teeth
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
tooth development from embryonic layers
tooth development begins in the oral epithelium (ectodermal in origin.) signals exchanged between the oral epithelium and NCC derived mesenchyme underneath initiate odontogenesis
localised thickening of oral epithelium occurs forming the labiogingival band. this separates into the labiogingival lamina and the dental lamina.
thickening of dental laminae on medial aspect of the labiogingival band
mesenchyme underneath each laminae condenses
dental lamina invaginates forming the dental bud
dental bud expands and branches to form an enamel organ to surround a NCC derived dental papilla
this dental papilla enamel organ complex will form the deciduous tooth
a small mass of cells bud off from the dental lamina of the deciduous enamel organ, this cell cluster is the primordium of the permanent tooth.
what do the inner enamel epithelium differentiate into, how are odontoblasts derived, what does dentine and cementoblasts do?
budding off of permanent tooth primordium continues
inner enamel epithelium (derived from oral epithelium) differentiates into ameloblasts.
cells in the dental papilla which are neural crest cell derived mesenchyme differentiate into odontoblasts.
as odondoblasts lay down dentine, central part of the dental papilla remains as the pulp and the dentine surrounds the pulp and extends downwards to form tooth rot.
later epithelial cells near distal part of tooth known as cementoblasts secrete cementum aorund tooth rot
ameloblasts
what do they secrete
how do they maintain contact with new unmineralised enamel
what characteristic do they form
what do they produce
what happens after they erupt
secrete enamel which forms the outer covering of the tooth crown
maintain contact with new unmineralised enamel via cellular projections called thomes fibres
form crown characteristc of each tooth type
produce matrix which is not remodelled
are lost upon tooth eruption
odontoblasts- what do they do and what type of cell are they
secrete dentine which forms before enamel and induces enamel formation
columnar
role of mesenchyme, how are tooth tissues laid down
mesenchymal cells can differentiate but have stable morphogenetic properties
experimentally molar tooth mesenchyme and non oral ectoderm was combined resulting in a tooth shaped structure, showing that mesenchyme carries instructures for tooth morphology
neural crest derived mesenchyme determines tooth type
when molar mesenchyme is paired with incisor epithelium in culture the tooth that forms is a molar
tooth tissues are laid down from the crown to the root
tooth does not reach its final length while still embedded in jaw, achieved after eruption begins
tooth eruption- temporary
eruption after crown is fully formed but before complete formation of the root
eruption provides space for completion of root
epithelial covering is continuous with gums upon eruption
wear removed epithelium
permanent tooth eruption
migrates into socket of temporary tooth
increasing pressure from tooth
resorption of temporary tooth root
loosening
shedding
permanent tooth replaces
what aids tooth eruption?
osteoclasts and odontoclasts resorb alveolar bone and root of the deciduous tooth to allow space for permanent tooth to move upward
bone remodeling occurs to allow the tooth to move upward
at the bottom of the developing root there is tissue fluid and blood supply which create hydrostatic pressure pushing the tooth upward as the root grows
the periodontal ligament remodel collagen fibres and generate contractile forces to help pull the tooth upwards
Poll
dentine
nature of production and rate
contents
produced continually
rate increases during repair
innervated
mineralised matrix- collagen type i, dentine, specific protein
odontoblasts recede from newly formed surfaces
like bone but acellular
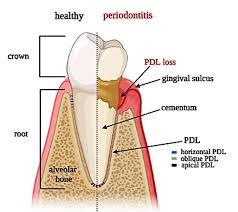
peridontal ligament
where does it suspend tooth from
what do the PDL fibres bridge
shape
what is it lined by
suspends tooth in its alveolar socket
fibres bridge alveolar bone and cementum
shaped to accomodate tooth root-may be branched
lined by compact bone
cementum
what does it surround
properties
what collagen
is it remodelled
surrounds dentine of root
mostly acellular
not readily resorbed
type i collagen
not remodelled
can alveolar bone be remodelled
yes
what is the furcation angle
point where roots diverge in teeth with two or more roots
where does the crown meet the root
cemento enamel junction
what does the enamel consist of
hexagonal prisms or rods of hydroxyapatite crystals held together by cementing organic matrix
pulp
connective tissue, nerves, lymph, blood vessels, collagen and undifferentiated reserve mesenchymal cells
what causes dentine to be sensitie to pain
Odontoblasts line the pulp cavity and branch into the dentine tubules. These branches, together with the fine nerve endings, cause the dentine to be sensitive to temperature and pain.
The odontoblasts lay down dentine and reduce the pulp cavity in size as the animal ages.
dangers to pulp
Physical trauma: may cause bruising, haemorrhage or pulpitis.
Accidental over-heating from polishing or scaling: may cause pulp necrosis.
Pulp exposure after tooth fracture: may cause pulpitis and possibly pulp necrosis.
Loss of blood supply following trauma: will cause ischaemic necrosis
dentine tubu;e
extends from external surface to the pulp
can transmit pain to pulp if the dentine is exposed
primary dentine
forms before tooth eruption
secondary dentine
forms after eruption
develops from odontoblasts living within pulp and laid down in layers within pulp cavity
reparative/tertiary dentine
forms as a result of trauma to the odontoblasts- can be thermal, chemical, bacterial, mechanical
few tubules and darker and dense
cribiform plate
densest bone that lines the alveolus
it may be seen radiograpically as a white line called lamina dura
periodontal ligament
what is it comprised of
where does it insert
3 type
comprised of taut collagen fibre bundles called sharpeys fibres- inserted into cementum and alveolar bone which are anchored to cementum of tooth and alveolar bone
gingival, trans septal and alveolodental fibres
blood vessels within periodontal ligament which are evenly dstributed
nerves capable of transmitting heat cold pain and pressre
cementum
what does it cover
what does it provide a point of attachment for
what is the composition similar to
how is it nourished
covers the enamel free root
provides a point of attachment for periodontal ligament
similar in composition to woven bone
capable of formation, destruction and repar
remodels continually throughout life
nourished from vessels within periodontal ligament
gingival sulcus
sulcus lining epitheium (junctional epithelium) renews more rapidly than oral
bathed in crevicular fluid which contains antibodies, neutrophils, lymphocytes
depth of more than 4mm in dogs is dangerous- sign of active disease and attachment loss
interdental papilla
prevents impaction of food and devris between closely adjaent teeth
should be preserved during surgery
when viewed from coronal aspect there is an indentation called the col (the epithelium of this is not keratanised)
junctional epithelium
where is it located
why is it important
what does it attach, and using what
where is the apical extent of it
bottom of the sulcus
important in control of periodontal disease
attaches the gingival tissues to the tooth using hemidesmosomes
apical extent usually the cemento enamel juncion
what does the free gingiva suround
surrounds the crown of the tooth
cemento enamel junction
between anatomical root and crown
not visible in health
so sight indicates recession of attachment of tooth
attached gingiva
what does it adhere to and how
properties
tightly adherent to subgingival connective tissue and bone via deep rete pegs
keratinised- withstand stress and ripping and tearing food
mucogingival junction
properties
reasons why is might change in height
between mucus membrane of the oral cavity and gingiva
remains stationary throughout life
may change in height de to hyperplasia, recession or attachment loss
function of the alveolar bone
provide structural support to the root
gingival fibres
where are they
where do they extend
what do they do
in the gingiva above the alveolar crest
extend from cementum into gingival tissue
attach gingiva to tooth and bone
transseptal fibres
run interdentally
extend from cementum of one tooth to cementum of adjacent, over the alveolar crest
maintain tooth to tooth alignment
stabilise the dental arch
alveolodental fibres
where do they run
what do they do
what do they attach
true periodontal ligament fibres
run between cementum and alveolar bone
attach tooth to the alveolar bone
absorb and distribute occlusal force during chewing