ICS Unit 3
1/177
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
178 Terms
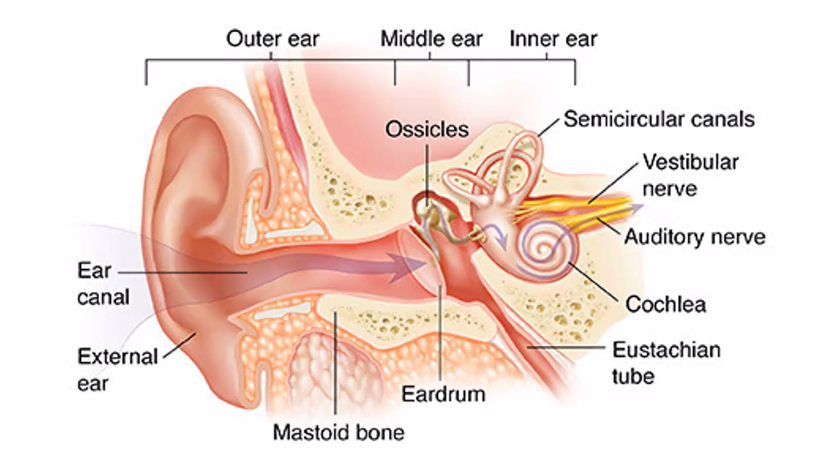
1. Outer Ear (Sound Collection)
The outer ear collects sound waves and directs them toward the eardrum.
Main parts:
Auricle (Pinna): The visible ear that funnels sound into the ear canal.
Ear Canal: Also called the external auditory canal.
It acts like a tube guiding sound waves to the eardrum.
Sound waves travel through the canal until they hit the eardrum.
2. Middle Ear (Sound Amplification)
The middle ear converts air vibrations into mechanical vibrations.
Eardrum (Tympanic Membrane)
When sound waves hit the eardrum, it vibrates.
Etymology
tympanum (Greek) = drum
So it literally means “drum membrane.”
Ossicles
The three smallest bones in the body:
Bone | Meaning | Function |
|---|---|---|
Malleus | hammer | attached to eardrum |
Incus | anvil | connects bones |
Stapes | stirrup | pushes into inner ear |
These bones amplify vibrations about 20×.
B)
endolymph is in scala media; it has high K+
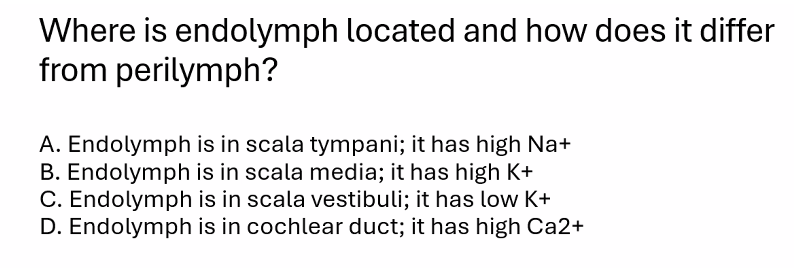
you missed a slide.
B)
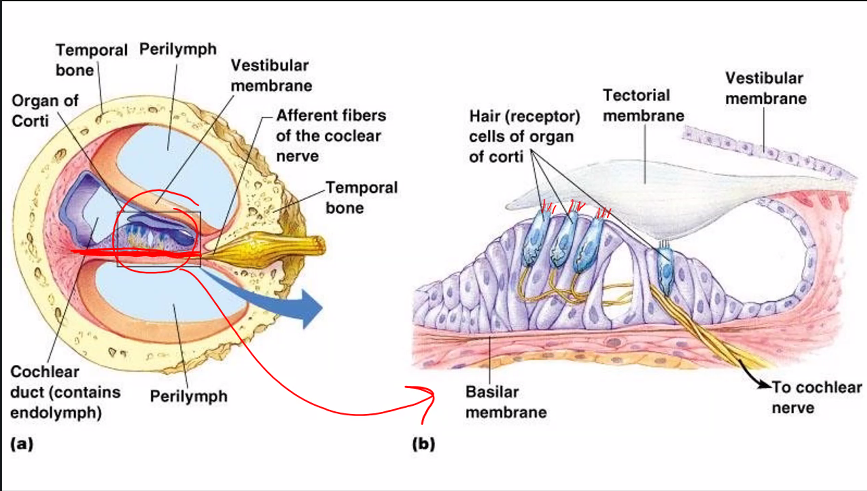
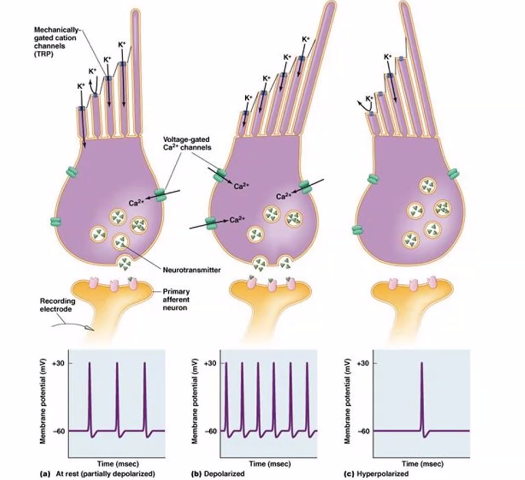
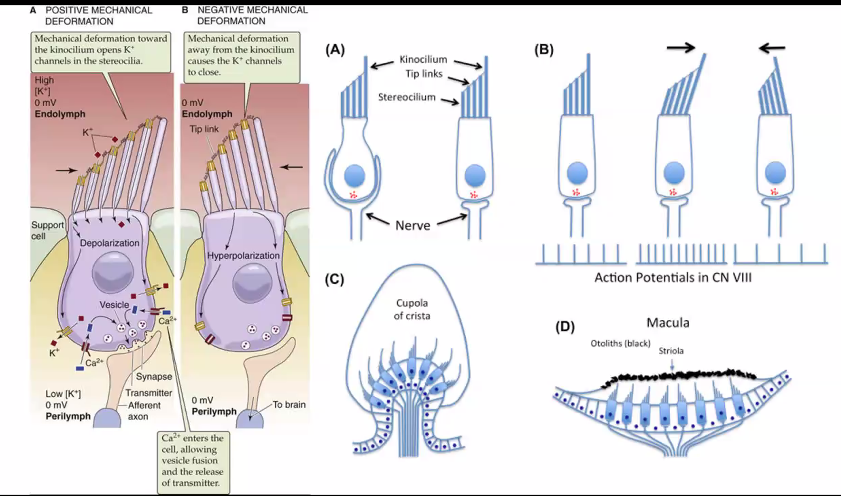
This figure shows how hair cells in the inner ear convert mechanical movement (sound or head motion) into electrical signals. This process is called mechanotransduction.
Hair cells are located in the Cochlea and are responsible for detecting sound vibrations.
Let’s walk through the three panels from left to right.
1. Structure of the Hair Cell
At the top of the cell are stereocilia (hair-like projections).
Inside these stereocilia are mechanically gated ion channels.
Important ions involved:
K⁺ (potassium) (very top)
Ca²⁺ (calcium) (middle)
At the bottom of the hair cell is a synapse with a primary afferent neuron that carries signals to the brain through the Vestibulocochlear Nerve.
2. Panel A — Resting State
When the stereocilia are not bent (resting), the hair cell is at its baseline electrical state.
What happens:
Some mechanically gated channels are slightly open.
A small amount of K⁺ enters the cell.
The cell releases a baseline level of neurotransmitter.
Result: The afferent neuron fires spontaneous action potentials.
The graph below shows a moderate baseline firing rate.
3. Panel B — Depolarization (Excitation)
When stereocilia bend toward the tallest cilium, the channels open wider.
Steps:
Mechanically gated channels open
K⁺ flows into the hair cell
The cell depolarizes
Voltage-gated Ca²⁺ channels open
Ca²⁺ enters the cell
More neurotransmitter is released
Result: The afferent neuron fires more action potentials.
The graph shows a higher firing frequency.
This signals increased sound intensity or movement.
4. Panel C — Hyperpolarization (Inhibition)
If stereocilia bend away from the tallest cilium, the channels close.
Steps:
Mechanically gated channels close
K⁺ cannot enter
The cell hyperpolarizes
Ca²⁺ channels close
Less neurotransmitter is released
Result: The afferent neuron fires fewer action potentials.
The graph shows reduced firing.
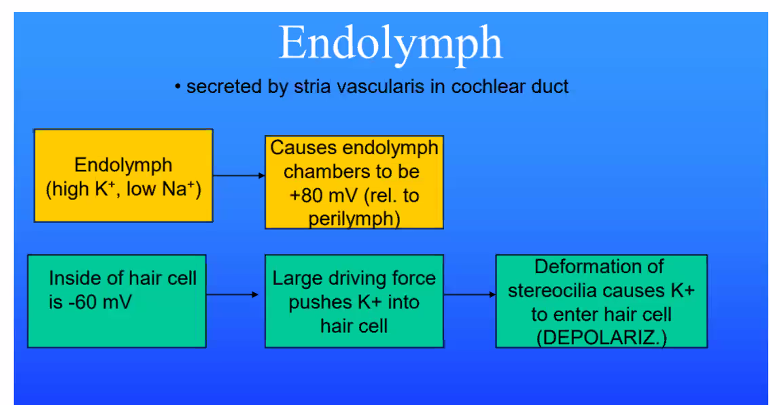
5. Why Potassium Enters the Cell
This is unusual because normally K⁺ leaves cells.
In the inner ear, however:
the surrounding fluid (endolymph) has very high potassium concentration
So potassium flows into the hair cell, causing depolarization.
6. Key Idea of the Diagram
Hair cells convert mechanical bending → electrical signals.
This allows the brain to interpret:
sound vibrations
head movement
balance
7. Simple Summary of the Three States
Stereocilia Movement | Cell Effect | Neuron Firing |
|---|---|---|
Neutral | baseline depolarization | normal firing |
Bend toward tall cilium | depolarization | increased firing |
Bend away | hyperpolarization | decreased firing |
Bending of hair-cell stereocilia opens or closes mechanically gated potassium channels, which changes neurotransmitter release and alters the firing rate of auditory neurons to encode sound or movement.
If you'd like, I can also show you the full cochlear sound-transduction pathway (basilar membrane → tectorial membrane → hair cells → spiral ganglion → auditory cortex), which connects this cellular diagram to how hearing actually works in the brain.
C)
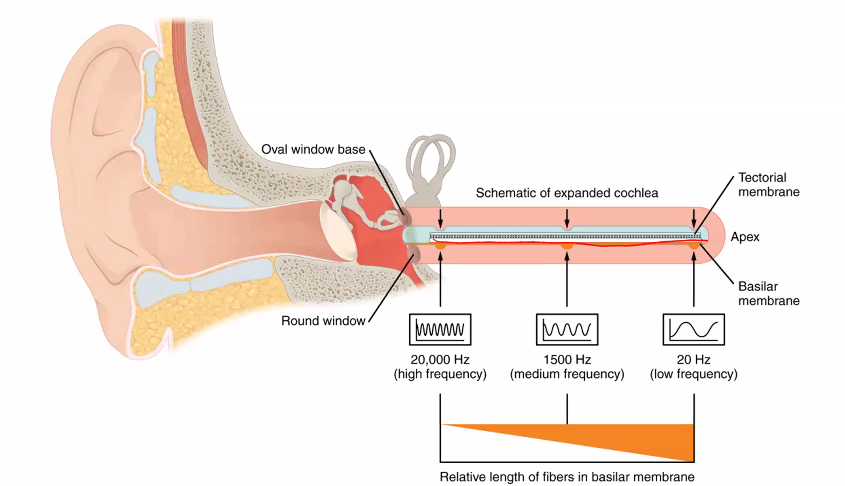
Tonotopic organization of the basilar membrane because frequency (pitch) in the cochlea is primarily encoded by place coding—that is, where along the basilar membrane the sound vibration is strongest.
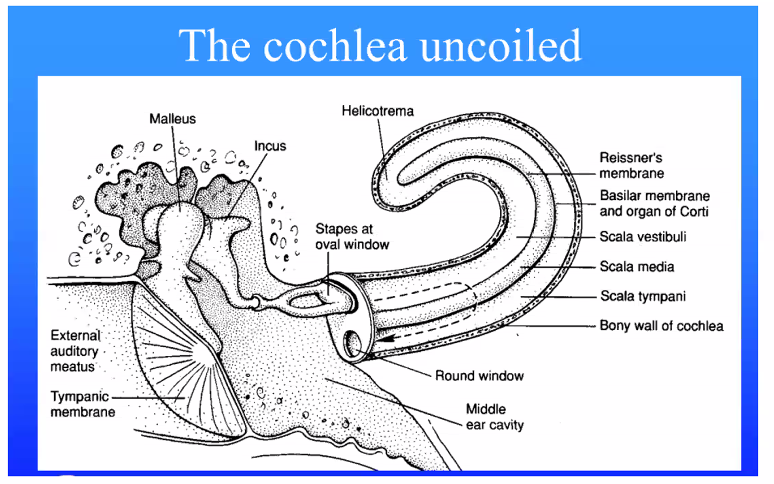
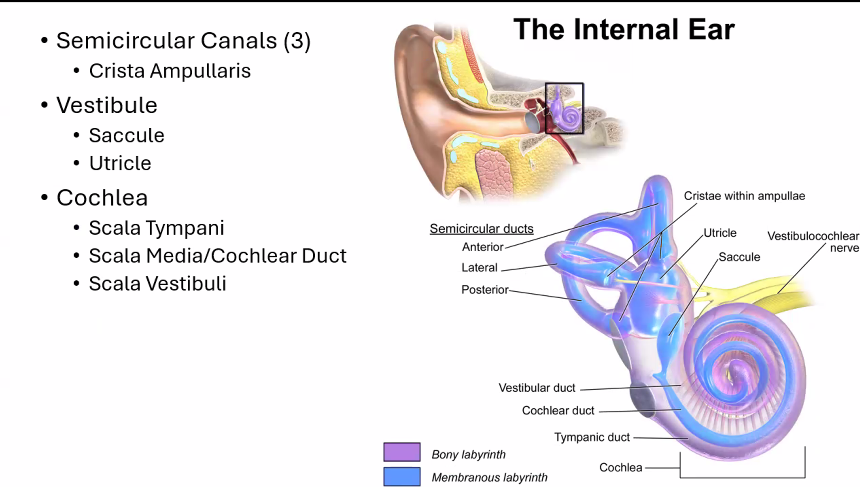
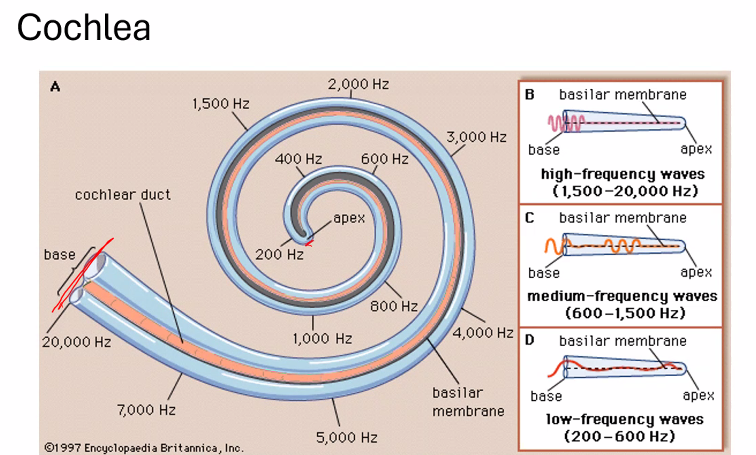
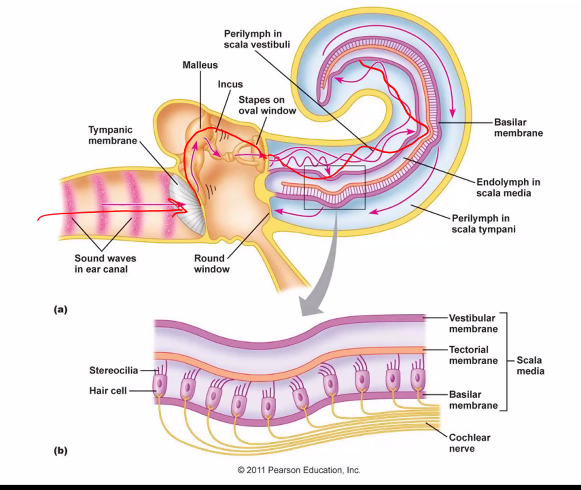
1. The Key Structure: Basilar Membrane
Inside the Cochlea is the Basilar Membrane.
Cochlea = “snail shell.”
The structure in the inner ear is named this because it looks like a spiral snail shell.
Hair cells sit on this basilar membrane.
When sound enters the cochlea, it creates traveling waves in the cochlear fluid, causing the basilar membrane to vibrate.
2. The Basilar Membrane Is Not Uniform
Different parts of the membrane respond to different sound frequencies.
Region of cochlea | Membrane properties | Frequency detected |
|---|---|---|
Base (near oval window) | stiff and narrow | high frequencies |
Apex (near helicotrema) | wide and flexible | low frequencies |
This arrangement is called tonotopy.
3. What “Tonotopic Organization” Means
Etymology
tono- = tone (sound frequency)
-topic = place or location
So tonotopic organization = different frequencies are represented at different locations.
Each sound frequency peaks at a specific place along the basilar membrane.
Example:
16,000 Hz → base of cochlea
200 Hz → apex of cochlea
Hair cells at that location activate the Cochlear Nerve, telling the brain which frequency is present.
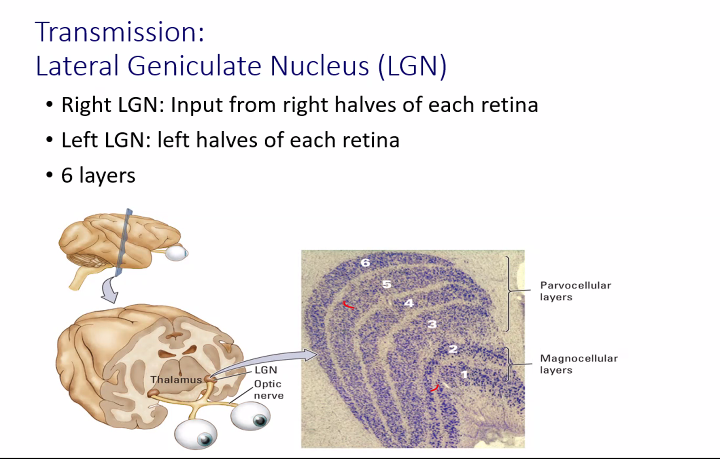
cochlea
C)
A)
B)
C)
A)
A)
A)
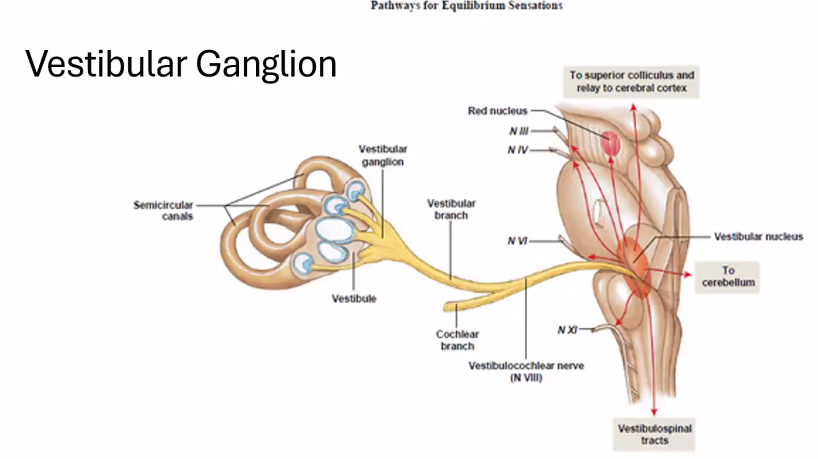
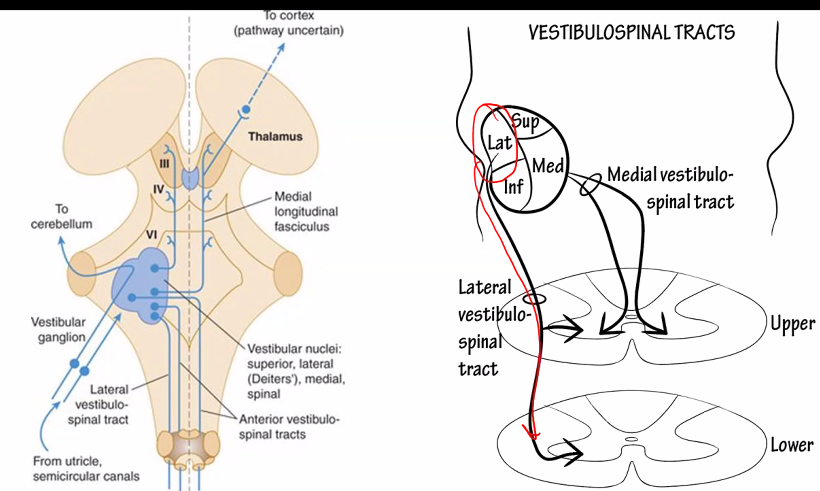
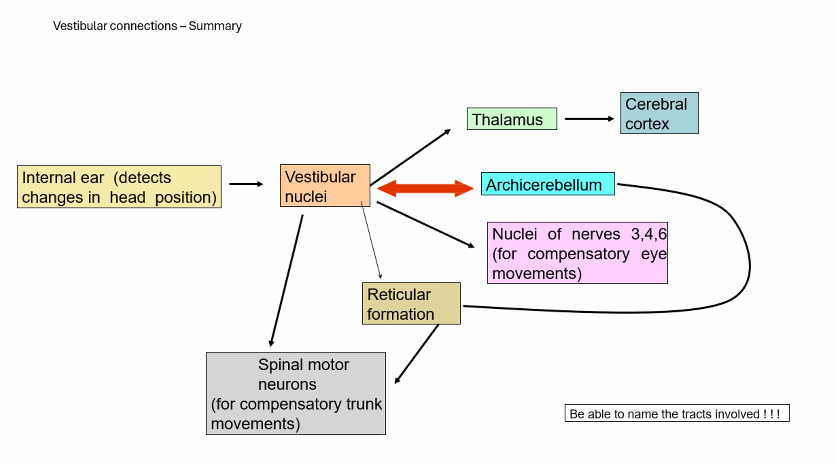
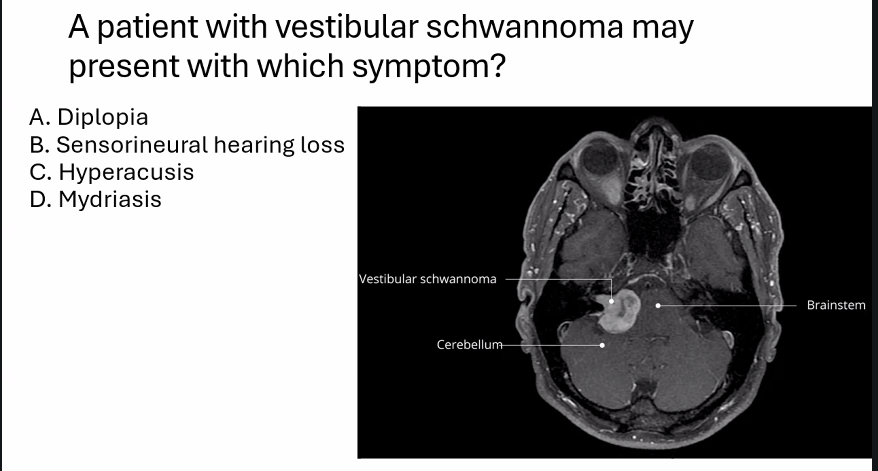
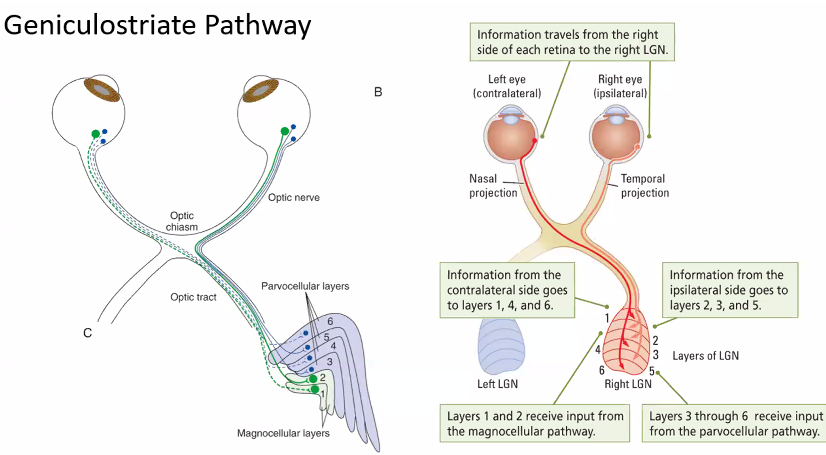
vestibular pathways
This diagram shows the vestibular pathways, which are the neural circuits that allow the brain to maintain balance, stabilize vision, and control posture when the head moves.
The signals begin in the inner ear balance organs and travel through brainstem nuclei to the eye muscles, spinal cord, and cerebellum.
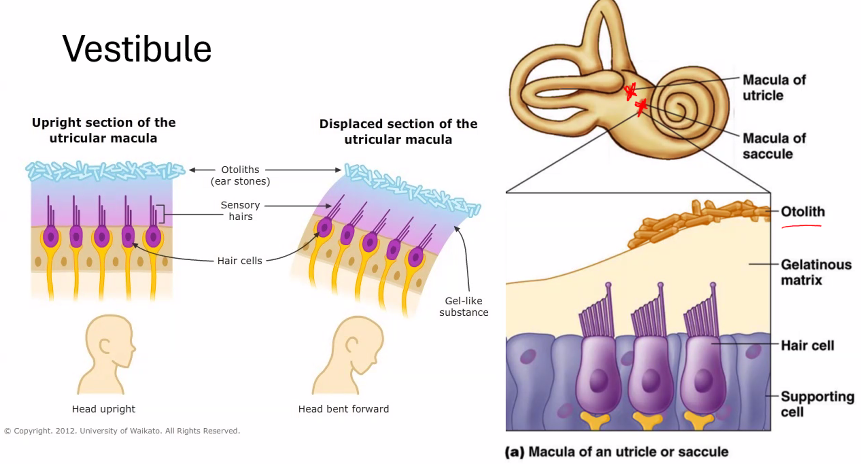
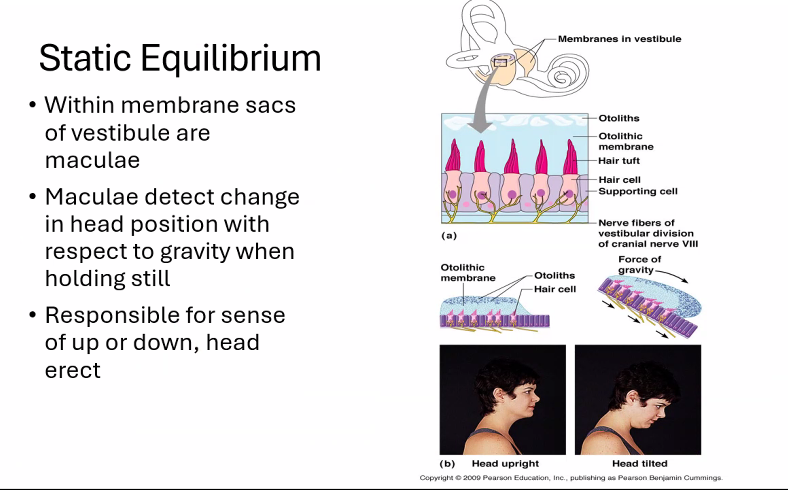
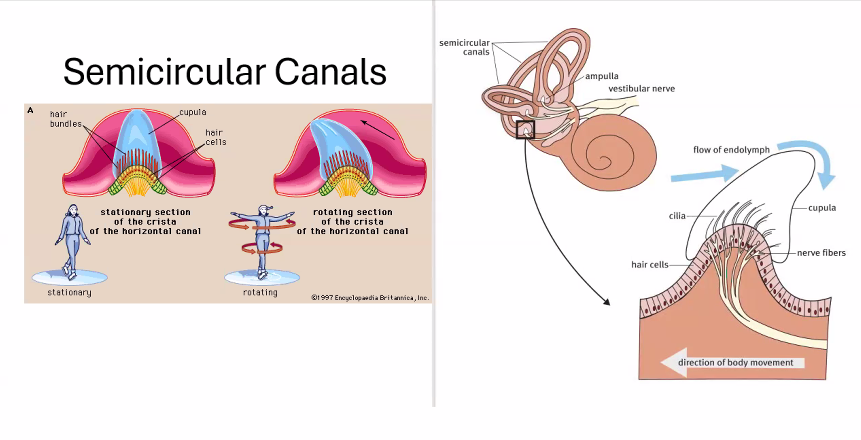
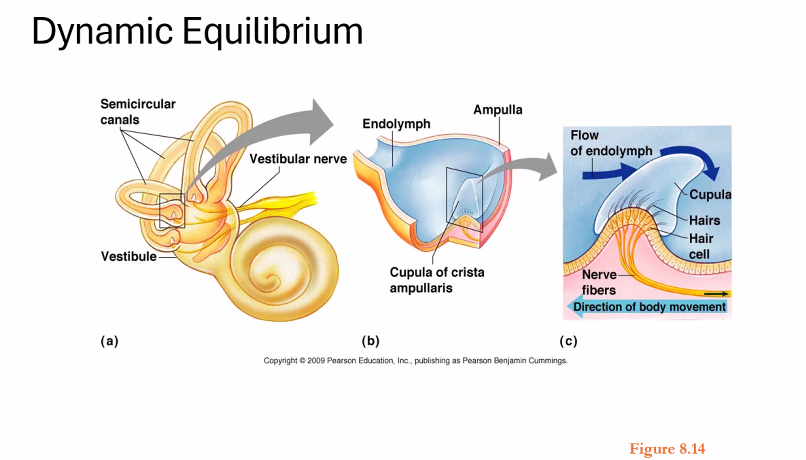
1. Where the Signals Start (Vestibular Organs)
The movement of the head is detected in the Semicircular Canals, Utricle, and Saccule.
Functions
Structure | Detects |
|---|---|
Semicircular canals | rotational head movement |
Utricle | horizontal acceleration |
Saccule | vertical acceleration |
These signals travel through the Vestibular Nerve.
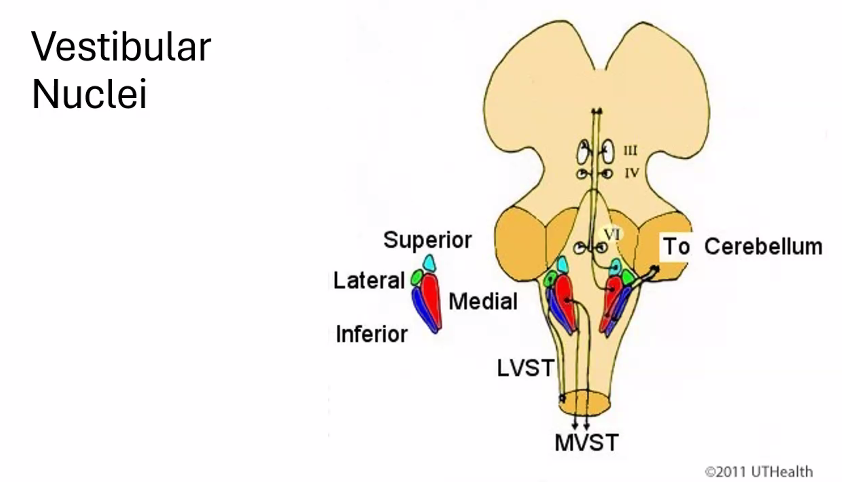
2. Vestibular Nuclei (Processing Centers)
The signals reach the vestibular nuclei in the brainstem.
Main nuclei:
Abbreviation | Name |
|---|---|
SVN | superior vestibular nucleus |
MVN | medial vestibular nucleus |
LVN | lateral vestibular nucleus |
IVN | inferior vestibular nucleus |
These nuclei coordinate eye movement, posture, and balance.
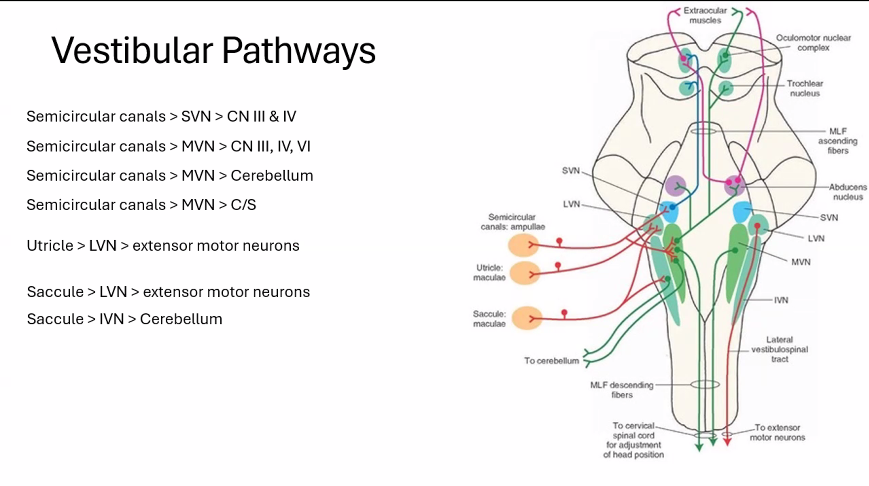
3. Pathways From the Semicircular Canals
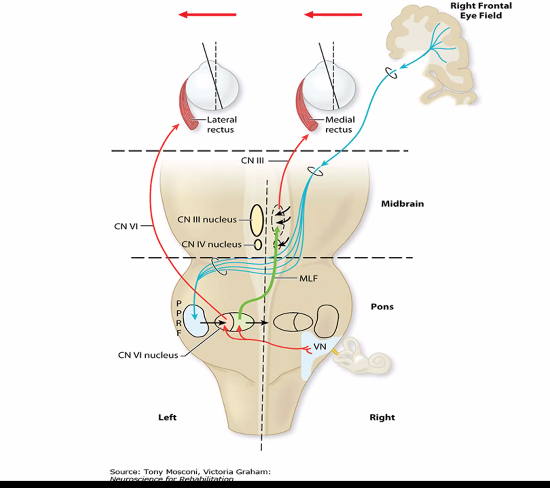
A. Eye Movement Control
Semicircular canals → SVN (superior vestibular nucleus, it is one of the four vestibular nuclei located in brainstem) → cranial nerves controlling eye muscles.
These include:
Oculomotor Nerve
Trochlear Nerve
Abducens Nerve
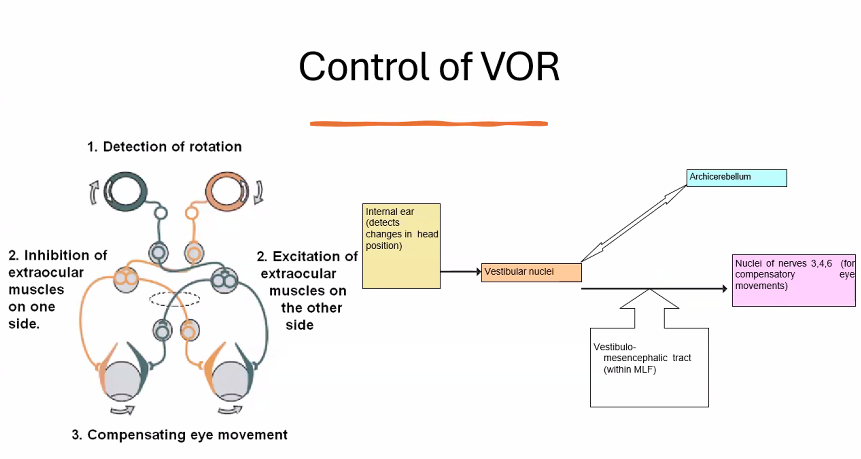
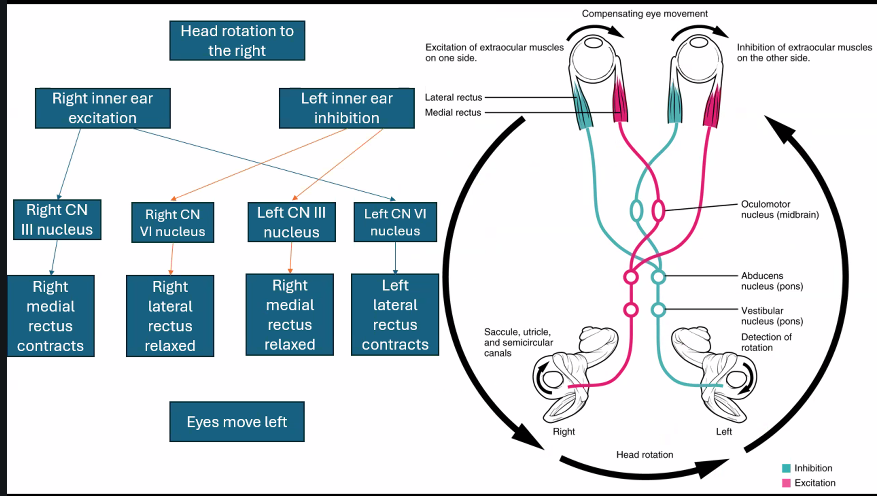
This pathway stabilizes vision when the head moves.
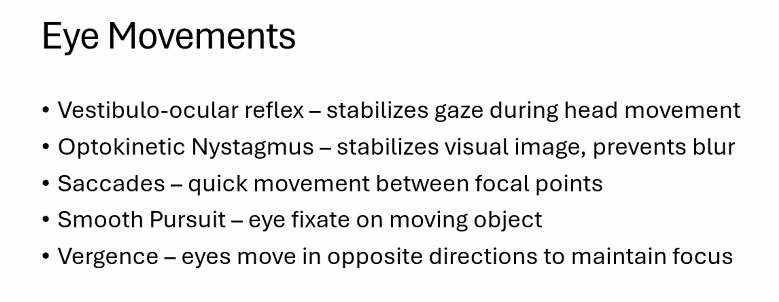
It forms the vestibulo-ocular reflex (VOR).
Example:
When you turn your head right, your eyes automatically move left to keep your gaze stable.
B. Cerebellar Coordination
Semicircular canals → MVN → cerebellum
The Cerebellum uses this information to fine-tune balance and coordination.
C. Spinal Cord Control
Semicircular canals → MVN → spinal cord
These signals adjust neck muscles and posture
4. Pathways From the Utricle
Utricle → LVN → extensor motor neurons
This pathway forms the lateral vestibulospinal tract.
Function:
activates extensor muscles
maintains upright posture
Example:
When you lean forward, this reflex activates muscles to prevent you from falling
5. Pathways From the Saccule
Saccule → LVN → extensor motor neurons
Also contributes to postural reflexes.
Another pathway:
Saccule → IVN → cerebellum
This provides balance information for coordination.
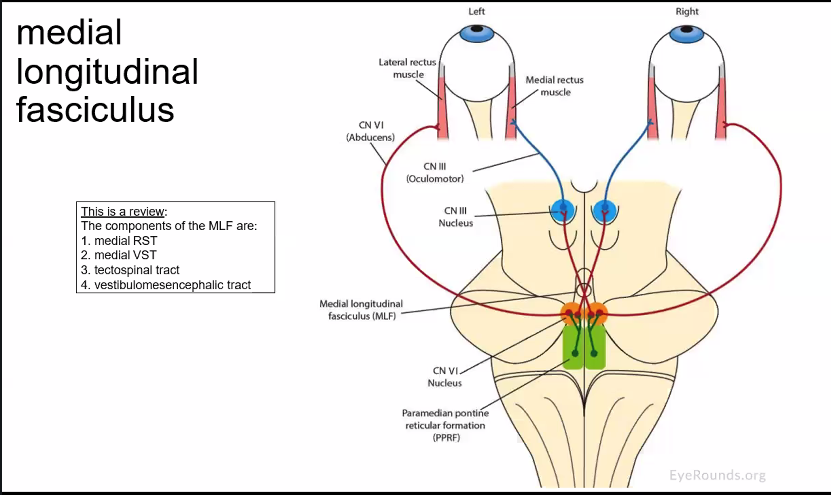
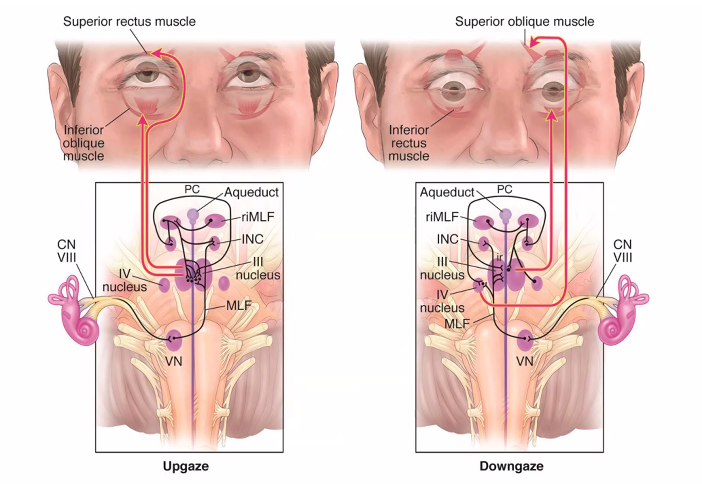
6. The Medial Longitudinal Fasciculus (MLF)
In the diagram you see the Medial Longitudinal Fasciculus.
This tract connects:
vestibular nuclei
eye muscle nuclei (III, IV, VI)
It allows rapid coordination of eye movements with head movement.
7. Big Picture
Vestibular pathways have three major functions:
Function | Pathway |
|---|---|
stabilize vision | vestibulo-ocular reflex |
maintain posture | vestibulospinal tracts |
coordinate balance | cerebellar connections |
B)
D)
A)
she guarantees one of not multiple questions on this next exam.
A)
C)
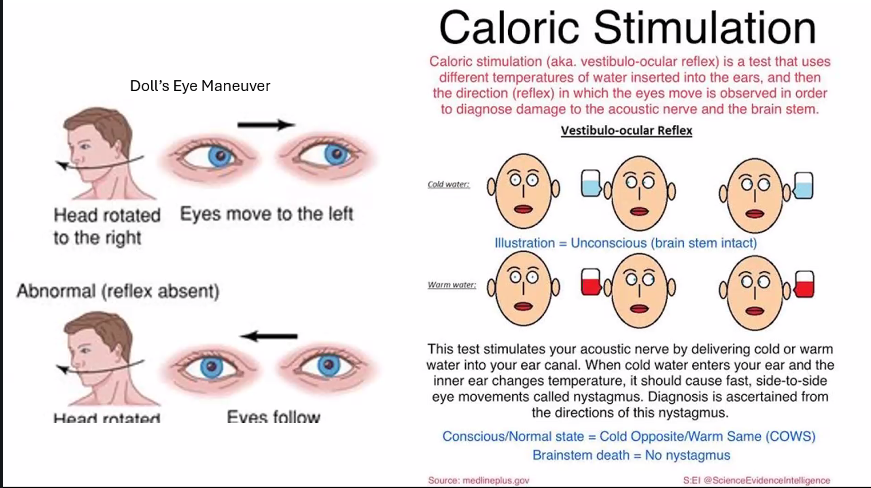
COWS:
cold→ opposite
warm → same
B)
B)
jerking eye movement (tiny but still there)
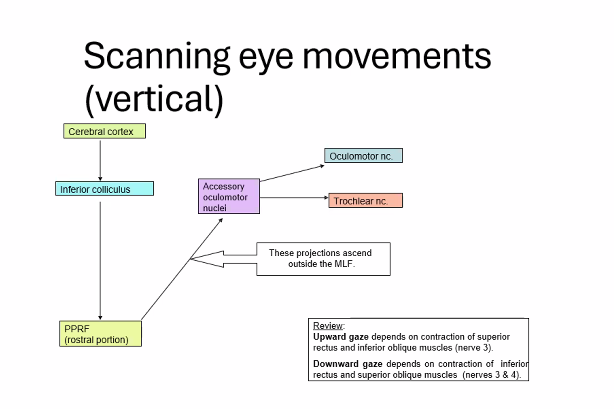
Saccades
-can be voluntary and involuntary
-this is normal, however, neurological disorder represents delay, undershooting or overshooting.
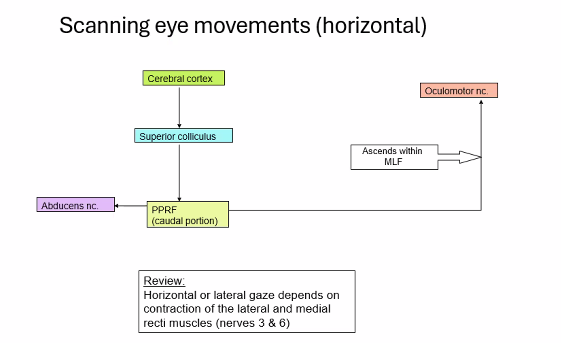
superior colliculus are most involved in saccadic eye movements.
A)
B)
vergence and convergence
B)
general appearance
These terms come from neurology and physical examination, especially when evaluating movement disorders during a clinical exam.
very important
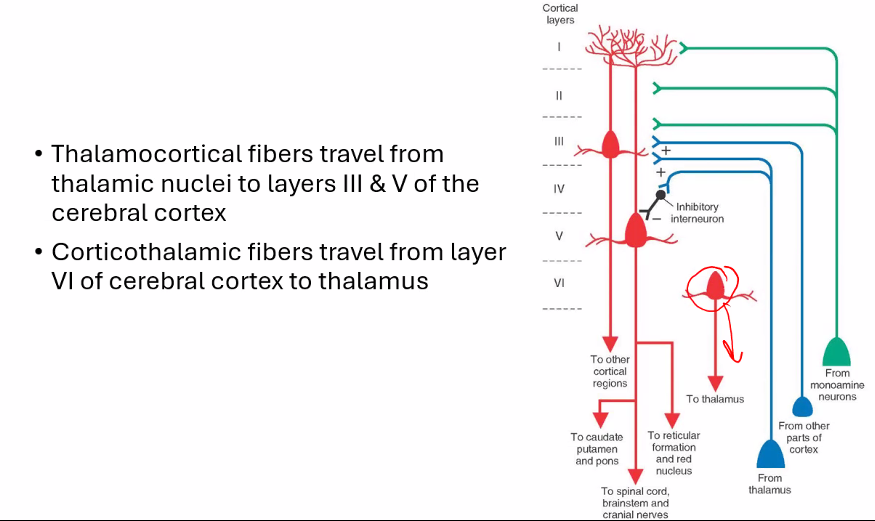
cerebral cortex excites the basal ganglia
basal ganglia sends inhibitory signals to the thalamus
thalamus excites the cerebral cortex
1. Step 1 — Cortex Excites the Basal Ganglia
The cerebral cortex sends excitatory signals (glutamate) to the striatum (caudate + putamen).
cerebral cortex (+) → Basal ganglia
Meaning: The cortex is basically saying: “I want to make a movement”
2. Step 2 — Basal Ganglia Inhibit the Thalamus
The output of the basal ganglia (mainly the globus pallidus interna) sends inhibitory signals (GABA) to the thalamus.
basal ganglia (-) → Thalamus
So normally the basal ganglia act like a brake on the thalamus.
basal ganglia = movement brake
3. Step 3 — Thalamus Excites the Cortex
The thalamus sends excitatory signals back to the cortex.
thalamus (+) → Cortex
When the thalamus is active, it stimulates the motor cortex, which then sends commands to the muscles.
4. Why This Loop Exists
The purpose of this loop is to control which movements are allowed.
The basal ganglia do two things:
Allow desired movements
Suppress competing movements
So they help make movements:
smooth
precise
coordinated
5. The Important Concept: “Disinhibition”
Movement happens when the basal ganglia temporarily remove their inhibition of the thalamus.
Normal state:
Basal ganglia inhibit thalamus
↓
Movement suppressed
When movement is selected:
Basal ganglia reduce inhibition
↓
Thalamus activates cortex
↓
Movement occursThis process is called disinhibition.
6. Simplified Analogy
Think of the system like a car.
Structure | Analogy |
|---|---|
Cortex | driver |
Basal ganglia | brake |
Thalamus | accelerator |
Muscles | wheels |
So movement occurs when:
Brake released
↓
Accelerator pressed
↓
Car moves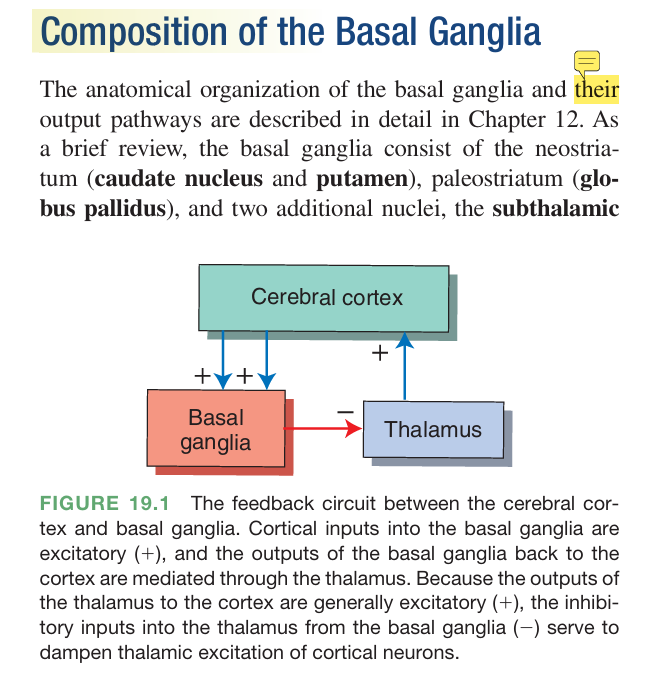
1. Chorea Etymology
Greek (choreia) = dance
Root choros = dance or chorus
Chorea refers to irregular, unpredictable, dance-like movements.
The movements:
are rapid
non-rhythmic
move randomly from one body part to another
It looks like the patient is dancing involuntarily.
Example diseases
Huntington's disease
Sydenham chorea
Mechanism
Usually due to damage to the basal ganglia, especially the striatum. why?
To understand why damage to the basal ganglia (especially the striatum) causes chorea, we need to look at how the basal ganglia normally control movement. The key idea is that the basal ganglia act as a movement filter:
they allow desired movements
they suppress unwanted movements
When that filtering system breaks, extra unwanted movements escape, which appear clinically as chorea.
1. What the Basal Ganglia Normally Do
The main structures involved are:
striatum (caudate + putamen)
globus pallidus
subthalamic nucleus
substantia nigra
thalamus
The striatum is the input center of the basal ganglia.
It receives signals from:
the cerebral cortex (motor plans)
dopamine from the substantia nigra
The basal ganglia then regulate the motor cortex through the thalamus.
So the circuit is roughly:
cortex → striatum → globus pallidus → thalamus → cortex
The basal ganglia use two major pathways to regulate movement.
2. The Two Pathways That Control Movement Direct Pathway
Purpose: facilitates movement
Sequence:
cortex excites striatum
striatum inhibits GPi
GPi normally inhibits thalamus
Wen GPi is inhibited → thalamus becomes active
Thalamus excites motor cortex
movement occurs
So the direct pathway turns movement ON.
Indirect Pathway
Purpose: suppresses unwanted movement
Sequence:
1. cortex exicites striatum
striatum inhibits GPe
GPe normally inhibits subthalamic nucleus
When GPe is inhibited → subthalamic nucleus becomes active
Subthalamic nucleus excites GPi
GPi strongly inhibits thalamus
Movement is suppressed.
So the indirect pathway turns movement OFF.
3. What Happens in Chorea
In chorea (like in Huntington's disease), the first neurons that die are in the striatum, specifically:
GABA neurons of the indirect pathway
This produces the following effect.
Step-by-step
1⃣ Striatal neurons of the indirect pathway degenerate
2⃣ The globus pallidus externa (GPe) is no longer inhibited
3⃣ GPe becomes overactive
4⃣ GPe inhibits the subthalamic nucleus too strongly
5⃣ The subthalamic nucleus becomes underactive
6⃣ The globus pallidus interna (GPi) receives less excitation
7⃣ GPi fails to inhibit the thalamus
8⃣ The thalamus becomes overactive
9⃣ The thalamus overstimulates the motor cortex
🔟 The motor cortex produces excess, uncontrolled movements
These are the jerky, dance-like movements of chorea.
2. Athetosis Etymology
Greek (athetos)
a- = without
thetós = fixed or placed
Meaning “without a fixed position.”
Athetosis refers to slow, writhing, snake-like movements.
Characteristics:
slow
continuous
twisting
mostly affects hands and fingers
The fingers may look like they are slowly twisting or flowing.
Cause
Often seen in:
cerebral palsy
basal ganglia injury
Athetosis is a hyperkinetic movement disorder characterized by slow, continuous, writhing movements, usually of the hands, fingers, feet, or face. The cause almost always involves damage to parts of the basal ganglia, particularly the striatum, especially the putamen and globus pallidus.
1. Primary Cause: Basal Ganglia Injury
The most common cause of athetosis is damage to the basal ganglia, especially:
Putamen
Globus pallidus
sometimes the caudate nucleus
These structures normally regulate muscle tone and suppress unwanted movements.
When they are damaged:
inhibitory motor control is disrupted
competing motor signals are not suppressed
muscles receive irregular signals
This produces slow twisting movements.
4. Why Movements Are Slow (Unlike Chorea)
Movement disorders depend on which part of the basal ganglia is damaged.
Disorder | Movement type | Speed |
|---|---|---|
Chorea | jerky dance-like movements | fast |
Athetosis | twisting writhing movements | slow |
Hemiballismus | violent flinging movements | very fast |
Athetosis often involves globus pallidus dysfunction, which affects muscle tone regulation, producing sustained slow contractions.
4. Dystonia Etymology
Greek:
dys- = abnormal or difficult
tonos = tension or muscle tone
Meaning abnormal muscle tone.
Meaning
Dystonia = sustained muscle contractions that produce:
twisting movements
abnormal postures
Example:
neck twisted to one side
hand locked in abnormal position
Mechanism
Usually due to basal ganglia dysfunction.
Dystonia occurs when the basal ganglia fail to properly regulate muscle activation, causing sustained, involuntary contractions and abnormal postures. To understand why, we need to look at what the basal ganglia normally do in movement control.
1. What the Basal Ganglia Normally Do
The basal ganglia function as a movement selection and inhibition system.
Their main job is to:
Select the desired movement
Suppress competing movements
Control muscle tone and posture
They do this through loops involving:
Striatum (caudate + putamen)
Globus pallidus interna (GPi)
Globus pallidus externa (GPe)
Subthalamic nucleus
Thalamus
Motor cortex
Normally: basal ganglia → regulate thalamus → regulate motor coordination
The GPi sends inhibitory signals to the thalamus, acting as a movement brake.
2. What Goes Wrong in Dystonia
In dystonia, basal ganglia inhibition becomes abnormal.
Specifically:
GPi output becomes irregular or reduced
The thalamus becomes overactive
The motor cortex receives excessive or disorganized signals
Multiple muscle groups activate simultaneously
Instead of one muscle contracting while the opposite relaxes:
agonist muscle contractions
antagonist muscle also contracts
This produces:
twisting
sustained contractions
abnormal postures
3. Loss of “Surround Inhibition”
One key mechanism is the loss of surround inhibition.
Normally the basal ganglia do this:
-activate the desired movement
-suppress the surrounding muscles
Example:
To move your finger:
finger flexor muscles activate
neighboring muscles are inhibited
In dystonia: Finger flexor activated
Nearby muscles also activated
Result:
twisting
abnormal posture
4. Abnormal Muscle Co-Contraction
Because the inhibitory control is lost:
agonist and antagonist muscles contract together
Example in cervical dystonia: sternocleidomastoid + opposing neck muscles both contract.
This produces torticollis (twisted neck).
5. Role of Dopamine and Neurotransmitters
Basal ganglia circuits depend on several neurotransmitters:
dopamine
GABA
acetylcholine
Imbalance in these signals can disrupt motor control.
Examples:
dopamine dysfunction
abnormal GABA inhibition
cholinergic imbalance
These disrupt the precision of motor control circuits.
6. Structural Areas Often Involved
The structures most associated with dystonia include:
putamen
globus pallidus interna
thalamus
cerebellar connections
Modern research shows dystonia involves a network disorder, not just a single nucleus.
5. Torticollis Etymology
Latin:
tortus = twisted
collum = neck
Meaning “twisted neck.”
A form of cervical dystonia where the neck muscles contract and the head turns to one side.
Torticollis (twisted neck) is most commonly a form of cervical dystonia, meaning the neck muscles contract involuntarily due to abnormal motor control circuits, particularly involving the basal ganglia and brainstem motor pathways. The mechanism can be understood at three levels: muscular, neural circuits, and neurotransmitters.
It describes a condition where the head is pulled to one side, rotated, or tilted due to involuntary muscle contraction.
2. Muscles Involved
The main muscle responsible is usually the:
sternocleidomastoid (SCM)
Etymology
sterno = sternum
cleido = clavicle
mastoid = mastoid process of temporal bone
Function of SCM:
Muscle contraction | Head movement |
|---|---|
One SCM contracts | head rotates to opposite side |
Both SCM contract | neck flexion |
The most common cause of torticollis is basal ganglia dysfunction.
Normally the basal ganglia:
coordinate muscle activity
suppress unwanted movements
ensure only the correct muscles activate
In cervical dystonia:
basal ganglia inhibition fails
Motor cortex sends EXCESSIVE signals
Neck muscles receive abnormal activation
Sustained Muscle contraction occurs
The globus pallidus interna (GPi) normally inhibits the thalamus.
If this inhibition becomes abnormal:
thalamus becomes overactive
motor cortex overstimulated
neck muscles contract involuntarily
In torticollis, one SCM contracts continuously, causing:
head rotation
head tilt
abnormal posture
Other neck muscles may also be involved:
splenius capitis
trapezius
levator scapulae
Causes
congenital
trauma
neurological disorders
The head may appear:
tilted
rotated
pulled to one side.
6. Opisthotonos Etymology
Greek:
opistho- = behind
tonos = tension
Meaning “backward muscle tension.”
A severe spasm where the body is arched backward.
Appearance:
head and heels bent backward
spine severely arched
Causes
Seen in severe neurological conditions like:
Tetanus
meningitis
severe brain injury
Mechanism:
extreme muscle hypercontraction.
3. Normal Motor Control
Normally, muscle tone is controlled by a balance between excitatory and inhibitory signals in the central nervous system.
Important inhibitory neurons use GABA and glycine.
These inhibitory signals suppress excessive muscle contraction.
Normal balance:
excitatory signals → activate muscles
inhibitory signals → limit contraction
4. What Goes Wrong in Opisthotonos
In opisthotonos, inhibitory control is lost.
This causes overactivation of motor neurons in the spinal cord.
Mechanism:
Loss of inhibitory interneurons
↓
Alpha motor neurons become hyperactive
↓
Extensor muscles contract continuously
↓
Severe body arching5. Classic Cause: Tetanus
The most famous cause is infection by
Tetanus.
Mechanism in tetanus
The bacterium produces tetanospasmin toxin.
Step-by-step:
Toxin enters peripheral nerves
Travels retrograde along axons to the spinal cord
Blocks release of inhibitory neurotransmitters
Specifically blocks:
GABA
glycine
This occurs in Renshaw inhibitory interneurons.
Result:
No inhibition of motor neurons
↓
Continuous firing of motor neurons
↓
Severe muscle spasms
↓
Opisthotonos6. Why Extensor Muscles Dominate
Extensor muscles (anti-gravity muscles) are normally more strongly activated in the spinal cord.
When inhibition disappears:
Extensors overpower flexors
↓
Body arches backwardThis is why opisthotonos produces backward arching rather than forward bending.
7. Tardive Dyskinesia Etymology
Tardive
Latin tardus = slow or delayed
Dyskinesia
dys- = abnormal
kinesis = movement (Greek kinesis = motion)
“Delayed abnormal movement.”
Meaning
A movement disorder caused by long-term dopamine receptor blockade.
Most commonly due to antipsychotic drugs.
Characteristic movements
lip smacking
chewing motions
tongue protrusion
teeth grinding
facial grimacing
These movements are:
repetitive
involuntary
Mechanism
Chronic dopamine blockade causes dopamine receptor supersensitivity in the basal ganglia.
2. Brain Structures Involved
The disorder primarily affects the basal ganglia, especially:
striatum (caudate + putamen)
globus pallidus
motor cortex circuits
The striatum is critical because it contains neurons with dopamine D₂ receptors that regulate movement.
3. Normal Dopamine Function in the Basal Ganglia
Dopamine from the substantia nigra modulates two pathways:
Direct pathway
Promotes movement.
Indirect pathway
Suppresses movement.
Dopamine:
stimulates the direct pathway
inhibits the indirect pathway
Net effect:
Dopamine → promotes smooth voluntary movement4. What Antipsychotic Drugs Do
Many antipsychotic medications block dopamine D₂ receptors.
Examples include:
Haloperidol
Chlorpromazine
Mechanism:
Drug blocks dopamine receptors
↓
Dopamine signaling decreases
↓
Indirect pathway becomes dominant
↓
Movement suppression
Early on this can cause parkinsonian symptoms.
5. Long-Term Adaptation of the Brain
With chronic dopamine blockade, neurons adapt.
They do this by increasing the number and sensitivity of dopamine receptors.
This process is called dopamine receptor supersensitivity.
Mechanism:
Chronic D₂ blockade
↓
Neurons upregulate dopamine receptors
↓
Receptors become hypersensitive6. When Dopamine Stimulates These Receptors
Once the receptors become hypersensitive:
Even small amounts of dopamine produce excessive motor activity.
Result:
Hypersensitive dopamine receptors
↓
Overactive striatal signaling
↓
Excess motor output
↓
Involuntary repetitive movementsThese movements include:
lip smacking
chewing motions
tongue protrusion
teeth grinding
facial grimacing
7. Why the Mouth and Face Are Commonly Affected
The orofacial region has strong representation in the basal ganglia motor circuits.
These circuits control:
chewing
swallowing
speech movements
When dysregulated, they produce stereotyped oral movements.
8. Role of GABA and Other Neurotransmitters
Besides dopamine, other systems become abnormal:
GABA neurons in the striatum degenerate
cholinergic interneurons become imbalanced
oxidative stress may damage neurons
These changes further destabilize motor control.
9. Why It Is “Tardive”
It is delayed because the receptor changes take months or years to develop.
Timeline:
Chronic dopamine blockade
↓
Gradual receptor upregulation
↓
Supersensitivity
↓
Dyskinesia appears10. Summary of the Mechanism
The central mechanism is dopamine receptor supersensitivity in the basal ganglia.
Long-term D₂ receptor blockade
↓
Receptor upregulation
↓
Hypersensitive dopamine signaling
↓
Excess motor output
↓
Tardive dyskinesiaResting Tremor
Resting: inactivity
Tremor: to shake
So resting tremor literally means “shaking that occurs when the body part is at rest.”
2. Definition
A resting tremor is a rhythmic shaking that appears when a muscle is relaxed and not actively being used.
Key characteristics:
occurs when the limb is at rest
decreases or disappears during voluntary movement
often returns when movement stops
Example:
A patient’s hand shakes when resting in their lap but stops when they reach for an object.
3. Classic Clinical Association
Resting tremor is most strongly associated with
Parkinson's disease.
Typical description:
“Pill-rolling tremor”
The thumb and fingers move as if rolling a pill or small object.
Frequency:
about 4–6 Hz
4. Brain Structures Involved
Resting tremor arises from dysfunction of the basal ganglia motor circuits.
Important structures include:
substantia nigra pars compacta
striatum (caudate + putamen)
globus pallidus
thalamus
motor cortex
The critical structure is the substantia nigra, which produces dopamine.
5. Normal Dopamine Function
The substantia nigra sends dopamine to the striatum through the nigrostriatal pathway.
Dopamine regulates two pathways:
Direct pathway
Facilitates movement.
Indirect pathway
Suppresses movement.
Dopamine normally:
stimulates the direct pathway
inhibits the indirect pathway
This produces smooth controlled movement.
6. What Happens in Resting Tremor
In Parkinsonian tremor:
dopamine-producing neurons in the substantia nigra degenerate
Result:
Dopamine levels fall
↓
Indirect pathway becomes overactive
↓
Thalamus is excessively inhibited
↓
Motor signals become unstable
This instability produces oscillatory signals in motor circuits.
7. Oscillatory Circuit Formation
The tremor arises from rhythmic activity in a loop involving:
Basal ganglia
↓
Thalamus
↓
Motor cortex
↓
MusclesBecause dopamine regulation is lost, the circuit becomes unstable and oscillates rhythmically, producing tremor.
8. Why Tremor Appears at Rest
During voluntary movement, the motor cortex and cerebellum strongly activate movement pathways, which temporarily suppress the abnormal oscillations.
When the limb is relaxed:
Basal ganglia oscillations dominate
↓
Tremor appearsThis is why the tremor is called resting tremor.
9. Why the Hands Are Commonly Affected
The basal ganglia have strong representation for fine motor control of the hands and fingers.
Because these circuits are highly active, they are particularly sensitive to dopamine imbalance.
Thus tremor is often seen in:
hands
fingers
jaw
lips
10. Summary of the Mechanism
Resting tremor occurs due to dopamine deficiency in basal ganglia circuits.
Mechanism:
Degeneration of substantia nigra neurons
↓
Reduced dopamine in striatum
↓
Basal ganglia circuit imbalance
↓
Rhythmic oscillatory activity
↓
Resting tremor✅ Key Concept
Resting tremor results from dopamine loss in the basal ganglia, which destabilizes motor control circuits and produces rhythmic oscillations that appear when the muscles are at rest.
Action Tremor 1. Etymology
Action
Latin actio = a doing, performing, or movement
Tremor
Latin tremere = to shake or quiver
So action tremor literally means “shaking that occurs during movement.”
2. Definition
Action tremor is a tremor that occurs when a muscle is voluntarily activated, such as when:
holding the arms out
writing
reaching for an object
drinking from a cup
It appears during movement and usually disappears at rest.
This contrasts with resting tremor, which occurs when the muscle is relaxed.
3. Main Brain Structures Involved
Action tremor is usually caused by dysfunction in the cerebellum or cerebellar circuits.
Important structures include:
cerebellum
dentate nucleus
red nucleus
thalamus
motor cortex
These structures form the cerebellar motor coordination loop.
4. Normal Cerebellar Function
The cerebellum acts as the brain’s movement coordinator.
It compares:
intended movement (from the motor cortex)
actual movement (from sensory feedback)
It then sends corrections to smooth the motion.
Normal circuit:
Motor cortex → movement command
↓
Cerebellum monitors movement
↓
Cerebellum corrects errors
↓
Smooth coordinated motion
5. What Goes Wrong in Action Tremor
When the cerebellum or its output pathways are damaged, the brain cannot properly fine-tune movements.
This leads to oscillating corrections.
Mechanism:
Movement begins
↓
Error detected
↓
Correction overshoots
↓
Opposite correction occurs
↓
Repeated oscillation
This oscillation produces rhythmic shaking during movement.
6. Types of Action Tremor
Action tremor includes several subtypes.
Postural tremor
Occurs when maintaining a position against gravity.
Example:
holding arms outstretched.
Common in
Essential tremor.
Kinetic tremor
Occurs during voluntary movement.
Example:
writing or drinking.
Intention tremor
Occurs when approaching a target.
Example:
finger-to-nose test.
The tremor gets worse near the target.
Typical cause:
cerebellar lesions
7. Classic Cause: Essential Tremor
The most common cause of action tremor is
Essential tremor.
Features:
postural and kinetic tremor
hands and arms most affected
improves with alcohol
often familiar
It likely involves abnormal oscillations in the cerebellothalamic circuit.
8. Other Causes
Action tremor may also occur in:
cerebellar stroke
multiple sclerosis
brain tumors
alcohol withdrawal
hyperthyroidism
medication side effects
9. Why the Tremor Is Rhythmic
The tremor becomes rhythmic because motor control circuits form feedback loops.
If the cerebellar correction system is unstable:
Movement error
↓
Overcorrection
↓
Opposite error
↓
Repeated oscillation
This creates a regular shaking pattern.
10. Summary
Action tremor mechanism
Voluntary movement begins
Cerebellar coordination system is impaired
Movement corrections overshoot
Oscillating corrections occur
Rhythmic tremor appears during movement
this will be the written portion of the exam.
reflexes
-this will be on your quiz.
memorize.
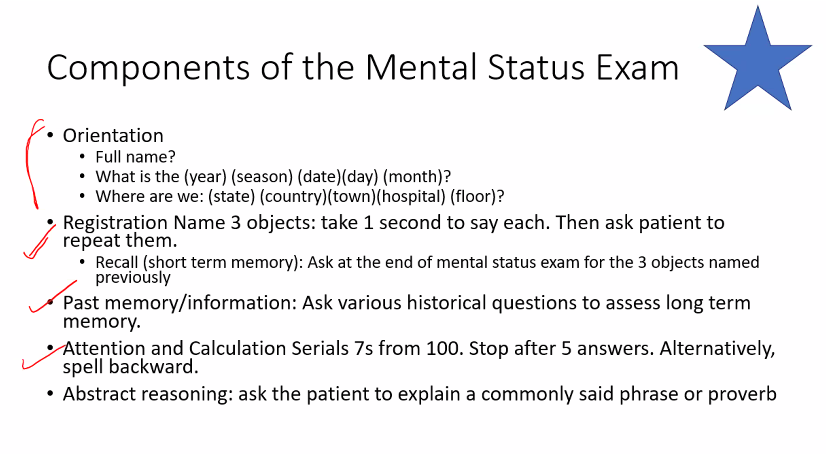
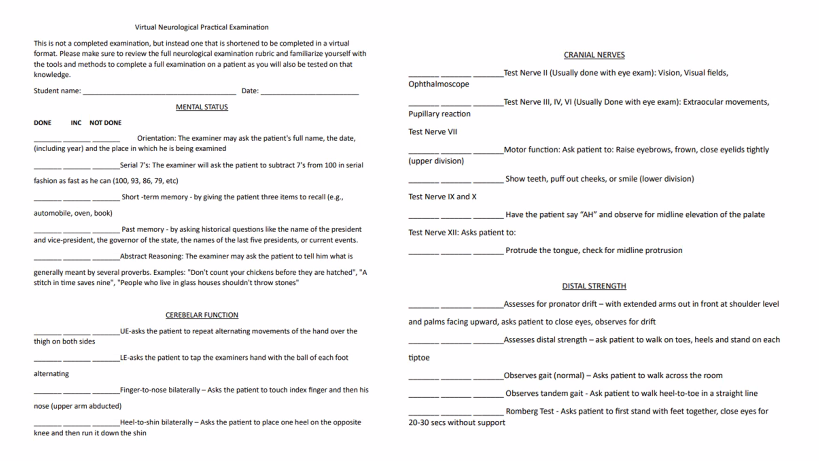
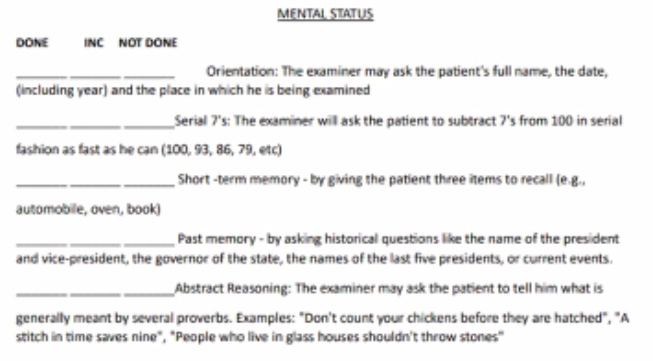
mental status
Orientation: examiner may ask the patients full name, the date (including the year), and the place in which he is being examined.
serial 7s: the examiner will ask the patient to subtract 7s from 100 in serial fashion as fast as he can (100, 93, 86, 79, etc.)
short term memory: by giving the patient three items to recall (eg. automobile, oven, book).
past memory: by asking historical questions like the name of the president and vice president, the governor of the state, the names of the last presidents, or current events
abstract reasoning: the examiner may ask the patient to tell him what is generally meant by several proverbs Examples: “Don’t count your children’s chickens before they’ve hatched".” “A stitch in time saves nine”, “People who live in glass houses shouldn’t throw bricks”.
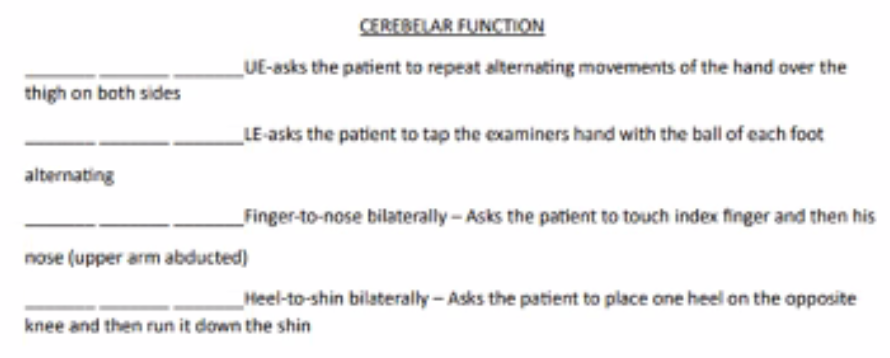
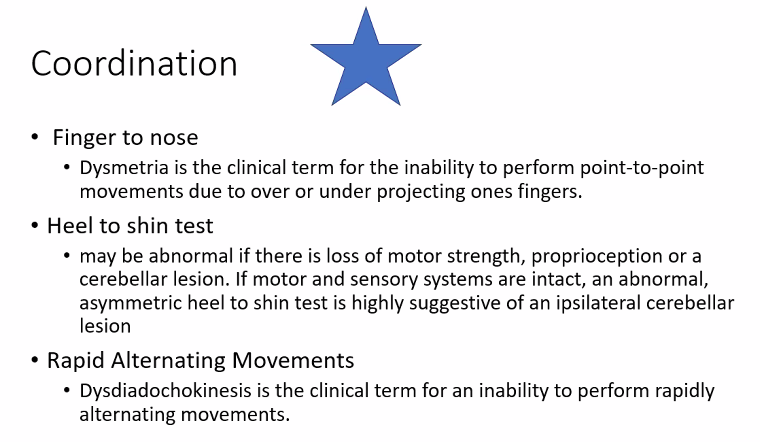
cerebellar function
UE asks the patient to repeat alternating movements of the hand over the thigh on both sides
LE asks the patient to tap the examiners hand with the ball of each foot alternating
Finger to nose bilaterally: asks the patient to touch the index finger and then his nose (upper arm abducted)
Heel to shin bilaterally: asks the patient to place one heel on the opposite knee and then run it down the shin.
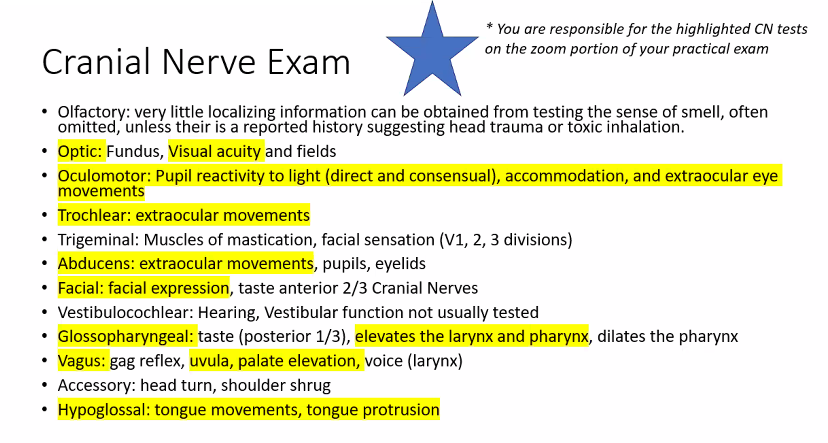
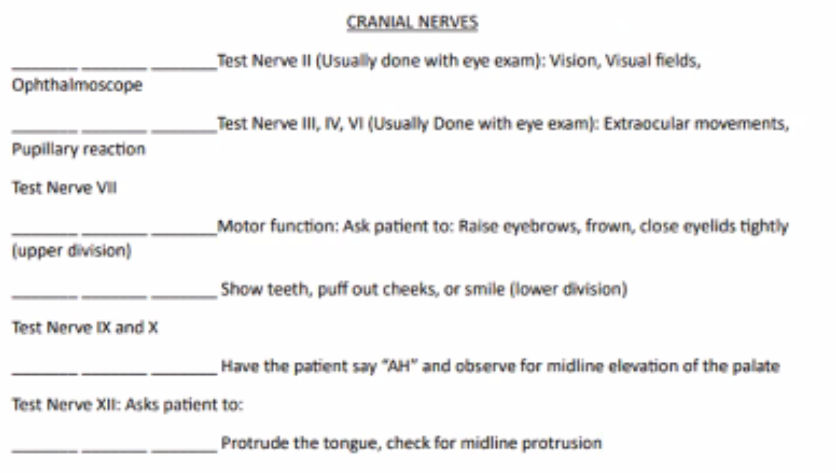
cranial nerves
test nerve II: (usually done with eye exam): vision, visual fields, Opthalmoscope
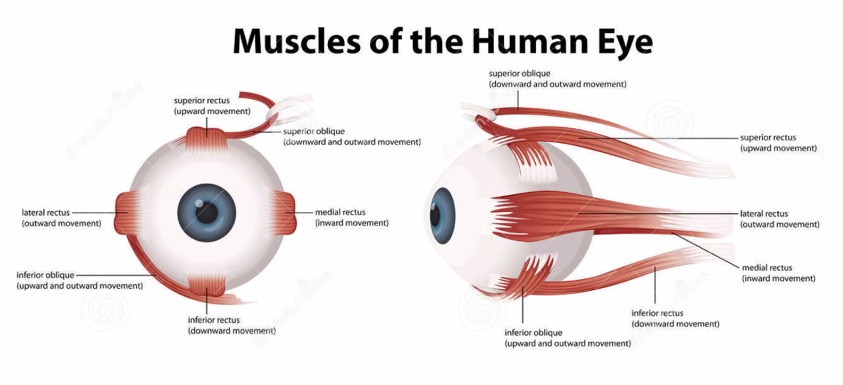
test nerve III, IV, VI: (usually done with eye exam): extraocular movements, pupillary reaction
test nerve VII: motor function: ask patient to: raise eyebrows, frown, close eyelids tightly (upper division)
(still nerve VII) show teeth, puff out cheeks, or smile (lower division)
test nerve IX and X: have the patient say “AH” and observe for midline elevation of the palate
test nerve XII: protrude the tongue, check for midline protrusion.
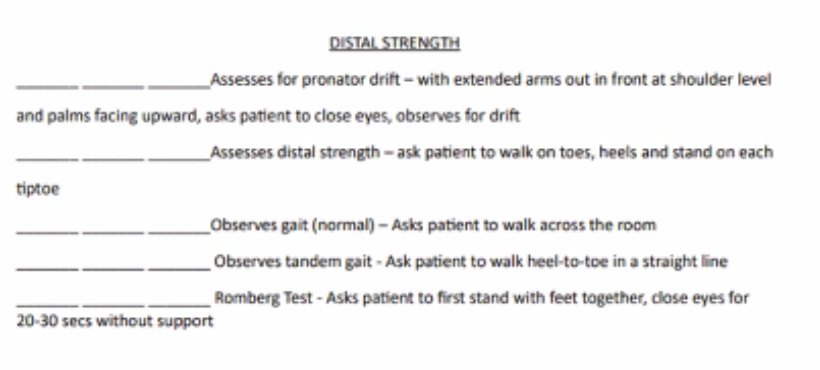
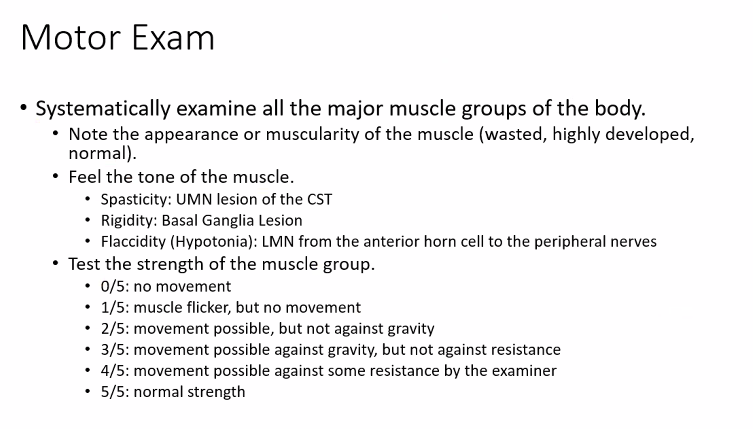
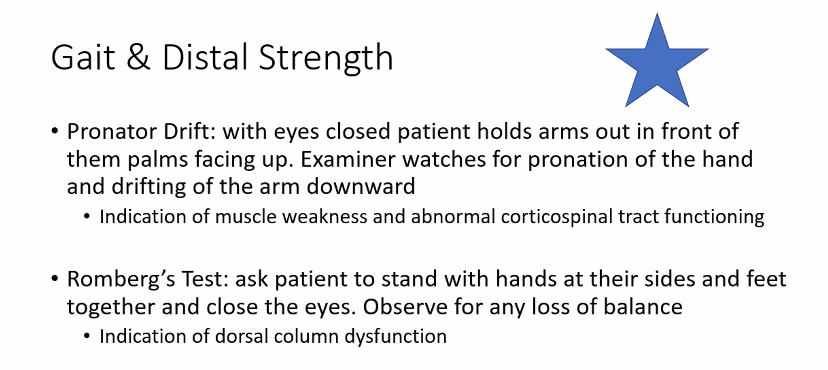
distal strength
assess for pronator drift- with extended arms out in front at shoulder level and palms facing upward, asks patient to close eyes, observes for drift
assess for distal strength: ask patient to walk on toes, heels, and stand on each tippy toe
observe gait (normal): asks patient to walk across the room
observes tandem gait: ask patient to wall heel -to-toe in a straight line
Romberg test: asks patient to first stand with feet together, close eyes with 20-30 secs without support.
romberg test for distal strength
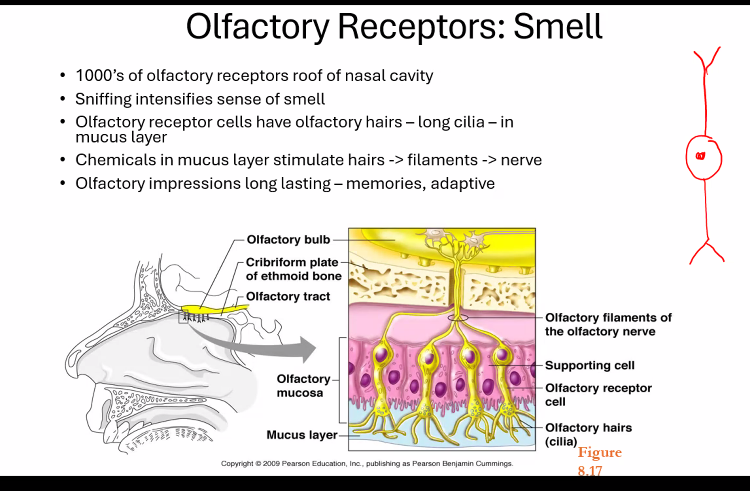
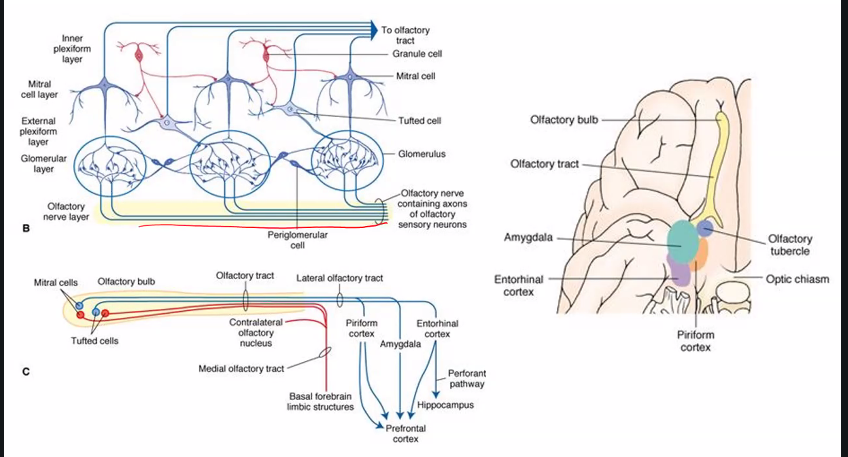
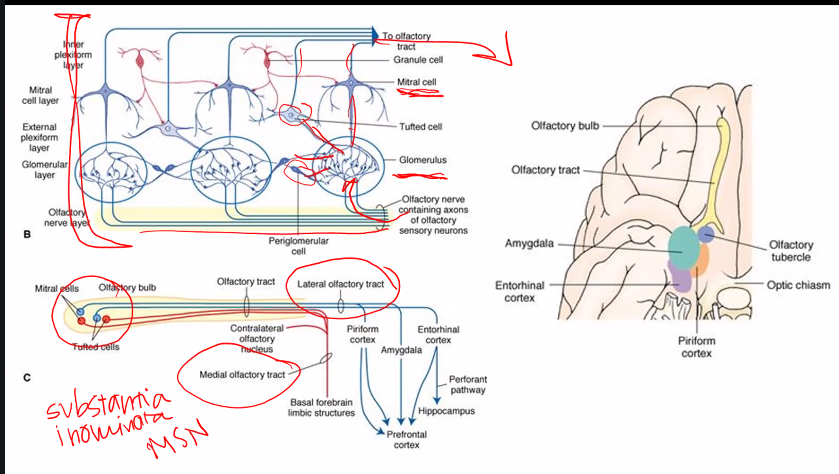
amygdala has to do with fears, especially learned responses to fears.
hallucination: parahippocampal uncus
amygdala: fear, lesion in amygdala results in loss of fear
why is parahippocampal uncus the correct answer?
This question is describing olfactory hallucinations (also called phantosmia) that are:
sudden
brief
episodic
This is classic for temporal lobe (uncinate) seizures.
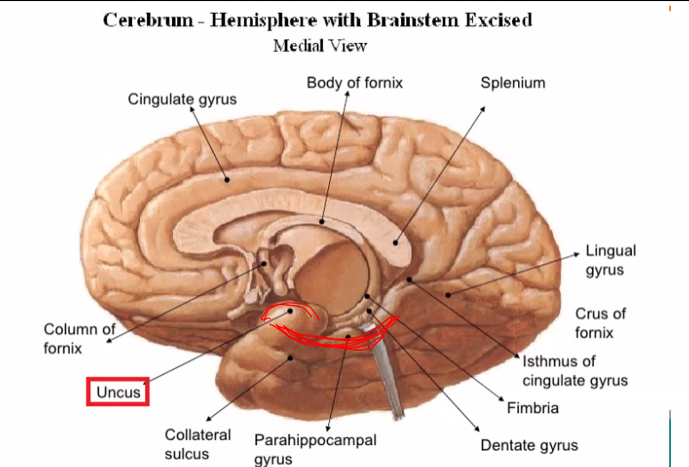
Parahippocampal Uncus Definition
The uncus is the medial, anterior part of the parahippocampal gyrus in the temporal lobe, and it contains part of the primary olfactory cortex (piriform cortex + amygdala connections).
Uncus = Latin for “hook”
→ hook-shaped structure
C)
A) and B)

B)
A)

A)
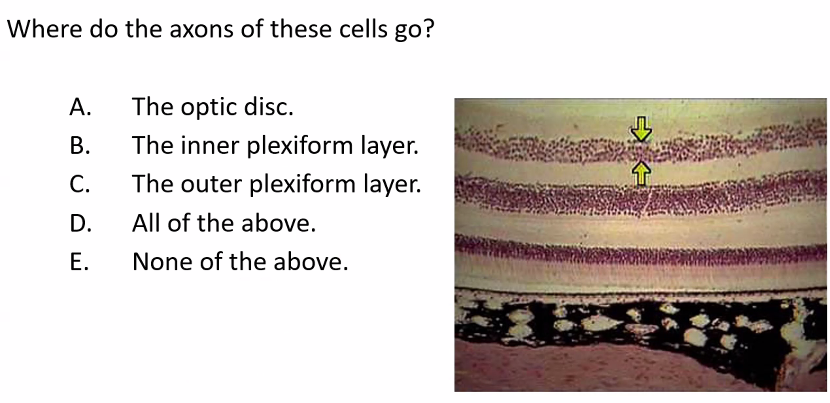
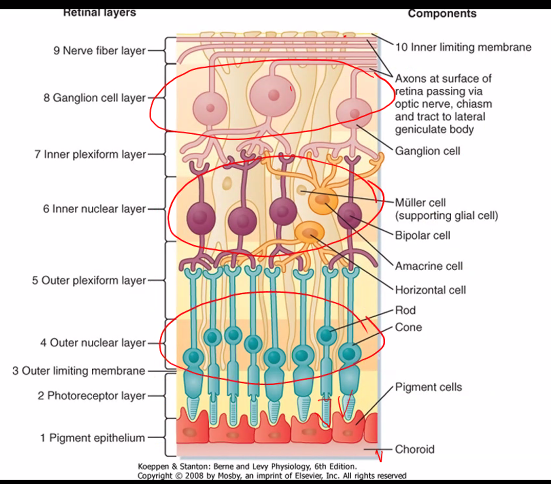
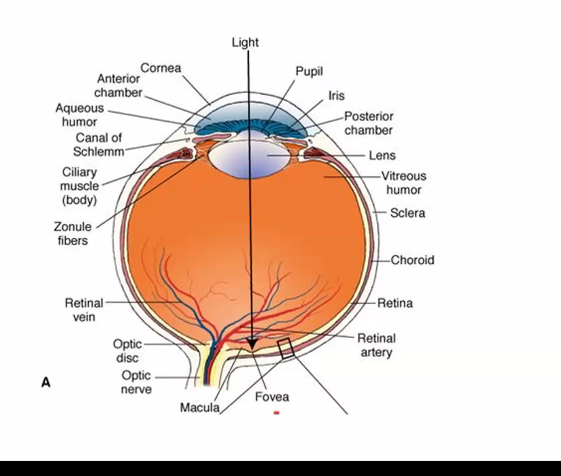
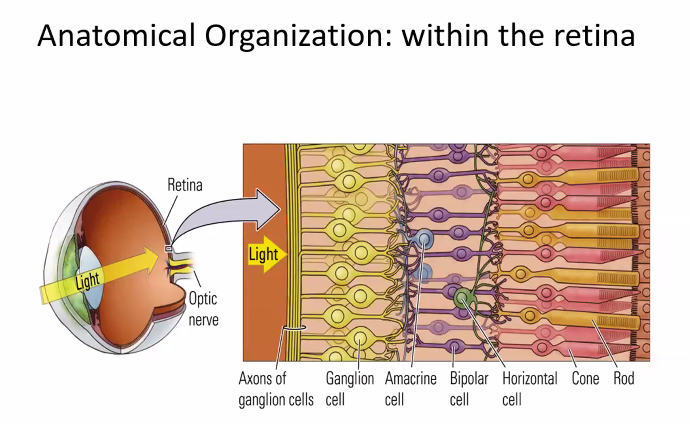
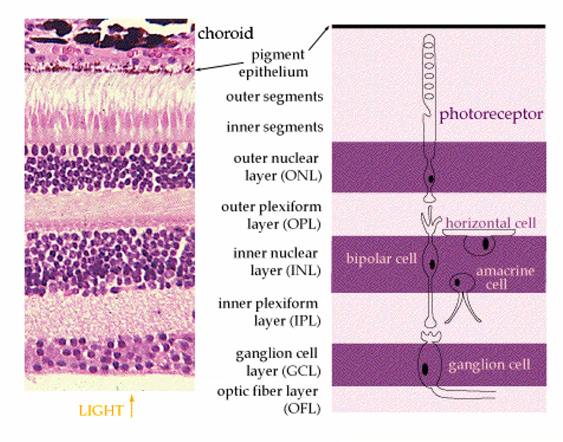
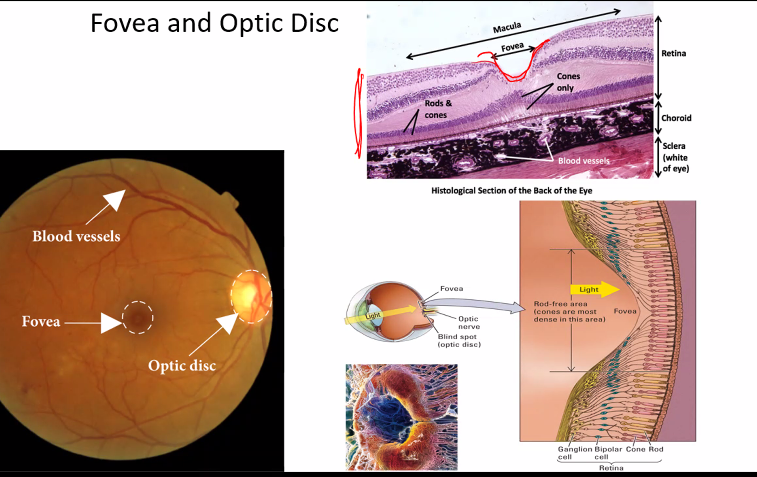
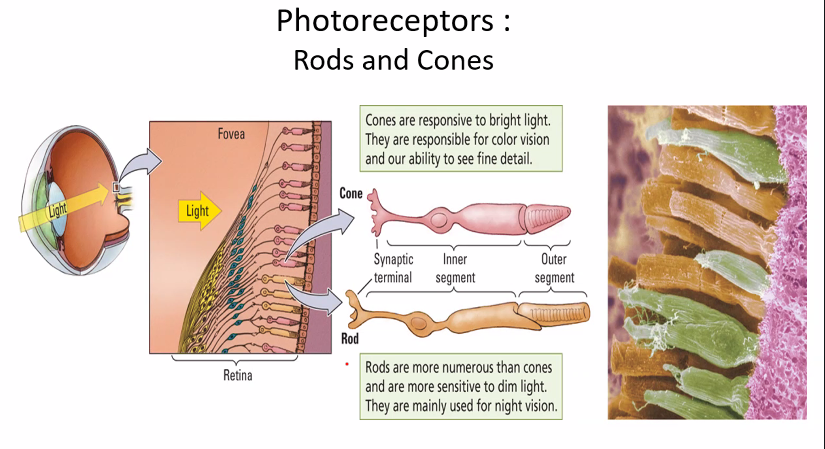
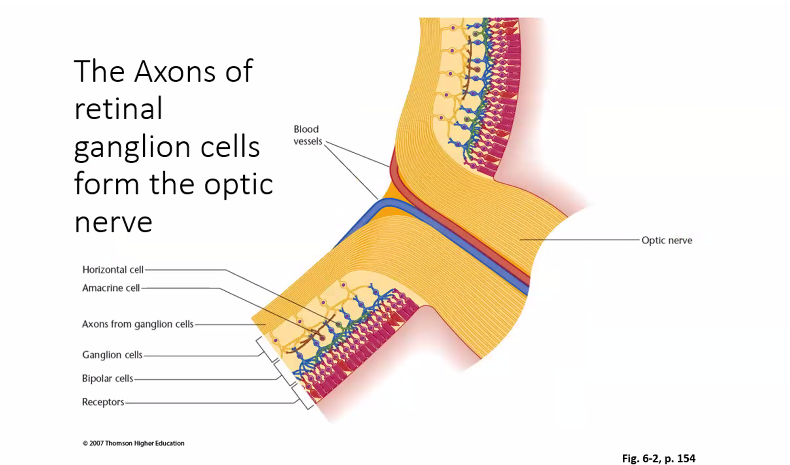
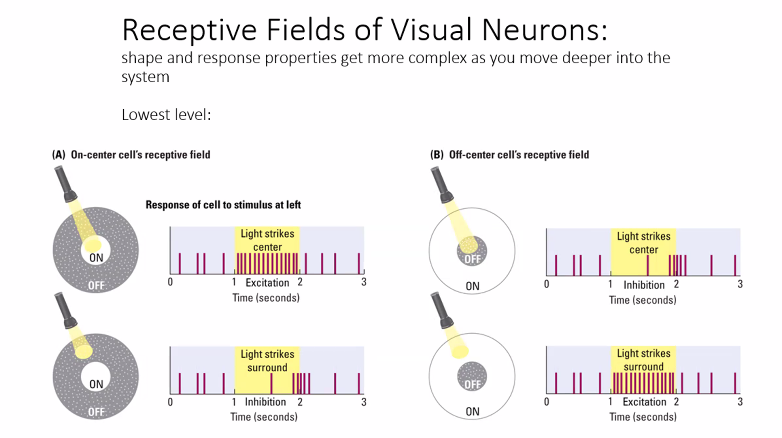
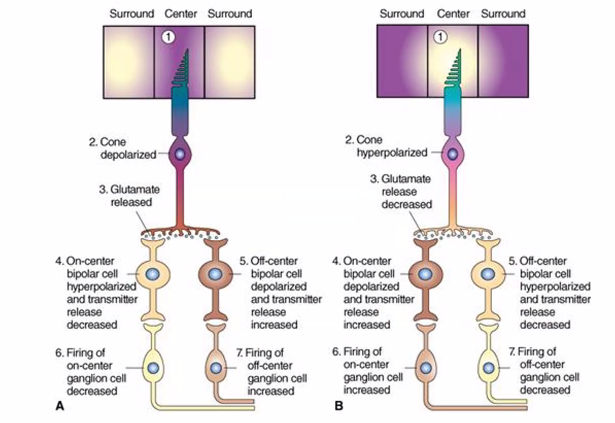
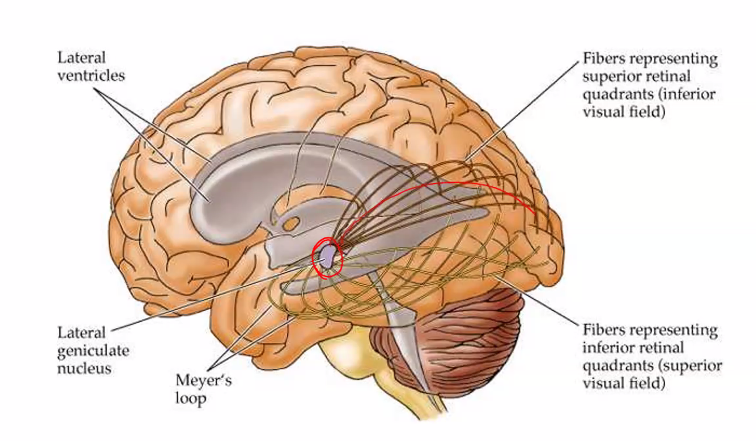
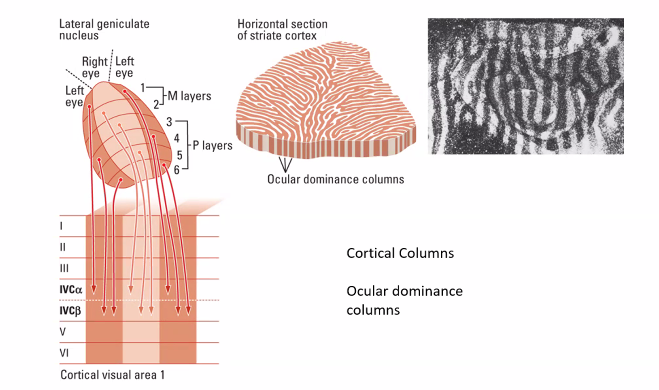
on the next exam, she will show you an image of the retina cells.
D)
D)
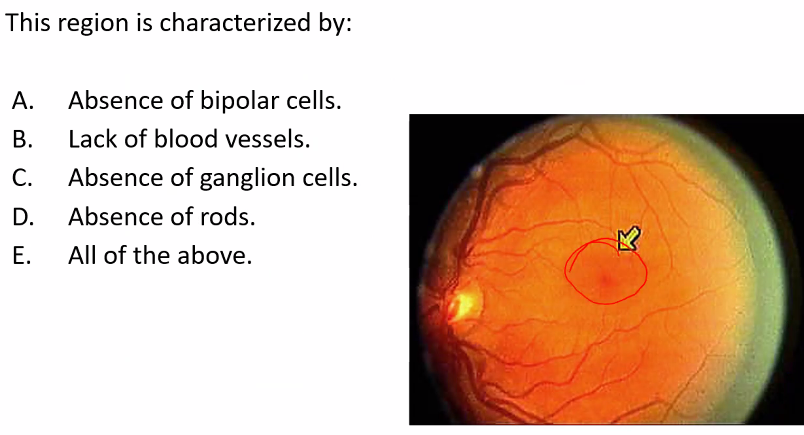
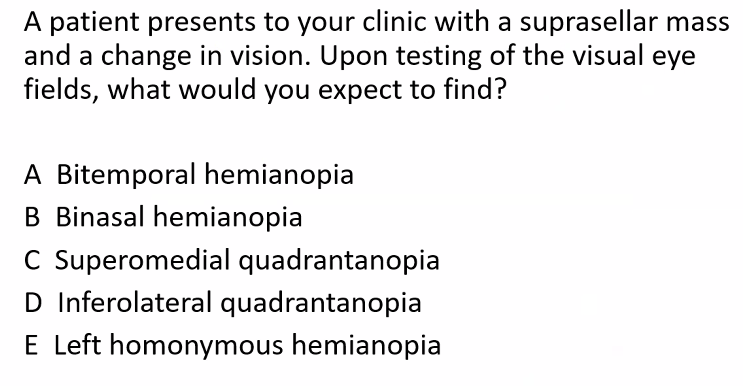
A)
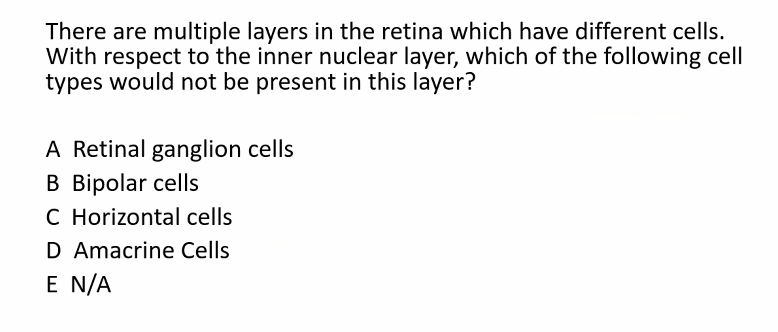
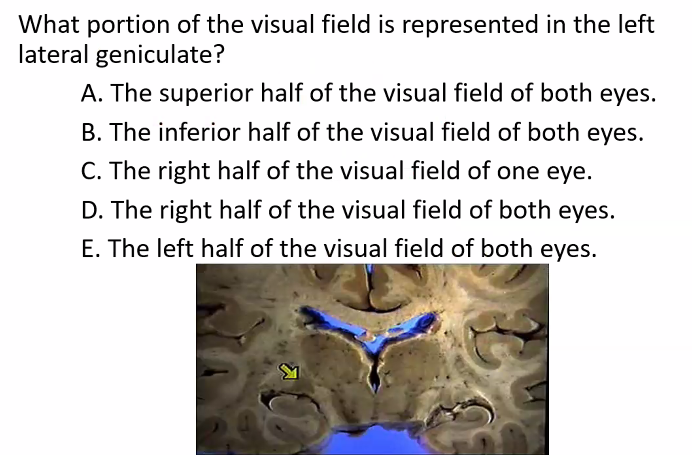
B is correct.
ignore, C D and E because those are also not true.
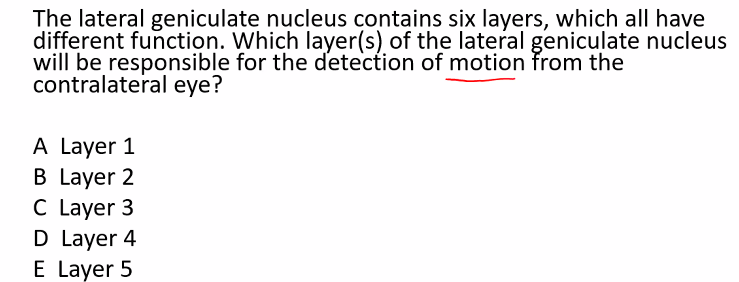
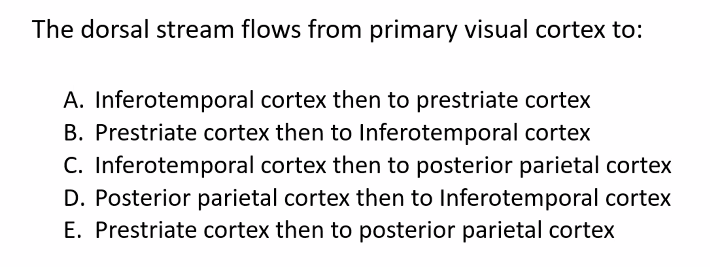
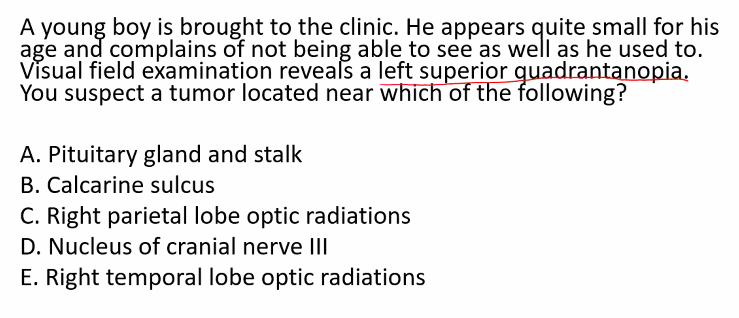
E)
C)

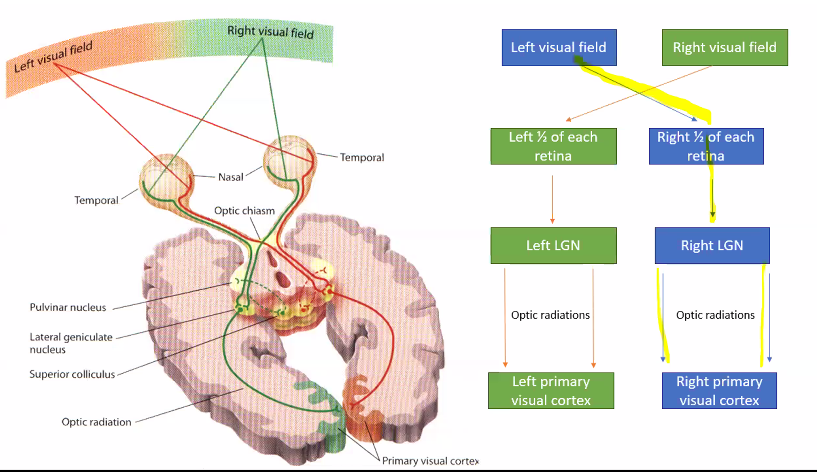
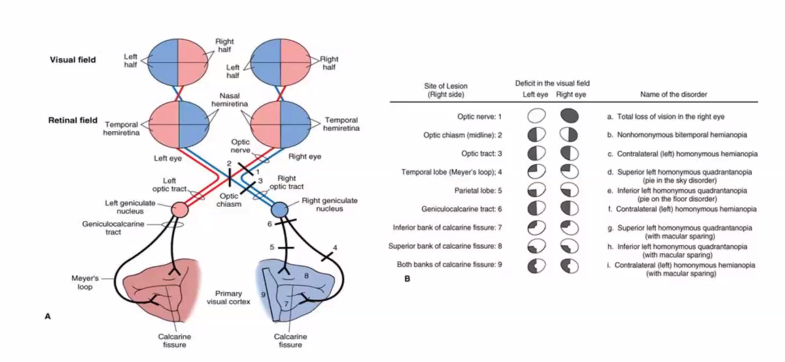
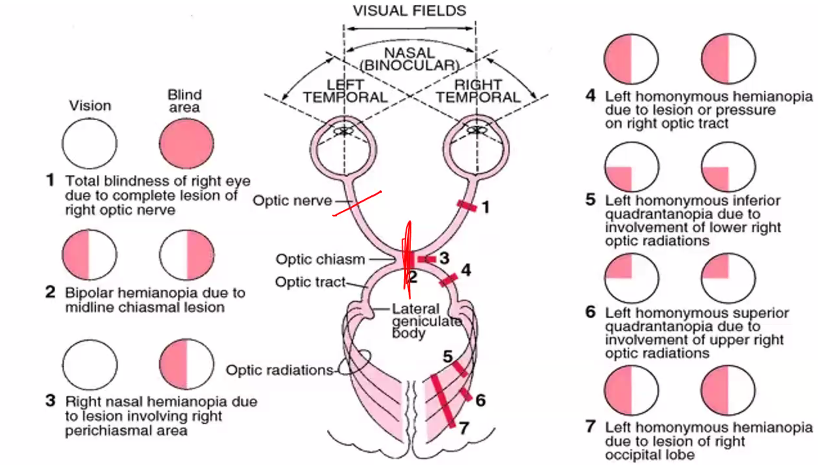
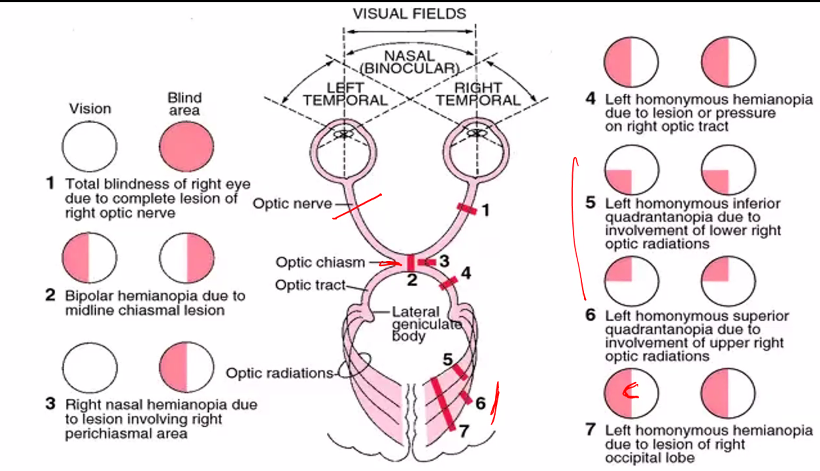
SHE WILL ASK YOU ABOUT LESIONS IN ANYONE OF THESE DIFFERENT REGIONS.
LESIONS WILL GIVE YOU A VERY SPECIFIC DEFICIT IN THIS VISUAL FIELD.
B)
C)
D)
C)
A)
E)
A)
it’s in the book.
E)
C)
C)
B)
B)
C)
C)
B)
D)
C)
B)
C)
C)
B)
B)
A)
C)
B)
A)
C)
I think you missed a question.
C)
B)
B)