Pharm II Week 5 (Antidepressants, Anxiolytics, Sedatives, Hypnotics)
1/127
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
128 Terms
Major Depressive Disorder
•Depressed mood or loss of interest ≥ 2 weeks with functional impairment
•DSM-5: ≥ 5 symptoms for ≥ 2 weeks, including depressed mood or anhedonia
Anxiety Disorders
•Persistent, excessive worry or fear causing distress or impairment
•DSM-5 (GAD): Excessive anxiety/worry most days for ≥ 6 months, difficult to control, with associated symptoms (e.g., restlessness, fatigue, poor concentration)
Insomnia Disorder
•Difficulty falling or staying asleep with daytime impairment
•DSM-5: Sleep difficulty ≥ 3 nights/week for ≥ 3 months, despite adequate opportunity for sleep
incidence MDD
8.3% of U.S. adults (~21 million) experience annually
Higher prevalence in women (10.3%) versus men (6.2%)
Highest rate in young adults (18-25 years)
incidence anxiety
19.1% of U.S adults experience annually
31% lifetime prevalence (nearly 1 in 3 adults)
Frequently coexists with depression
incidence insomnia
30-40% of adults report insomnia symptoms
Strongly associated with depression, anxiety, substance use disorders
Drivers of Increasing Rates
Strong Evidence: COVID-19 stressors; economic hardship; improved screening; reduced stigma
Moderate: Primary care recognition; social stress; sleep disruption
Mixed: Social media use; lifestyle changes
Overview of CNS Neurotransmitters
Serotonin (5-HT)
Mood regulation, anxiety control, sleep initiation, appetite regulation
Overview of CNS Neurotransmitters
Glutamate
Primary excitatory neurotransmitter, learning and memory, synaptic plasticity
Overview of CNS Neurotransmitters
Norepinephrine (NE)
Alertness, attention, stress response, sympathetic activation
Overview of CNS Neurotransmitters
Gamma-Aminobutyric Acid (GABA)
Primary inhibitory NT, reduces neuronal excitability, promotes relaxation and sleep
Overview of CNS Neurotransmitters
Dopamine (DA)
Motivation, reward pathways, focus and cognition
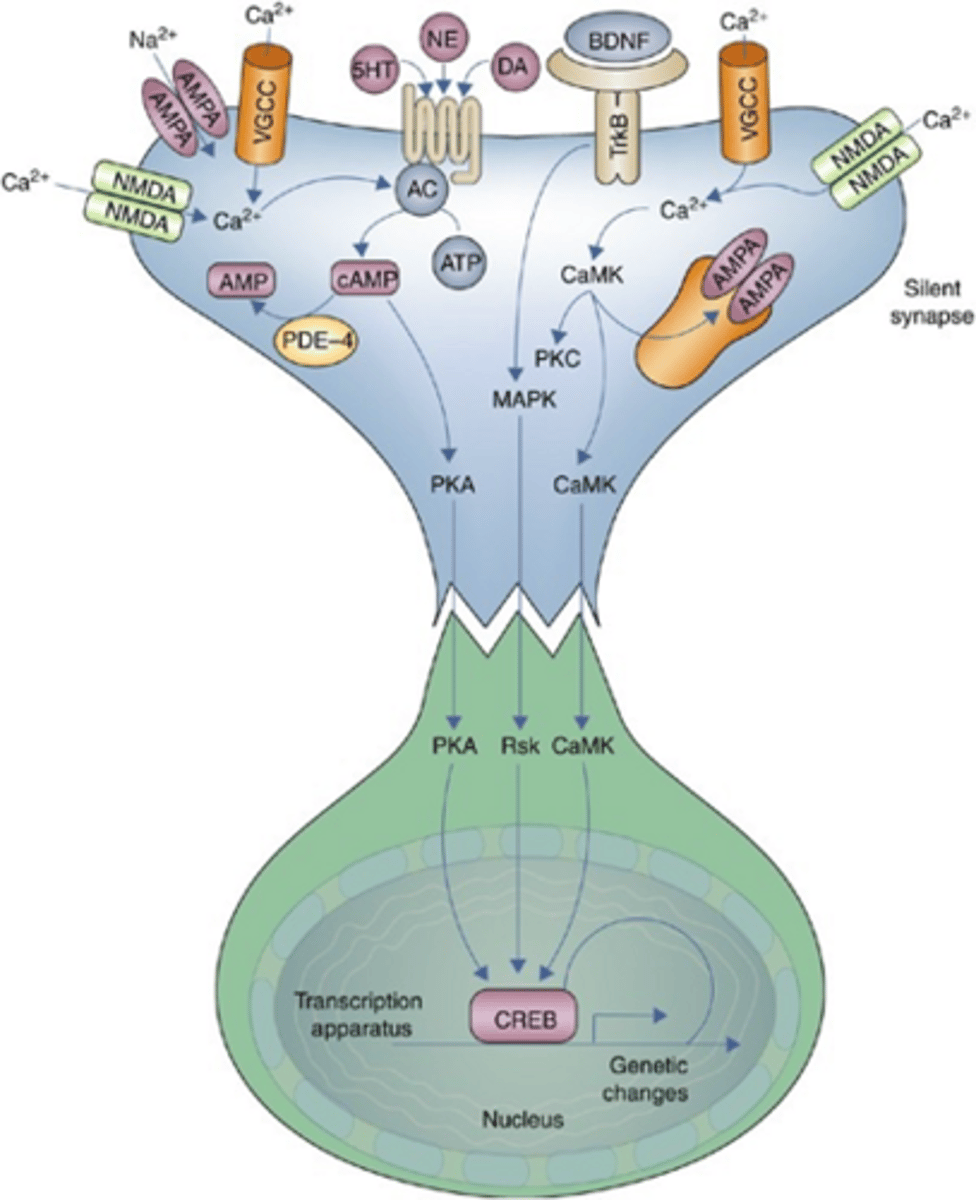
Pathophysiology of Depression
2 key parts
•Monoamine Deficiency Hypothesis (purple box): have less/ineffective toward 5HT, NE, and or DA. initiator.
•Neuroplasticity Changes: longer term effects. decreased brain-derived neurotrophic factor (BDNF), decreased neurogenesis, hippocampal atrophy, impaired synaptic signaling
Pathophysiology of Anxiety Disorders
GABA and Glutamate Imbalance - normal vs in anxiety?
Normal Balance
- GABA: inhibitory
- Glutamate: excitatory
In Anxiety
- Decreased GABA inhibition, increased excitatory neurotransmission, increased amygdala activity
- Manifests as restlessness, hypervigilance, muscle tension, sleep disturbance
Pathophysiology of Anxiety Disorders
Noradrenergic Overactivity
Increased norepinephrine causes: tachycardia, sweating, tremors, panic symptoms
Linked to locus coeruleus activation, sympathetic nervous system stimulation
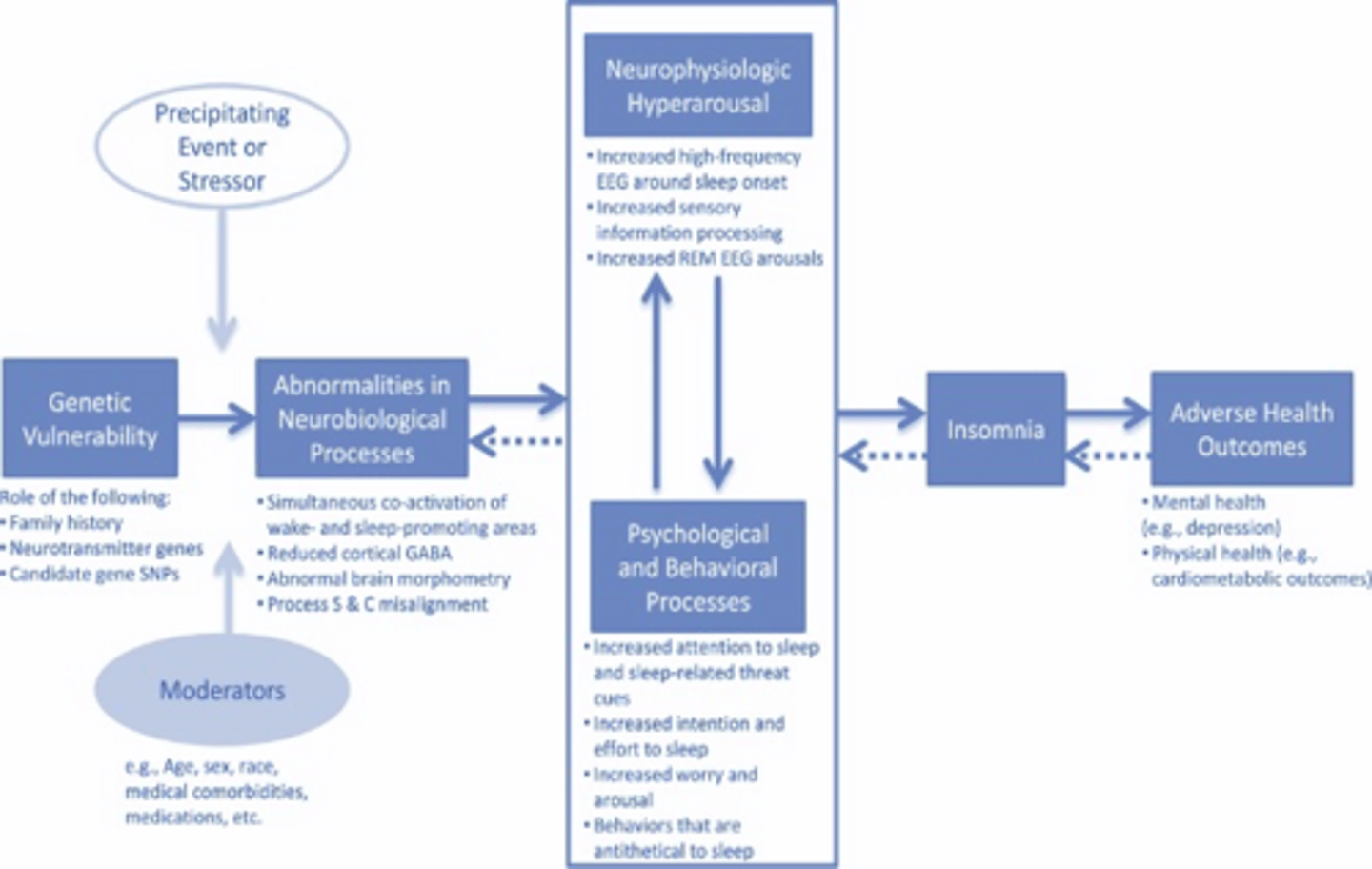
Pathophysiology of Insomnia
Sleep-Wake Dysregulation
Normal regulation involves GABA-mediated sleep pathways, circadian rhythm control, melatonin release
Insomnia: Increased CNS arousal, decreased GABA activity, disrupted circadian rhythm control
hyperactivation of the stress response system with strong cognitive and behavioral component.
Neural Substrates: Related Brain Regions (what do they process?)
Amygdala
Prefrontal Cortex
Hippocampus
Locus coeruleus
Hypothalamus
Amygdala
Fear and threat processing
Prefrontal Cortex
Executive control and emotional regulation
Hippocampus
Memory and mood regulation
Locus coeruleus
Norepinephrine release center
Hypothalamus
Sleep and circadian regulation
Antidepressants: Big Picture
1.SSRIs
2.SNRIs
3.Atypical antidepressants
4.TCAs
5.MAOIs
SSRIs: Mechanism & Role
-Block serotonin reuptake results in increased serotonin in synapse
-First-line for depression and anxiety disorders
-Favorable safety profile compared to older agents
SSRIs: common issues
• GI upset
• Sexual dysfunction: Major cause of nonadherence
• Activation or sedation: Activation can worsen anxiety early
• Discontinuation symptoms (dizziness, irritability, “brain zaps” Flu-like symptoms, insomnia)
• Do not stop abruptly: Slow taper
SSRIs: Additional Highlights
Time to Effect
takes time!!
Initial improvement: 1–2 weeks
Full response: 4–6 (up to 8) weeks
Early side effects often appear before benefit
Serotonin Syndrome Risk
SSRI + MAOI (contraindicated!)
SSRI + another (tramadol / linezolid / other serotonergics)
stop offending agent and monitor fluids, consider 5HT antagonist. can be fatal!
serotonin syndrome triad
Triad
1.Mental status changes
2.Autonomic instability (fever, tachyc)
3.Neuromuscular hyperactivity (tremors, seizures, etc.)
CYP Drug Interactions
Strong inhibitors: fluoxetine, paroxetine, fluvoxamine (strongest)
Lower interaction burden: sertraline, escitalopram
Can increase levels of many co-administered drugs (e.g., inc level of warfarin, BB, antipsychotics)
Comparing SSRIs / Overview
know the major pearls well! and halflife application with withdrawl.
fluoxatine: primary activator, very long half life (less discontinuation sdr)
sertraline: versatile! less SE
Paroxetine (Paxil): shortest! most withdrawl sx if quickly stopped
Escitalopram (Lexapro): better version of Citalopram. LESS SE. dual inidcation for ANX AND DEP.
Fluvoxamine (Luvox): MANY drug interactions. some usage in OCD.
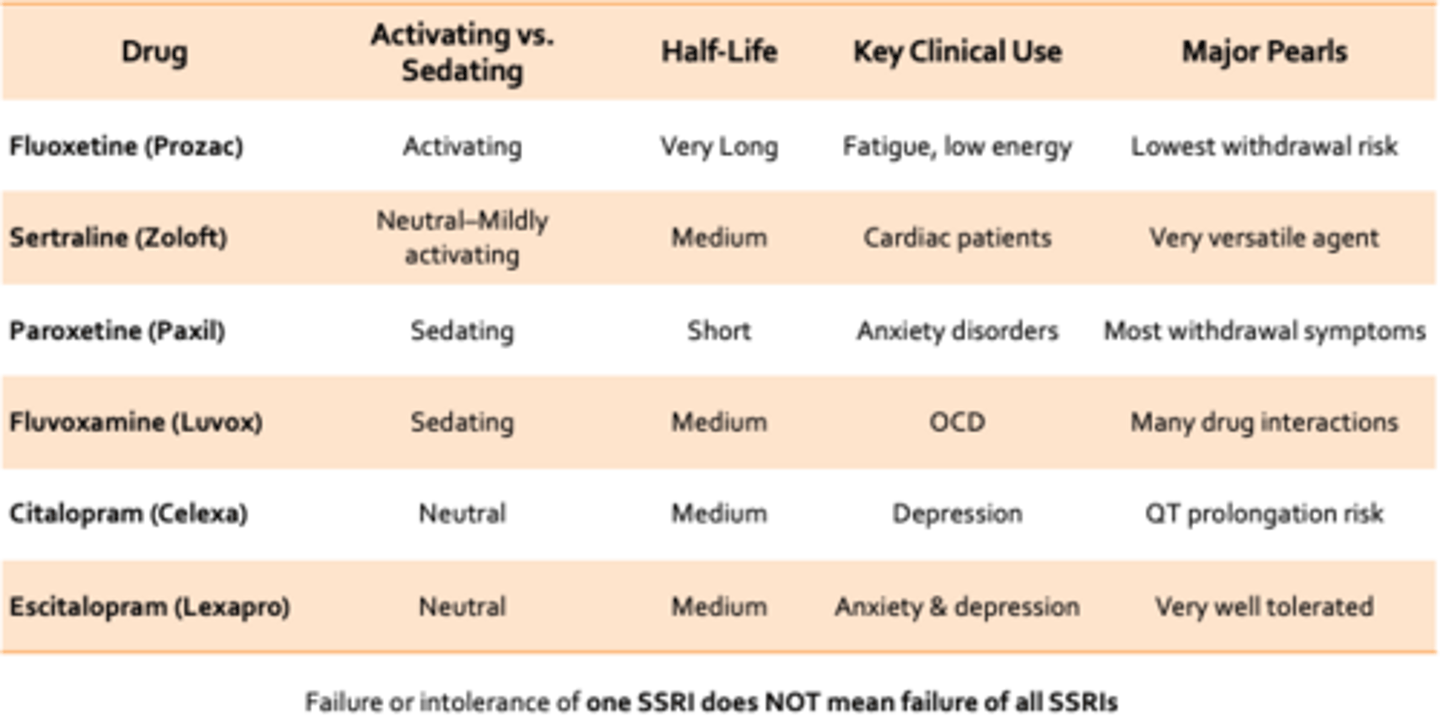
Failure or intolerance of one SSRI does NOT mean?
Failure or intolerance of one SSRI does NOT mean failure of all SSRIs
SNRIs: Mechanism
Inhibit reuptake of serotonin (5-HT) and norepinephrine (NE)
NE effects become more prominent at higher doses
SNRIs Clinical Indications
• Major depressive disorder
• Generalized anxiety disorder
• Neuropathic pain (key differentiator from SSRIs) !!
• Fibromyalgia
• Diabetic peripheral neuropathy
• Musculoskeletal/chronic pain syndromes
Why choose an SNRI instead of an SSRI?
• Depression + pain symptoms
• Partial response to SSRI
• Prominent fatigue/low energy symptoms
• Comorbid anxiety + somatic symptoms
SNRIs ADRs
•Cardiovascular: hypertension, tachycardia, palpitations
•CNS / Systemic: insomnia or activation, sweating, anxiety, nausea
SNRIs Discontinuation Syndrome
•Particularly venlafaxine (most notorious)... bc SHORT HALF LIFE
•Can occur within 1–3 days of missed doses
•FINISH pneumonic
SNRIs Monitoring Recommendations
•Blood pressure (baseline and follow-up)
•Heart rate in symptomatic patients
•Monitor adherence closely
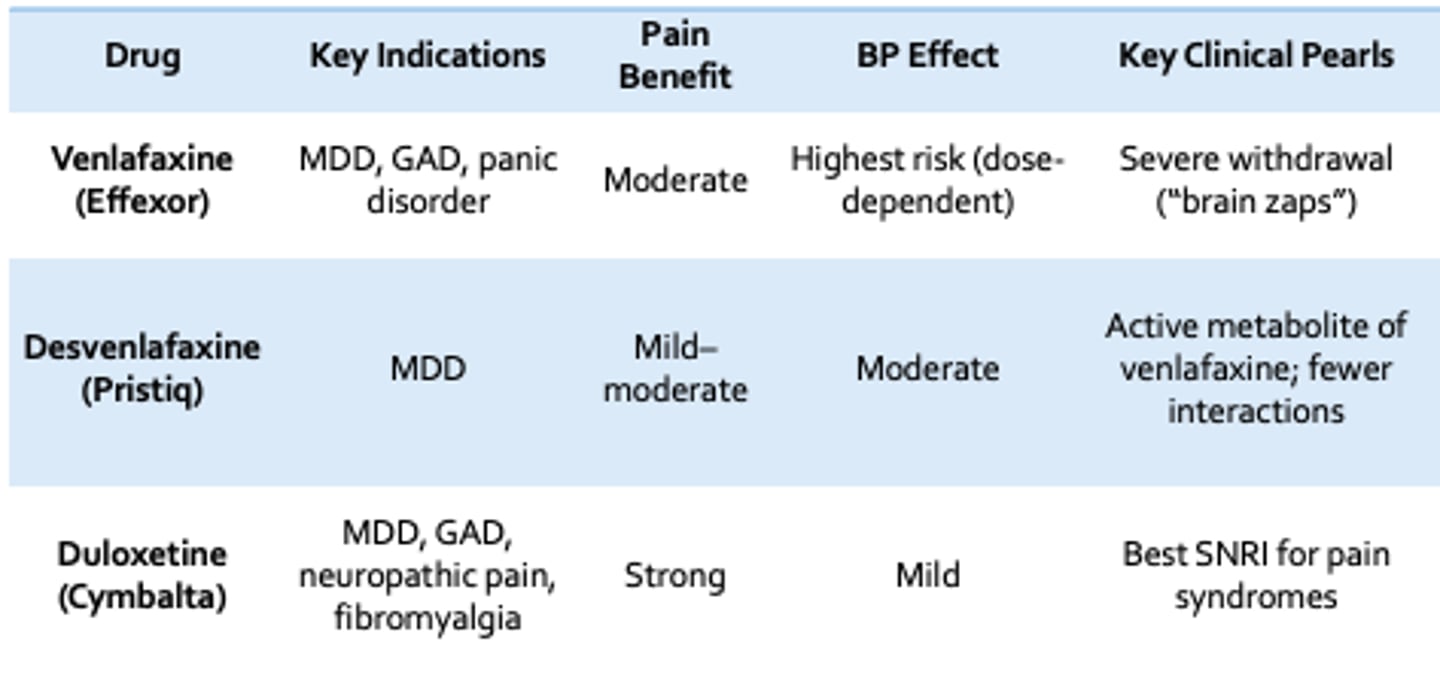
Comparing SNRIs
know the top 3 BEST
Venlafaxine (Effexor): MDD, GAD, panic disorder. highest BP risk
Desvenlafaxine (Pristiq): MDD only. fewer drug drug interactions.
Duloxetine (Cymbalta): Best SNRI for pain syndromes
Clinical Pearls for SNRIs
- Venlafaxine = highest withdrawal risk SNRI
- Always taper slowly when discontinuing
- Missing even 1-2 doses can trigger symptoms in sensitive patients
- Duloxetine preferred when pain is a major component
•Depression + pain → ?
•Depression + anxiety → ?
•Poor tolerance to venlafaxine → ?
•Need more NE effect → ?
•Depression + pain → Duloxetine
•Depression + anxiety → Venlafaxine
•Poor tolerance to venlafaxine → Desvenlafaxine
•Need more NE effect → Levomilnacipran
Overview of Drug Class - Atypical Antidepressants
Antidepressants that do not primarily act via serotonin reuptake inhibition (SSRIs) or serotonin/norepinephrine reuptake inhibition (SNRIs)
major agents - Atypical Antidepressants
Bupropion
Mirtazapine
Trazodone
indications for atypicals?
- Target specific symptom profiles
- Improve tolerability when SSRIs/SNRIs fail
- Manage side effects of SSRIs (e.g., sexual dysfunction, insomnia)
Buproprion MOA
Inhibits reuptake of dopamine (DA) and norepinephrine (NE)
Buproprion Clinical Uses
- Major depressive disorder
- Seasonal affective disorder
- Smoking cessation (Zyban)
- SSRI-induced sexual dysfunction (common switch/add-on strategy)
Buproprion Key Advantages
- No sexual dysfunction (major differentiator)
- Weight neutral or weight loss
- Activating (improves energy, motivation)
Buproprion ADRs
- Insomnia
- Anxiety/activation
- Lower seizure threshold (dose-related risk)
Buproprion Contraindications
Seizure disorder
Eating disorders (bulimia/anorexia)
Abrupt alcohol/benzodiazepine withdrawal
Mirtazapine MOA
α2 antagonism: ↑ norepinephrine + serotonin release
- Blocks 5-HT2 (reduces anxiety/insomnia) and 5-HT3 (reduces GI effects)
Strong H1 blockade → sedation
Mirtazapine Clinical Use
Depression with insomnia
Depression with weight loss or poor appetite
Frail or underweight patients
Mirtazapine Key Advantages
Strong sedation (especially at lower doses)
Appetite stimulation --> weight gain
Minimal sexual dysfunction
Mirtazapine ADRs
Sedation (dose-dependent pattern)
Weight gain
I
ncreased appetite
Rare neutropenia
Trazodone MOA
Weak serotonin reuptake inhibition
5-HT2 antagonism
Strong H1 and alpha 1 blockade
Trazodone Clinical Uses
Insomnia (most common use at low dose)
Depression (higher doses)
Trazodone ADRs
Sedation (avoid combining with other CNS depressants when used for sleep)
Orthostatic hypotension
Dizziness
Priapism (rare)
TCAs: Why Not First-Line?
work on a variety of receptors. variable and diverse drug --> many SE and toxicity concerns! such as:
1. Anticholinergic Toxicity
2. Narrow Therapeutic Index
3. Cardiovascular Toxicity
anticholinergic toxicity TCA symtoms
Dry mouth
Blurred vision
Constipation
Urinary retention
Confusion/delirium (especially elderly)
Strong reason TCAs are avoided in older adults
narrow therapeutic index - TCAs
High risk of overdose
“3 Cs of TCA overdose”:
•Coma
•Convulsions
Cardiotoxicity
Cardiovascular Toxicity - TCAs
Sodium channel blockade _ QRS widening
Orthostatic hypotension (_1 blockade)
Arrhythmias
QT prolongation risk
Important: dangerous in patients with cardiac disease
TCAs: Where are they used then?
Neuropathic Pain
Migraine Prophylaxis
Sleep (off-label)
TCAs - Neuropathic Pain
Diabetic neuropathy
Postherpetic neuralgia
Chronic pain syndromes
Migraine Prophylaxis - TCAs
Amitriptyline commonly used
Especially helpful in:
-- Chronic migraines
-- Patients with comorbid insomnia
Sleep (off-label) - TCAs
Sedating TCAs (amitriptyline) sometimes used at low doses
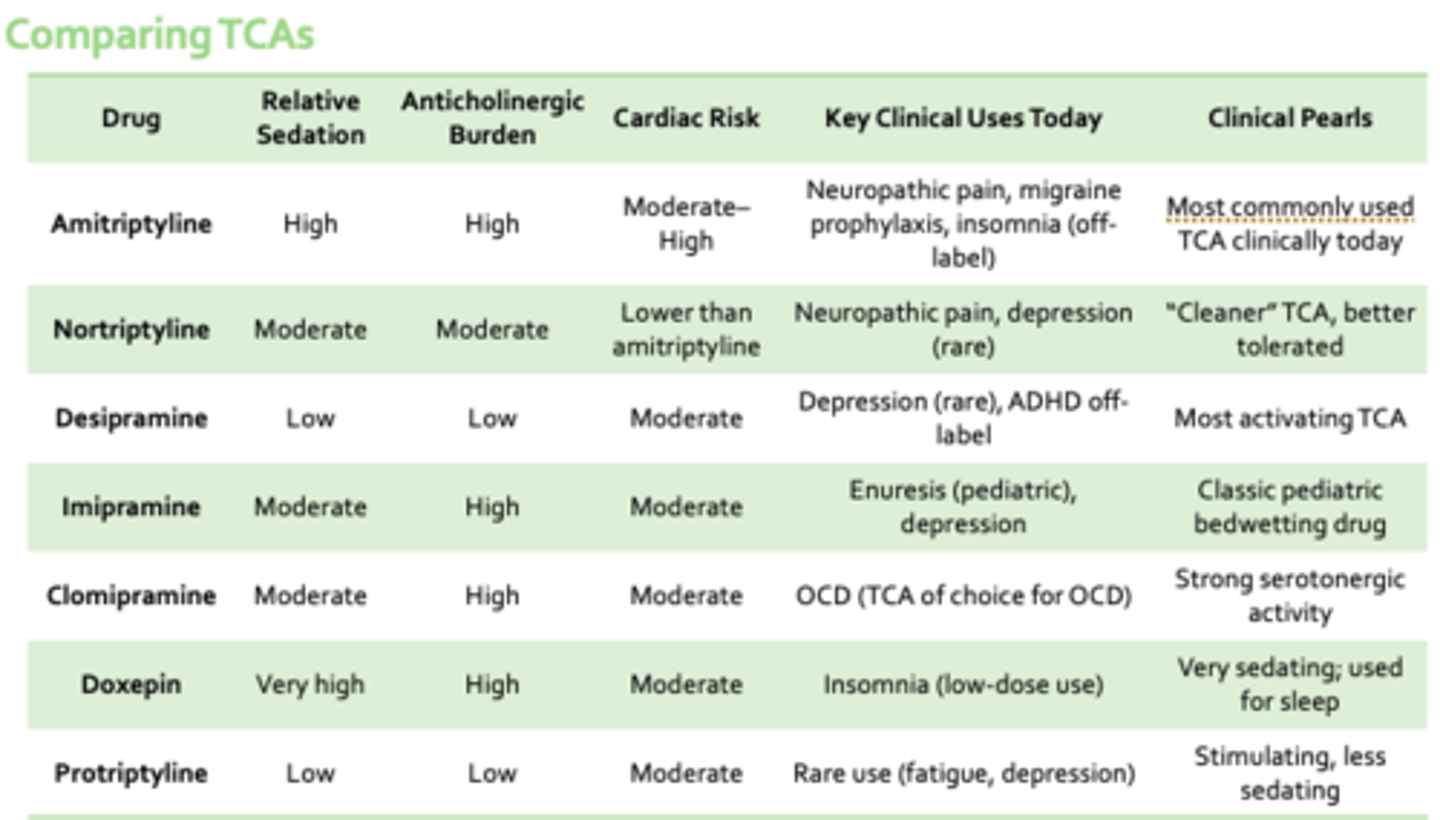
Comparing TCAs
Amitriptyline - Most commonly used TCA clinically
Nortriptyline - “Cleaner” TCA, better tolerated
Desipramine - Most activating TCA
Imipramine - Classic pediatric bedwetting drug
Clomipramine - Strong serotonergic activity
Doxepin - Very sedating; used for sleep
Protriptyline - Stimulating, less sedating
Monoamine Oxidase Inhibitors (MAOIs)
MOA
Inhibit monoamine oxidase (MAO-A and MAO-B)
Prevent breakdown of serotonin, norepinephrine, dopamine → ↑ synaptic monoamines
Where MAOIs Are Still Used
- Treatment-resistant depression
- Atypical depression (hypersomnia, hyperphagia)
- Parkinson disease (MAO-B inhibitors like selegiline)
Key MAOIs
• Phenelzine (nonselective, more sedating)
• Tranylcypromine (nonselective, more activating)
• Selegiline (MAO-B selective with low-dose; patch form reduces dietary restriction somewhat... minimizes ADRs)
MAOIs: High Risk
dietary restrictions
• Tyramine (aged foods) normally broken down by MAO
• MAOI → tyramine accumulation → hypertensive crisis
• High-risk foods: aged cheeses, cured meats (salami, pepperoni), fermented foods (soy sauce, kimchi), tap beer / draft beer
think charcuterie board stuff + soy sauce + beer
MOAIs - Drug Interaction Burden
Contraindicated combinations?
Contraindicated combinations:
SSRIs / SNRIs
Tramadol
Meperidine
Dextromethorphan
Linezolid
Safety Concerns MOAs
Hypertensive crisis (tyramine reaction)
Serotonin syndrome
Orthostatic hypotension
Weight gain, sexual dysfunction
46-year-old male presents with:
Depressed mood, low energy
Difficulty concentrating
Diabetic neuropathic pain
Requests medication that will “help mood and pain”
Current meds:
Metformin
Tramadol PRN (think abt serotonin sdr here)
Best initial antidepressant?
A. Sertraline B. Bupropion C. Duloxetine D. Amitriptyline E. Not indicated
✅ Answer: C. Duloxetine
(Duloxetine)
💡Rationale:
Treats depression + neuropathic pain
SNRI dual mechanism ideal fit
46-year-old male follow-up:
Increased restlessness
Episodes of sweating and tremor
Recently increased tramadol use for pain
Current meds:
Metformin
Tramadol PRN
Duloxetine
What is the most likely issue?
A. Serotonin syndrome B. Duloxetine toxicity C. Opioid withdrawal D. Hypoglycemia E. Not indicated
A. Serotonin syndrome
SNRI + tramadol = serotonergic overload risk
Always reassess new medications or dose changes
sx are indicative
Key Points for Antidepressants
Suicidality Warning (BBW)
BBW: ↑ SI risk in children, adolescents, young adults (<25)
•Highest risk: first weeks or dose changes
•Requires close follow-up, not avoidance of therapy
Key Points for Antidepressants
Pregnancy and Lactation
•Untreated depression also carries risk
•SSRIs commonly used when needed
•Avoid abrupt discontinuation (ESP in PREGNANCY)
Key Points for Antidepressants
Initiation and Titration
•Start low, go slow
•Early side effects common and do NOT equal failure... can switch to another class! esp SSRIs
Key Points for Antidepressants
Expected Timeline
• 1–2 weeks: side effects > benefit
• 2–4 weeks: early symptom improvement
• 4–6+ weeks: full therapeutic effect
Key Points for Antidepressants
when to switch meds
No response after adequate trial (4-6 weeks)
Intolerable side effects
Drug interactions or safety concerns
Key Points for Antidepressants
how to switch
Direct switch (most SSRIs / SNRIs)
Cross-taper (selected cases)
Washout required: MAOIs
• SSRI --> MAOI: 14 days (mitigate SE like serotonin sdr)
• Fluoxetine --> MAOI: ~5 weeks (logistically not great)
Key Points for Antidepressants
when to cross taper
High-dose antidepressant
Hx of discontinuation sx // Relapse risk is high!
Partial response to current med
Switching between different antidepressant classes (SSRI --> TCA, SNRI --> mirtazapine)... bridges
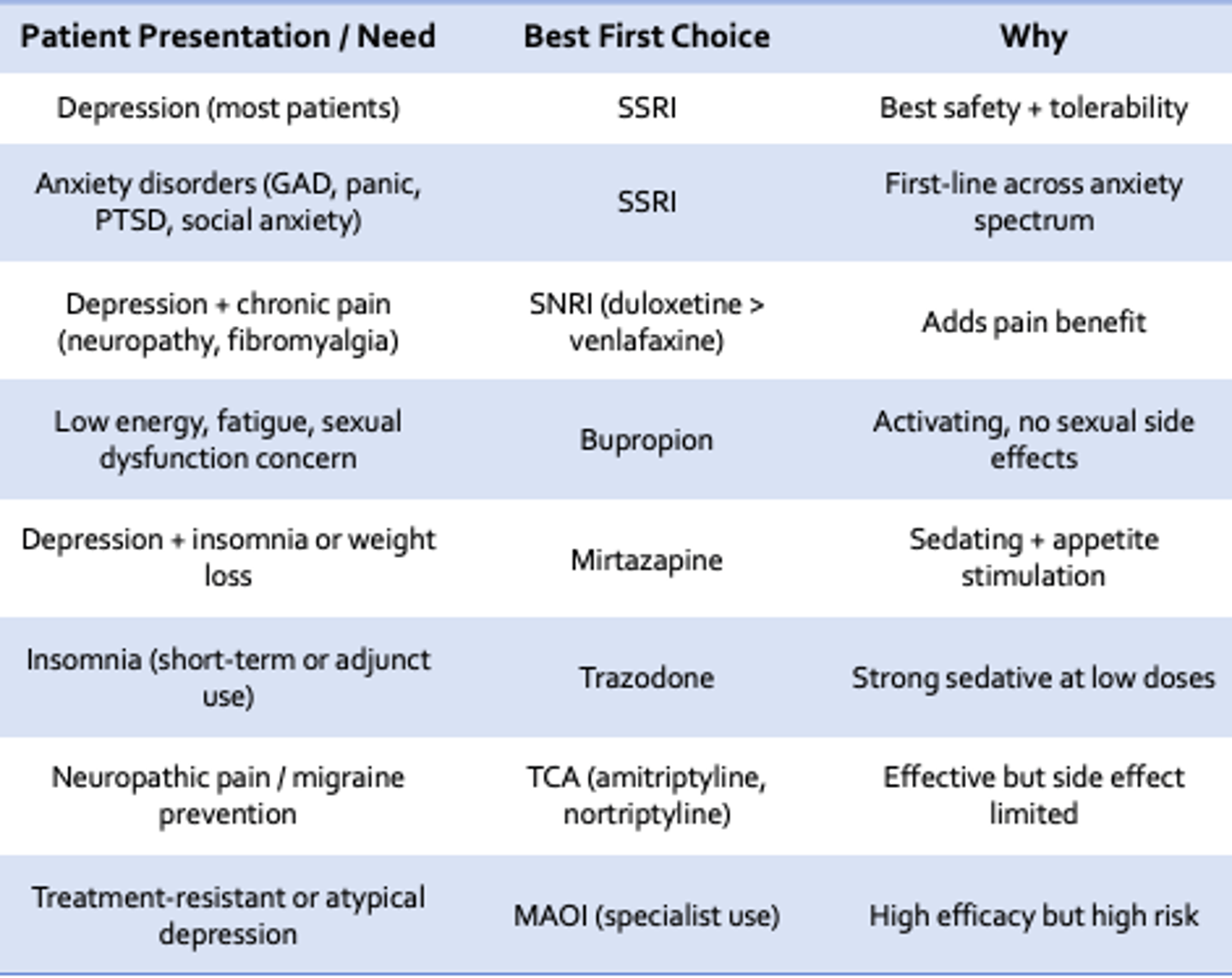
Concluding Thoughts on Antidepressants
know this well! be able to ID these based on need
Anxiety Disorders: Big Picture
Medication Categories
1. SSRIs/SNRIs (first-line long-term)
2. Benzodiazepines
3. Buspirone
4. Hydroxyzine
5. Pregabalin
6. Beta-blockers (situational anxiety)
•Benzodiazepines are not first-line long-term
•Goal: treat anxiety without creating dependence
Benzodiazepines MOA
Enhance GABA Activity
Benzodiazepines increase GABA, the brain’s main inhibitory neurotransmitter
Benzodiazepines Result
Result:
- Sedation
- Anxiolysis
- Muscle relaxation
- Anticonvulsant activity
Indications - Benzodiazepines
Acute anxiety
Panic attacks
Alcohol withdrawal
Status epilepticus
Procedural sedation
Nausea/vomiting
Catatonia
Benzodiazepines - Clinical Usage
- Short-term rescue medications
- Not ideal for chronic anxiety management
- Often used as bridge therapy while SSRIs take effect
Benzodiazepines - Adverse Effects
Sedation
Dizziness
Delirium
Memory impairment (anterograde amnesia)
Respiratory depression (especially when with opioids or alcohol)
Falls (especially elderly)
Dependence and withdrawal
Tolerance
Paradoxical reactions
Increased Risk Of Withdrawal
Increased Risk Of Withdrawal - Benzodiazepines
Higher doses
Longer duration
Shorter-acting agents
Withdrawal can be life-threatening and should not be stopped abruptly
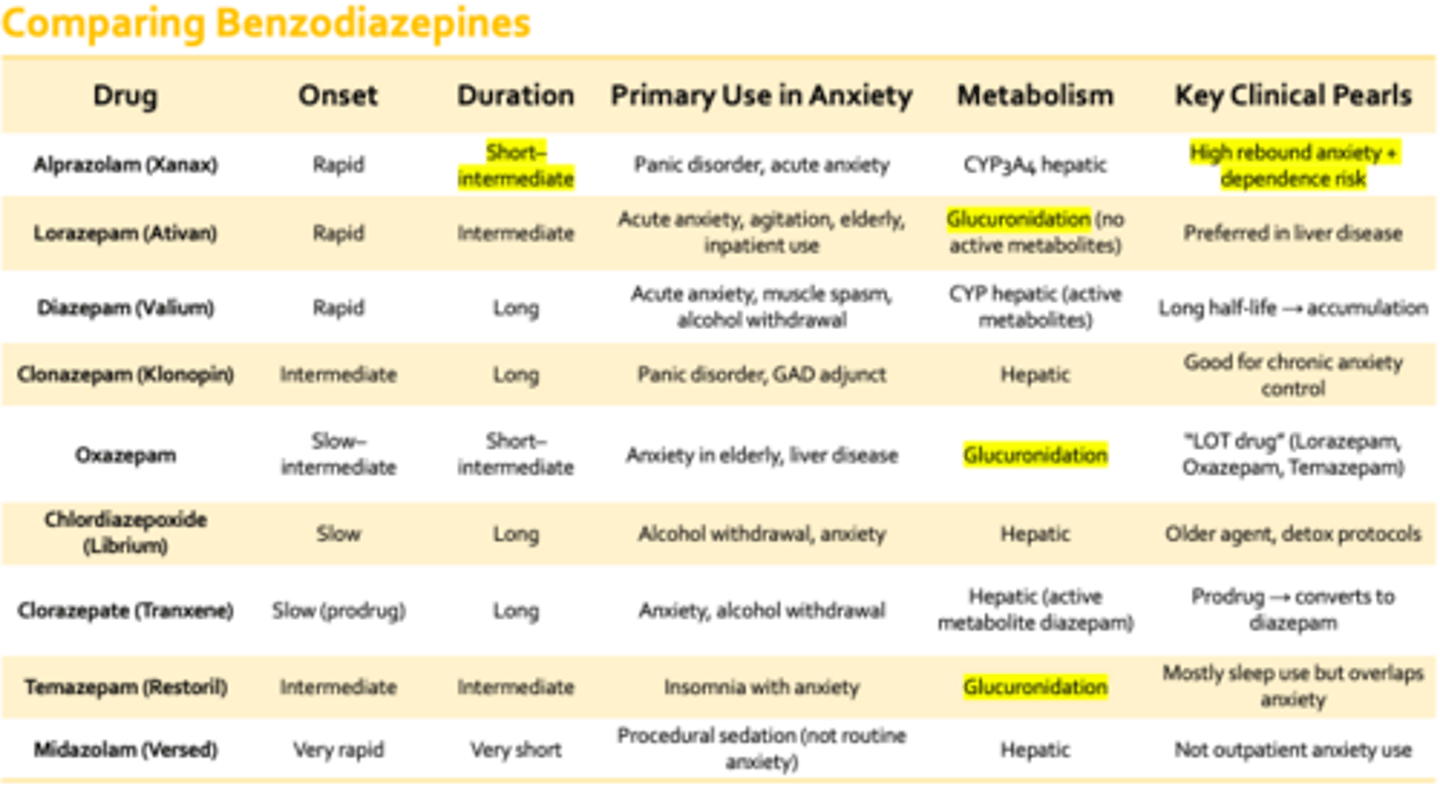
Comparing Benzodiazepines - Agents and key clinical perals
•Lorazepam = safest all-around acute benzo
•Clonazepam = chronic panic control
•Diazepam = long-acting (withdrawal, muscle spasm)
•Alprazolam = fast but high dependence risk... short 1/2 life = high rebound anx
LOT drugs = metabolized by Glucuronidation so no active metabolites, thus have LESS drug drug interactions (from a CYP standpoint)
Non-Benzodiazepine Anxiolytics
Buspirone (Buspar) MOA
5-HT1A partial agonist
Modulates serotonin signaling
No GABA activity
Buspirone (Buspar) Clinical use
Generalized Anxiety Disorder (GAD)
Adjunct in SSRI-treated anxiety
***not great for acute scenarios
Buspirone (Buspar) Key Advantages
No dependence or withdrawal
No respiratory depression
No cognitive impairment (minimal sedation)
Buspirone (Buspar) Limitations
Delayed onset (2–4 weeks)
Not effective for acute anxiety or panic attacks
Less effective for severe anxiety compared to benzos
Hydroxyzine (Atarax, Vistaril) MOA
H1 receptor antagonist
Mild anticholinergic and sedative effects
Hydroxyzine (Atarax, Vistaril) Clinical Use
Short-term anxiety
Acute situational anxiety
Adjunct for insomnia related to anxiety
Agitation
Pre-procedural sedation (mild)
Hydroxyzine (Atarax, Vistaril) Key Advantages
No dependence
Works quickly (unlike buspirone)
Useful as PRN alternative to benzodiazepines
Hydroxyzine (Atarax, Vistaril) Limitations
Sedation (common)
Anticholinergic effects - dry mouth, blurred vision , urinary retention (caution in elderly)
Not for long-term anxiety control
Pregabalin (Lyrica) MOA
GABA analogue (binds alpha-2-delta subunit of voltage-gated Ca2+ channels)
Decreases excitatory NT release (glutamate, norepinephrine, substance P)
Pregabalin (Lyrica) Clinical Uses
Generalized Anxiety Disorder (GAD) (off-label in US; approved in some countries)
Neuropathic pain (diabetic neuropathy, post-herpetic neuralgia)
Fibromyalgia
Adjunct for partial seizure disorders
Pregabalin (Lyrica) Advantages
No benzodiazepine-type dependence pattern
No serotonin syndrome risk
Useful when anxiety + chronic pain overlap
Pregabalin (Lyrica) Limitations
Additive CNS depression - alcohol, opioids, benzos - dizziness, somnolence, blurred vision
Weight gain
Peripheral edema
Dose adjustment needed in renal impairment
Misuse potential exists (though lower than benzos)
Beta Blockers (Propranolol, Atenolol)
MOA
Block Beta-adrenergic receptors
Reduce sympathetic symptoms:
- Tachycardia
- Tremor
- Sweating
- Palpitations
*Does not treat psychological anxiety directly
Beta Blockers (Propranolol, Atenolol) - Clinical Use
Performance anxiety (stage fright)
Public speaking
Test-taking anxiety (situational)
Performance-related tachycardia/tremor
Beta Blockers (Propranolol, Atenolol) - Key Advantages
- Non-sedating
- No dependence or abuse potential
- Rapid onset (taken PRN before event)
Beta Blockers (Propranolol, Atenolol) -Limitations
Does NOT treat generalized anxiety disorder, panic disorder (core symptoms)
Can cause bradycardia, hypotension, fatigue, hypoglycemia (masks also)
Avoid in asthma/COPD (nonselective agents like propranolol)
40-year-old female presents with:
Daily anxiety
Palpitations in social situations
Muscle tension
Wants “non-addictive PRN option”
Medical history:
Mild intermittent asthma
Uses albuterol PRN
Best PRN treatment?
A. Propranolol B. Buspirone C. Hydroxyzine D. Alprazolam E. Not indicated
✅ Answer: C. Hydroxyzine
(Hydroxyzine)
💡 Rationale:
Avoid beta-blockers due to asthma + albuterol use (so not A)
Non-addictive PRN option appropriate (so not D)
Buspirone long onset time (2-4 wks)