Module 10- the digestive system
1/4
Earn XP
Description and Tags
What- the digestive system breaks down the food you eat into nutrients needed for metabolic processes, such as making ATP and rids the body of materials that cannot be used, such as fiber. How- chewing breaks down food into smaller peices, easy for enzymes to access. Enzymes then chemically digest food into nutrients that are actively trnasported into blood and delivered to cells around the body. Why- the digestive system is essential for providing the body with the energy and building bloacks it requires to maintain life
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
5 Terms
Structure and function of the digestive system
Learning outcome 1: outline the 2 anatomical groups of digestive system organs (gastrointestinal tract and accessory organs) and describe fundamental digestive processes they facilitate
Digestive system: structure
the 2 groups of organs that comprise the digestive system are the gastrointestinal tract and the accessory organs.
Gastrointestial tract
The GI tract is a continuous canal that extends from the mouth to the anaus. The GI tract contains food from the time it is eaten, until it is digested and absorbed or eliminated from the body. Organs of the gastrointestinal tract include the orgal cavity, the pharynx, the stomach and the small and large instestine. The length of the GI tract is 5-7meters.
oral cavity
pharynx
oesophagus
somach
small intestine
large intestine
anus
Accessory digestive organs
The accessory digestive organs include teeth, tongue, digestive glands (salivary glands, liver, pancreas) and gallbladder. The teeth and the tongue are located in the oral cavity, while the digestive glands and gallbaladder lie outside the GI tract and are connected to the tract by ducts. These organs assist digestion
tongue
teeth
salivary glands
liver
gallbaldeer
pacncreas
Digestive system: function
We can view the GI tract as a disassembely line in which food becomes less complex at each step of processing and its nutrients become avaiblae to the body. The processing of food by the digestive system involves 6 essential activities.
Ingestion- ingestion is taking food into the digestive tract (eating)
Mechanical breakdown- mecahnical breakdown increases the surface area of ingested food, physically preapring it for chemical digestion by enzymes. These processes include chewing (mastication), mixing food with saliva by the tongue, churing food in the stomach and segmentation (rhythmic contractions) of the small intestine
Propulsion- propulsion moves food through the alimentary canal. It includes swallowing, which is initated volunatrily, peristalsis which is a involuntary process.
Digestion- digestion involved a series of steps in which enzymes secreted into the lumen (cavity) of the GI tract break down complex food molecules to their chemical blocks
Absorbtion- absorbtion is the passage of digested end products (nutrients, electrolytes and water) from the lumen of the GI tract through the mucosal cells in the lining of the wall into the blood and lympth. This allows our body to use them for out normal metabolic processes of store them for later.
Defecation- defication eliminates undigested substances from the body via the anus in the form of feces
Peristalsis and propulation
Peristalsis is the unidirectional movement and is part of the propulation process (wave like)
oesophagus, stomach, small intestine
main function is to move food forward along the GI tracgt
coordinated, longituational contractions
like squeezing toothpaste from a tube
Segmentation is the bidirectional movement that occours during the mechanical breakdown of food
small instestine
its main function is to mix food with enzymes and enhancing nutrient absorbtion
muscle action is alternate and circualtiong
like kneeding dough
Gastrointestial tract: wall and support
Learning outcome 2: describe the 4 main layers of the wall of the gastrointestinal tract and explain their functions
Learning outcome 3: describe the strucutre and function of the perotoneum
Gastrointestinal wall
The wall of the gastrointestial tract, from the lower oesophague to the anal canal has the same basic- 4 layerd arrangement of tissues. These layers, from the inside out, are the mucosa, submusosa, muscularis and serosa
Mucosa- this is the inner layer of the GIT wall. It is compsed of epithelium in direct contact with GIT contents, a layer of aroelar connective tissue and a thin layer of smooth muscle that creates folds to increase the surface area for digestion and absorbtion. The mucosa also contains lymph nodules that protects against pathogens
Submucosa- this is a connective tissue layer that binds the musoca to the muscularis. It contains blood and lympthatic vessels that recieve absorbed food moleculaes. It also contains the submucosal plexus
Muscularis externa- this is a thick layer of muscle. In the oral cavity, pharynx and upper oesophague, it consists of skeletal muscle important for voluntary control of swallowing. Skeletal muscle also froms the external anal sphincter for defecation. In the rest of the GI tract, distal to the oesophague, the muscualris is composed of smooth muscle layers. The inner layer contains circualr fibres that wrap around the wall, while the outer layer had longituaional fibres that run the length of the wall. Movement of these musclles is involuntary and controlled by the myentric plexus
Serosa- this is the outermost layer that is comosed of simple squamous epithelium and areolar connective tissue. It secreates a watery lubricant called serous fluid, which allows the GI tract to glide easily past other organs as it moves around due to digestion
Peritoneum
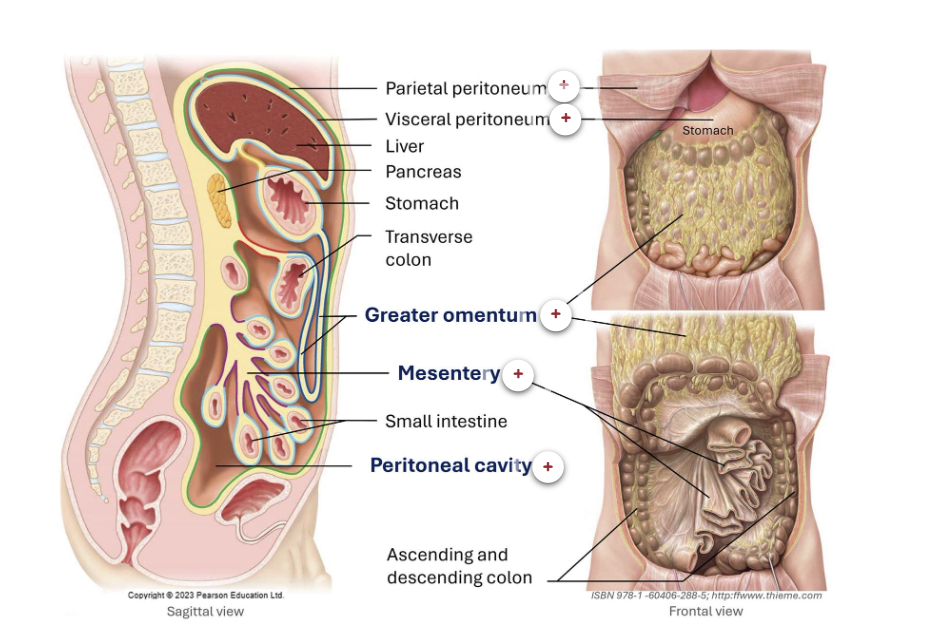
Most digestive organs are located in the abdomincal cavity, which is lined by a slippery serous membrane called the peritoneum. This membrane has 2 layers, the pariental peritoneum, which lines the abdomincal call and the visceral periotenum which covers the digestive rogans. Between them lies the periotneal cavity, a space containing a small amount of fluid that reduces friction as organs move.
The 2 layers are continuous: when the partiental peritoneum folds inwards to envelop the organs, it becomes the cisceral periotenum.
Intraperitoneal organs are entirelt enclosed by the visceral peritoneum, except at narrow regions where it reflects onto adjacnt strucutres or the abdomincal wall to become pariental periotenum. These reflections form periotenal folds, such as the mescentrey, which acnhors the small intesting to the posterior abdomincal wall.
stomach
small instesting
liver
transverse colon
Retroperotoneal organs lie on the posterior abdomincal wall behind the parietal peritoneum and are covered by the peroteum only on their anteropr surfaces
kidney
ureters
pancreas
The peritoneal cavity is a fluid filled space between the visceral and pariental periotenum
Peritoneal folds, such as the mesentery, play a crucial role in maintaining the structural organisation of the abdominal cavity. They anchor organs to the abdominal walls and connect organs to one another, helping to stabilise their positions and prevent displacement during movement. These folds also serve as conduits for blood vessels, lymphatics, and nerves that supply the abdominal organs. In addition to adipose tissue, peritoneal folds contains numerous lymph nodes, macrophages, and antibody-producing plasma cells, which contribute to immune defence by helping to combat and contain infections within the gastrointestinal tract.
Gastrointestinal tract: regions
Learning outcome 4: examine the strucutre and function of individual digestive organs, explaining their specific contributions to the overall digestive process
Oral cavity
The oral cavity or mouth is the entry point of the digestive system, where ingestion occours and digestion begins. The mouth is the site for a volunatry phase of swallowing and mechanical breakdown involving chewing by teeth and mixing morements by the tongue. Some chemical digestion is initated by enzymes present in saliva such as salivary amalyse (digestion of startch) and lingual lipase (digestion of fat). From the oral cavity, the soften food now a bolus is pushed to the pharynx during swallowing.
The lips surround the anterior opening of the mouth. The posterior boundary if sormed by the fauces that are arches seperating the oral cavity from the pharynx. The roof of the mouth is formed by the hard and soft palate while its floor is formed by skeletal msucles and the toungue resting on them. The lateral walls are the cheeks, composed of skin muscles of facial expression and connective tissue
Hard palate- the hard palate is the bony, anterior part of the roof of the oral cavity. It simulatnouly forms the floor of the nasal cavity. The hard palate is mostly formed by the maxillae and palatine bones
Soft palate- the soft palate is the muscualr, posterir part of the roof of the oral cavity. It is primarily composed of skeletal muscles. The soft palate elevates during swallowing to close off the nasopharynx, preventing the ingested material from enering the nasophaynx and nasal cavity
Palatine tonsil- the palatine tonsils are masses of lymphoid tissue located on either ides of the facuses. They have an important tole in immune defence by detecting and responding to pathogens entering through the mouth or nose
Lingual tonsils- the linguial tonsil is a collection of lymphoid tissue located at the base of the tongue, behind the oral cavity. It forms part of the immune system, helping to detct and respond to pathogens entering through the mouth or nose, and it one of the components of Waldeyers ring
Fauces- the fauces form the posterior boundary of the oral cavity, connecting it to the oropharynx through an arched opening. They serce as a passageway for both food and air and are borded by the 2 palatine arches with the palatine tonsils situated between them
Pharynx
The pharynx transports food from the mouth to the oesophagus via swallowing, a coordinated musclar process. Swallowing begins with a volunatray phase, where the tongue pushes the bolus into the oropharynx, followed by an involuntary phase involving reflecive contractions of the pharyngeal muscles. During this process, the soft palate elevates to block the nasopharynx, as the larynx rises, causing the epiglottis to close over the laryngeal inlet, to prevent food entry into the respiratory tract
the bolus of food is propelled from the oropharynx, into the laryngropharaynx and then into the oesphagus via perastalsis
Oesophagus
The oesophague is a fibrous muscualr tube, approxametely 25cm long that transports the bolus from the pharynx to the stomach via peristalsis duriing the involuntary phase of swallowing
the oesophagus begins at the C6 veterbea
it is continuous with the oropharynx
at this junction lies the upper oesophageal sphincter, a ring of skeletal muscle that remains closed at rest to prevent air entey and opens during swallowing to allow food passage
The oesophague descends through the neck then the mediastanim, and then devidates to the left to pass through the opening in the diaphragm to enter the abdominal cavity, where it almost immedigately joins the stomach
the junction between the oesophagus and sopmach contains a ring of smooth muscle called the lower oesophaeal spincter, which prevents the reflux of gastic contents back into the oesophague
Stomach
The stomach is a J shaped muscualr organ located predominantly in the upper left abdomical quadrant beheth the liver and diaphragm. It has 4 main regions (cardia, fundus, body and pyloric part) and functions as both a mixing chamber and a temporary reservoir. The stomach recieves the bolus from the oesphagus and digests it mechanically and chemically into a semi liquid mixture of partially digested food and gastric secretions called chyme
This organ plays a key role in chemical digestion by secreting pepsin, an enzyme that begins the breakdown of proteins into smaller peptides. Absorbtion in the stomach is limited to small inorganic sucbastances such as alcohol and some drugs. The stomach gragually resleases chyme into the duodenum (the first part of the small intestine) via the pyloric sphincter
Parts of the stomach
Cardia- the cardia is the region where the oesophagus connects to the stomach. It marks the entry point of ingested food from the oesophague into the stomach through the lower oseopheageal sphincter. The cardia are aditionally supported by a musclar fiber of the diaphragm providing further protextion against gastic reflux
Fundus- the fundus of the stomach is the dome shaped region located above and to the left of the cardia, just beneath the diaphragm. It typically contains swallowed air and playes a role in storing food temporarly before it moves into the body of the stomach for mixing and digestion
Body- the body of the stomach is the central and largest region that serves as the main site fort mixing and mechanical breakdown of food
Pyloric part- The pyloric part of the stomach is the lower funnel shaped portion that connects to the duodenum, the first part of the small intestine
Pyloric sphincter- the pyloric sphincter is a thick, circualr band of smooth muscle located at the junction between the stomach and the duodemun. It opens periodically to allow small amounts of chyme to enter to small intestine, ensuring proper difestion and also prevents backflow
Greater curvature- the greater curvature of the stomach is the longer, convex border on the left hand side of the stomach. It stretches from the cardia to the pylorus, forming the outer surve of the stomach
Lesser curvature- the concave border on the right hand side of the stomach that extends from the cardia to the pylorus
Small intestine
The small intestine is the primary site for digestion and absorbtion, aided by accessory organs such as the liver and pancreas. Segementation by smooth muscle of the small intestine continually mixes contents with digestive jusces, together with peristaltic waves moving food along the tract. Digestive enzymes delivered from the pancreas and intestinal mucosa, as well as bile from the liver, complete the digestion of macronutrients.
The small intestine is a long, convoluted tube extending from the pyloric sphincter of the stomach to the ileocecal valve, where it joins the large intestine. It is the longest part of the alimentary canal, occupying all 4 quadrants in the centre of the abdomical cavity, surrondided by the large intestine
duodenum- this is the first and shortest part of the small intestine. It begins at the pylorus of the stomach and ends as it becomes continuous with the jejeunim. It is located in the right upper quadrant of the abdomincal cavity. It curves around the head of the pancreas, and recieves secretions of the liver and pancreas to assist with chemical digestion
jejunun- the jejenum is the second part of the small intestine and exntends from the duodenum to teh ililum. It is locared promarity in the left upper quadrant of the abdominiopelvic cavity. This is where most of the chemical digestion and absorbtion occours
ilium- the ileium is the third and longest part of the small intestine extending from the jejunum to the large intestine at the ileocecal valve. The ilium is located primarily in the lower right quadrant of the abdomincal cavity. By the time chyme has reached the ilium, most of the digestion processes have occoured
Large intestine
The large intestine is primarily responsible for absorbing water and electrolytes, and for forming and storing feces. The 4 major functions of the large intestine are recovery of water and electrolytes, formation and storage of faeces and fermentation of some indigestible food matter by bacteria
ceacum- the caecum is a bline ended sac at the start of the large intestine, located in the right lower quadrant and extending from the ilocaecal valve to the ascending colon. The appendic, a thin, lymphoid rick projection typically arises from its posterior aspect
Ascending colum- the ascending colon continues from the caecum, running superiorly along the right slide of the abdomiopelvic cavity. It spans the right upper and lower abdomincal quadrants and ends at the right colic fkexure, where it blends to join the transverse colon near the liver
transverse colon- the transverse colon extends from the heaptic flexture to the splenic flexure, crossing the upper abdomen from right to left. It lies in the right and left upper quadrands of the abdomen
Descending colon- the descending colon extends from the splenic colic flexture down the left side of the abdominopelvic cavity, spanning the left upper and lower abdomincal quadrants. It continues into the sigmoid colon
Sigmoid colon- the sigmoid colon continues from the descending colon in the left lower quadrant, curving in a S shape before joining the rectum
Rectum- the rectum is the straight continuation of the sigmoid colon, located in the pelvis. it expands to steore feces before defication
Anal canal- the anal canal is the final segment of the large intestine, passing through the pelvic flood to the end of the anus
Accessory organs of digestion
Learning outcome 4 continued
Accessory organs of the oral cavity
Salivary glands- saliva cleanses the mouth, dissolves food chemicals to aid taste, moisten food and helps form it into a bolus. It also contains the enzyme amylase, which beginst the digestion of starches. Most saliva is produced by three pairs of major salivary glands: (a) the parotid gland, located anterior to the ear, with its duct opening into the oral vestibule (space between the lips and theeth); (b) the submandibular gland, found beneath the mandible, which produces the majority of saliva and opens under the tongue; and (c) the sublingual gland, located beneath the tongue, with multiple ducts opening into the floor of the mouth. In addition, numerous minor (intrinsic) salivary glands are scattered throughout the oral mucosa.
Tongue- The tongue is a muscular organ that plays a vital role in digestion and oral function. It manipulates food during chewing, helps mix it with saliva, and assists in forming a bolus for swallowing. The tongue also houses taste buds that detect food chemicals, contributing to the sense of taste. Its surface is covered with various types of papillae (some containing taste buds) and its movements are controlled by intrinsic and extrinsic muscles. In addition to its digestive functions, the tongue is essential for speech and oral cleansing.
Teeti- Teeth are anchored in sockets (alveoli) within the gum-covered margins of the mandible and maxilla. Chewing (mastication) involves coordinated jaw movements and the tongue to position food between the teeth, which tear and grind it into smaller fragments for easier swallowing and digestion. Humans develop two sets of teeth: 20 deciduous (milk) teeth, which begin to appear around 6 months of age, and 32 permanent teeth that gradually replace them between ages 6 and 12. As permanent teeth grow, they resorb the roots of the deciduous teeth, causing them to loosen and fall out. The permanent dentition (arrangement of teeth) includes four types of teeth (incisors, canines, premolars, and molars) each adapted for different functions such as cutting, tearing, and grinding. Each quadrant of the mouth contains 2 incisors, 1 canine, 2 premolars, and 3 molars (including the third molar or wisdom tooth), totaling 32 teeth in a full adult set.
The liver
The liver is a vital organ with numerous metabolic and regulatory fuctions, including detoxifying blood, processing and storing nutrients and vitamins, and synthesising plasma proteins.
Its digestive role is to produce bile, a fat emulsifier that aids difestion by breaking down fats into smaller particles for easier absorbtion.
The liver and the gallbladder, together with their ducts carry bile to the small intestine, refereed to as the hepatobilary system
the liver is the largest gland in the body. It is located promarily in the right upper quadrant of the adbomen, extending into the left upper quadrant, and lies beneath the diaphragm, protected by the rib cage. The liver has 2 surfaces: the diaphragmatic surface, which contacts the diaphragm, and the visceral surface, which bears impressions from adjacent abdomincal organs.
Anatomically, the liver is divided into 4 lobes: right, left, cuadate, quadrate. Functionally it is split into right and left halves, which do not directly corrospond to the anatomical lobes. The right and left lobes are seperated on the diaphragmatic surface by the flaciform ligament, a periotoneal fold anchoring the liver to the anterior abdomincal wall. On the visceral surface, the caudate and quadrate lobes flank the porta hepatis, the centeal gateway for hepatic vessels and ducts
Flaciform ligament- this is the thin peritoneal fold that attached the liver to the anterior abdomincal wall and diaphragm, marking the divsion between its right and left anatomical lobes
common hepatic duct- the common hepatic duct drains bile from the liver. It carries bile from the liver towards the common bile duct, where it joins with the cystic duct of the gallbladder. This duct is part of the bilary system that transports bile to the duodenum to aid in digestion.
cystic duct- the systic duct is a small tube that connects the gallbladder to the common bile duct. It allows bole stored in the gallbladder to flow into the common bile duct and then into the duogenum for digestion. It also enables bile form the liver to enter the gallbladder from storage
Common bile duct- the common bile duct carries bile from the liver and gallbladder to the major duodenal papillae located in the duodemun. It is formed by the unition of the common helatic duct (from the liver) and the cyctic duct (from the gallbladder). its main role is to deliver bile, which helps emulsify fats
the gallbladder- the galbladder is a small, pear shaped organ located beneath the right lobe of the liver. Its main function is to store and concentrate bile, a digestive fluid produced by the live, and releases it into the duodenum to help break down fats during digestion
Caudate lobe of liver- the caudate lobe is one of the 2 smaller subdivisions of the right lobe on the visceral surface of the liver. It has a tail like projection and lies next to the inverror vena cava, which runs in a depression on the viscueral surface of the lifer
Porta Hepatis
the porta hepatis is a central region on the visceal surface of the liver in between the caudate and quadrate lobes. It is the gateway of structures entering and exeting the liver. Includiding blood and lymphatic vessels. There are 3 main strucutres that either enter or exit the liver at the porta hepatis
portal vein that beings nutrient rich venous blood from the digestive tract to the liver for processing
Hepatic artery- that delivers oxygenated blood to nourish the liver itself
common hepatic duct which carries bile produced by the liver
Microsocpically, the liver is made up of repeating structural units called lobules, which are hexagonal arangements of hepatocytoes (liver cells) surrounding a centeal vein. Hepatocytes carry out essential meatabolic and detoxifying functions and also produce bile, which is collected via bile ducts to aid in fat digestion. Blood from the protal vein and hepatic artery flows through spaces called sinusoids, allowing exchange between blood and hepatocytes. The liver also contains specialised macrophages that help remove pathogens
Pancreas
The pancreas is a soft, tadpole shaped gland that stretches across the abdomen, from its tail near the spleen to its head, which is nestled within the C shaped curve of the duofenum. Most of the pancreas lies retroperitoneally, posteriorly to the stomach, primarily in the left upper quadrant, with a small portion extending into the right upper quadrant. It is a mixed gland, with both endocrine and exocrine functions. The endocrine component consists of scattered pancreatic islets, which sectrte insulin and glucagon, the they hormones in carbohydrate metabolies. The exocrine portion produces pancreatic juice, a mixture of digestive enzymes and bicarbonate. Enzyme rich fluid is secreted by acinar cells arranged in clusters called acini. Approxamately 1.5L of pancreatic juice is producted daily. The pancreatic enzymes include: proteases, amalyse, lipase, nucleases.
Pancreatice juice is collected into a series of ducts that merge into larger ones culminating in the main pancreatic duct, which joins the common bile duct and drains inot the duodemium via the major duodenal papilla. A smaller accessory pancreatic duct also drains a portion of the pancreatic juice inot the duodenum through the minor duodenal papilla, located superior to the major papilla
Major pancreatic duct- the main pancreatic duct is the largest duct in the pancreas. It carries pancreatic juice to the duodenum through the major duodenal papilla
Accessory pancreatic duct- the accessory pancreatic duct is a smaller duct in the pancreas. It drains a portion of pancreatic juice into the duodenum through the minor duodenal papilla
Major Duodenal papillae- the major duodenal papilla is the main opening in the duodenum releasing bile from the common bile duct and pancreatic juices from the main pancreatic duct into the duodenum, aiding digestion
The exocrine part of the pancreas produces pancreatic juice and consists of the following
Acini- these are clusters of secretory acinar cells that produce the enzyme rich compondet of pancreatic juide
ducts- that transport secretions of acinar cells. Epithelial cells of the smallest ducts secrete water and the bicarbonate that neutralises stomach acid and provides the environment optimal for enzymatic activity
Foundations of nutrient metabolism
Learning outcome 5: outline the processes involved in the digestion, absorbtion and metabolism of nutrients
Every time we eat, our body begins a complex journey to break down food, absorb nutrients and use them to fuel cells and maintain health.
Mouth and associated organs
ingestion: food is voluntarily places into the oral cavity
propulaion: voluntary (buccal)phase of deglutition (swallowing) initated by the tongue, which propells food into the pharynx
mechanical beakdown: mastication- chewing my teeth and mixing movements by the tongue
digestion: salivary amalyse in saliva, produced by the alivary glands, begins the digestion of starch
Pharynx and oesophagus
propulsion: peristalic waves move food bolus to stomach
Stomach
mechanical breakdown and propulsion: peristaltic waves mix food with gastric juice and propel it inot the duodenum
digestion: pepsin begins the digestion of proteins
absorbtion: absorbs a few fat soluble substances
Small intestine and associated organs
mechanical breakdown and propulsion
digestion: digestive enxymes delivered from the pancreas attach to the microvilli membranes to complete digestion
absorbtion
Large intestine
digestion: some remaining food residues are digested by gut bacteria
absorbtion: absorbs the remaining water
propulsion: propels feaces towards rectum by mass movements
defecation
Therefore digestive activities involve highly coordinated actions of multiple organs and occour in 3 overlapping phases
Cephalic- sensory and cognitive cues related to food activate brain centers that stimulate salivary and gastric secretions, prepating the mouth and stomach for incoming food
Gastric- the presense of food in the stomach stimulates stretch and chemical receptors, triggering neural and hormonal responses that enhance gastric secretions
Intestinal- the arrival of chyme in the small intestine triggers hormoal and neural responses that regualte gastric activiy and stimuate digestion, adsorbtion, and secretion in the intestine and accessory organs
Digestion is the catabolic process, where larger food molecules are broken down into monomers. This is especially relevant for macronutrients, like proteins, lipids and carbohydtates. Digestion is accomplished by enzymes secreted into the lumen of the alimentray canal by intrinsic and extrinsic organs.
Absorbtion is the process by which nutrients from the lumen of the alimentary canal across the epithelial cells of the intestial mucosea into the interstital fluid and then into blood capilaries
Regulation
The activities of the GI tract are regulated by neural, hormonal, and local mechanisms to ensure coordinated digestion and absorption. The enteric nervous system controls many functions within the gut wall, while signals from the autonomic nervous system (especially parasympathetic input) help modulate motility and secretion. Parasympathetic stimulation (mainly via the vagus nerve) generally enhances GI activity, while sympathetic stimulation inhibits it.
Hormones released by cells in the GI tract respond to the presence of food and help regulate digestive processes. These hormones also influence accessory organs: for example, they stimulate the pancreas to release digestive enzymes, the liver to produce bile, and the gallbladder to release bile into the small intestine. Local factors, such as stretching of the gut wall and chemical changes in the lumen, also trigger reflexes that adjust activity. Together, these systems ensure that digestion is well-timed and efficient across the entire digestive tract.