MCB topic 5.1
1/30
Earn XP
Description and Tags
Weeks 10-11
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
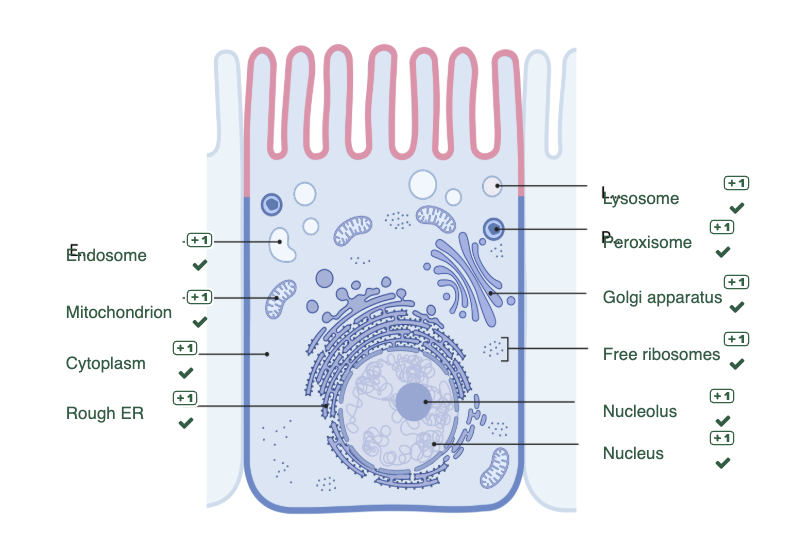
Describe the organelles
The nucleus of the cell contains the genetic material, is the site of DNA transcription and regulates the functions of the cell.
Within the nucleus, the nucleolus is the site of rRNA transcription and processing, and of ribosome assembly. The assembled ribosomes are transported to the cytoplasm. Cytosolic proteins are translated by free ribosomes whereas proteins destined for the cell surface or secretion are translated by ribosomes that form the rough ER. Further protein modification occurs in the golgi apparatus.
Cytosolic proteins are tagged and degraded in the proteosome. The lysosome contains enzymes that can degrade macromolecules including proteins, sugars, nucleic acids, and lipids, and the peroxisome contains oxidative enzymes that can break down long-chain fatty acids.
Material from the extracellular environment is transported by endosomes. The structure of the cell is supported by the cytoskeleton which also plays a role in intracellular transport. The cellular organelles and cell are surrounded by membrane composed of lipid bilayers. The integrity of the inner and outer lipid membranes of the mitochondria is essential to their role in energy generation and the induction of apoptosis. The lipid bilayer of the plasma membrane is asymmetric and composed of phospholipids, cholesterol, and proteins.
Describe the features and functions of tissues and organs
While most cells in the human body are composed of the organelles described above, the organs of our bodies are each composed of specific cell types that contribute to the specific function of the tissue in that organ.
The functional tissues of an organ are referred to as the PARENCHYMA, and it is composed of these unique PARENCHYMAL CELLS.
The cells and extracellular matrix (ECM) that support and give structure to an organ is called the STROMA. The stromal cells include the epithelial cells that define the boundary of the organ, the endothelial cells of the blood vessels that supply oxygen and nutrients to the organ, and the mesenchymal cells (such as fibroblasts) that produce the ECM.
The components of the ECM control the structure of the organ by providing scaffolding and support and define the boundaries of the organ. The components of the ECM control the function of the organ by storing growth factors and providing signalling receptors for cell growth and differentiation.
The ECM is not static and is constantly being remodelled.
What are the features of the ECM?
Basement membrane - a highly organised type of ECM that forms around epithelium, endothelial cells, and smooth muscle cells. It is composed of proteoglycans and collagen.
Interstitial matrix - the amorphous gel that connects the components of the ECM.
Adhesive glycoprotein - connect elements of the ECM together and initiate signalling cascades that affect locomotion, proliferation, and differentiation. E.g., integrin.
Fibrous structural proteins - collagen and elastin provide tensile strength and recoil.
Water-hydrated gels - proteoglycans form water-hydrated cells that give the tissue compressive resistance and lubrication.
Fibroblasts - are mesenchymal cells that are found in the stroma where they make the components of the extracellular matrix and contribute to the repair of injury.
Describe the proliferative capacity of cells in labile, stable, and permanent tissue
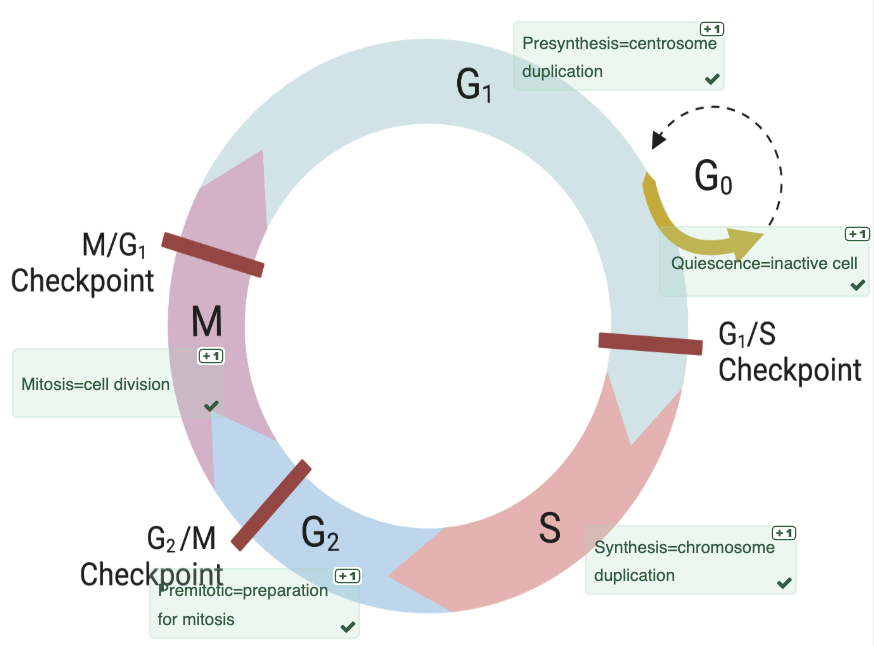
Tissue homeostasis and growth is maintained by a balance between cell proliferation (mitosis) and cell death (apoptosis).
Cell proliferation is determined by:
Growth factors that promote cell cycle entry, relieve blocks in cell cycle arrest, prevents apoptosis, and enhances biosynthesis.
Extracellular matrix that displays growth factors and signalling receptors.
Cyclins that regulate the activity of cell cycle activators (cyclin dependent kinases) and inhibitors (cyclin dependent inhibitors).
Labile tissue?
composed of cells that are continuously lost and replaced by either proliferation of mature cells or stem cells. Labile cells include most hematopoietic and epithelial cells.
Stable tissue?
composed of quiescent cells that have left the cell cycle (G0). These cells have limited proliferative capacity but can enter the cell cycle and proliferative in response growth factors (for example following injury). Stable cells include the parenchyma of most solid organs (liver, kidney, pancreas) and endothelial cells, fibroblasts, and smooth muscle cells.
Permanent tissue?
composed of terminally differentiated cells that have left the cell cycle (G0) and cannot re-enter the cell cycle and have limited stem cell reserves. Permanent cells include neurons, cardiac muscle cells and skeletal muscle cells.
Understand the principles of histological stains and recognise the features of structures visualised with H&E stain
Morphology = macroscopic (gross) or microscopic appearance of cells and tissue. Most cells are transparent so staining procedures are used to make cells more visible.
Haematoxylin and Eosin or H&E is the most commonly used histological stain.
Haematoxylin is considered a basic dye. It is used to stain acidic (or basophilic) structures a purplish blue. Haematoxylin stains nucleic acids (DNA in nucleus, RNA in ribosomes, and RER). It is the nucleic acids in the nucleus of the heart tissue cells that are stained PURPLE.
Eosin is an acidic dye. It stains basic (or acidophilic) structures red or pink (also sometimes termed 'eosinophilic'). Eosin stains most proteins. It is the proteins in the cytoplasm of the heart tissue cells that are stained PINK.
Important terms: etiology, pathogenesis, pathology, clinical manifestations, complications, prognosis, and epidemiology
Etiology: the cause of disease.
Pathogenesis: the mechanism causing disease.
Pathology: molecular and morphologic changes to cells or tissues.
Clinical manifestations: signs and symptoms.
Complications: the secondary, systemic, or remote consequences of disease.
Prognosis: the anticipated course of disease.
Epidemiology: incidence, prevalence, and distribution.
E.g., smoking > genetic alterations > tumour > breathless > metastasis > death/remission > risk.
Adaptation - hypertrophy, atrophy, hyperplasia and metaplasia
Adaptation: A response to stress or increased demand that maintains the cells functions by a new steady state.
Types of adaptation: physiological adaptation-cellular response to normal stimulation - hormones and endogenous chemicals.
Pathological adaptation-cellular response to stimulation secondary to underlying disease/to avoid injury by modulation of structure and/or function.
TERMS:
Hypertrophy: increase cell size and organ size. Increased work load = physiological (body builder) and pathological (hypertension) stimuli. No new cells, just larger cells. Non-dividing cells increase in size (myocytes, skeletal muscle). Increased amount of structural proteins and organelles.
Hyperplasia: increase cell number and organ size. Only in cell populations capable of dividing. Physiological (hormonal response during puberty) and pathological response (chronic stress - callous).
Atrophy: decrease cell size/number and organ size. Physiological atrophy is common during normal development (embryonic structures, uterus following pregnancy), and pathological atrophy depends on the underlying cause. E.g., decreased workload, loss of innervation, loss of blood supply, inadequate nutrition.
Metaplasia: change in cell type. Cells sensitive to stress replaced by a cell type is better able to withstand stress. E.g., stem cell reprogramming. Cigarette smoking: ciliated columnar -> stratified squamous.
*ALL reversible if stimulus is removed.
Reversible/sublethal injury: a response to stimuli that compromises cellular function.
Irreversible injury/lethal injury: a response to stimuli that compromises cellular function to the point that it cannot recover.
Adaptation examples - heart, puberty, and smoking
The heart is a permanent tissue where the parenchyma is composed of terminally differentiated cardiac (heart) muscle cells (cardiomyocytes). In response to increased workload associated with hypertension (an underlying disease typically caused by atherosclerosis) the adaptation would be best described as pathologic hypertrophy.
During puberty, replication of glandular epithelial cells of the female breast is an example of physiologic hyperplasia in response to hormones. The reduction in the size of a limb following immobilisation is best described as atrophy, which is a reduction in the size of an organ by a reduction in the size and / or number of cells in response to reduced workload.
In a smoker, the replacement of ciliated epithelial cells by stratified squamous epithelial cells that are able to withstand the stress from the harmful chemicals in tobacco smoke, is an example of metaplasia. In response to stress, adaptation is a reversible response that maintains cellular homeostasis without compromising the function of the cell.
Injury
Injury is caused by an injury-inducing stimulus, described as the aetiology of a disease.
Hypoxia: oxygen deficiency. Interferes with aerobic oxidative respiration, and can arise from:
Pneumonia = inadequate oxygenation.
Blood loss anaemia.
Carbon monoxide poisoning.
Ischemia = loss of blood supply to tissue.
Chemical agents: poisons, tobacco, alcohol, environmental agents (pollution, lead, mercury), therapeutic and non-therapeutic drugs, glucose and salt-alter osmotic balance, and oxygen.
Infectious agents: bacteria, virus, fungi, and parasites.
Immunologic reactions: immune imbalance - autoimmunity, hypersensitivities, immune deficiency. Graft rejection.
Genetic defects - congenital malformations (down syndrome), single base mutations causing functional deficiency or protein misfolding.
Nutritional imbalance: deficiency = malnutrition, vitamins (vitamin A, D). Excess = obesity, type 2 diabetes, hypertension, hyperglyceridemia.
Physical agents: mechanical trauma (abrasions, contusions, lacerations, etc). Thermal injury (burns, hyperthermia, hypothermia), electrical injury, ionising radiation, atmosphere (pressure).
Recognise the point at which injury becomes irreversible
Injury occurs when the function of the cell has been compromised. This can be as a consequence of failure to adapt to increased workload or stress, or can occur directly in response to an injury inducing stimulus or insult. Not all injured cells will die (irreversible injury) and that in response to a mild insult or insult of short duration a cell may recover its function (reversible injury). A cell is irreversibly injured when the plasma membrane has lost its integrity (ruptured) and when the cell no longer has functioning mitochondria.
Explain how cell and injury specific factors affect progression from reversible to irreversible injury
The outcome of injury (reversible or irreversible) is determined by features of the injury inducing stimulus and factors intrinsic to the cell or tissue being injured.
Features of the injury: whether the severity of an injury inducing stimulus is mild or severe with exposure over a short or long period of time (duration) will effect whether the induced injury is reversible or irreversible.
Factors intrinsic to the cell or tissue: the difference in function and metabolic activity of different cell types will determine its response to injury.
The state of cell can also effect the cells ability to survive an injury. I.e., a hypoxic injury to an athlete before they have run a marathon will be less damaging than that the same hypoxic injury after they have run a marathon.
The ability to adapt to stress is another factor that will contribute to the cells response to injury.
The genetics of an individual will determine the outcome of injury. Each individual has differences in their genetic composition which determines how they respond to injury.
Recovery or death
Reversible injury - recovery if damaging stimulus is removed. Compromise cell function. May compromise organ function.
Reversibly injured monocytes (transient ischemia) may be transiently non-contractile which will affect function of the heart.
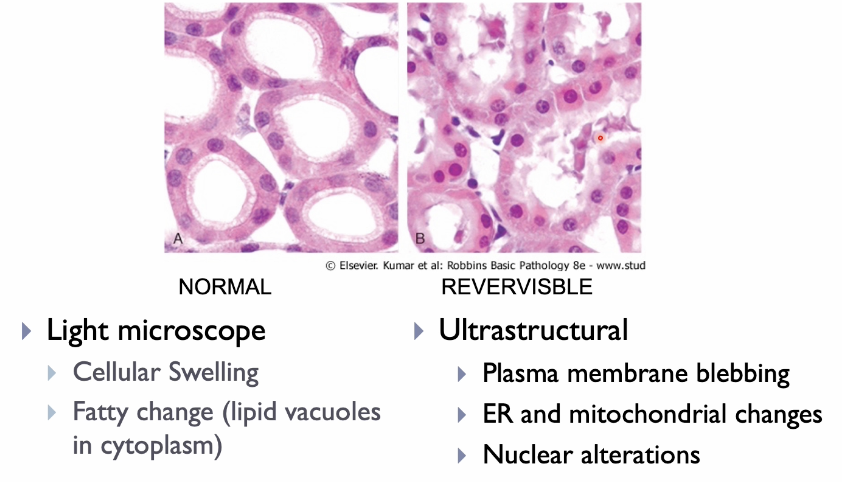
Morphological features of injury-light microscope
Cell swelling.
Irreversible injury and cell death: when the cell cannot recover and it dies. Two types of cell death which differ in morphology, cause and roles in disease.
Necrosis
Apoptosis
May have occurred before morphological changes become apparent.
Morphology of necrosis
Explain the mechanisms of cell injury
Generation of ROS: reactive oxygen species (ROS) are generated by inefficient aerobic respiration. ROS attack macromolecules including proteins (cytoskeleton), lipids (phospholipid membranes), and DNA.
Damaged organelle membranes: intact mitochondrial membranes are required to maintain the proton gradients used to synthesise ATP. Membrane damage or the formation of a channel in the mitochondrial membrane (mitochondrial permeability transition pore) can lead to reduced or less efficient ATP production and the release of Ca2+. Damaged lysosomal membranes lead to the leakage of lysosomal enzymes into the cytoplasm. These enzymes are activated in the acidic intracellular pH of the injured cell.
Damaged plasma membrane: damaged plasma membrane (separated the interior of the cell from the outside environment) leads to the loss of osmotic balance and influx of fluids and ions.
Cytoskeleton and membrane damage: decreased synthesis of macromolecules (proteins and lipids) and activation of calcium dependent enzymes (proteases and lipases) damages the cells cytoskeleton (protein) and membranes (phospholipids).
Calcium dyshomeostasis: calcium (Ca2+) concentration are tightly regulated and kept at low (micromolar) concentrations within the cytoplasm (relative to millimolar concentrations in the extracellular space) or sequestered within cellular organelles (mitochondria and ER). Injury can lead to an increase in cytoplasmic concentrations (failure of ion channels and damaged membranes) and subsequence activation of calcium dependent enzymes.
ER stress: cell injury can lead to the accumulation of misfolded proteins in the ER leading to ER stress.
ATP is required to maintain the activity of ATP-dependent ion channels. Failure of ATP-dependent ion channels result in the accumulation of intracellular sodium, efflux of potassium and net gain of water. ATP-dependent ion channels also contribute to maintaining the low intracellular concentration of calcium in the cytoplasm.
Reduced macromolecule synthesis: ATP is required for synthesis of lipids and proteins that are needed to maintain the structure of phospholipid membranes (plasma, mitochondria, and lysosome) and cytoskeleton.
Decreased ATP production: decreased ATP production can occur in an hypoxic environment where oxygen is not available for aerobic respiration or as a consequence of mitochondrial damage.
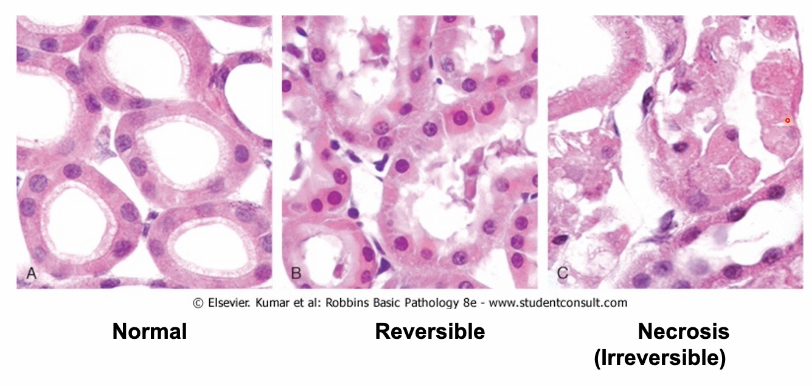
Recognise the morphological features of reversible and irreversible injury
Autolysis: ROS and lysosomal enzymes digest cell contents. Digestion of nucleic acid (kayolysis) leads to decreased staining of the nucleus with hemotoxylin. Denaturation of cytoplasmic proteins leads to more staining with eosin and loss of RNA leads to less hemotoxylin staining giving the cytoplasm of injured cells a bright pink (eosinophilic) appearance and the loss of glycogen particles gives cells a 'glassy' appearance.
Condensation or clumping of chromatin: in response to decreased aerobic respiration cells with glycogen reserves may undergo anaerobic respiration. The production of lactic acid, as a product of anerobic respiration, lowers the pH of the cell and can lead clumping of chromatin that can be observed as dense hemotoxylin staining of the nucleus.
Cell swelling: Failure of ATP-dependent ion channels leads to the isosmotic gain of water and swelling of the cell and organelles (mitochondria and ER).
Cell membrane blebbing: loss of cytoskeletal proteins affects the structure of the cell and leads to bulging of regions of the cell membrane in response to swelling.
Irreversible injury: Injury to cells is irreversible when the integrity of the plasma membrane is lost. Lysosomal membranes rupture and lysosomal enzymes digest the content of the cell (lysosomal enzymes are active due to the reduced pH of the cells cytoplasm) and mitochondrial membranes are irreversibly damaged.
Explain the mechanisms of cell injury (apoptosis)
Apoptosis - where the cell membrane remains intact.
Generation of ROS: ROS attack macromolecules including proteins that can trigger apoptosis through the unfolded protein response and introduce mutations and breaks in DNA that can trigger apoptosis.
Damaged organelle membranes: membrane damage or the formation of a channel in the mitochondrial membrane (mitochondrial permeability transition pore) can lead to the release of Ca2+ and cytochrome C into the cytoplasm, triggering caspase activation and apoptotic death.
Apoptotic bodies: caspases activate enzymes that degrade the cell's proteins and nucleus. The end result is the characteristic cellular fragmentation of apoptosis where cellular contents are packaged into apoptotic bodies.
DNA and protein damage: severe DNA damage may trigger apoptosis. Intracellular accumulation of proteins can trigger apoptosis. Proteins accumulate due to misfolding, increases in their production or reduced ability to eliminate them. This can be due to inherited or acquired mutations, aging, ROS, and exogenous factors such as hypoxia and viral infections that affect protein production and quality control.
Calcium dyshomeostasis = apoptosis: calcium (Ca2+) concentration are tightly regulated and kept at low (micromolar) concentrations within the cytoplasm or sequestered within cellular organelles (mitochondria and ER). Injury can lead to an increase in cytoplasmic calcium concentrations (failure of ion channels and damaged membranes) and subsequent activation of calcium dependent enzymes including caspases.
ER stress = apoptosis: cell injury, including through genetic mutations that affect protein structure or clearance, can lead to the accumulation of misfolded proteins in the ER, ER-stress and the induction of the unfolded protein response (UPS). This adaptive response attempts to rebalance protein synthesis (increased chaperone proteins and decreased protein synthesis) but if this response fails proapoptotic sensors are activated.
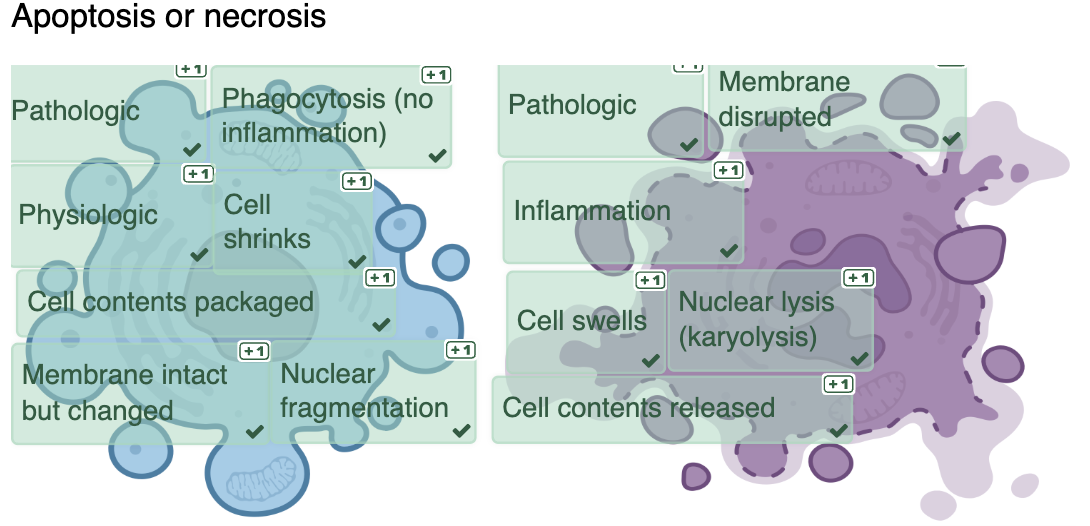
Necrosis
Occurs when there is a disturbance of membrane function or inability to reverse mitochondrial dysfunction.
Morphological features:
Increased eosinophilic staining-denatured protein and loss of RNA.
Vacuolation-digested cytoplasmic organelles.
Swelling of ER and mitochondria.
Myelin figures-whorls of phospholipid from damaged membranes.
Discontinuous plasma and organelle membranes.
Nuclear changes due to breakdown of DNA and chromatin.
Karyolysis-decreased basophilia from DNA breakdown.
Pyknosis-nuclear shrinkage and increased basophilia (condensed).
Karyorrhexia-nuclear fragmentation.
Patterns of tissue necrosis
When large numbers of cells die, the tissue is said to be necrotic.
Distinct patterns of necrosis may provide clues to the cause.
Appearance of necrotic lesion is influenced by the balance between:
Coagulative - cells dead, tissue architecture preserved. DENATURATION.
Liquefactive - cells digested, no tissue structure. DIGESTION.
TYPES OF NECROSIS
Coagulative necrosis: denaturation is greater than digestion. Most common. Due to severe ischemia - occurs in solid organs (except brain). Nucleus lost, architecture of cells preserved.
Liquefactive necrosis: Digestion is greater than denaturation. Complete digestion of dead cells. Associated with infection (bacterial and fungal). Inflammatory response contributes to digestion of tissue. Ischemia in brain - necrotic area becomes fluid-filled cyst.
Caseous necrosis - fragmented lysed cells with amorphous granular appearance. Tissue architecture obliterated. Associated with infection with mycobacterium tuberculosis
Large numbers of organisms and degenerating tissue.
Fat necrosis - refers to focal areas of fat destruction. Enzymes liquefy membranes of fat cells. Release fatty acids which combine with calcium to cause patchy white lesions (fat saponification). Most common in acute pancreatitis.
Fibrinoid necrosis - occurs in blood vessels in response to deposition of immune complexes. Necrosis associated with leakage of fibrin and inflammatory cells.
Gangrenous (lower limb) necrosis - usually describes coagulative necrosis that occurs in a lower limb which has lost its blood supply. Liquefactive necrosis may accompany a bacterial infection - wet gangrene.
APOPTOSIS
Irreversible injury leading to apoptosis.
Cell shrink - intensely eosinophilic cytoplasm.
Nuclear chromatin condensation and fragmentation (but not karyolysis).
Formation of apoptotic bodies (nuclei and cytoplasm) membrane bound vesicles of cytosol and organelles.
Quickly phagocytosed.
No inflammatory response.
Phagocytosis
A form of endocytosis in which specialised endocytic vesicles (phagosome) are used to ingest large organisms (microbes or dead cells).
Phagocytes
Macrophages - professional phagocytes that reside in tissues throughout the body.
Neutrophils - short-lived cells, abundant in blood but not present in normal tissues.
Apoptosis or necrosis
Other mechanisms of cell death and survival
CELL DEATH:
Necroptosis - 'programmed necrosis'.
Ferroptosis - form of cell death associated with high levels of iron and excess ROS causing lipid peroxidation.
Pyroptosis - form of cell death associated with release of fever inducing IL-1.
SURVIVAL:
Autophagy - a survival mechanism induced under stress conditions by recycling metabolites.
REGENERATION AND REPAIR
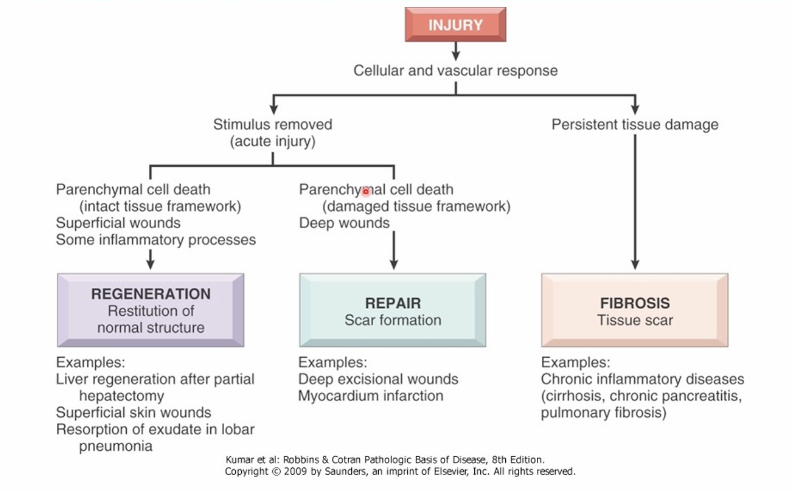
Healing
Regeneration:
Tissues composed of cells with proliferative capacity AND the underlying structure of the tissue has not been too severely damaged.
Repair by scar formation:
Tissues composed of cells with limited or no proliferative capacity OR the underlying structure of the tissue is lost.
STEPS involved in repair by scar formation
Injury to permanent tissue composed of non-proliferating cells or injury to labile and stable tissue where the underlying structure have been lost will be repaired by the laying down of connective tissue (collagen) that forms the scar.
Hemostasis - following a traumatic injury, a blood clot (hemostasis) forms to stop bleeding.
Inflammation - acute inflammation removes the cause and consequence of injury. Repair occurs when anti-inflammatory M2 macrophages replace pro-inflammatory M1 macrophages. The M2 macrophages promote repair by secreting growth factors that promote repair through angiogenesis and activation of fibroblasts to produce collagen - the essential elements of repair by scar formation. M1 macrophages are pro-inflammatory and phagocytic.
Granulation tissue - new blood vessels (angiogenesis), recruitment and proliferation of fibroblasts, deposition of connective tissue (collagen). New blood vessels develop from existing blood vessels, through the recruitment and proliferation of endothelial cells. Fibroblasts are recruited to the site of repair where they proliferate and become activate to secrete collagen, the main extra-cellular matrix component of the scar.
Remodelling - the connective tissue that has been deposited is reorganised to produce the stable fibrous scar. There is a reduction in vascularisation and connective tissue is reorganised to increase the strength of the stable fibrous scar. Wound strength increases through crosslinking of collagen fibres and replacement of provisional type III collagen deposited early in repair with thicker, more resilient type I collagen. Over time, the scar shrinks due to the action of matrix metalloproteinases (MMPs) that digest the extracellular matrix components.
Factors that affect healing:
Foreign bodies: such as glass interfere with successful would healing by prolonging inflammation and causing further injury.
Nutrition: good nutrition is essential for successful wound healing. Vitamin C is required for the synthesis of collagen.
Location: the location of the injury can effect contraction of the wound.
Poor perfusion: reduces the supply of blood needed for successful wound healing by limiting inflammation needed to remove the cause and consequence of injury and preventing the recruitment of cells required for the healing process.
Diabetes: can delay wound healing.
Medication: some anti-inflammatory agents can inhibit the chemical mediators (cytokines) that promote collagen deposition.
Mechanical factors: mechanical factors such as pressure caused by immobilisation or torsion caused by movement can cause wounds to tear apart.
Infection: prolong inflammation and may increase local tissue injury.
Recognise the complications of healing
Wound splitting (dehiscence): can occur as a result of infection inappropriate suturing, poor nutrition, or mechanical forces.
Chronic wounds that do not heal due to poor blood supply and low oxygen - e.g., ulcers and pressure sores.
Excessive scarring can lead to hypertrophic scars and keloids where there excessive collagen deposition or proud flesh where there is excessive granulation tissue.
Contracture is an exaggeration of the contraction of wounds that is part of the normal healing process that leads to deformities of the wound and the surrounding tissues.
Fibrosis is a term used to describe the abnormal deposition of collagen typically associated with chronic disease.