Basic Principles of Pharmacology
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
What is pharmacodynamics vs pharmacokinetics?
- pharmacodynamics: what the drug does to the body
- pharmacokinetics: what the body does to the drug
what is pharmacotherapeutics?
- use of drugs to prevent and treat diseases
- indication as to why you are using the drug
what is posology?
- science of drug dosing
what is a drug?
- a medicine or other substance which has a physiological effect when ingested or otherwise introduced into the body
what is a receptor?
- binding site w/ biological effect
what is affinity?
- potential for drug-receptor binding
- some drugs really want to bind to a receptor, but some drugs do not, doses are adjusted accordingly
- how well a drug binds to a receptor
what is Intrinsic activity?
- capacity to produce (vs inhibit) a biological effect
- basically means how well the drug activates the receptor once it is bound
what is intrinsic activity also called?
- efficacy
what is an agonist?
- substances that stimulate a receptor to produce a physiologic reaction
what is an antagonist?
- substances that oppose or interfere with the activity of a receptor and its endogenous substrate without producing a physiologic effect itself
which have both affinity and intrinsic activity, agonist or antagonist?
- agonist
which has only affinity but no intrinsic activity, agonist or antagonist?
- antagonist
what is specificity?
- ability to act at a specific receptor
what happens when a drug has low specificity?
- it binds everywhere
- low specificity drugs cause lots of side effects
ex: antihistamines
what is selectivity?
- the tendency to act on more than one specific receptor
- how much more strongly a drug acts on one receptor compared to another
What is EC50?
- Concentration of drug that produces 50% of maximal response
- in vitro
what is ED50?
- 'effective' dose to illicit a 50% response (in vivo)
what is maximum dose?
- minimum amount of drug producing maximum therapeutic effect
- sometimes called ED95 on graph
what is potency?
- biological response to a given dose
- C has the highest potency out of all of the others
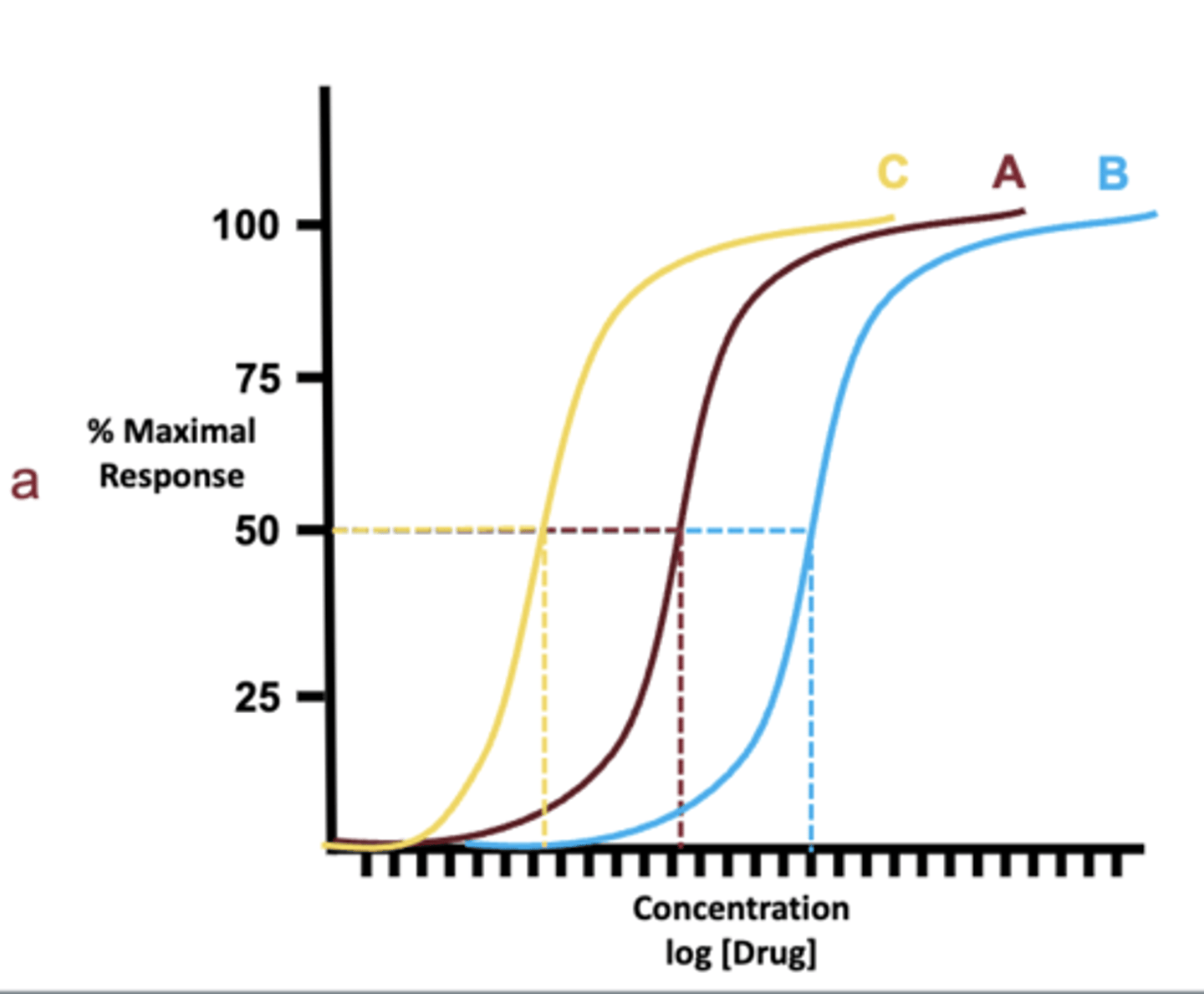
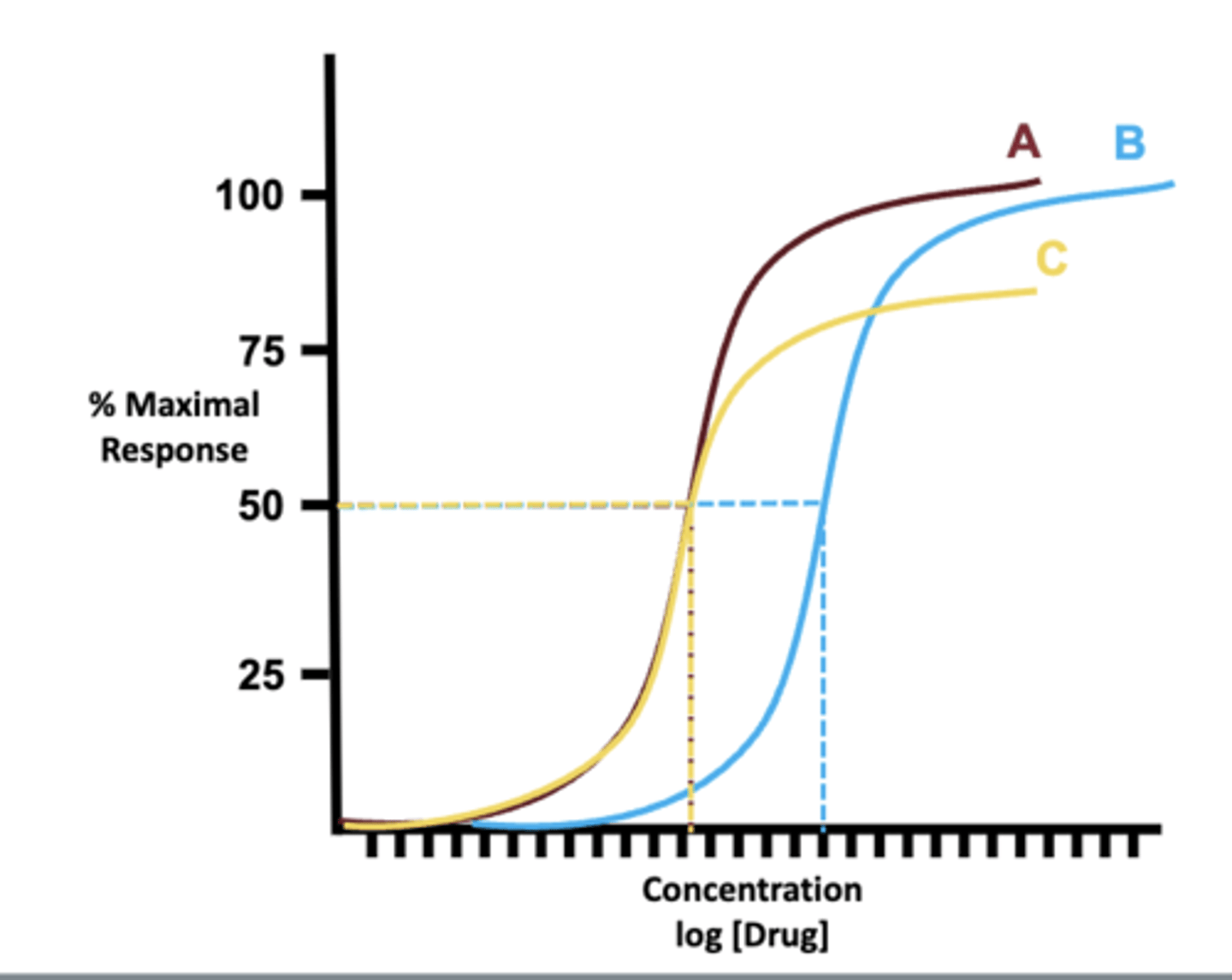
what is efficacy?
- the ability of a drug to produce a maximum response
- A and B have the equivalent efficacy, C has the lowest
- A is also more potent compared to B
what is toxicity?
- the degree to which a substance can harm humans or animals
what is therapeutic index?
- TD50 / ED50
is higher or lower therapeutic index better?
- high
- on graph, further away from each other is better.
what is IC50?
- 'inhibitory' concentration is needed to inhibit, in vitro, a given biological process or biological component by 50%
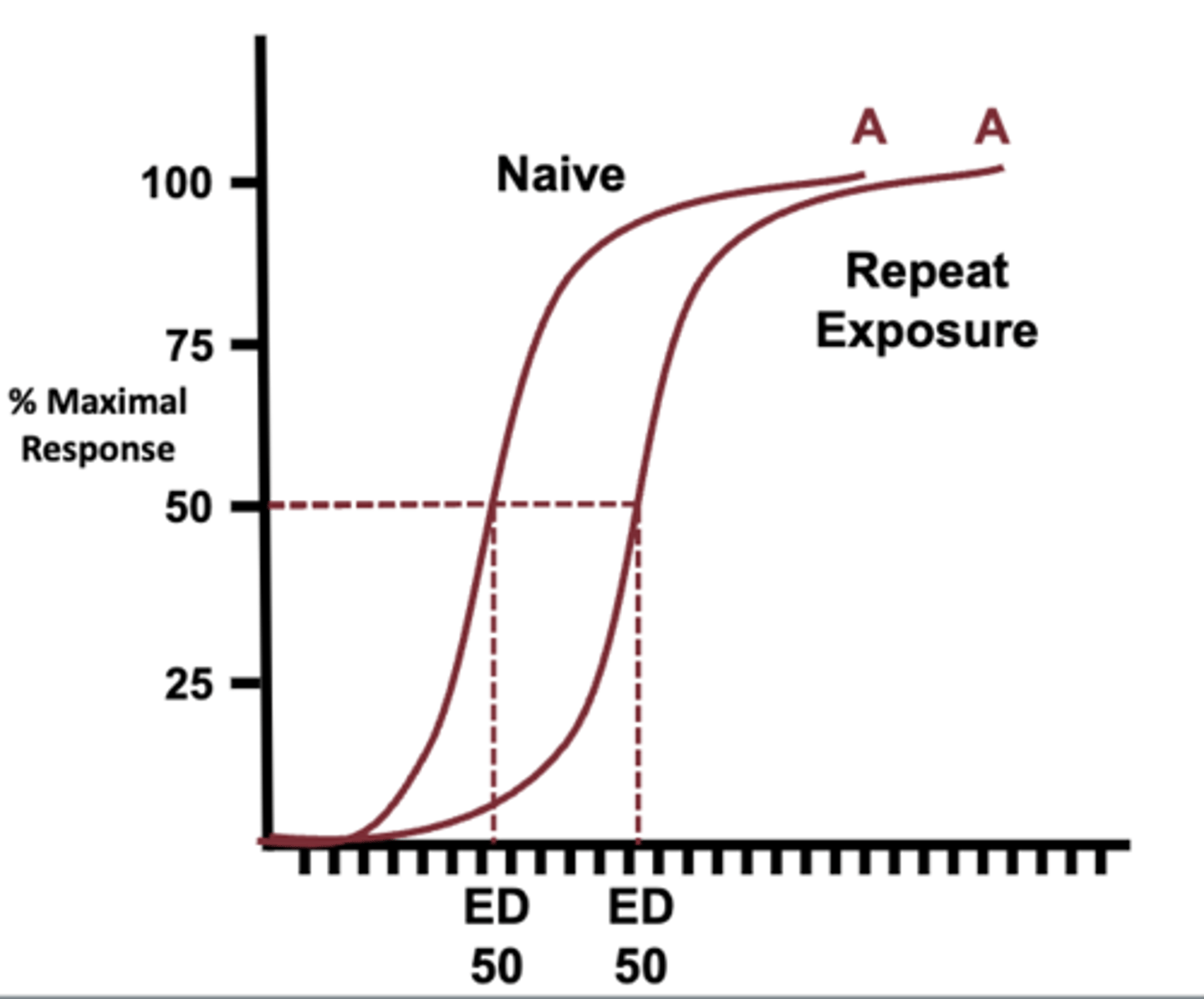
what is tolerance?
- a decrease in response to a drug that is used repeatedly
- can be overcome by increased concentration
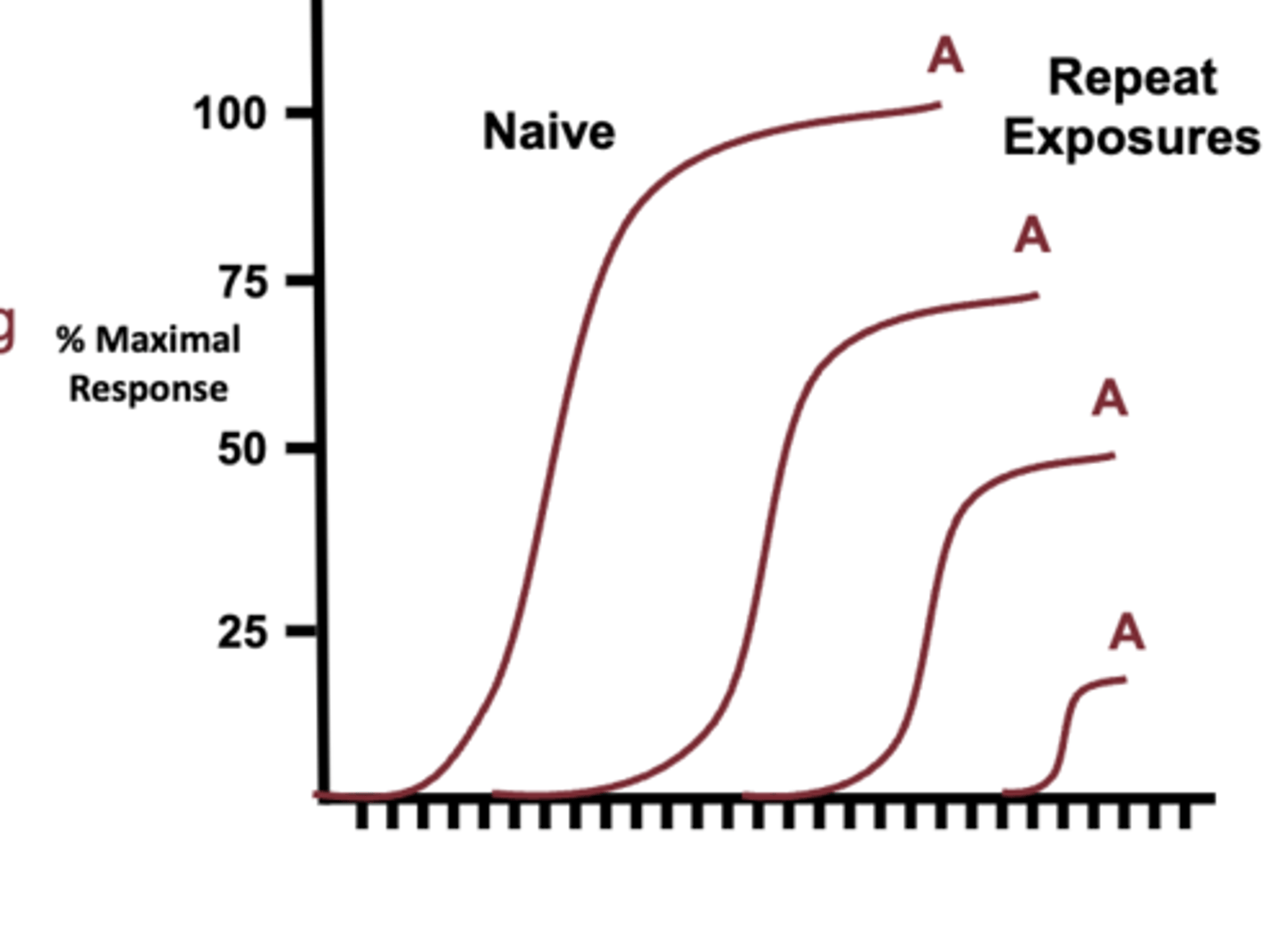
what is Tachyphylaxis?
- rapidly decreasing therapeutic response, cannot be overcome by increased concentration
what are the types of receptors?
A. Ligand-gated ion channels
B. G protein-coupled receptors (most common in ocular pharm)
C. Enzymatic
D. Calcium Release
E. Nuclear
what are the different modes of action for agonist?
−Direct
−Indirect
−Mixed
−Inverse
−Partial
what is a direct agnost?
- binds directly to the binding site and activates it
- ex: phenylephrine
what is an indirect agnost?
- does not bind to binding site
- causes release of something that does bind to the binding site
- ex: cocaine, causes release of norepinephrine to bind to alpha one receptor
what is a mixed agonist?
- it can be an agonist or an antagonist depending on the concentration in the body
- ex: tamoxifen
What is an inverse agonist?
- Agonist that binds to the same site as an agonist however produces an opposite response
- ex: antihistamines
What is a partial agonist?
- A drug that binds to its receptor but produces a smaller effect at full dosage than a full agonist
- used to reduce dependency on a drug
how can antagonist be classified?
- binding integrity
- binding site selectivity
- mode of action
what are the type of binding integrity of antagonist?
- reversible
- irreversible
what are the types of binding site selectivity of antagonist?
- competitive
- non-competitive (allosteric)
- Uncompetitive (allosteric binding in presence of substrate slows ligand dissociation and response rate)
what are competitive antagonist?
- antagonist that bind to the receptor site of the agonist
What is a non-competitive antagonist?
- A non-competitive antagonist binds to a different receptor (allosteric) and causes the receptor of the agonist so it can no longer bind
- can be either reversible or irreversible
- if irreversible, then there is formation of covalent bonds at the receptor
what is an uncompetitive antagonist?
- uncompetitive antagonist are unable to bind to allosteric site until there is an agonist that is bound, once agonist is on receptor, it binds and locks agonist in so other agonist can not bind to the receptor
- usually reversible
what are the different modes of action of antagonist?
- biological
- chemical
- physiological
what is ADME?
- absorption
- distribution
- metabolism
- excretion
what influences a medications ability to get absorbed?
- first pass metabolism
- barriers: degree of vascularity at site of administration
- patient age, gender, weight, pregnancy, health
what is distribution influenced by?
- Volume of Distribution (Vd) = dose/[drug in plasma]
− Influenced greatly by route of administration
what is metabolism influenced by?
− Reflected by drug half life
− Influenced greatly by health of metabolizing organ(s)
what is elimination?
− Routes may include fecal, urinary, sweat, respiration and saliva
− Drug clearance = [drug volume eliminated] ÷ [time]
what is the volume of the tear film?
- 10 microliters
what is the max surface volume of the tear film?
- 30 microliters
what is the volume of a drop of medication?
- 25-50 microliters
what are the three layers of the tear film?
- Lipid, aqueous, mucin
where is most of a drop of medication eliminated in the eye?
- 80% is eliminated in the nasolacrimal drainage with first 2 minutes
what is done to help reduce elimination of a drop of medication?
- punctal occlusion
what kind of medication can pass through the corneal epithelium?
- epithelium has tight junctions, which are barriers to drugs (helps to keep bacterial/infection out)
- barrier to hydrophilic drugs
- favors absorption of lipophilic
what must a drop of medication be to absorbed by corneal epithelium?
- lipophilic
- small
how does the cornea play a role in the pharmacokinetics of a medication?
- major barrier to ocular penetration
- major site of absorption for topical drugs
- corneal esterase metabolizes lipophilic prodrugs
- reservoir (distribution)
epithelium: lipophilic
stroma: hydrophilic
how do larger/hydrophilic molecules get absorbed in the eye?
- get absorbed through conjunctiva or sclera
- less than 20% of drug passage to iris and ciliary body due to high vascularization and blood vessels
what percentage of medication reaches the anterior chamber?
- 1-7%
- cornea is a good barrier
how often is the aqueous recycled?
- about every 50 minutes, especially hydrophilic drugs
- aqueous humor = 200 microliters
how does the iris affect pharmokinetics?
- pigment granules of the iris epithelium absorb light and also can absorb lipophilic drugs
- tropicamide is a lipophillic drug, patients with darker iris are dilated less bc the pigment granules absorb more
- most anti-cholinergics are lipophillic
who dilates easier blue or brown eyes?
- blue eyes bc there is less pigment for the medication to attach onto
does the crystalline lens act as a barrier to medication?
- yes, especially to hydrophilic and large molecules (hydrophobic barrier meaning it does not allow hydrophilic in and allows hydrophobic)
- prevents drug penetration from anterior chamber to posterior chamber
(we do not want things to reach the posterior chamber and the vitreous is mainly made up of water)
- lens epithelium is hydrophobic/lipophilic, this is significant bc some of the lens absorbs steroids leading to PSC.
how would you get medication into the posterior chamber?
- injections
what part of the eye is the blood-aqueous barrier?
- ciliary body
- entry point for systemic drug
- primary drug metabolism site major ocular source of drug metabolizing enzymes
what is the role of the vitreous in medication?
- can serve both as a major reservoir (distribution) for drugs and as a temporary storage depot
• Elimination −anterior chamber−choroid
what is the outer blood retinal barrier?
- tight junction complexes (zonula occludens) in the RPE
what is the inner blood retinal barrier?
- capillaries of the retina are lined by continuous, close-walled, endothelial cells
- helps prevent blood from leaking, but also does not let medications leave
what is the function of the blood retinal barriers?
- barrier to metabolites and toxins and is effective against most hydrophilic drugs
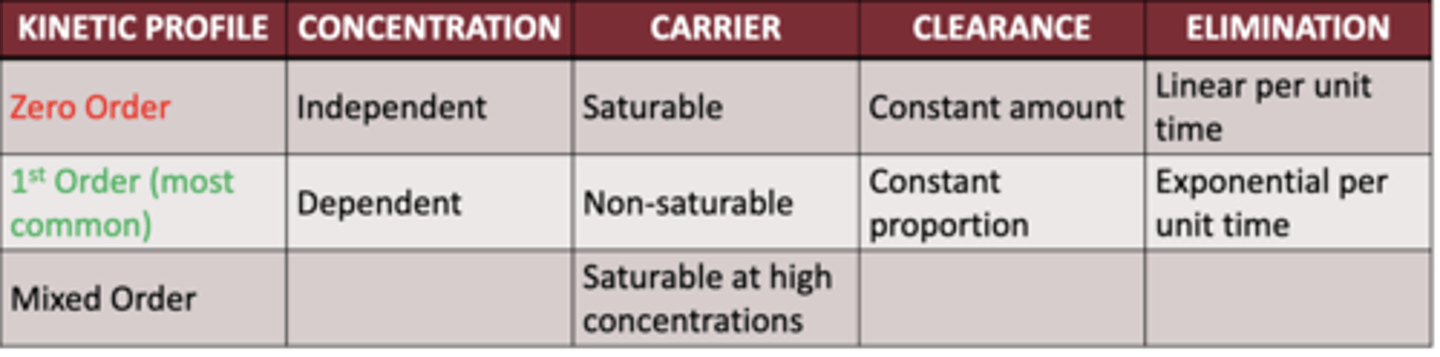
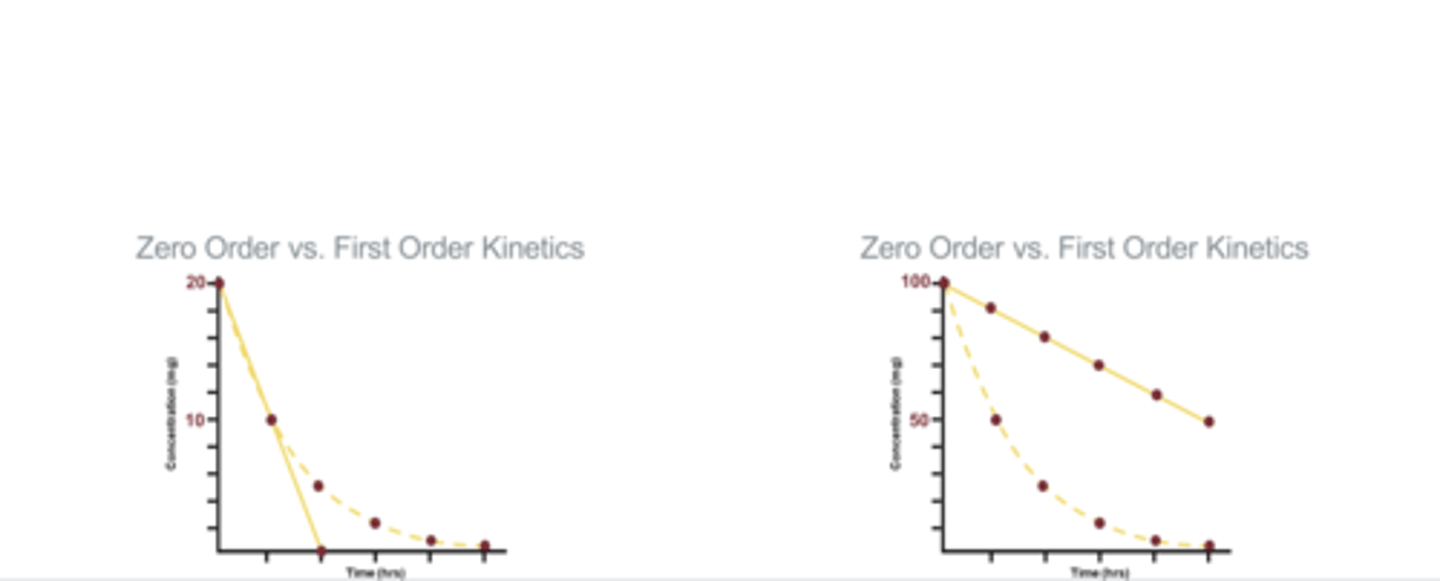
when would zero order kinetics be more advantageous for a medication when compared to first order?
- when there is a small dosage of the drugs
- eliminates at a constant rates
when would first order kinetics be more advantageous for a medication when compared to zero order?
- when there is a large amount of the drug
- left is low dose
- right is high dose
is alcohol consumption first or zero order kinetics?
- zero, there is a fixed rate at which we can eliminate alcohol
- reason as to why we get drunk
what is posology based off?
- first and zero order kinetics
what is a steady state of a drug?
- first order kinetics
- achieved when rate of intake equals rate of elimination
- the rate of elimination depends on the concentration of the drug
how does zero order kinetics affect dosing schedules?
− Greater demand for dose modification: loading vs maintenance
− Doubling a dose calls for twice the time to be metabolized
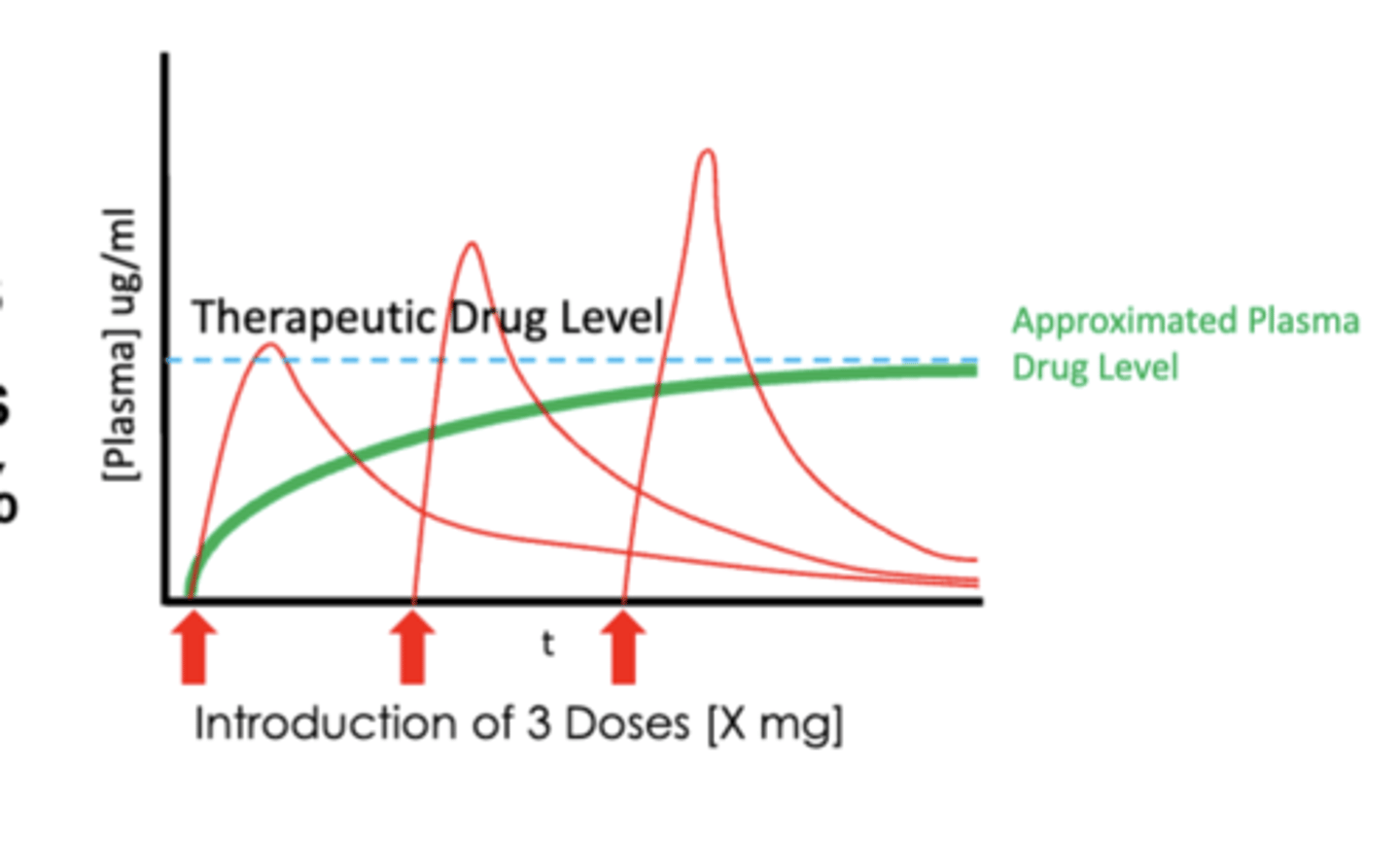
what must be done in order to achieve a steady state?
- Dosing intervals need to achieve a steady state
• The steady state must approach the therapeutic drug level for the given condition
• Adjustments may be required to dosing frequency
• To reach new therapeutic levels
• To improve compliance
- in this picture, after the first dose, it temporarily reaches a therapeutic level, but then decreases due to elimination
- additional doses are needed to maintain steady states
what would be done if an increase in therapeutic level in needed to treat a disease?
- increase the concentration, increase in dosing is not needed
- increase frequency of dosing, keep concentration the same
- in some cases, certain concentrations are not available
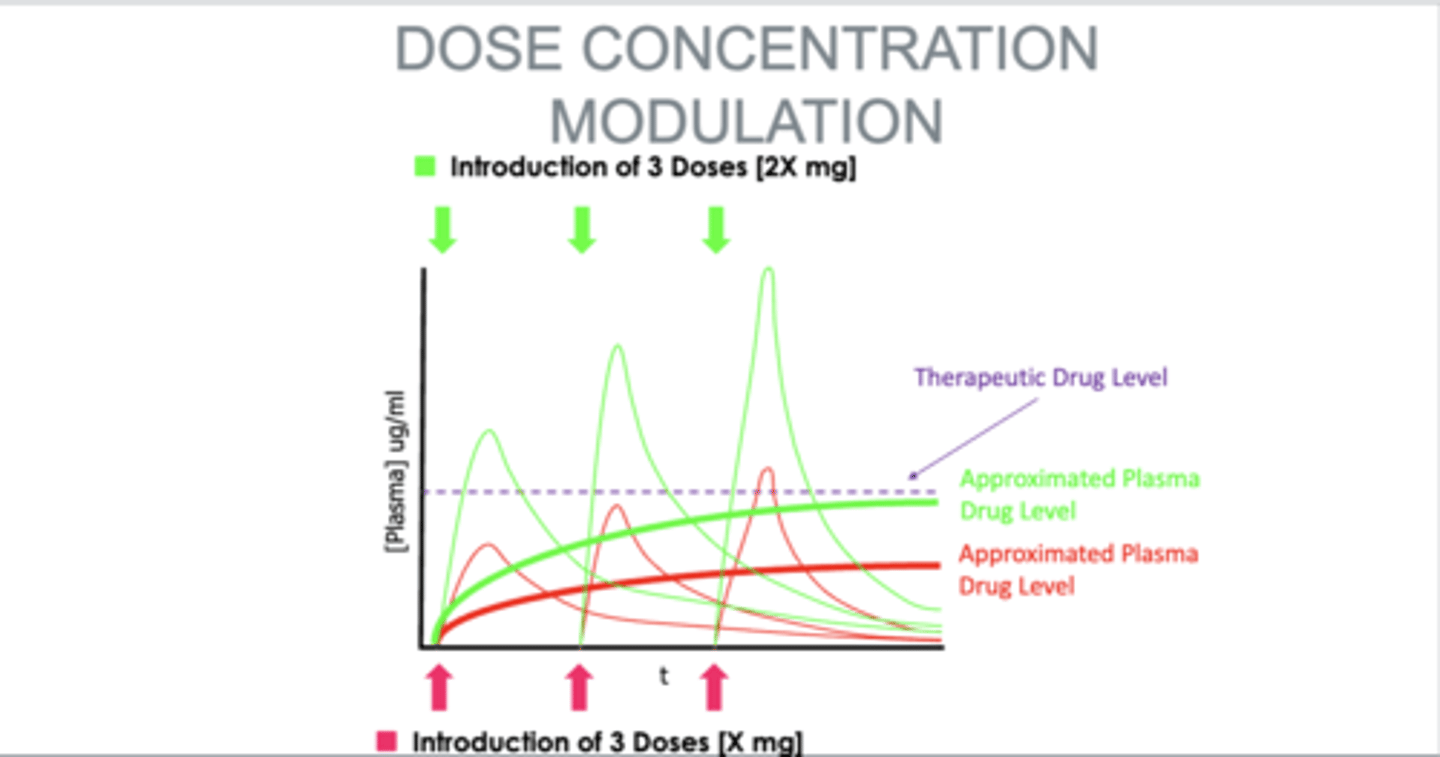
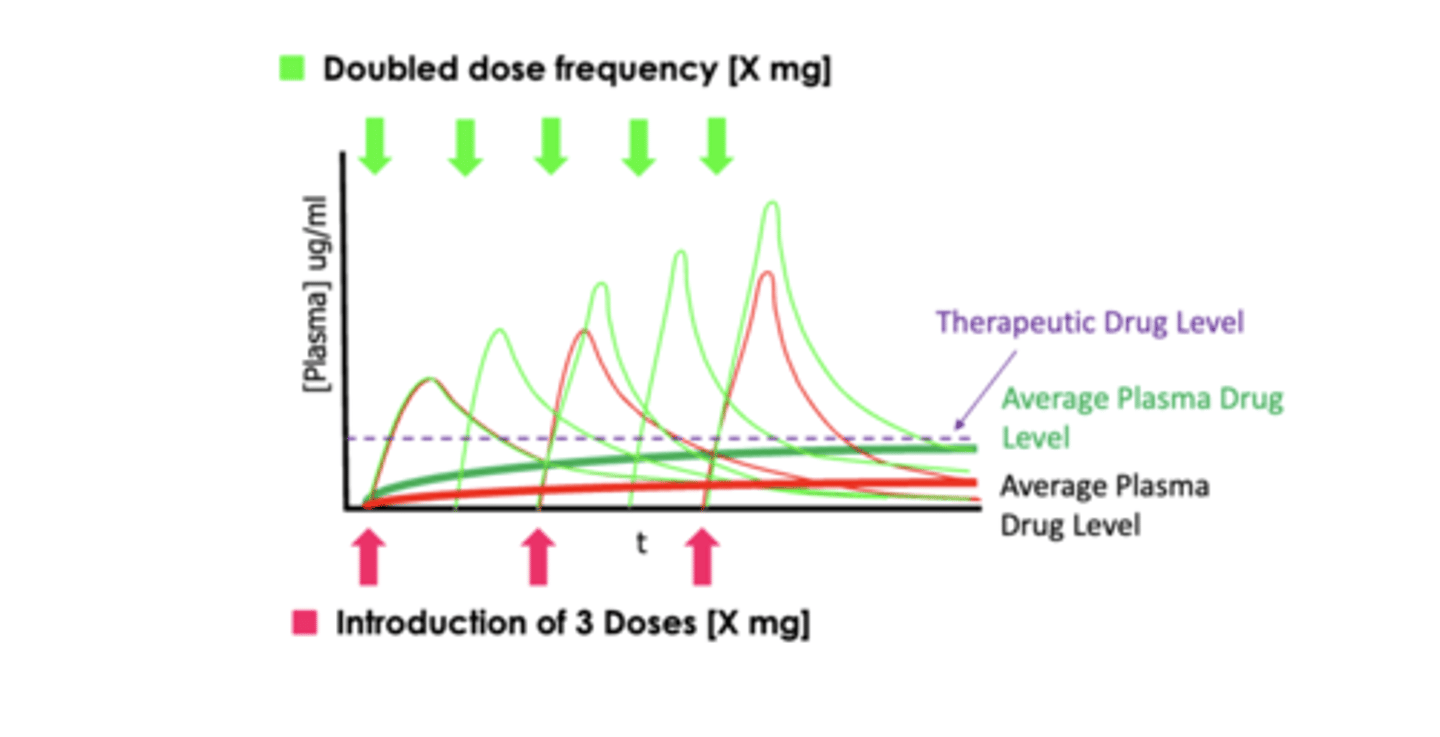
what can be done to improve compliance?
- increase concentration, lower the frequency of dosage the patient has to take
what is polypharmacy?
- use of 5 or more medications
what is resistance?
- loss of pharmacological effect especially to bacteria
what is Teratogenesis?
- congenital malformation
what is Bioavailability?
- amount of active drug reaching target tissue
what does DPA stand for?
- diagnostic pharmaceutical agent
what does TPA stand for?
- therapeutic pharmaceutical agent