Lecture 7: Hemoperitoneum/Peritonitis
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What is hemoperitoneum or hemoabdomen?
abnormal accumulation of blood in the peritoneal cavity
What are the potential causes of hemoperitoneum?
traumatic: HBC, kicks, falls
nontraumatic: neoplasia, nontraumatic adrenal gland rupture, nonmalignant disease (GDV, splenic torsion, vitamin K antagonists etc)
What is the #1 nontraumatic cause of hemoperitoneum in dogs and cats?
neoplasia
What is the typical clinical presentation of a hemoperitoneum case?
signalment:
younger = more likely trauma
older = more likely neoplasia
hx:
• Trauma or suspected trauma
• Neoplasia is usually nonspecific
• Previous hemorrhage
• Access to toxins or rodenticide
• Previous diagnosis of a mass
• Previous surgery or diagnostic procedure
How do hemoperitoneum cases present upon physical exam?
• External signs of trauma
• Abdominal distension (+/- fluid wave)
• Abdominal tenderness
• Contusion / Discoloration of abdominal wall
• Bulging umbilicus
What is the classic description of hemoabdomen rads?
loss of abdominal detail with focal or generalized “ground glass” appearance
What type of imaging is more sensitive with small quantities of fluid for a hemoabdomen case?
ultrasound - AFAST exam
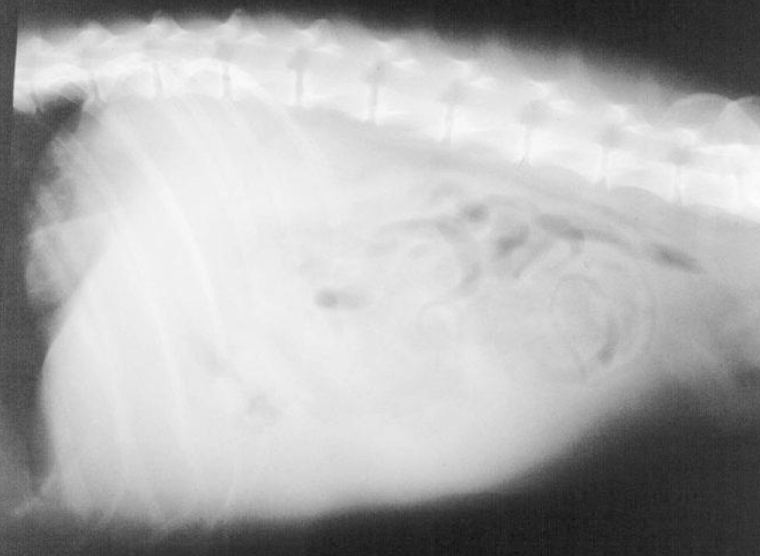
Describe this radiograph.
Loss of abdominal detail with focal or generalized “ground glass” appearance
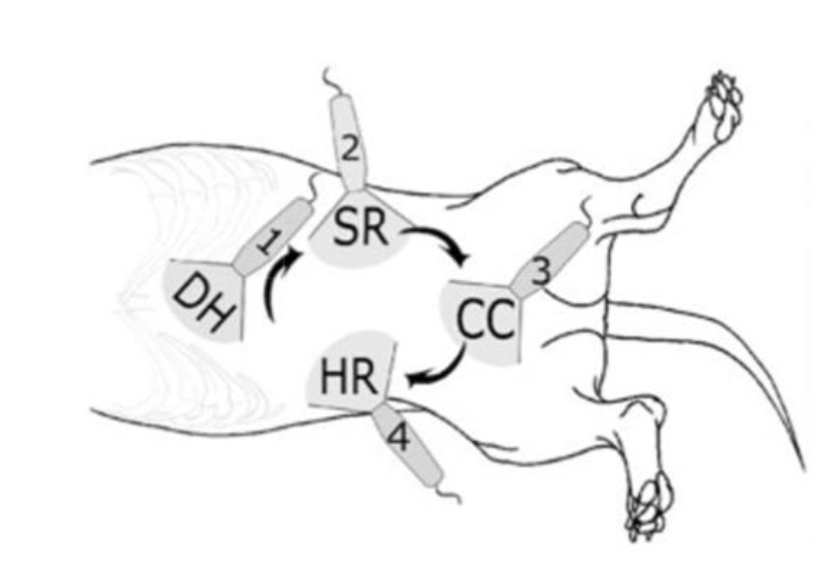
What type of imaging is this?
AFAST exam
What are the four views of an AFAST exam?
diaphragmaticohepatic
splenorenal
cystocolic
hepatorenal
True or false: Clinicopathologic abnormalities in dogs with hemoabdomen are typically similar regardless of the cause of the abdominal bleeding.
true
How is hemoperitoneum diagnosed?
by finding nonclotting bloody fluid in abdomen by abdominocentesis or diagnostic peritoneal lavage (DPL)
What is replacing the use of DPL in trauma?
FAST exam
What are the negative of DPL?
invasive
low specificity
false negatives: retroperitoneal injury, ruptured diaphragm
True or false: trauma patients with hemoabdomen that stabilize after medical management still require surgery.
false - they often do not
How are hemoabdomen cases medically managed?
• IV fluid replacement therapy
• Blood transfusion
• Tight abdominal wrap? (during stabilization)
• Oxygen therapy
What preoperative issues need to be managed before a hemoabdomen surgery?
stabilize shock
correct fluid, acid-base, electrolyte, and CV abnormalities
blood transfusion if PCV< 20%, hypoxic from anemia or respiratory depression, or if ongoing bleeding is expected
Why should barbiturates and acetylpromazine be avoided in hemoabdomen patients?
barbiturates: cause splenic congestion
acetylpromazine: RBC sequestration, hypotension, impact on platelet function
What are the indications for hemoabdoment surgery?
• Undetermined source of hemorrhage
• Uncontrolled hemorrhage
• Evaluation/Removal of intra-abdominal neoplasia
What is primary generalized peritonitis?
Spontaneous inflammation of the peritoneum with no obvious intra-abdominal reason for leakage of bacteria
What is secondary generalized peritonitis?
inflammation of peritoneum in conjunction with an intra-abdominal reason for the inflammation/infection (infectious or noninfectious)
What is the predominant form of peritonitis in dogs?
secondary generalized
What most commonly causes secondary generalized peritonitis?
bacteria usually originating from contamination from GI tract (sx wound dehiscence, GI neoplasia)
Besides bacteria from the GI tract, what are some other causes of secondary generalized peritonitis?
• Gal Bladder perforation, rupture, or neoplasia
• Gastric or intestinal foreign bodies
• Intussusception
• Mesenteric avulsion
• GDV
• Cystocentesis
• Necrotizing Cholecystitis
• Pancreatic Abscess
• Prostatic Abscess
• Foreign body penetration of the body wall
Why is differentiating primary from secondary generalized peritonitis important?
because surgery is not routinely performed in Primary Generalized Peritonitis but is required in Secondary Generalized Peritonitis
Describe the bacterial association in peritonitis?
• Gram-positive bacteria more common in Primary
• Gram-negative bacteria more common in Secondary
• Primary are more likely to be monobacterial
• Secondary are more likely to be polybacterial
What is the typical presenting complaint for peritonitis cases?
lethargy, anorexia, V/D, and/or abdominal pain
cats more likely to present with lethargy, depression, and anorexia, than abdominal pain or vomiting
When suspected peritonitis, what needs to be ruled out in a sick intact female dog?
pyometra
What is usually found during the PE of a peritonitis case?
• Abdominal palpation often causes pain
• Vomiting, Diarrhea
• Abdominal distention
• Pale mm, Prolonged CRT
• Tachycardia may indicate shock
• Dehydration and arrhythmias may occur
What is usually seen on a peritonitis radiograph?
• Intestinal tract may be dilated with air or fluid or both
• Free abdominal air → Rupture of a hollow organ, Gas-producing anaerobic bacteria
• Localized peritonitis , secondary to pancreatitis, may cause a “sentinel loop” by making the duodenum appear to be fixed and elevated
What is the most common laboratory finding in peritonitis?
marked leukocytosis
What was a prognostic indicator of peritonitis in cats, with higher levels associated with poorer prognosis?
lactate levels
Why is surgery not indicated if a diagnosis of primary peritonitis is made preoperatively?
• May result in worsening of underlying disease
• Associated with increased morbidity
What are the medical management goals of peritonitis?
1. Eliminate cause of contamination
2. Resolve the infection
3. Restore normal fluid & electrolyte balance
What are the indications for abdominocentesis?
• Shock with no apparent cause
• Undiagnosed abdominal disease
• Suspicion of post-op GI dehiscence
• Blunt or penetrating abdominal injury (gunshot. Dog bite, HBC)
• Abdominal effusion
• Undiagnosed abdominal pain
When should diagnostic peritoneal lavage be performed?
in animals suspected of having peritonitis if abdominocentesis and 4- quadrant paracentesis are unsuccessful in obtaining fluid for analysis and ultrasonography (AFAST) or CT imaging are not available
When is exploratory surgery indicated in peritonitis cases?
Cause of peritonitis cannot be determined
Bowel rupture
Intestinal obstruction (e.g., bowel incarceration, neoplasia)
Mesenteric avulsion is suspected
Why is intraoperative peritoneal lavage controversial?
could disseminate localized peritonitis
if too much fluid is not removed the fluid inhibits the body’s ability to fight off infection, probably by inhibiting neutrophil function
What is the most appropriate lavage fluid for intraoperative peritoneal lavage?
warmed isotonic saline
True or false: there is no evidence that adding antiseptics or antibiotics to intraoperative peritoneal lavage fluids is of benefit.
true
How is open abdominal drainage performed?
a small section of abdominal incision left open → sterile wraps placed around wound and changed based on fluid drainage and external soiling
What are the complications of open abdominal drainage?
• Persistent fluid loss
• Hypoalbuminemia
• Weight Loss
• Adhesion of abdominal viscera to bandage
• Contamination of the abdominal cavity with cutaneous organisms
What are the advantages of open abdominal drainage?
• Improved metabolic condition
• Fewer abdominal adhesions
• Fewer abscesses
• Access for repeated inspection/exploration
What are the disadvantages of open abdominal drainage?
• Hypoalbuminemia
• Hypoproteinemia
• Anemia
• Nosocomial Infections
What type of drainage is effective in dogs and cats with generalized peritonitis if effusion is serous in nature and involves far less time and effort than OAD?
closed suction drainage

What is this?
Jackson-Pratt Drainage Catheter
How is an abdominocentesis performed?
• Insert 18-20g 1 ½ inch over-the-needle catheter (with added side holes) at most dependent point
• Do not attach syringe
• Allow fluid to drip from catheter → Collect in sterile EDTA tube → Submit samples for culture (aerobic & anaerobic) → Make smears
• If fluid does not drip, use a 3-cc syringe with gentle suction
How is a diagnostic peritoneal lavage performed?
• Make 2 cm skin incision caudal to umbilicus
• Hemostasis to avoid false positives
• Small incision into the linea alba → Hold edges of incision while peritoneal lavage catheter is installed (without trocar)
• Direct catheter caudally into pelvis
• Gently aspirate
• If negative aspiration, attach catheter to IV line with bag of warm sterile saline (20 ml/kg) and infuse into abdominal cavity
• Roll patient gently side-to-side to disperse fluid
True or false; DPL does not reliable exclude significant retroperitoneal injury or hemorrhage.
true
When can the abdominal incision from open abdominal drainage be closed?
when bacterial numbers have declined and neutrophils are no longer degenerative (usually 3-5 days post-op)
How is closed suction drainage performed?
• In cats and small dogs, place one drain between the liver and the diaphragm
• In large dogs, place a second drain into the caudoventral abdomen
• Exit the drain tubes through the body wall thru a paramedian stab incision
• Suture drains to the abdominal skin with a Roman Sandal or Chinese Finger Trap
• Close the abdomen routinely
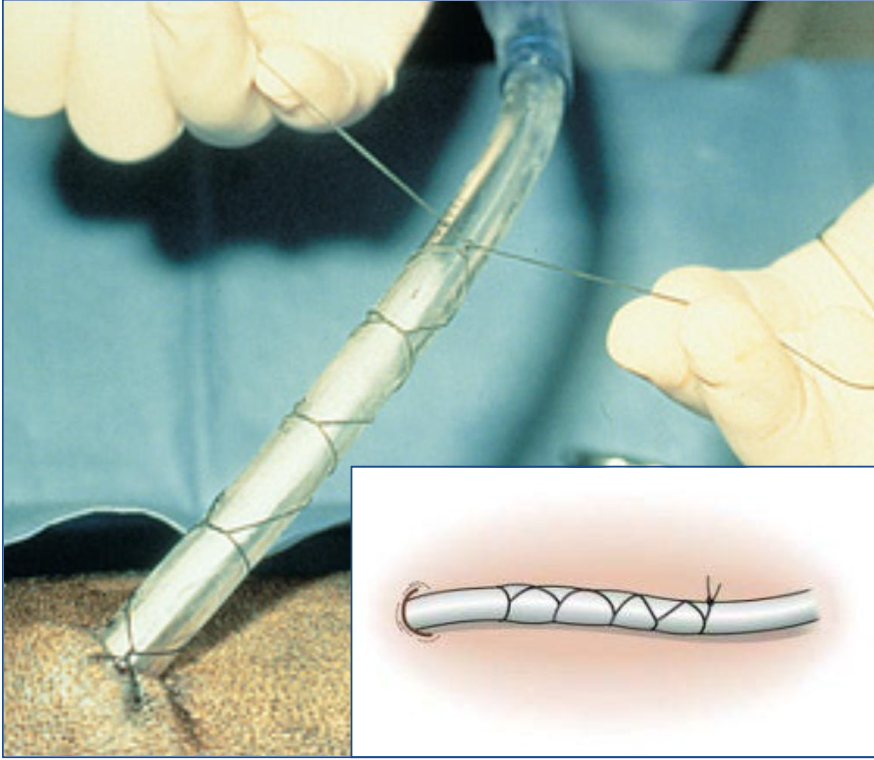
What is the roman sandal suture pattern (chinese finger trap)?
suture pattern to attach drain to abdominal skin
What is the recommended suture material in peritonitis cases?
• Use monofilament nonabsorbable suture or slowly absorbable suture
• Do NOT use braided suture
• Do NOT use suture that is rapidly degraded
What post-op assessments are required after peritonitis procedures?
• Fluid therapy continued (especially if OAD)
• Monitor electrolytes, acid-base, serum protein and correct as required
• Nasal oxygen if sepsis
• Ensure adequate caloric intake
• Consider plasma if hypoproteinemic
• Analgesia
What is the prognosis of peritonitis cases?
generalized peritonitis = guarded
many survive with aggressive therapy