boderline personality disorder and parenting
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
what is bpd also known as and problems with names
emotionally unstable personality disorder
Can be a certain element of stigma with personality disorders - personalities are who you are, so labelling it as being disordered can feel bad
EUPD is more informative but may not be better than bpd as the condition has more stigma associated with it
DSM refers to it as BPD, WHO refers to it as EUPD
origin of the name of bpd
Means when some patients came in, psychiatrists saw signs of neurosis, psychosis, schizophrenia but not those completely - on the borderline of these conditions
potential causes of bpd
Really complex condition - lots of comorbidity
Childhood trauma eg sexual abuse, adversity (Paris, 2008)
Developmental precursors
Temperament, less stable/settles, more irritability, predisposition for impulsivity (Bozzatello, 2019)
Maladaptive parenting (Johnson, 2006; Paris, 2003) leads on to
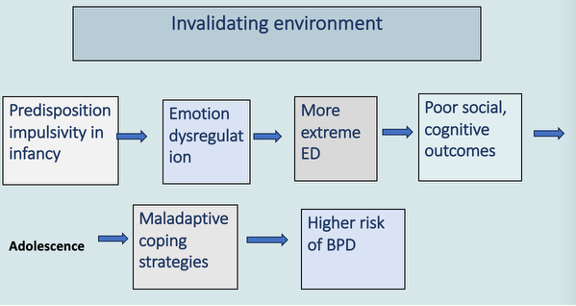
invalidating environment as a cause of bpd
SES seems to create extra issues, parental mental illness, substance misuse (Stepp, 2016; White, 2003)
Brain differences (Mauchnik, 2005) prefrontal cortex less well developed and activated - difficulties with self-control, impulsivity. hippocampus has less grey matter (involved in memory) more activity in the amygdala - processes emotions, fear, anger, sadness
Hereditary (Zanarini, 2004), almost 50% is genetic, may not mean that genetically if you are predisposed to BPD you will develop the condition, also involves environment
Contemporary theories: biosocial model (Linehan 1993; Crowell 2009) have an interaction. Eg genetically may be predisposed to this condition, may also have temperament that predisposes you even more to have it, could then have other environmental issues going on that exacerbate it
biosocial model of bpd
All of these factors are made worse by the overarching invalidating environment
If had sensitive parenting trajectory might not happen - may give coping strategies etc
who does it affect
1-6% of general population, chances are its higher, people aren't diagnosed
10% psychiatric outpatients and 20% inpatients have BPD
More prevalent than schizophrenia and bi-polar disorder together
Some studies show equal male/female prevalence
Females experience greater symptoms (more emotional, may then lead to self-harm) and more likely to be seen in clinical settings, men have more angry symptoms
Many misdiagnosed or remain undiagnosed eg bipolar, depression, ptsd although maybe not misdiagnosis to a point, childhood traumas that have been experienced act in a very similar way to ptsd
Typically diagnosed in late adolescence/early adulthood, impulsivity may lead to having children at quite an early age which may lead to issues with parenting
long term outcome (prognosis)
Possible to recover and treat
70% will attempt suicide at some point
High rate of mortality – death by suicide 50 x general population, 8-10% complete attempt, dont want to end life, just dont know what they can do in order to live their life
Self-harm high – c.75% way of communicating level of despair, release tension and pressure that has built and built
Remission possible – Gunderson (2011), 85% remitted over 10 years; Paris (2011), 92% no longer met diagnostic criteria after 27 years
Remission more likely in those with higher IQ, functioning adequately at work, with a stable relationship, and not frequently hospitalised
Impulsivity first to remit, ED slower, relationship difficulties remain - could be due to the effects of ED
Co-occurring conditions
Anxiety disorders
Post traumatic stress disorder (PTSD)
ADHD
Substance misuse
Eating disorders
Other personality disorders, quite often an overlap between conditions
Mood disorders/depressive disorders - 83% lifetime prevalence of major depressive disorder (Zanarini et al., 1998), very common to co-exist
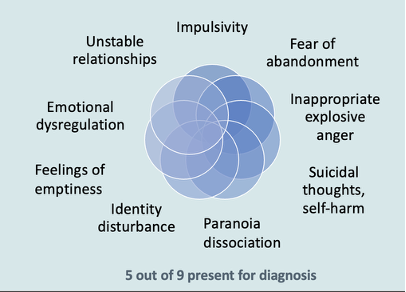
BPD diagnostic criteria (DSM-5)
Lots go hand in hand with each other - interconnected
5 out of 9 present for diagnosis - heterogeneous condition, may have first 5 or last 5 etc, some people might have all 9
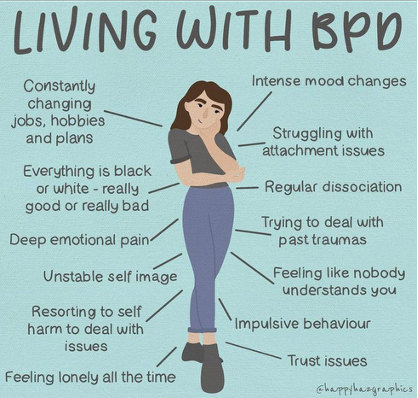
Living with BPD
Very impulsive - dont have a sense of identity dye hair to reinvent herself - lack of sense of self
Scared people are going to leave eg boyfriend, friends - can be real or imagined. Fear is very strong - leads to pushing away or being really clingy
Black and white thinking - love one of their friends, if they don't text back can go to hating them. Feeling is so intense. Stew on it all day. Don't integrate the whole person - good friend when doing something they're happy with, bad person when they do something slightly wrong
0-100 - have a good day, something happens then ruined for the whole day. Very intense compared to bi-polar as just one word can ruin the day
examples of optimal parenting
sensitive, responsive
afectionate, warm
encouraging autonomy
supportive
guiding, scaffolding
regulating beh
emotional availability
safety, security
physical care
still face experiment
Sat in front of the child, engage in normal way, smiles, looks where pointing etc
Mother is told to stop playing with the child and have an expressionless face
Child tries to get mother to engage
Quickly becomes distressed - has made such a difference
attachment
Bowlby’s attachment theory – motivational system for establishing attachment to primary caregiver
Ensures survival of infant – attachment figure as secure base for exploration and support in times of stress. Eg can explore new places as know they have a secure base to come back to
Believes parent and child are built with predispositions for this, caregiver wants to care for the child, child has social releasers that help parents to attach
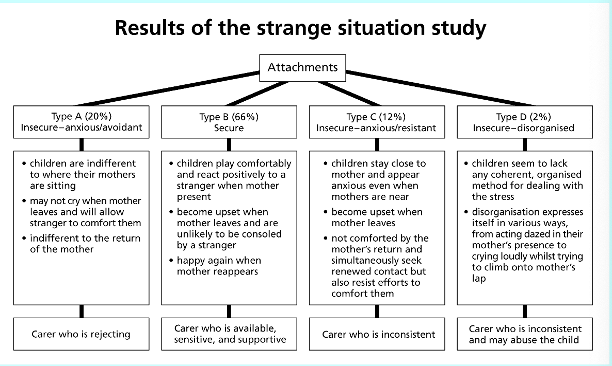
ainsworth’s attachment categories
How might having a diagnosis of BPD make parenting difficult?
Anger is not good around a child
Insecure attachment
Lack of independence for child - need to let child be more autonomous but scared of abandonment
When a baby is born, they split. Good mum feeds me, bad mum leaves me to cry. Over time have this cycle, when child has a need, mother responds sensitively to that need. Eventually learns mother will come. If that cycle doesn’t come or is interrupted, have potential difficulties. Process allows them to bring the two together, the reason people with BPD split is because they haven’t had that emotional support when they are younger
Start of splitting between good mother and bad mother haven't had that emotional support when they were younger
Struggles with emotional dysregulation - child is born dysregulated - role as primary caregiver is to help regulate their emotions so very difficult to do this
parenting beh of mothers with bpd
some van parent very well, others maladaptive
maladaptive parenting in bpd
Less sensitive (e.g., Crandell et al., 2003)
Overprotective, intrusive, overinvolvement (e.g. Elliot et al., 2014) coming from a place of wanting to care for child as often experienced issues when they were younger
More hostile (e.g., Newman et al., 2007)
Less engagement, rejection (Hobson et al., 2009; Reinelt et al., 2014), less involved
Maladaptive interactions (e.g., Macfie et al., 2014) role reversal (child becomes the parent), withdrawn, inhibiting autonomy
other parenting characteristics
No difference from controls on maternal warmth (e.g., Herr et al., 2008) not someone who doesn't want to care for child, really want to care but have difficulties
Inconsistent parenting (Stepp et al., 2012, Eyden et al., in prep) do same thing but sometimes get
Maternal distress (Dittrich et al., 2020)
5-year-old child of a mother with BPD (Macfie, 2009)
Story-stem completion task, depict story, let child play, act out or say something with that story
Researcher tells a story of a birthday party using family dolls and a cake, then asks the child: "Show me and tell me what happens now"
The girl tells of how presents are opened, and the family eats cake
She then adds: "and then mum takes off her clothes and gets drunk"
Mother acts inappropriately - child thinks this is the norm at a birthday party
15-year-old daughter of mother with BPD (Macfie, 2009)
D: Now you’re acting even younger. You’re giggly and weird
M: Oh well, that’s just because I’m being rebellious at the moment. I want to try to have fun.
D: I’m the teenager I’m supposed to do that.
M: It has been so long since I’ve had fun and done the things that I want to do. Yeah, I miss being a teenager. It’d be nice if we could have that little bit of experience together and have fun.
D: No, you’re supposed to be my Mom.
M: Well, maybe someday I can be your Mom again
D: By the time you’re my Mom, I’ll be an adult, so it won’t even matter.
Mother acting more like teenager, teenager acting like the adults, teen may even start having to care for the mum
Parenting knowledge of mothers with BPD (Eyden et al., 2023)
Do mothers with BPD know what 'good' parenting looks like?
26 BPD mothers, 25 depressed, 25 no mental illness
Q-sort task on 'ideal' parenting
Ranked 90 behaviours - best possible beh to worst beh
No difference between groups with parenting knowledge
Parenting self-efficacy of mothers with BPD (Eyden et al., 2023)
Do mothers with BPD think they are good at parenting?
26 BPD mothers, 25 depressed, 25 no mental illness
Questionnaire parenting self-efficacy
BPD and depression lower on perceived parenting efficacy
Symptom severity predicted parenting self-efficacy, negative correlation
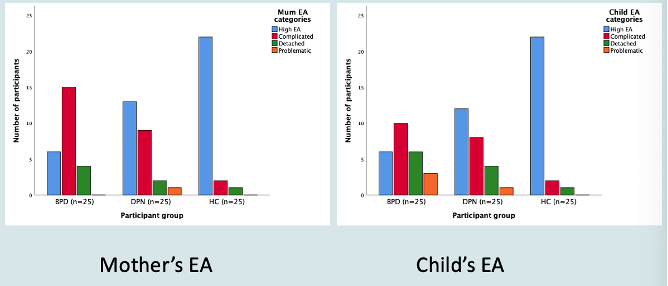
Are BPD mothers emotionally available to child? Eyden et al., (in prep)
Emotional Availability - open dyadic communication, available for play, communication etc. encompasses lots of parenting domains you’d want to look at
Assessed via observations (mother and child playing) and EAS coded
25 BPD, 25 depression, 25 no mental illness. Difficult to do research in this area as have to build lots of trust to film interactions and do research, feel they’d be judged, heightened sensitivity
More intrusive and overprotective
Less sensitive, more hostile only prevalent for those with BPD
Mental health severity predictor for maternal EA
Maternal sensitivity predicted child EA. if can be more sensitive, could improve child’s emotional availability
emotional availability categories of mother and child
Key links to attachment categories
Depression - 50% are high in emotional availability, other 50% are the other categories
BPD - high in complicated attachment
With depression, times there would be a slight mismatch which is complicated, when a mum acts in a certain way, delay in how the child is reacting, or delay in the way the mum is responding to the child
When look at children’s emotional availability, don’t mirror
With BPD - fewer in the complicated category, more of them starting to withdraw. Dont know how the mum is going to react in this situation so they just shut up
Outcomes for offspring of mothers with BPD Eyden et al., (2016)
Higher levels of BPD symptoms-especially emotional dysregulation (e.g., Macfie et al., 2014)
Higher levels of general psychopathology (depression common) (Barnow et al., 2013)
Higher internalising/externalising problems (eg rumination/behavioural problems such as aggressiveness) (e.g., Barnow et al., 2006) lots of acting out beh - act out for attention, way of dealing with inconsistencies
Psychosocial difficulties (Abela et al., 2005; Barnow et al., 2006) effects on self-esteem, self-critical
Poorer executive function (Zalewski et al., 2018)
Interpersonal difficulties (withdrawn/dysfunctional mother-child interactions) (e.g., Schacht et al., 2013) if having difficulty with emotions harder to make friends
More likely to be categorised as insecurely attached (Gratz et al., 2014)
Higher family instability (Feldman et al., 1995) have more frequent moves, more MH within parent, more likely to have sibling or relative that has gone to prison
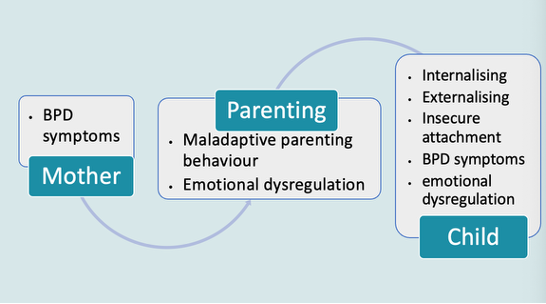
Mechanisms of transmission of vulnerability
Clearly a relationship between mother’s vulnerability and child’s vulnerability - is there something that is mediating this (instead of a direct relationship)
Some heritability: .40, so ~40% of individual differences in BPD symptoms attributable to genetics in some way
Offspring of BPD mothers may be more likely to experience childhood adversity/trauma
Maternal emotional dysfunction mediates mother-child association
Maladaptive parenting (insensitive, rejecting, hostile) as mediator, inconsistent, rejective, hostile parenting
Biosocial developmental model – inherited vulnerability to impulsivity interacts with environmental risk factors
If have invalidating environment on top of all of this, adds to problems
Child vulnerability
Factors affecting impact of parental mental illness
Timing of episode(s)
Effects on parenting and child strongest when symptoms are current
Depends on developmental stage of child, strongest in 1st year, most important part for relationship between parent and child
Chronicity and severity of mental illness
Child’s own temperament (positive and negative)
Associated with inter-parental conflict
Could explain rise in externalising problems in children
Parental depression leads to child depression - interparental discord then has an impact on conduct problems, if there is lots of rowing going on you want attention - may lead to this attention seeking conduct beh
buffers
Not all children go on to develop these outcomes
Social support for mother eg friends help with babysitting. Tend to be single mothers so social support is very important
‘Secondary parents’ – father, grandparent, mother’s friends, aunt etc.
Siblings and friends
Secure attachment (could be with another person)
Higher IQ, positive personality traits
More resourceful, better coping strategies (Rutter et al., 2012) resilience - children go through intense difficulties and function normally - what is it about them that is different
Interventions for individuals with BPD
Dialectical Behaviour Therapy (DBT) (Linehan, 1993; 2014) one of the best ones, individual and group therapy, based on cbt. Ways you can influence and change beh, distress tolerance, emotional regulation etc
Mentalization-Based Therapy (MBT) (Bateman & Fonagy, 1999; 2009) examine own thoughts and beliefs, change them, manage emotions and relationships, important to have a good client-therapist relationship
Schema-Focussed Therapy (Young, 1994), explores maladaptive early schemas eg self-depleting, replace with more positive ones
Other recognised therapies e.g., Systems Training for Emotional Predictability & Problem Solving (Blum et al., 2002; 2004); General Psychiatric Management (Gunderson & Links, 2014) some are shorter therapies - fairly effective but difficulties when therapy stops. Good for early intervention
Parenting interventions for mothers with BPD
General parenting programmes e.g., Confident Parents (Mouton et al., 2018); Triple P Positive Parenting Programme (Sanders 1999); Watch, Wait & Wonder (Muir et al., 1999) but difficult because follow childs lead, wait for them to do something (overly involved with child so need to help them with that first)
Project Air Parenting with Personality Disorder and Complex Mental Health Issues (McCarthy et al., 2015). How to care for yourself as well as others, deal with children at all ages. Also talk to children so they can start to understand
Parenting Skills for Mothers with Borderline Personality Disorder (Rosenbach et al., 2020). Echoes a lot of the deficits in the emotional availability study. What is developmentally appropriate for the child. Emotional regulation and conflict resolution.
Perinatal emotional skills group for BPD (Moran el al., 2024). Mother-infant DBT, try to understand how the child is feeling
Measures of parenting intervention efficacy
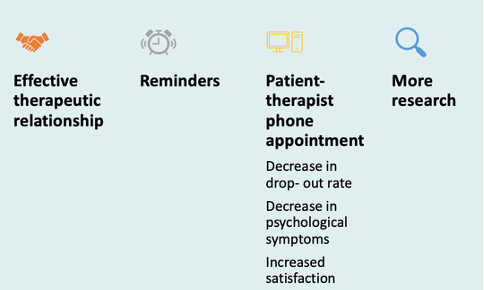
Barriers to intervention
Practical
Caught up with being a mother, where to put child when in therapy
Disorganised, may be late to appointments
Engagement
Drop-out rates high
Treatment completion varies 36-100%
Many studies DBT – bias? Mostly talk about DBT studies which people tend to engage better with
Behavioural
Impulsivity – distracted by other tasks
Challenging behaviours with therapist/psychiatrist. Almost want to test whether the therapist will leave them, pushes boundaries. Becuase of sensitivity, constantly want reassurance
Lack of commitment to change
Fear
Being judged
Child being removed
Overcoming barriers to intervention
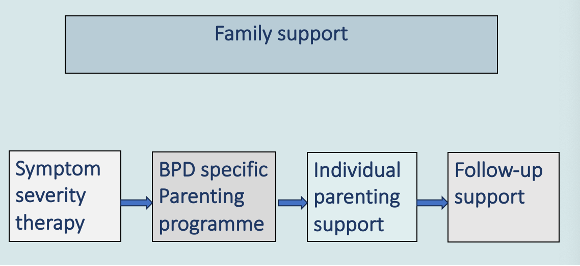
Ideal model of intervention
Don't often get all of it, not looked at it as a holistic thing
Initially - have DBT or MBT, helps you manage your symptoms. When can manage symptoms effectively, allows you to engage with other therapies
2 - aware of the things, scaffold and guide through
3 - then have individual parenting support. Record playing with the child and play it back to them. What could they have done differently.
4 - how to continue support, as go through life stages way you need to parent adapts - how to do this
Whilst this is happening have family support so the people around them know what they’re dealing with/going through
why is bpd important to research
Impact on parenting
Impact on child
Prevalence c.6% of general population
Female gender bias in clinical setting
Onset age: late adolescence/early adulthood
Need for early intervention
Implications for research
What are the ethical considerations? What is appropriate, safeguarding for both the researcher and mother. How to protect mother when asking about childhood and parenting etc
Potential recruitment difficulties? Don't want to be observed/asked about parenting. Also very likely to have high drop out rates
Methodological design considerations? Have children of dif ages, large range. How do you come up with a method suitable for all of them. Then how do you compare