C) Disorders of lung
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
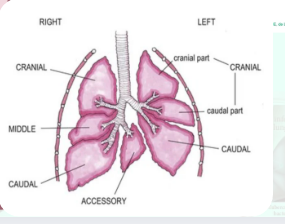
cranial lobe
caudal lobe
In all domestic species, the left
lung consists of:
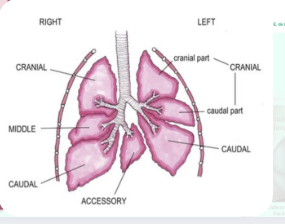
cranial lobe
middle lobe
caudal lobe
accessory lobe
The right lung usually contains:
Type I: (cattle, sheep, goat, pig)
Extremely well developed secondary lobules , marked interlobular septa and thick pleura
Type II: (monkey, dog, cat)
absence of secondary lobules, ill-defined parenchymal supportive tissue strands, with thin membranous pleura
Type III: (horse and humans)
developed secondary lobules, wel defined but hephazzardly arranged interlobular septa, and with thick vascular pleura
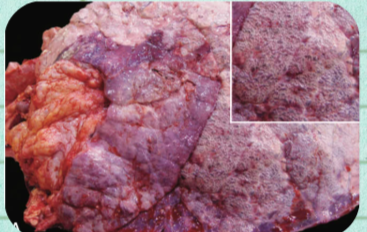
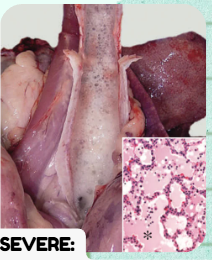
CONGENITAL MELANOSIS
What congenital lung anomaly is a common incidental finding seen at slaughter in pigs and ruminants, presenting as multifocal flat black spots across the parenchyma?
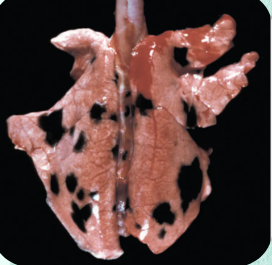
pigs, ruminants, and "black-face" breeds, especially sheep
CONGENITAL MELANOSIS
In which specific livestock categories and selective sheep breeds is Congenital Melanosis most commonly encountered?
No clinical significance, and the texture of pigmented lungs remains unchanged.
CONGENITAL MELANOSIS
What is the clinical significance of Congenital Melanosis, and what happens to the physical tissue texture of the pigmented areas?
black spots, often a few centimeters in diameter
CONGENITAL MELANOSIS
Describe the gross physical appearance and size of the lesions characterizing Congenital Melanosis:
1. meninges
2. intima of the aorta
3. caruncles of the uterus
CONGENITAL MELANOSIS
Beyond the main site of the lungs, list the 3 other specific anatomical organs/structures where these congenital black spots are mainly seen:
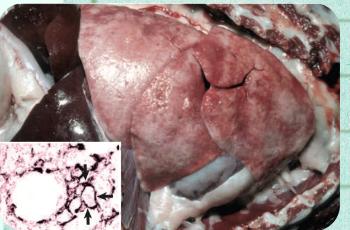
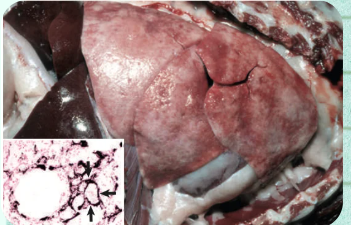
PULMONARY CALCIFICATION (CALCINOSIS)
What metabolic lung disorder can result from hypercalcemic states or chronic diseases, causing the tissue to develop a "gritty" texture and fail to collapse when the thoracic cavity is opened?
Hypervitaminosis D
PULMONARY CALCIFICATION (CALCINOSIS)
Hypercalcemic states driving pulmonary calcification often result from what nutritional/toxicological condition?
Solanum malacoxylon containing vitamin D analogs
PULMONARY CALCIFICATION (CALCINOSIS)
Ingesting what specific toxic plant can lead to pulmonary calcinosis, and what active compounds does it contain?
uremia and hyperadrenocorticism
PULMONARY CALCIFICATION (CALCINOSIS)
Beyond primary toxicosis, pulmonary calcification is commonly seen following which two specific metabolic/endocrine conditions in dogs?
pulmonary necrosis
PULMONARY CALCIFICATION (CALCINOSIS)
What localized tissue event can lead to pulmonary calcification across various animal species?
exhibit a "gritty" texture
fail to collapse when the thoracic cavity is opened
PULMONARY CALCIFICATION (CALCINOSIS)
List the two classic tactile and structural behaviors of affected lungs during a post-mortem exam:
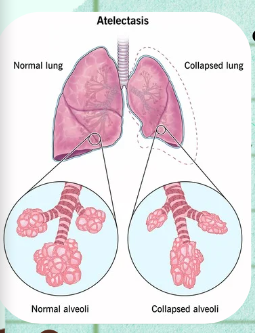
ATELECTASIS
Incomplete expansion of alveoli, typically describing the lungs.
CONGENITAL/NEONATAL ATELECTASIS
Lungs that did not expand with air at birth.
ACQUIRED ATELECTASIS OR ALVEOLAR COLLAPSE
Lungs that have collapsed after initially inflating.
gaseous exchange
a balanced ratio of the volumes of air to
capillary blood must be present in the
lungs (ventilation/perfusion ratio), and
the air and capillary blood must be in
close proximity across the alveolar
wall.
A ventilation-perfusion mismatch occurs if pulmonary tissue is either collapsed (atelectasis) or overinflated (hyperinflation and emphysema)
A ventilation-perfusion mismatch occurs if pulmonary tissue is either collapsed (_______) or overinflated (hyperinflation and _______)
ATELECTASIS (CONGENITAL AND ACQUIRED)
What lung expansion disturbance category includes both congenital and acquired forms, representing incomplete expansion or collapse of pulmonary parenchyma?
A mosaic pattern of normally inflated (lighter) and atelectatic (darker) lobules.
In multifocal neonatal atelectasis, what specific visual layout is formed by the contrasting lung zones? Describe which zones are lighter and which are darker.
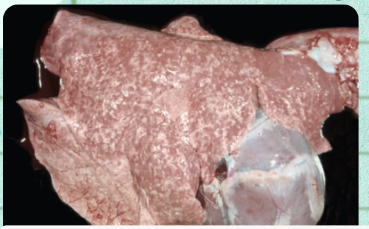
amniotic fluid, meconium, and squamous epithelial cells
ATELECTASIS (CONGENITAL AND ACQUIRED)
Neonatal airway obstruction leading to this mosaic pattern of atelectasis is typically caused by the aspiration of which three specific components?
small bronchi and bronchioles
ATELECTASIS (CONGENITAL AND ACQUIRED)
Aspiration of amniotic fluid, meconium, and squamous epithelial cells causes obstruction in which specific levels of the respiratory tree?
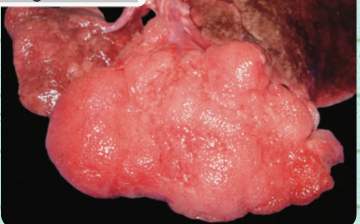
PULMONARY EMPHYSEMA
a congenital dog shows severe distention in the left cranial lobe
The affected lung exhibits notable crepitus upon palpation
crepiptus
palpable or audible grating or crunching sensation
Acquired Compressive Atelectasis
Acquired Obstructive Atelectasis
ATELECTASIS (CONGENITAL AND ACQUIRED)
2 types
Lung tissue is compressed from outside, preventing normal expansion; caused by pleural masses, fluid, gas, or pressure from adjacent organs.
Define Acquired Compressive Atelectasis based on its primary mechanism and listing the general physical causes acting from the outside:
Abscesses and Tumors
Acquired Compressive Atelectasis
List the two specific types of space-occupying lesions in the pleural cavity that cause compressive atelectasis:
Bloat
Hydrothorax
Hemothorax
Chylothorax
Empyema
Acquired Compressive Atelectasis
List the 5 clinical conditions that cause compressive atelectasis via increased pressure transferred to the lungs:
Pneumothorax; when caused by pneumothorax, the atelectasis is often massive and is commonly called lung collapse.
Acquired Compressive Atelectasis
what specific event causes a loss of negative pressure in the thoracic cavity, what is its diagnostic name, and what is this massive atelectasis commonly called?
Airway is narrowed or blocked, preventing air from reaching alveoli; caused by mucus plugs, exudate, foreign material, or lungworms.
Define Acquired Obstructive Atelectasis based on its mechanical mechanism and its primary physiological consequence:

Mucosal edema and Inflammation
Acquired Obstructive Atelectasis
List the two localized pathogenic mechanisms that cause Airway narrowing:
Mucus plugs
Exudate
Aspirated foreign material
Lungworms
Acquired Obstructive Atelectasis
List the 4 distinct physical/parasitic entities that cause direct mechanical Airway obstruction:
PULMONARY EMPHYSEMA
What inflation disturbance is defined as a marked overdistention of alveoli with destruction of supporting alveolar and interstitial structures?
airway obstruction and air trapping
PULMONARY EMPHYSEMA
Pulmonary emphysema is commonly secondary to other respiratory conditions, especially diseases that cause which two mechanical processes?
alveolar emphysema
interstitial emphysema
PULMONARY EMPHYSEMA
2 categories
Distention and rupture of alveolar walls, forming variably sized air spaces in the pulmonary parenchyma; occurs in all species.
PULMONARY EMPHYSEMA
Define Alveolar emphysema based on its structural cellular lesions and its species distribution:
Air escapes into the interstitial connective tissue, especially the interlobular septa
PULMONARY EMPHYSEMA
Define Interstitial emphysema based on where the gas anatomically escapes, noting the specific septal structures involved:
cattle
PULMONARY EMPHYSEMA
In which livestock species is Interstitial Emphysema mainly seen due to their distinct lung anatomy?
CIRCULATORY DISTURBANCES
What category of lung pathology involves a breakdown in the organ's highly vascular network, potentially causing secondary systemic failure in the heart and liver?
pulmonary and bronchial arteries
CIRCULATORY DISTURBANCES
The lungs are highly vascularized with dual circulation. What two specific arterial networks supply this system?
hypoxemia and acidosis
CIRCULATORY DISTURBANCES
Disruptions to the pulmonary circulation can rapidly lead to which two life-threatening systemic blood status changes?
Chronic pulmonary disease causing persistent pulmonary hypertension, leading to cardiac dilation and right heart failure.
CIRCULATORY DISTURBANCES
Define cor pulmonale based on its primary trigger mechanism and its downstream effects on cardiac structure:
1. cardiac dilation
2. right heart failure
3. liver congestion (nutmeg liver)
4. generalized edema (anasarca)
CIRCULATORY DISTURBANCES
Persistent pulmonary hypertension from chronic lung disease creates a cascade of systemic failures. List the 4 progressive steps that follow:
nutmeg liver
anasarca
CIRCULATORY DISTURBANCES
Give the specific clinical/pathological terms used on the slide to describe the following secondary effects of cor pulmonale:
Congestion of the liver
Generalized edema
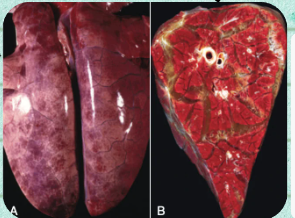
HYPEREMIA AND CONGESTION
What dual circulatory disturbances of the lung involve an increase in blood volume within the pulmonary vasculature, differentiated primarily by active vs. passive mechanisms?
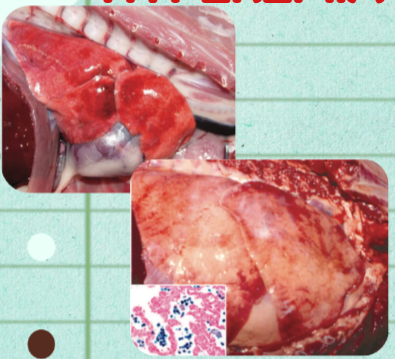
An active response linked to acute inflammation.
HYPEREMIA AND CONGESTION
Define Hyperemia based on its physiologic type of response and its classic clinical association:
A passive result of reduced venous blood flow.
HYPEREMIA AND CONGESTION
Define Congestion based on its physiologic type of response and its primary circulatory cause:
heart failure
HYPEREMIA AND CONGESTION
Pulmonary congestion is most often clinically due to what systemic condition?
blood stagnation in pulmonary vessels
HYPEREMIA AND CONGESTION
Heart failure leads to what mechanical vascular change within the respiratory system's network?
edema and red blood cell leakage into alveolar spaces.
HYPEREMIA AND CONGESTION
Stagnation of blood in the pulmonary vessels downstream of heart failure causes what two structural complications to occur within the lung tissue?
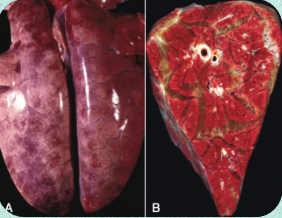
PULMONARY EDEMA
What circulatory disturbance develops when the rate of fluid transudation into the interstitium or alveoli exceeds removal mechanisms, leaving the lungs grossly "wet and heavy"?
lymphatic and alveolar removal
PULMONARY EDEMA
Pulmonary edema develops when the rate of fluid transudation from pulmonary vessels into the interstitium or alveoli exceeds the rate of what two structural clearance pathways?
wet and heavy
PULMONARY EDEMA
What are the two core gross descriptive terms used on the slide to outline an edematous lung?
foamy fluid; generated from the mixing of edema fluid and air
PULMONARY EDEMA
In severe cases of pulmonary edema, what specific fluid type fills the bronchi and trachea, and what mechanical action generates it?
protein-rich edematous fluid admixed with a few inflammatory cells
PULMONARY EDEMA
Under severe states, the alveoli are filled with what type of fluid, and what cellular elements are admixed within it?
rounded edges
PULMONARY EDEMA
According to the text panel on the right, what physical structural change happens to the borders of the lung lobes when they are distended by edema fluid?
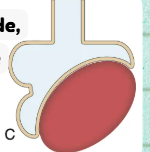
PULMONARY EMBOLISM
What circulatory disturbance refers to both local thrombus formation and the translocation of a clot from the venous circulation into the lungs?
Local: local thrombus formation
Translocation: translocation of a thrombus present elsewhere in the venous circulation
PULMONARY EMBOLISM
Define the two different dynamic origin pathways that lead to a pulmonary embolism as stated on the slide:
Fragments released inevitably reach the lungs and become trapped in the pulmonary vasculature.
PULMONARY EMBOLISM
What mechanical event happens to these physical fragments once released, and exactly where do they become confined?
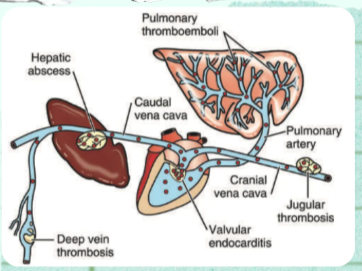
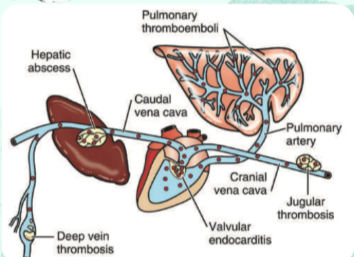
1. Rupture of a hepatic abscess into the caudal vena cava
2. Vegetative valvular endocarditis involving the tricuspid valve
3. Jugular thrombosis
4. Deep vein thrombosis
PULMONARY EMBOLISM
List the 4 specific clinical sources/conditions where pulmonary emboli (represented by red dots on the diagram) originate:
Caudal vena cava
PULMONARY EMBOLISM
Rupture of a hepatic abscess translocates septic material directly into which specific major systemic vein?
Tricuspid valve
PULMONARY EMBOLISM
Vegetative valvular endocarditis generating pulmonary emboli specifically involves which heart valve?
PULMONARY EMBOLISM
What specific secondary vascular entity is detailed here through the clinical consequences of its variable sizes (small sterile vs. large), parasitic agents, and predisposing endocrinopathies?
Because they can be rapidly degraded and disposed of by the fibrinolytic system.
PULMONARY EMBOLISM
Why do small sterile thromboemboli have little clinical or pathologic significance in the lung?
1. small airway constriction
2. reduced surfactant production
3. pulmonary edema
4. atelectasis
PULMONARY EMBOLISM
List the 4 localized intrapulmonary tissue changes caused by larger thromboemboli:
hypoxemia, hyperventilation, and dyspnea
PULMONARY EMBOLISM
These 4 localized tissue changes from large thromboemboli ultimately result in which 3 systemic clinical/respiratory signs?
Dirofilaria immitis
Angiostrongylus vasorum
PULMONARY EMBOLISM
Name the two specific genus and species of parasites highlighted as causative agents for pulmonary embolism:
Organ pathology: glomerulopathies
System status: hypercoaguable states
PULMONARY EMBOLISM
Beyond endocrinopathies, what other broad organ pathology category and system status are named as predisposing systemic causes?

PULMONARY INFARCTS
What circulatory disturbance of the lung parenchyma is generally rare and asymptomatic, but when visible, typically presents as a cone or wedge-shaped lesion at the lung margins?
Rare and asymptomatic
PULMONARY INFARCTS
How are pulmonary infarcts characterized regarding their clinical occurrence frequency and presentation severity?
congestive heart failure and lung lobe torsion
PULMONARY INFARCTS
Pulmonary thrombosis and embolism can worsen compromised circulation under which two specific clinical conditions?
red to black, swollen, firm, and typically cone or wedge-shaped
PULMONARY INFARCTS
List the 4 tactile and color parameters used to describe the gross physical appearance of a pulmonary infarct:
at lung margins
PULMONARY INFARCTS
Where anatomically within the lung lobes are these characteristic cone or wedge-shaped infarct lesions especially located?