples: Carmol 10% ,20% and Lac-Hydrin 5%
Comments: Humectant
Side effects: burning, stinging, irritation on broken skin due to its acidic properties
OTC moisturizers: Emollients
Examples: Cetaphil Lotion, Keri Original, Neutrogena Lotion
Comments: Less effective and apply 3 x /day or more, after bathing/washing
What type of OTC moisturizer provides the best barrier?
Petroleum, while it may be greasy it has the best occlusive properties
When should a patient be referred to a physician for treatment of their AD?
If symptoms do not improve or worsen within 2-3 days of self treatment or if atrophy of the skin or infection while using a topical steroid occurs
What is the mechanism of action of topical corticosteroids?
When we give a steroid, it is always carried around the body by a protein. The glucocorticoid-binding globulin is what carries the steroid. The drug is carried around in our blood and then is eventually able to enter the cell. Once it enters the cell, it binds to the nuclear receptor. When any of our nuclear receptors are floating around in the cytosol, they are being chaperoned by other proteins and cannot be alone. The NR is chaperoned under it runs into the steroid, which then binds together, resulting in a steroid/receptor pair. The pair will find another steroid receptor pair and dimerize. They have to dimerize to be able to move into the nucleus and sit down on the glucocorticoid response element and affect gene transcription. This is the direct mechanism of a steroid.
Topical corticosteroids indication
Corticosteroid-responsive dermatoses, Anal genital pruritus, Hemorrhoids, Ulcerative colitis
Topical corticosteroids ADR
Skin burning, tingling, cracking, pruritus, acne, alopecia, headache, skin atrophy, delayed wound healing
Topical corticosteroids contraindications
Hypersensitivity to steroids, systemic fungal infections, obstruction, abscess, peritonitis,and treatment of diaper dermatitis
Topical corticosteroids pharmacokinetics
Absorption: varies depending on age, skin integrity, thickness of skin, and anatomic location
Topical corticosteroids counseling points
-Apply to clean and dry area
-Apply a thin layer and rub in gently until medication vanishes
-Store in a cool, dry, room temperature location
-Do not apply for longer than 2 weeks
What is the first line therapy for AD?
topical corticosteroids
What are the key guidelines for using topical hydrocortisone 1% for skin flare-ups?
Potency: Low to medium; safe for body and always used for the face.
Application: Apply twice daily for a maximum of 3–7 days, or until the flare-up clears.
Precautions:
If not resolved after 7 days, seek medical advice.
Do not use longer than 2 weeks.
In general, topical corticosteroids should not be used longer than what?
14 days but medical advice should be sought out after 7 days of use if there is no resolution
Steroid vehicle influences what?
the strength of the medication
Dosage forms in order of highest to lowest topical corticosteroid
Ointment > Creams > Lotions > Solutions > Gels > Sprays
Clobetasol Propionate 0.05% ointment, cream, or foam is a ___ potency topical corticosteroid
very high
Betamethasone dipropinate 0.05% cream, ointment, foam, solution is a ___ potency topical corticosteroid
high
Flucocinonide 0.05% cream, gel, ointment, solution is a ___ potency topical corticosteroid
high
Mometasone furoate 0.1% ointment is a __ potency topical corticosteroid
high
Mometasone furoate 0.1% cream is a ___ potency topical corticosteroid
medium
Triamcinolone acetonide 0.1% cream/ointment is a ___ potency topical corticosteroid
medium
Which topical corticosteroid is the lowest potency?
Hydrocortisone
Hydrocortisone 1% is available ___
OTC
What is the second line treatment option for atopic dermatitis?
Calcineurin inhibitors
Calcineurin inhibitors MOA
Action: Inhibit activation of T cells and mast cells → block production of proinflammatory cytokines and mediators
Effect: Reduce the extent and severity of symptoms
Note: Acts as an immunosuppressant
CD4⁺ T-Cell Activation & Calcineurin Inhibitors
Signal 1: APC presents antigen on MHC II, binding to T-cell receptor (TCR) → antigen recognition.
Signal 2 (Co-stimulation): APC CD80/86 binds CD28 on T-cell → activates intracellular signaling → calcineurin activates NFAT, which triggers IL-2 gene transcription.
Signal 3: Secreted IL-2 binds IL-2 receptor (CD25) on the same T-cell → drives T-cell proliferation and clonal expansion.
Calcineurin inhibitors (e.g., cyclosporine, tacrolimus):→ Block calcineurin, preventing NFAT activation → no IL-2 transcription → suppressed T-cell activation and immune response.
What is the indication for topical calcineurin inhibitors?
Mild-moderate AD, second line treatment
What ADRs are associated with topical calcineurin inhibitors?
skin burning, tingling, cracking, pruritus, coughing, and flu-like symptoms
Calcineurin inhibitors should ONLY be used as what?
Second-line treatment for a short, intermittent period of time
Calcineurin inhibitors are contraindicated with what?
Hypersensitivity to calcineruin inhibitors or any component of the formulation
Calcineurin inhibitors cannot be used in children under what age?
2
How should you counsel a patient on using calcineurin inhibitors?
-Apply to clean and dry area
-Apply a thin layer and rub in gently until medication vanishes
-Do not bathe, shower, or swim right after application
-Store in a cool, dry, room temperature location
-Do not use in children < 2 years of age
-Response in weeks, continue to apply (1-8 weeks)
What are the two topical calcineurin inhibitors?
Pimecrolimus and Tacrolimus
What is the brand name for pimecrolimus?
Elidel
What is the brand name for tacrolimus?
Protopic
What are pimecrolimus (Elidel) and tacrolimus (Protopic) used to treat?
mild to moderate eczema in children 2 years of age or older and adults
Pimecrolimus (Elidel) reduces the incidence of __
flares
What dosage form does Pimecrolimus (Elidel) come in?
1% cream that is applied to the affected area twice a day
What dosage form does tacrolimus (Protopic) come in?
ointment