Bio 207 Exam 3
1/120
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
121 Terms
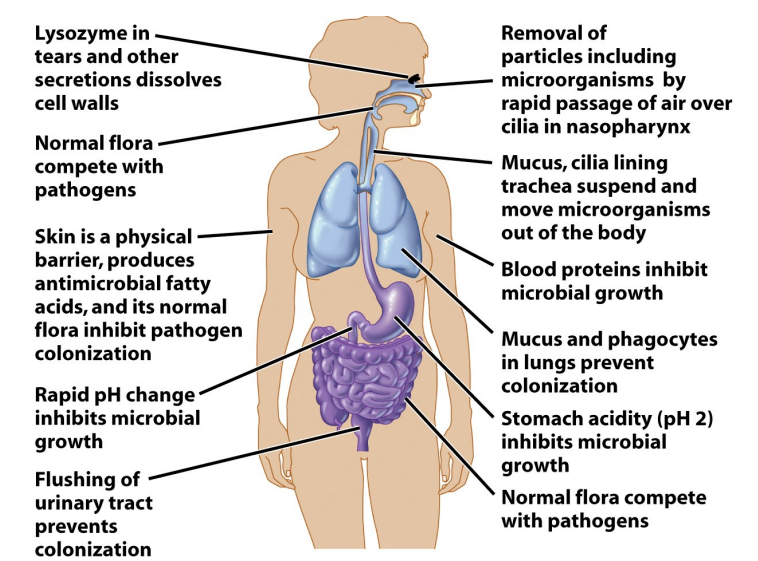
General Host Defenses (first line of defense)
Skin & Mucosal Surfaces
organism must penetrate, adhere, grow
there is tissue specificity for most infectious agents
tight junctions in epithelial tissue seal off "inside"
mucus limits direct access to epithelial cells
breaks in epithelium allow microbes to bypass these barriers
Normal Flora
young are more susceptible before stable adult flora develops
diet, drugs can alter normal flora
Antimicrobial Secretions
lysozyme & other enzymes kill bacteria in saliva and tears
defensin proteins insert in microbial membranes
blood proteins sequester nutrients
fatty acids on skin lower pH
Physical Removal
cilia/mucus movement
urine flushing
Stomach Acid
Blood & Lymph Systems
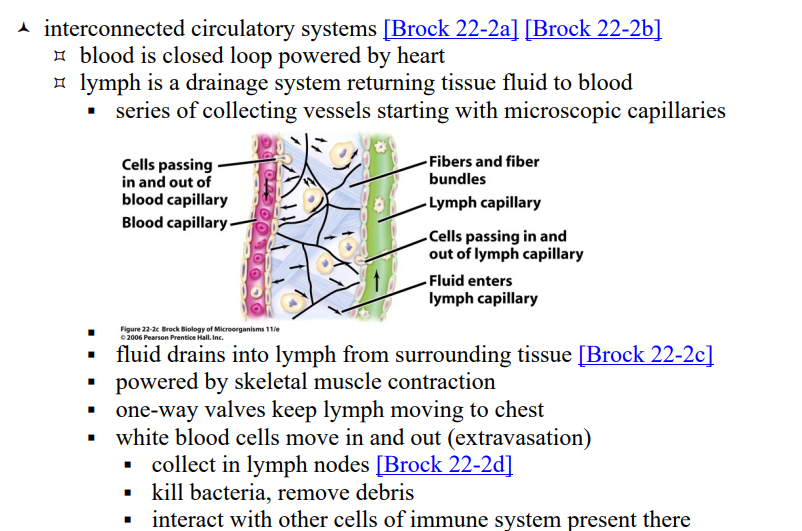
Organs/Tissues
primary- where lymphocytes develop
thymus & bone marrow
secondary- where lymphocytes collect
spleen, lymph nodes, tonsils, adenoids, appendix
SALT, MALT, GALT- skin, mucus, gut-associated lymphoid tissue
M cells in skin, tonsils, adenoids, intestines monitor flora
Blood cells
~45% of blood volume
erythrocytes- red blood cells (not part of immune system)
platelets- involved in clotting
leukocytes- white blood cells
erythrocytes
red blood cells
not part of immune system
enucleated - nucleus has been removed (cells w/out nucleus)
carry oxygen
platelets
blood cells
involved in clotting
Development of white blood cell components of the immune system (diagram)
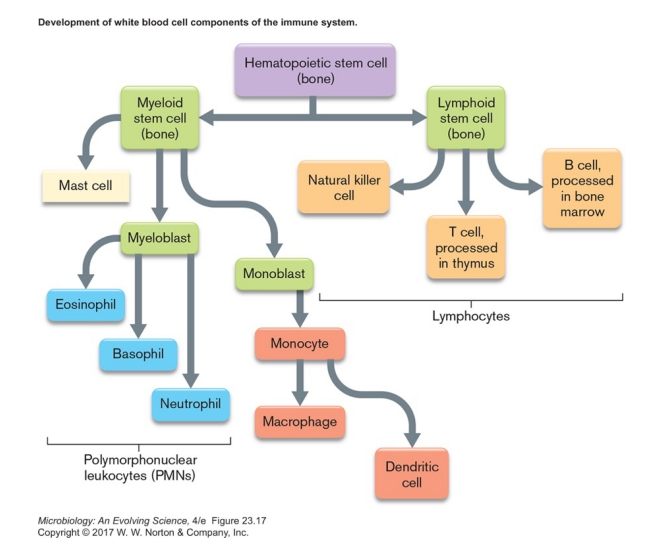
leukocytes
white blood cells
monocytes, dendritic cells, macrophages- phagocytic, antigen-presenting cells (APCs)
polymorphonuclear leukocytes (PMNs or granulocytes, in blood)
mast cells- mediate inflammation throughout body, not in blood
lymphocytes (mostly in spleen and lymph nodes)
lymphocytes (mostly in spleen and lymph nodes)
leukocytes- white blood cells
natural killer cells- kill infected or cancerous cells
T cells- central to adaptive immunity
B cells- part of adaptive immunity, produce antibodies
mast cells
leukocytes- white blood cells
mediate inflammation throughout body, not in blood
monocytes, dendritic cells, macrophages- phagocytic, antigen-presenting cells (APCs)
leukocytes- white blood cells
engulf foreign cells, viruses, proteins
break these down & display foreign peptides on their surface
monocytes circulate in blood
dendritic cells & macrophages attach to different tissues
polymorphonuclear leukocytes
leukocytes- white blood cells
(PMNs or granulocytes, in blood)
neutrophils- phagocytic cells, migrate to site of infection
can use Neutrophil Extracellular Trap (NET) to kill cells
eosinophils- anti-protozoan secretions
basophils- inflammation mediator
neutrophils
polymorphonuclear leukocytes
phagocytic cells, migrate to site of infection
can use Neutrophil Extracellular Trap (NET) to kill cells
eosinophils
polymorphonuclear leukocytes
anti-protozoan secretions
basophils
polymorphonuclear leukocytes
inflammation mediator
natural killer cells
lymphocytes (mostly in spleen and lymph nodes)
kill infected or cancerous cells
T cells
lymphocytes (mostly in spleen and lymph nodes)
central to adaptive immunity
B cells
lymphocytes (mostly in spleen and lymph nodes)
part of adaptive immunity, produce antibodies
Plasma proteins
soluble in fluid portion of blood (~55% of blood volume)
fibrinogen- clotting
antibodies
complement
iron sequestration & other antibacterial proteins
Inflammatory Response
Innate Immunity (second line of defense)
a non-specific response to wounds & infection
signs described 2000 years ago
redness (rubor)
heat (calor)
pain (dolor)
swelling (tumor)
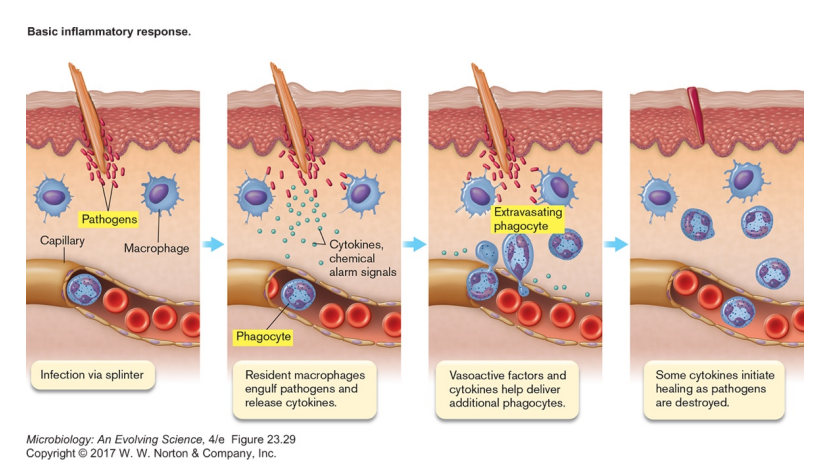
Detection of foreign cell
Innate Immunity (second line of defense)
triggered by unique signals of invader (MAMPs, microbe-associated molecular patterns)
bind to Toll-like receptors (in membrane) or Nod-like receptors (in cytoplasm)
cause transcription and release of cytokines

Clotting
Innate Immunity (second line of defense)
clotting factors released by platelets
attempt to contain infection
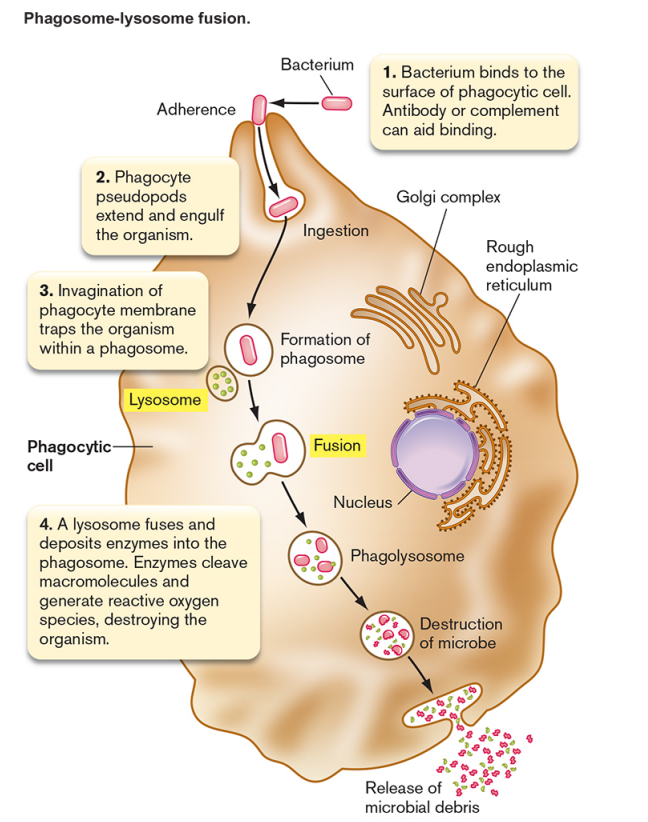
Phagocytosis
Innate Immunity (second line of defense)
phagocyte (macrophage) engulfs microbe
invader is recognized because it does not have self-antigen (CD47)
some pathogens can avoid because of capsule
antibodies can increase phagocytosis (opsonization)
microbe is killed/digested in phagolysozome
multiple pathways used
some pathogens resistant to digestion
peptides from invader may be displayed on phagocyte surface (antigen presentation)
peptide release can stimulate/attract other leukocytes
macrophages also release (and are activated by) cytokines
Extravasation
Innate Immunity (second line of defense)
Extravasation brings neutrophils from nearby capillaries
cytokines cause local endothelial cells to make selectins
selectins/integrin/ICAM-1 retain passing neutrophils from circulating blood
bradykinin from damaged host cells loosens connections between endothelial cells
allows neutrophils to squeeze out
attracted to wound by chemokine gradient
triggers mast cells in tissue to release histamines
causes vasodilation (blood volume increases), bringing more cells
vessel wall permeability increases, leading to edema (fluid buildup)
triggers prostaglandin release → pain
aspirin and related pain relievers prevent prostaglandin synthesis
Inflammation summary
benefits of inflammation
increased blood volume brings in more antimicrobial agents
increased temperature makes phagocytes more efficient, may inhibit bacteria
clot may isolate area of infection
downside of inflammation
may release nutrients & promote bacterial growth
microbe can gain access to further tissue via blood vessels
high fever can harm host
chronic inflammation damages host tissue
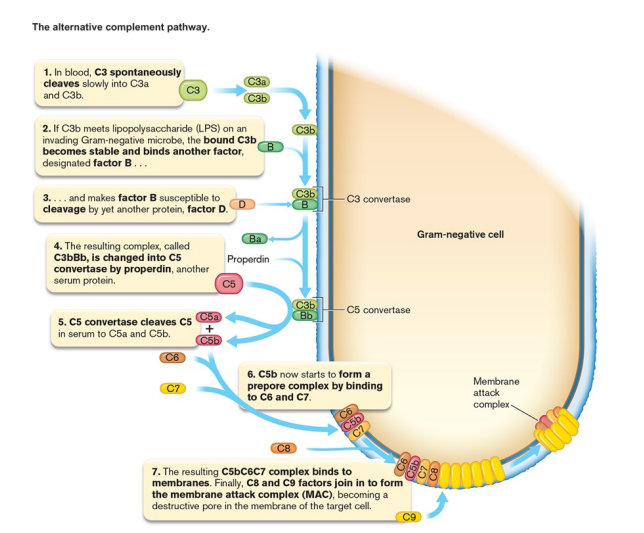
Complement System
serum proteins that can work with or independent of antibodies to kill bacteria
cascade of protein interactions leads to pores forming in bacterial membrane
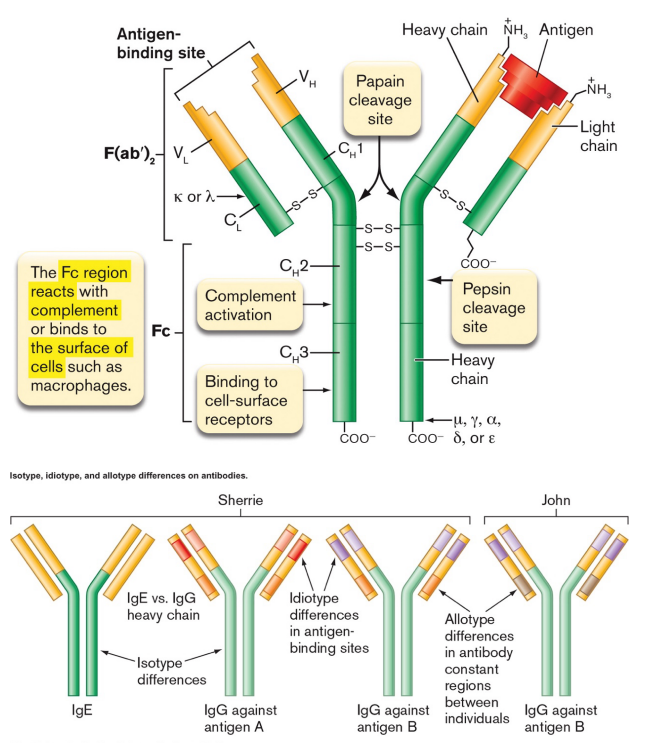
Antibodies
secreted proteins that bind antigen
four polypeptide chains, 2 light & 2 heavy, held together by disulfide bonds
each chain has constant (C) and variable (V) regions
C regions are the same for that individual/chain (allotype) and class (isotype)
i.e., all IgG light chain C regions in an individual are the same
V regions are unique to each antibody (idiotype)
antigen binding domains are formed by V regions of 1 H and 1 L chain
on a given antibody, all binding domains bind the same antigen
antigen=whatever antibody binds to, usually protein (carbohydrate,lipid,DNA)
epitope = the specific part being bound
antigen
whatever antibody binds to, usually protein (carbohydrate,lipid,DNA)
epitope
the part of the antigen the antibody is binding to
five different classes of antibody (in humans)
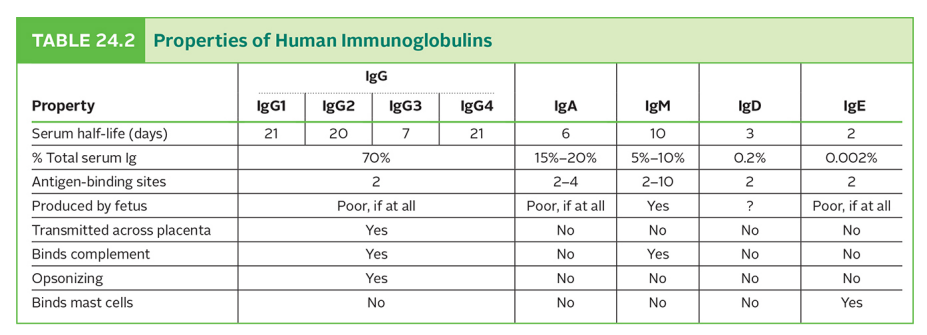
IgG
IgG is bivalent, will bind 2 of the exact same antigen
IgG is found in blood serum
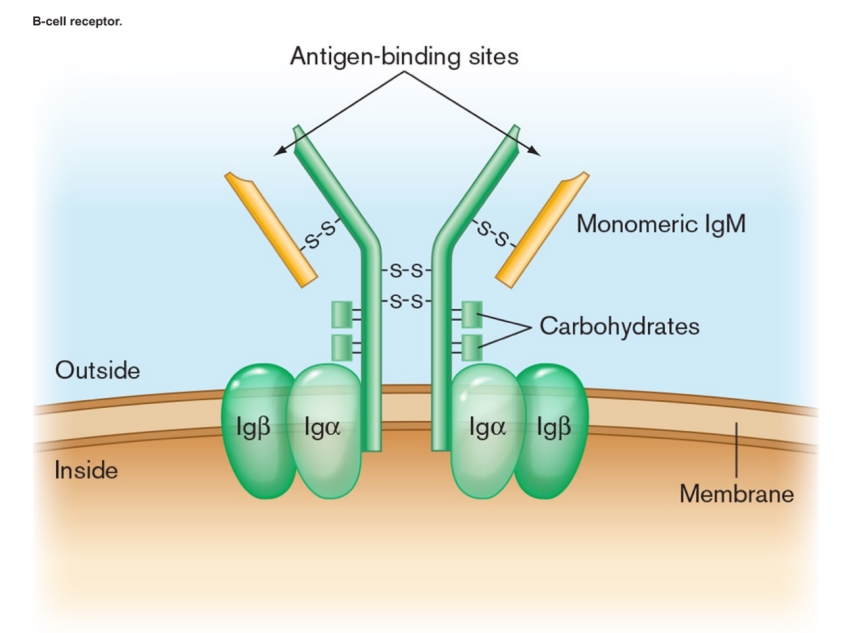
IgM
five antibody proteins held together
longer constant domain
generally the first Ig made in immune response
IgM monomers in B cell membrane bind antigen, help bring it in for presentation
IgA
two antibodies held together
common in body secretions (tears, breast milk, mucus, etc.)
IgE
longer constant domain (has CH4)
binds to mast cells
important in allergic reactions
IgD
helps antigen bind to B cells
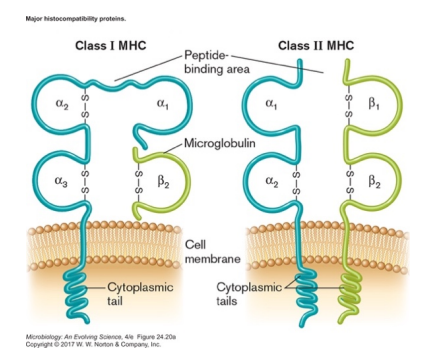
Major Histocompatibility Complex (MHC)
proteins that exist in plasma membrane of host cells
unique to individual, help determine "self" (HLA type)
important in transplant rejection
two types, both will bind and display antigens
binding of antigen depends on shape of two variable regions
Class I and Class II
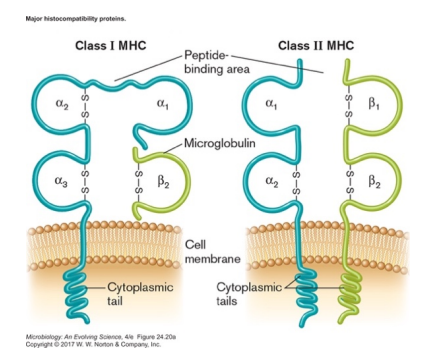
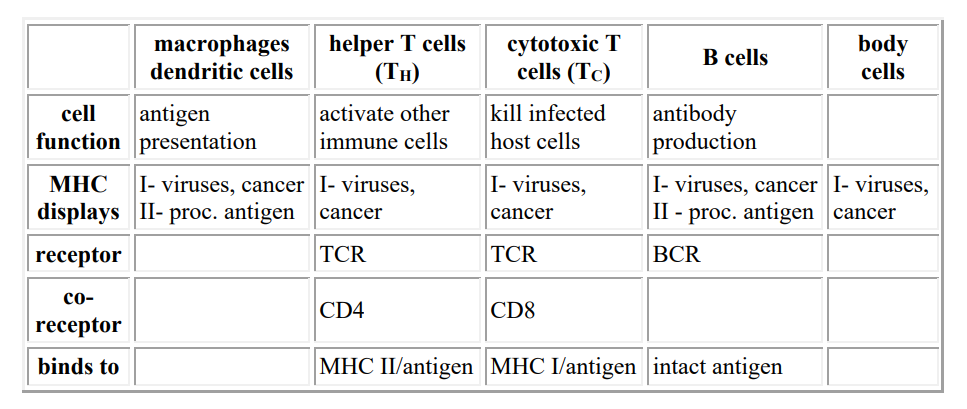
Class I vs. Class II MHC
Class I- all nucleated cells
alerts immune system that cell is infected
Class II- B cells and antigen-presenting cells (APCs)
tells other immune cells that APC has found a foreign antigen
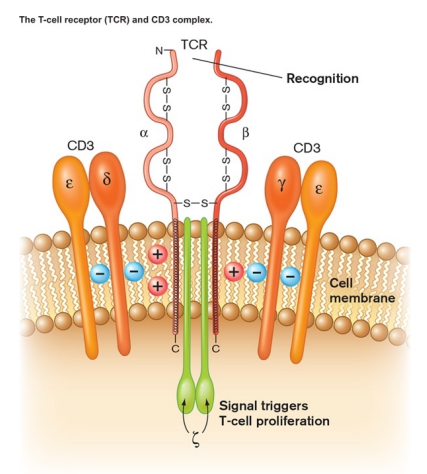
T Cell Receptor (TCR)
is similar to MHC but only found on T-cells
each T cell has roughly 100,000 copies of one particular type of TCR
each type of TCR will bind only one antigen (with limited cross-reactivity to others)
variable region is different in each cell, ensuring a range of TCR binding specificities
B cell receptor and antibodies
antibodies are secreted by activated B cells
BCR has extra domain in tail to insert into membrane
Receptor interactions (chart)
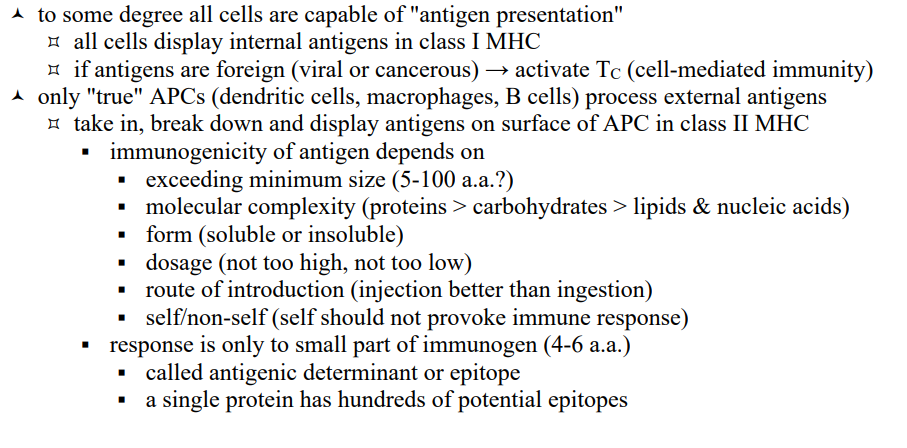
Antigen Presentation
Adaptive Immunity (third line of defense)
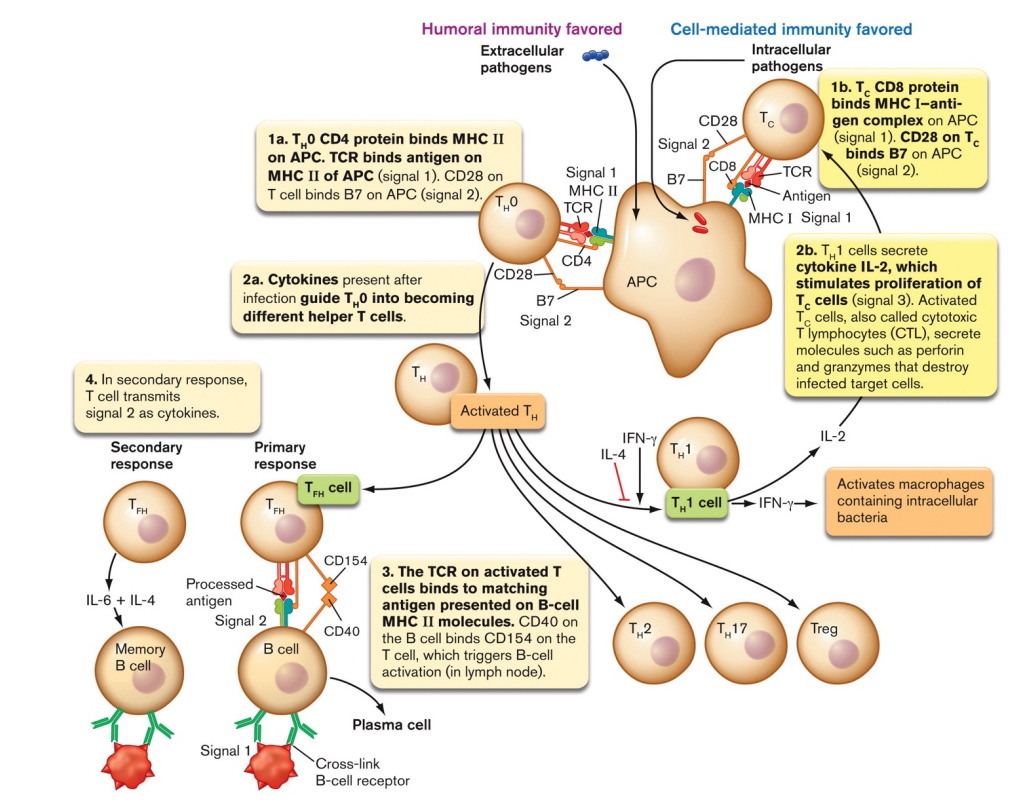
Activation of T-helper (TH0) cells
Adaptive Immunity (third line of defense)
a naive T-helper cell (TH0) recognizes the foreign antigen/class II MHC via its T-cell receptor (TCR) and CD4 co-receptor
binding of B7 & CD28 serves as confirmation signal
APC releases cytokines, triggering development of TH0
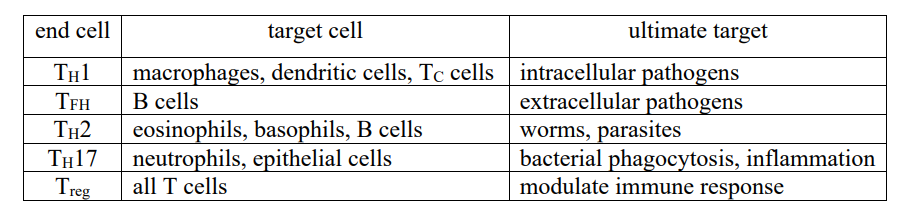
TH0 cells chart
Cell-Mediated Immunity
Adaptive Immunity (third line of defense)
effective against virally infected cells or cancerous host cells
operates via activated cytotoxic T-cells (TC)
TC cell recognizes the foreign antigen/class I MHC on APC via its T-cell receptor (TCR) and CD8 co-receptor
binding of B7 & CD28 serves as confirmation signal
IL-2 secreted by TH1 induces proliferation of TC cells
activated TC kills infected host cells
TC cell recognizes the foreign antigen/class I MHC on infected cell via its T-cell receptor (TCR) and CD8 co-receptor
in this case, no binding of B7 & CD28
signals to TC cell that it is binding to an infected cell, not an APC
binding results in secretion of cell killing proteins
perforin
granzymes
proliferation is selective, i.e., only TC cells with TCR fitting foreign antigen are activated
activation will only occur if APC is also activating nearby TH1
activated TH1 will also bind to macrophages via TCR and secrete cytokines that activate macrophages and promote inflammation
perforin
cell killing proteins - cell mediated immunity
protein which inserts in infected cell membranes, makes pore
granzymes
cell killing proteins - cell mediated immunity
proteins which trigger apoptosis, programmed cell death
Humoral Immunity
Adaptive Immunity (third line of defense)
effective against any pathogen outside a host cell (viruses, bacteria, protists, etc.)
operates via differentiated B-cells
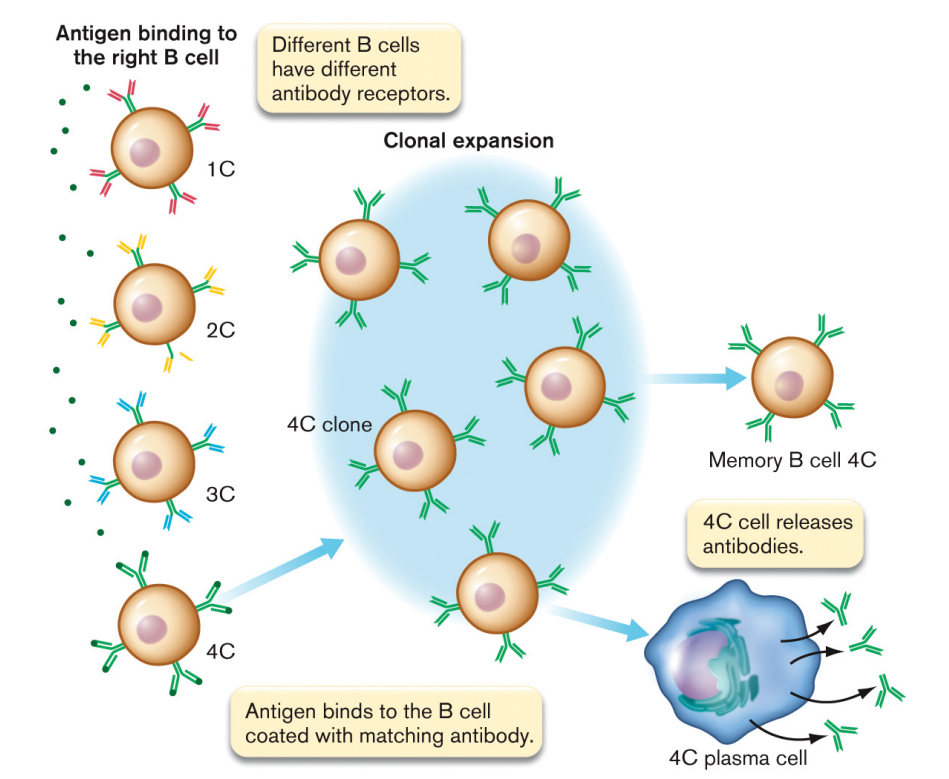
can happen two ways
direct encounter of antigen
antigen binding to B-cell receptor (BCR) causes clustering (capping)
B-cell differentiates into plasma cells (secrete IgM) and memory cells
interaction with TFH/ TH2
Steps in antibody formation (diagram)
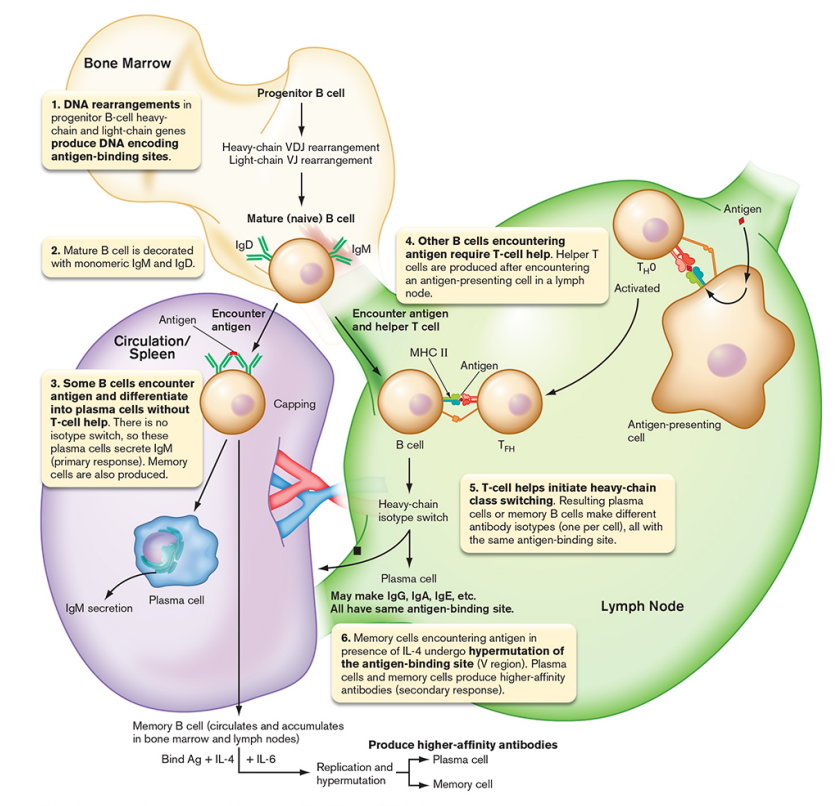
interaction with TFH/ TH2
Humoral Immunity
B cells can act as APCs for antigens bound to its BCR
internalize that antigen and display it in class II MHC
TFH/ TH2 cell recognizes the foreign antigen/class II MHC on B cell via its T-cell receptor (TCR) and CD4 co-receptor
binding of CD154 & CD40 serves as confirmation signal
TFH/ TH2 cell releases cytokines that initiate B cell differentiation
class-switching of heavy chains occurs (all classes possible)
new cells all recognize same antigen (clonal selection)
plasma cells- secrete antibodies
memory cells- long lived
higher number of B cells specific for that antigen after first exposure
don't require TH activation to convert to plasma cells, just binding to BCR
hypermutation of variable region may give even higher affinity antibodies
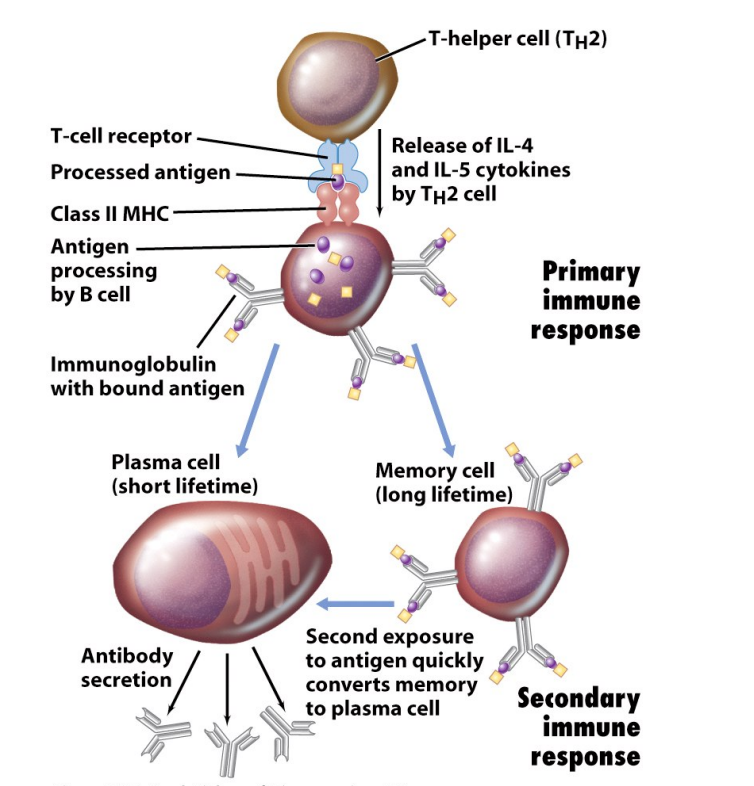
plasma cells
secrete antibodies
memory cells
long lived B cells
don't secrete antibodies
exist to ensure faster, stronger response to second exposure
What can the immune system can do?
respond to anything, even if never encountered before (antibody/receptor diversity)
strengthen its response upon encountering something (clonal proliferation and memory)
discriminate between self and non-self (clonal deletion)
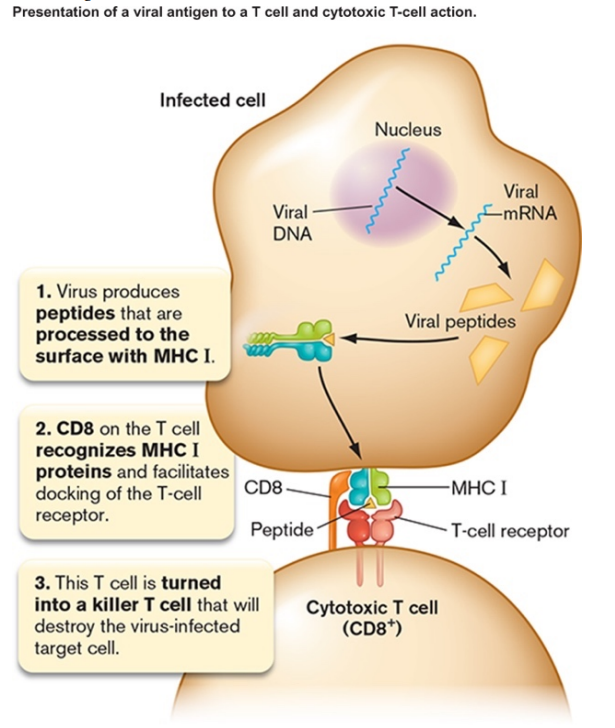
What Happens When a Virus Infects a Person?
Virus enters those body cells with the proper receptor, begins replicating
new viruses are produced → free (extracellular) virus particles
however, some viral antigens will be displayed on surface of infected cell by MHC I
Macrophages and other APCs will engulf free virus particles
APCs typically encounter virus in spleen, lymph node, other specialized tissue
display viral antigens in MHC II and MHC I
A few TH0 cells will have a TCR that fits the combination of MHC II/antigen on APC
TH0 cells bind to APC via TCR and CD4
causes APC to release cytokines, causing that specific TH cell to proliferate
can differentiate into TH1 and/or TH2 depending on cytokines present
in either case, more copies of TH with TCR recognizing that particular viral antigen
activated TH cells will release cytokines as well
Separately, a few TC cells will have a TCR that fits MHC I/antigen on APC
TC cells bind APC via TCR and CD8
activated TH1 cells induce proliferation of that specific TC cell
therefore, more copies of TC with TCR recognizing that viral antigen
TC cells migrate to site of infection
TC cells bind to virally infected cell via TCR and CD8
causes TC cell to release proteins that kill the infected cell
Separately, a few B cells will have a BCR that fits free virus
B cells will endocytose virus bound to BCR and display antigens in MHC II
TH2 cells bind to B cell via TCR and CD4
activated TH2 cell induces differentiation of that specific B cell
plasma cells make lots of antibody specific for that viral antigen
memory cells for that viral antigen are defense against future infection
Eventually, infection is brought under control by
TC cells killing virally infected cell
antibody neutralization of free virus
Reinfection leads to rapid secondary response
Function of Antibodies
Virus or toxin neutralization
bind to viral surface or toxin and prevent intended interaction of virus or toxin with host
Agglutination/Precipitation
clump antigens together
if soluble antigen, may cause it to precipitate
Activate complement system of proteins
antibody bound to bacterial cell surface triggers binding/cleavage of complement proteins
cleaved complement proteins cause inflammation
other fragments of complement proteins insert into membrane
pores form, cell dies
doesn't work for Gram positives
Opsonization
antibodies and complement on cell surface "flag" cell for phagocytosis
works for all bacteria
can also clump cells or toxin molecules leading to easier phagocytosis
Generation of Antibody Diversity
Each B cell produces only one kind of antibody
Ability to respond to anything out there depends on millions of different B cells, millions of different antibodies
diversity is created by uniquely splicing DNA segments in each B cell
Similar processes result in TCR diversity
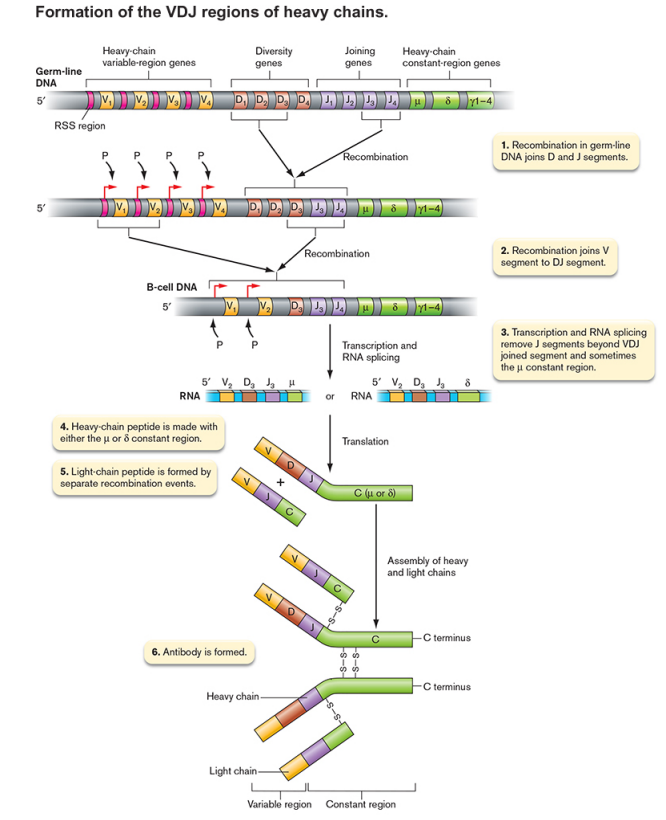
Antibodies are proteins, does this mean there are millions of different antibody genes?
NO, diversity is created by uniquely splicing DNA segments in each B cell
multiply the segments to realize the possibilities
remember that C region determines class, is not involved in antigen binding
320 light chains x 16,200 heavy chains = > 5 million binding specificities
even more variation because of
imprecise joining of segments
high mutation rate during B cell proliferation
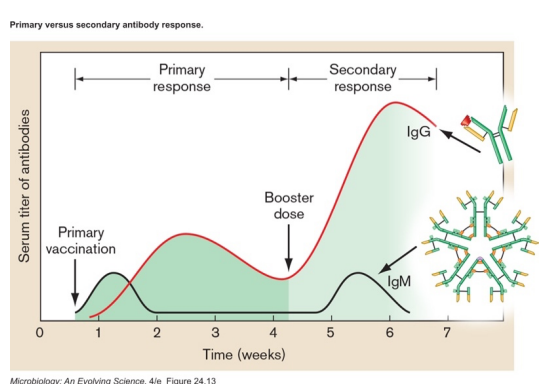
Natural active immunity
disease exposure
infection leads to immune response, boost in memory cells (takes weeks)
second exposure results in stronger, faster response
Artificial active immunity
vaccination
vaccination leads to immune response (takes weeks)
whole organism- killed or attenuated
subunit- natural, modified or recombinant
hapten + carrier molecule- when antigen is too small on its own
second exposure (or booster) results in stronger, faster response
Natural passive immunity
maternal immunity
antibodies are received from mother through placenta, breast milk (instant protection)
no host immune response, no boost for later exposure
Artificial passive immunity
antitoxins
injection of antibodies from another individual or animal (instant protection)
used against toxins
no host immune response, no boost for later exposure
Immune Disorders
Allergies can be an overreaction of the immune system
Autoimmune diseases- the immune system attacks self-antigens
Superantigens can activate T cells indiscriminately and destabilize the system
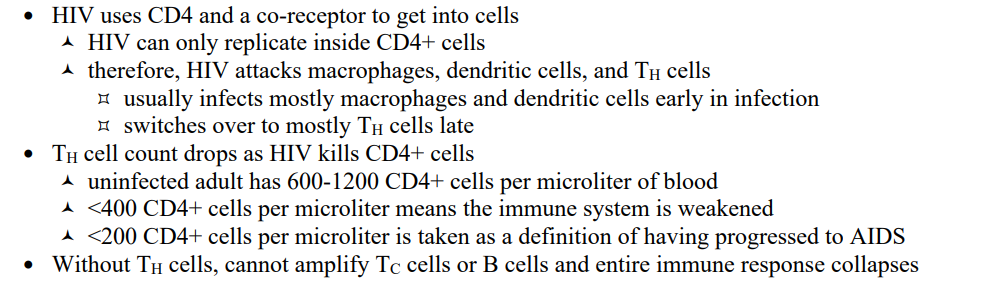
The devastating effect of HIV
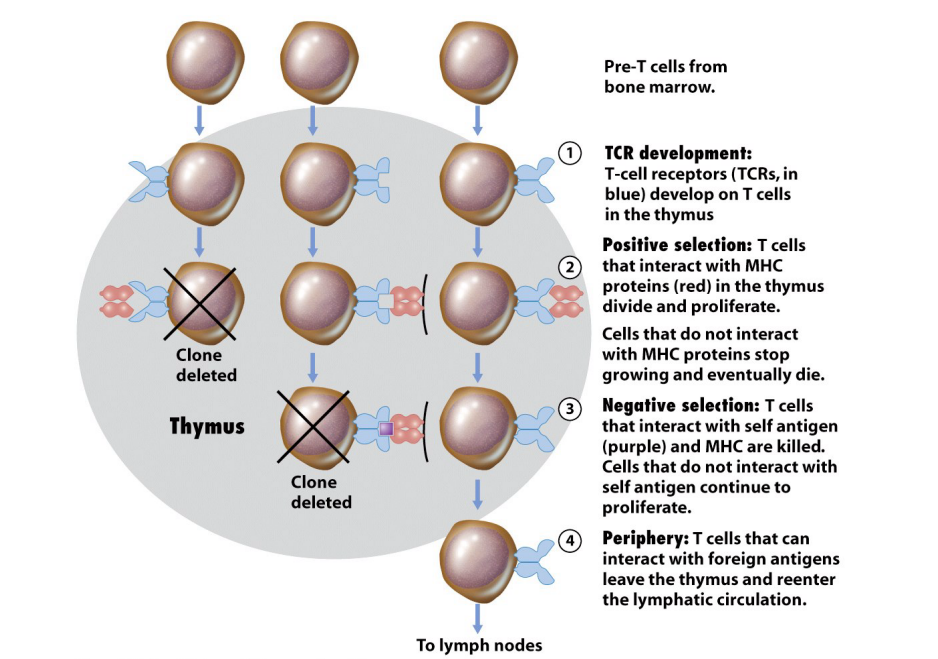
Clonal Selection in recognition of self and non-self
Each B & T cell makes a unique antibody or TCR
When binding to antigen, proliferation occurs
a clonal line is expanded
descendent cells produce identical antibody or TCR (except for mutation)
During embryonic/neonatal development, those B & T cells that bind antigen (presumed to be self) are deleted
B cells mature in bone marrow; T cells mature in thymus
it is thought even in adults, those tissues are kept free of "new" antigens
if maturing cell does not react with MHC, it dies
if maturing cell does react with antigen, it dies
clonal line expansion diagram
What is critical to effective treatment?
Identification by Microscopic Observation
Staining/morphology is rarely definitive (for bacteria)
however, the appearance of some organisms in conjunction with symptoms and location sampled can often be presumptive (enough to start treatment)
Specialized staining techniques can highlight microbes in tissue figure
Identification by Growth and Biochemical Tests
Proper plating/media
media should be enriching, if not selective
failing that, a differential medium can distinguish between species
must maintain temperature and oxygen conditions
Identification by metabolic fingerprint, the results of multiple biochemical tests
based on flow charts for identification
now worked into strips/kits
or even automated
Immunological Methods Overview
Current infection can be detected by using lab antibodies to detect antigen in patient
Past infection can be inferred by detecting patient antibodies in blood using lab antigen
antibody titer can be a signal of time of infection
draw blood, spin out cells
dilute serum by factors of 2
look for reaction against lab antigen
Precipitation/Agglutination
Immunological Methods of Detection
at equal concentrations of antibody and antigen, bridging will occur
will precipitate soluble antigen and agglutinate (clump) cells
is the basis for blood typing
allows rapid detection of some infectious agents (or specific strain for epidemiology)
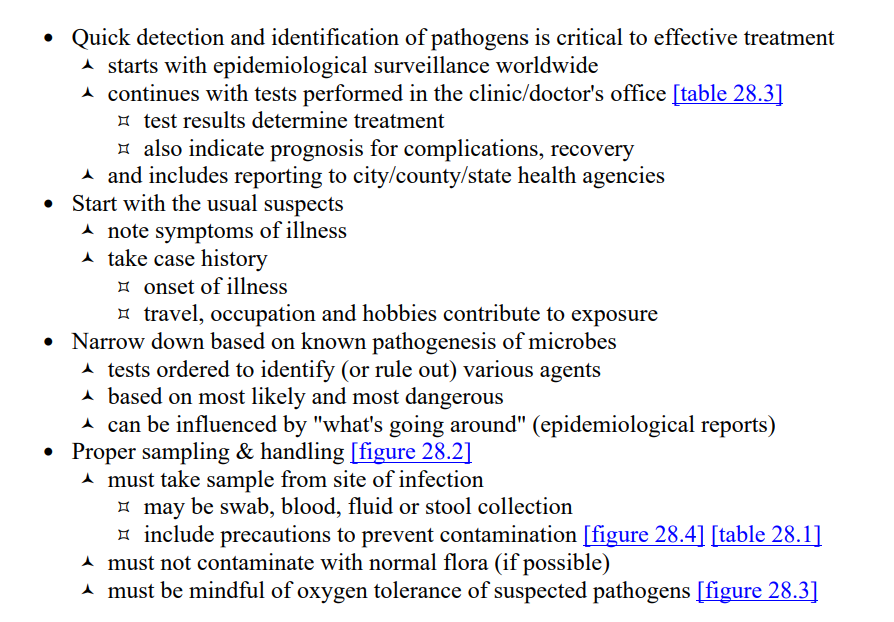
Fluorescent Microscopy Direct Method
Immunological Methods of Detection
Useful in identifying cells
This method tests for antigen in patient
antibodies are conjugated to fluorophore
conjugated antibodies are allowed to bind to cell suspension from patient
will bind if antigen is on cell surface
can be examined by light microscopy
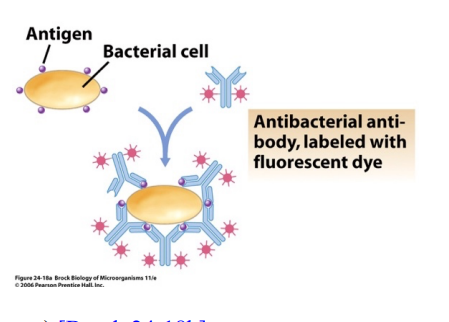
Fluorescent Microscopy Indirect Method
Immunological Methods of Detection
Useful in detecting past exposure
This method tests for antibodies in patient serum (past exposure)
serum from patient is collected
serum is mixed with test antigen
if antibodies present, will bind cells
if not, serum is washed away
secondary antibody with fluorophore added to cells
2º ab must be from other species
2º ab binds to any ab from 1st species in Fc region
e.g., 2º ab = rabbit anti-human IgG
can be examined by light microscopy
Use of 2º ab saves time & trouble adding fluorophore to serum antibodies; labeled 2º ab binds to many different serum ab
Fluorescent Microscopy
Immunological Methods of Detection
direct method (useful in identifying cells)
indirect method (useful in detecting past exposure)
can be used in combination with a cell sorter (FACS machine)
laser activates fluorescently labeled cells (labeled antibody bound to surface antigen)
charge difference is used to separate cells
Immunoelectron Microscopy
Immunological Methods of Detection
antibodies are conjugated to gold bead
conjugated antibodies allowed to bind to cell section
will bind wherever antigen is
Enzyme-Linked Immunosorbent Assay (ELISA)
Immunological Methods of Detection
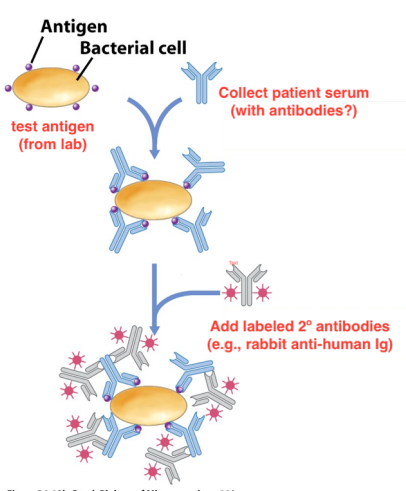
direct ELISA- tests for antigen (antigen capture)
indirect ELISA-tests for antibody
detection based on colorimetric enzyme reaction
because of enzyme, more sensitive than fluorescent methods
must conjugate enzyme to constant region of antibody
amazingly, does not affect antibody binding or enzyme activity
direct ELISA
Immunological Methods of Detection
Tests for Antigen (Antigen Capture)
unconjugated antibody stuck to well
antigen allowed to bind
enzyme conjugated antibody then added
color based reaction carried out
strength of color depends on how much antigen bound
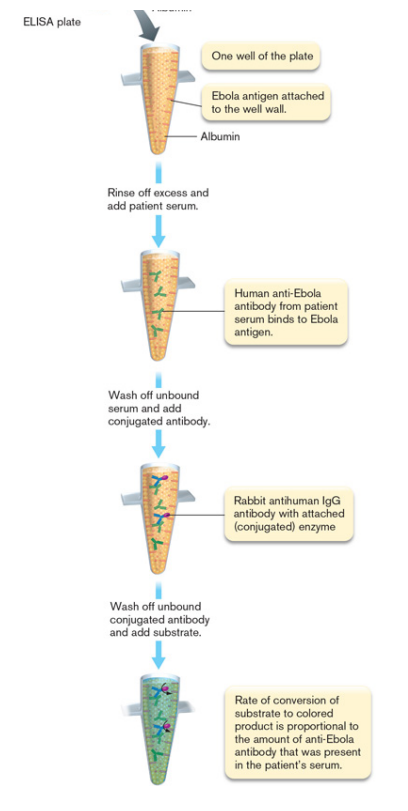
indirect ELISA
Immunological Methods of Detection
Tests for antibody
antigen stuck to microtiter well
serum from patient passed over
if antibodies present, will bind antigen
if not, serum is washed away
enzyme-conjugated 2º antibody added
example- 2º ab = rabbit anti-human IgG
color based reaction carried out
strength of color depends on how antibody titer in patient serum
Immunoblot (Western blot)
Immunological Methods of Detection
run proteins out on gel
blot proteins onto membrane
add unlabeled (primary) antibodies for specific protein
add enzyme-conjugated (secondary) antibodies against first antibodies
reaction will occur where antibody is bound
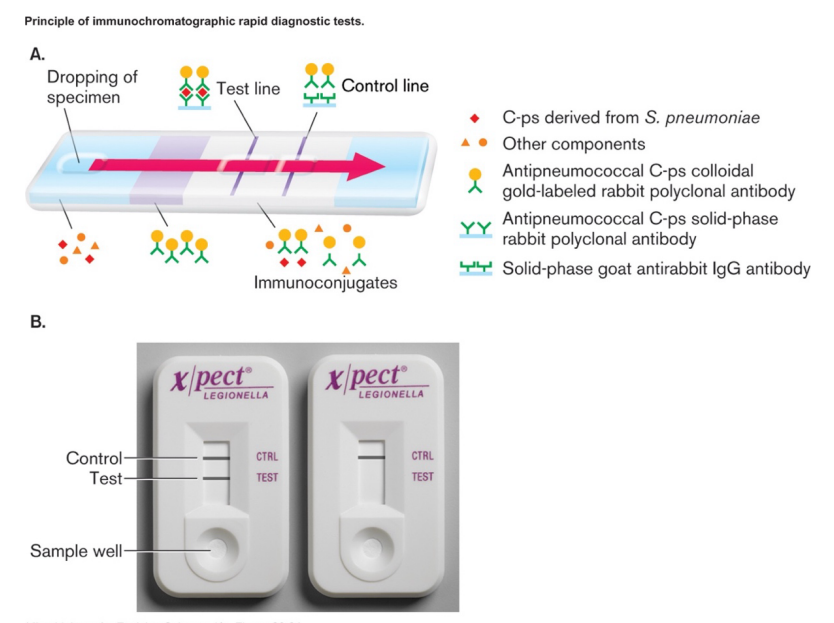
Antibody-based rapid detection methods
Immunological Methods of Detection
advantage- fast, no culturing required, immediate treatment based on result
disadvantages- false positives and negatives, no information about antibiotic resistance
blood, sputum or urine (with antigen) added to one end of filter strip
capsular protein from Streptococcus pneumoniae in example above
beta subunit of human chorionic gonadotropin in pregnancy test
spike or nucleocapsid protein for rapid Covid tests
capillary action carries fluid through region with labeled-antibody for particular antigen
labeled antibodies are mobile
will be carried along by fluid (with or without antigen binding)
are from species 1 (rabbit in the example above)
fluid passes line of immobilized antibodies for antigen
labeled antibodies will stop on test line if bound to antigen
fluid passes on to second line, immobilized antibodies for species 1
must be from second species (goat in above example)
serves as control, to ensure labeled antibodies were carried past test line
PCR
Nucleic Acid Methods (NAAT = Nucleic Acid Amplification Tests)
use primers for distinctive genes
size of fragment can indicate species and strain, antibiotic resistance
can be multiplex, i.e., include primer pairs for multiple genes
sensitive and fast (no culturing)
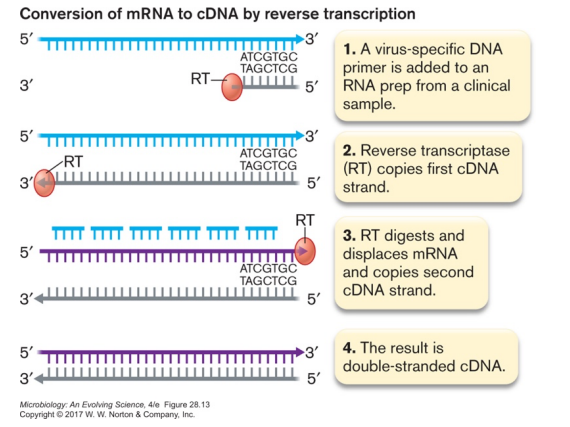
RT-PCR
Nucleic Acid Methods (NAAT = Nucleic Acid Amplification Tests)
Used to detect RNA from pathogen, especially for RNA viruses (Covid tests)
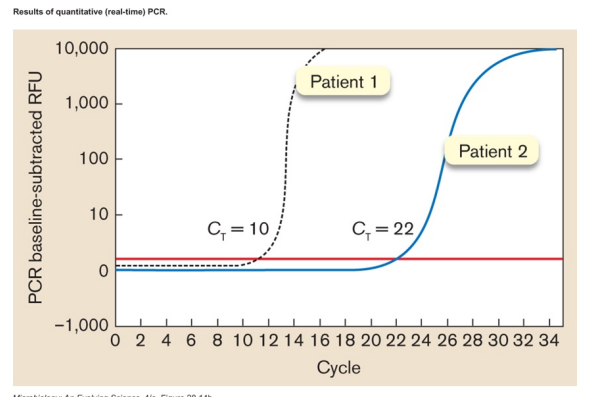
qRT-PCR
Nucleic Acid Methods (NAAT = Nucleic Acid Amplification Tests)
follow increase in product, tells you how much starting template there was
can track viral loads during infection
Tests for SARS-CoV-2 (chart)
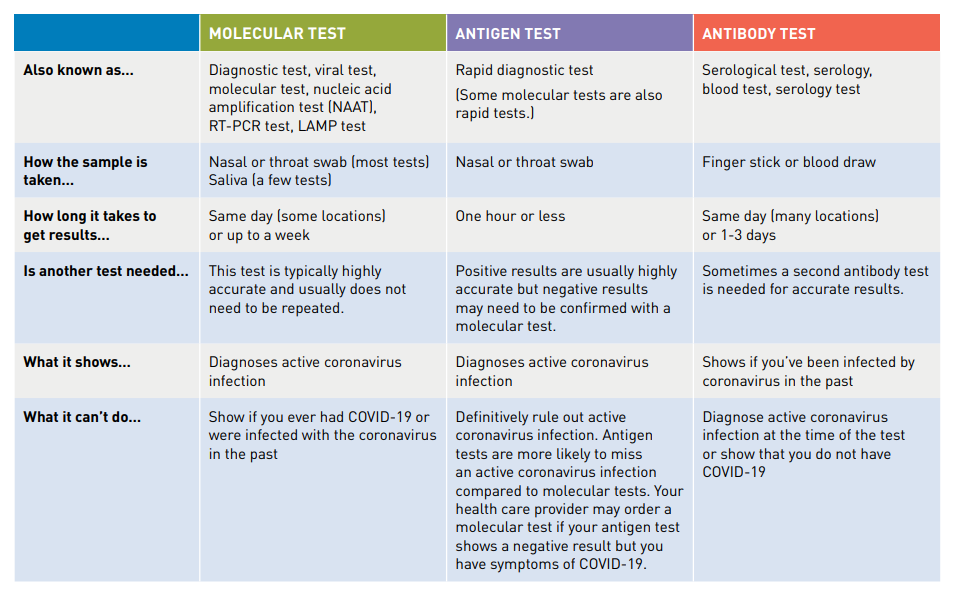
Diagnostic tests for SARS-CoV-2
Detect current infection
Antibody tests for SARS-CoV-2
Detects past infection (at least 2 weeks ago)
starts with a blood sample
detects IgM and/or IgG specific for the virus
may help determine when person was infected or if they can donate plasma
may provide data for epidemiological models
if not specific enough (cross-reacts with cold viruses), false positives a problem
Antibiotics
Antimicrobial compounds produced by microbes
source is typically fungi or soil bacteria
Exhibit selective toxicity
antibiotic must target something unique about pathogen
May also have side effects
typically = allergies, stomach upset, diarrhea, kidney and/or liver damage
side effects are dosage dependent
Effective range varies
drugs can be broad or narrow spectrum in terms of effectiveness against pathogens
may kill pathogen (bactericidal) or limit its growth (bacteriostatic)
Commercial antibiotics can be natural, synthetic or semi-synthetic
Commercial antibiotics can be natural, synthetic or semi-synthetic
growing the organism & purifying the drug (at scale) can be technical challenges
took ~ 15 years from discovery to introduction of penicillin
first successful treatment of systemic infection (1942) used half available supply
within two years, was being mass-produced
best source strain = isolate from moldy cantaloupe in Peoria IL
growth medium = corn steep liquor
deep tank fermentation resulted in best yields
how to introduce oxygen without contaminating the culture
natural drugs are often modified
natural penicillin is rapidly excreted
probenecid given with penicillin to outcompete penicillin excretion
synthetic penicillin makes this unnecessary
Modes of antibiotic administration
oral- must be acid tolerant, well absorbed
topical- typically only for superficial infections
injection- most direct, but also most difficult
Antibiotic Resistance
a predictable evolutionary result
selection for resistance increases their numbers
horizontal gene transfer spreads resistance genes
we should limit indiscriminate antibiotic use
an increasing problem, especially in hospitals
need to find new drugs or modify old ones
determinizing effectiveness
Kirby-Bauer method
Minimum Inhibitory Concentration (MIC)
Mechanisms of Antibiotic Resistance
reduced permeability of cell envelope
alter pore proteins (for hydrophilic antibiotics)
alter membrane lipids (for hydrophobic antibiotics)
efflux pumps to transport drug out
may add on to existing transport systems
inactivate antibiotic
by cleaving it
by modifying it
mutate target of action
avoid/alter target pathway
Kirby-Bauer method
Antibiotic resistance determinizing effectiveness
uses disk diffusion method
compare diameter of zone of inhibition to standard
must maintain consistency of medium, temperature, etc.
Minimum Inhibitory Concentration (MIC)
Antibiotic resistance determinizing effectiveness
determine by dilution or test strip
in vivo levels don't match in vitro tests
Steps in peptidoglycan synthesis
Cell Wall Synthesis
synthesis of NAG & NAM-peptide precursors
transport across cytoplasmic membrane by bactoprenol
polymerization into existing wall by transglycosylases
cross-linking chains by transpeptidases
Beta-lactam antibiotics
Antibiotic - Cell Wall Synthesis
examples- penicillin, cephalosporin
mechanism- resembles D-ala dipeptide, competes for binding to transpeptidase
used against- Gram-positives, some Gram negatives (OM limits access to wall)
resistance- enzymes which break down antibiotic
Vancomycin
Antibiotic - Cell Wall Synthesis
mechanism- binds to peptides, interferes polymerization and cross-linking
used against- Gram positives, drug of last resort
Cycloserine
Antibiotic - Cell Wall Synthesis
mechanism- interferes with formation of D-ala dipeptide
used against- Mycobacterium
Bacitracin
Antibiotic - Cell Wall Synthesis
mechanism- interferes with bactoprenol, peptidoglycan subunit transfer
used against- Gram positives
Gramicidin
Antibiotics - Membrane Integrity
a cyclic peptide with D and L amino acids
mechanism- inserts into membrane, creates pores
Polymixin
Antibiotics - Membrane Integrity
polypeptide
mechanism- acts like detergent to disrupt cytoplasmic membrane
used- topically (also disrupts human cell membranes)
Daptomycin
Antibiotics - Membrane Integrity
non-ribosomal peptide (i.e., an enzyme, not ribosome, links amino acids together)
mechanism- forms ion channel
Quinolones
Antibiotics - DNA Synthesis and Structure
examples- nalidixic acid, ciprofloxacin
mechanism- interfere with DNA gyrase
used against - broad spectrum