3_SCL+Fitting-Acc-Handout
1/124
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
125 Terms
What is included in the baseline examination for a new daily-wear soft contact lens wearer?
Assess patient needs
Perform comprehensive examination and fitting
Dispense appropriate soft contact lenses or place order
Provide insertion/removal (I&R) training
What happens at the dispensing visit for a new daily-wear contact lens wearer, and when is it scheduled?
Scheduled as needed, typically 1–2 weeks after baseline
Assess fit and vision of lenses
Reinforce insertion/removal training
If adjustments are needed: re-order lenses and schedule a new dispense
What is the purpose of the 1–2 week follow-up after successful dispense for a new contact lens wearer?
Evaluate fit, vision, and comfort
Ask about insertion and removal success
If problems remain: adjust, re-order, and schedule another dispense visit
What is the longer-term follow-up schedule for a neophyte daily-wear contact lens patient?
6-month follow-up: only as needed (rare)
Yearly exam:
Reassess needs
Perform comprehensive exam
Evaluate habitual lenses
Re-order or refit if needed
What is included in the baseline examination for a new extended/continuous wear contact lens patient?
Assess patient needs
Perform comprehensive examination and fitting
Dispense appropriate FDA-approved extended wear soft contact lenses or place order
What occurs at the dispensing visit for a new extended/continuous wear lens wearer, and when is it scheduled?
Scheduled as needed, 1–2 weeks after baseline
Assess fit and vision of lenses
If adjustments are needed: re-order and schedule a new dispense
What is the purpose of the 1-day follow-up in a new extended/continuous wear contact lens patient?
Occurs after first overnight wear
Scheduled the first morning after overnight wear
Evaluate fit, vision, comfort, and corneal edema
Ask about insertion and removal
If needed: adjust, re-order, and schedule new dispense visit
What is the purpose of the 6-month follow-up for extended/continuous wear lenses?
Long-term follow-up
Done to assess long-term hypoxic changes to the cornea from overnight wear
Reassess fit, vision, and comfort
What is included in the yearly examination for an extended/continuous wear contact lens wearer?
Reassess needs
Perform comprehensive examination
Evaluate habitual lenses
Re-order or refit as needed
What follow-up feature is especially important for extended/continuous wear compared with daily wear?
Next-morning (1-day) follow-up after first overnight wear
6-month follow-up to monitor for corneal hypoxic changes/corneal edema
What is done at the yearly examination for a veteran daily-wear contact lens patient?
Assess patient needs
Perform comprehensive examination
Evaluate habitual lenses
Re-order or refit as needed
What is the follow-up plan for a veteran daily-wear patient if no modifications are needed at the yearly exam?
No interim follow-up required
Patient returns at the next yearly examination
What happens if modifications are needed for a veteran daily-wear contact lens patient?
Dispensing visit scheduled 1–2 weeks after baseline/yearly exam
Assess fit and vision of lenses
If further changes are needed: re-order lenses and schedule new dispense
What is assessed at the 1–2 week follow-up after successful dispense in a veteran daily-wear patient?
Evaluate fit, vision, and comfort
Ask about insertion and removal
If adjustments are needed: re-order and schedule new dispense visit
When are the 1-3 month and 6-month follow-ups used in veteran daily-wear contact lens care?
1-3 month follow-up: rarely needed
Used to assess lens adaptation, especially if concerns arose at dispense
6-month follow-up: rarely needed
What are the components of a prefitting/comprehensive exam before contact lens fitting?
Typical routine exam procedures
Contact lens (CL) history
Measure corneal shape
Perform manifest refraction (vertex if needed)
Slit lamp exam, including eyelid eversion and tear film evaluation
Binocular vision (BV) evaluation is important
What corneal shape measurements are important in a contact lens prefitting exam?
Corneal curvature (Ks)
Corneal asphericity
Horizontal visible iris diameter (HVID)
Corneal sagittal depth
What special exam steps may be needed during contact lens prefitting beyond a standard refraction/slit lamp exam?
Vertex the manifest refraction if necessary
Perform eyelid eversion at the slit lamp
Evaluate the tear film
Assess binocular vision, since BV issues can affect lens success
Why are tear film, eyelid eversion, and BV evaluation important in contact lens prefitting?
Tear film affects lens comfort, stability, and vision
Eyelid eversion helps detect lid/conjunctival findings that may affect wear
BV evaluation identifies visual function issues that can impact contact lens success
At what types of visits can contact lens selection/fitting occur?
Stand-alone visit
Comprehensive exam
Dispensing visit
What lens care counseling is required during contact lens selection?
All lenses except daily disposables require a care/cleaning plan
What is a key difference in patient education between daily disposable lenses and other contact lenses?
Select modality: daily wear, extended wear, or continuous wear
Select replacement/disposal schedule
Select soft lens brand / base curve radius (BCR) based on sagittal depth
Determine lens power
What are the main contact lens modalities a clinician may choose from?
Daily wear
Extended wear
Continuous wear
What replacement/disposal schedules are available for soft contact lenses?
Daily
Weekly
Every 2 weeks
Monthly
Quarterly = every 3 months
Annually
How is a soft lens brand / BCR selected during contact lens fitting?
Chosen based on sagittal depth to help achieve an appropriate fit
What is important to remember about power determination/selection in contact lens fitting?
The needed lens power may not always be available in inventory
What is the difference between modality and replacement schedule in contact lens selection?
Modality = how the lens is worn (daily, extended, continuous wear)
Replacement schedule = how often the lens is replaced/disposed (daily, biweekly, monthly, quarterly/3 months, etc.)
What are the main steps in assessing contact lens fit after selecting a lens?
Determine if the lens must be ordered or is available
Apply lenses to the eye
Allow appropriate settling time
Assess fitting relationship
Check visual acuity
Perform over-refraction
Do surface evaluation at comprehensive and progress checks
What is evaluated in the fitting relationship assessment of a contact lens?
Centration
Coverage
Movement
Push-up test
Why is settling time important before assessing contact lens fit?
Allows the lens to stabilize on the eye
Prevents judging fit too early before the lens reaches a more representative position/movement pattern
What is the purpose of checking visual acuity and doing an over-refraction during contact lens fitting?
Visual acuity: assesses how well the patient sees in the trial lens
Over-refraction: refines residual refractive error to determine whether a power change is needed
When should surface evaluation be performed in contact lens fitting?
At comprehensive exams
At progress checks/follow-up visits
What are the steps in a contact lens dispensing exam?
Check entrance visual acuity with habitual correction
Take a brief interval history (ask about any changes)
Assess lens fit
Decide whether to dispense/educate or reorder and repeat dispensing exam
What should be reviewed at the start of a dispensing exam?
Entrance VA with habitual correction
Brief history to identify any changes since the previous visit
Fitment assessment
What are the two possible outcomes of a contact lens dispensing exam?
Educate patient and send home to try lenses
May require insertion and removal (I&R) training
Reorder lens and repeat dispensing exam
When can you proceed with dispensing soft contact lenses to the patient?
Proceed if:
Acuity is acceptable
Fit is acceptable
Over-refraction is minimal
What should be done if the dispensing exam shows good fit/vision but a slight power change is needed?
You may send the patient home with the lenses
Reorder a slight power update if needed
What should be done if lens acuity, fit, or over-refraction is not acceptable at the dispensing visit?
Start re-fitting rather than dispensing the current lenses
How long should a soft contact lens dispensing visit usually take?
20 minutes or less
What questions should be asked about a patient’s contact lens type and wearing history?
What lens(es) are worn?
How many years has the patient worn them?
What is the wear schedule?
What is the disposal/replacement schedule?
What compliance-related questions are especially important when taking a contact lens history?
How often do you sleep in your contact lenses?
What solutions do you use?
Do you wash your hands before handling lenses?
What are the main domains to cover in additional contact lens history questions?
Lens type and duration of wear
Wear and replacement schedule
Sleeping in lenses
Lens care solutions
Hand hygiene
Lens case hygiene
How is central corneal curvature measured during contact lens fitting?
Keratometry (“Auto Ks”)
Corneal topography (Ks and Asphericity)
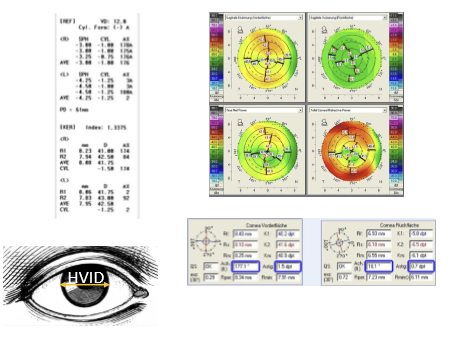
What is HVID, and how is it measured?
HVID = Horizontal Visible Iris Diameter
Can be measured with a PD ruler or corneal topography
WTW (white-to-white) is generally greater than HVID
What are the typical average corneal curvature and astigmatism values used in contact lens fitting?
Mean corneal power/curvature: 43.50 ± 1.7 D
Mean corneal astigmatism: 0.9 ± 1.1 D
What is the typical HVID in contact lens fitting?
Average HVID = 11.50 mm
Typical range: 10 to 13.5 mm
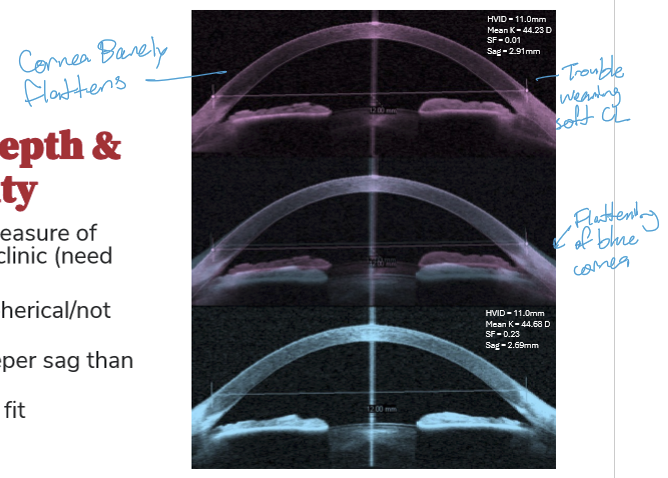
Why is corneal asphericity important in contact lens fitting?
Corneal asphericity affects corneal sagittal depth (sag)
A cornea that is unusually spherical / less aspheric has deeper sag than a more aspheric cornea
These eyes are often more difficult to fit, especially with soft contact lenses
What fitting problem can occur if the cornea is not very aspheric (more spherical / barely flattens toward the periphery)?
The cornea has a deeper sagittal depth
This can make soft contact lens fitting more difficult
Why is corneal asphericity not always routinely available in clinic?
It usually requires corneal topography
It is not commonly measured directly in routine clinic without topography
What is the difference between axial maps and tangential maps on corneal topography?
Axial maps: best represent the optical characteristics of the cornea; commonly preferred in refractive surgery
Tangential maps: represent true/local curvature better and provide better peripheral shape information; preferred in contact lens practice
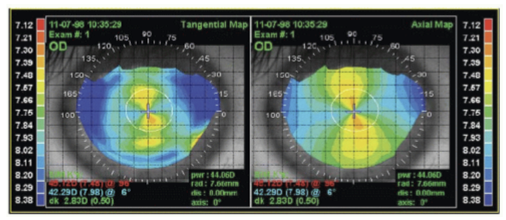
Which corneal topography map is generally preferred in contact lens practice, and why?
Tangential map: Better reflects true curvature data and peripheral corneal shape, which is important for contact lens fitting
What is corneal sagittal depth?
The height/depth of the cornea over a specified chord diameter
It helps describe overall corneal shape in a way that is useful for contact lens fitting
What is the average corneal sagittal depth?
Mean sagittal depth ≈ 2.74 mm
Why is corneal curvature alone not enough for contact lens fitting?
Corneal curvature alone does not fully explain how deep or shallow a contact lens must be to fit well
Sagittal depth gives a better overall description of fit requirements
What clinical outcomes are associated with sagittal depth in contact lens fitting?
Adverse events
Discomfort
Contact lens dropout
What factors determine corneal/contact lens sagittal depth?
Corneal curvature
HVID
Asphericity
Why is sagittal depth clinically important in soft contact lens fitting?
Helps estimate how deep/shallow the lens fit should be
Better predicts fit than K readings alone
Relevant to comfort, safety, and long-term lens success
What is the sagittal depth formula for a spherical surface in contact lens fitting?
s = r − (r² − h²)^(1/2)
Where:
s = sagittal depth
r = radius of curvature
2h = chord diameter
Why are contact lenses described as “thick lenses” in the context of sagittal depth?
Because the sagittal depth is short relative to the chord diameter
What important limitation does the basic sagittal depth formula have?
It is simplified and does not account for asphericity
If a soft contact lens does not match the cornea, what two lens parameters can be changed to alter sagittal depth?
2h = lens diameter / OAD
r = lens curvature / BCR
Why does changing soft lens sagittal depth often require choosing a different brand?
Because soft lens manufacturers often offer only one fit within a given brand/lens design
If more sagittal depth modification is needed, clinicians often switch to a different brand
What is the clinical goal of sagittal depth in contact lens fitting?
To align the contact lens to the cornea
Matching lens sagittal depth to corneal sagittal depth helps achieve an appropriate fit
What is an important limitation of AS-OCT when measuring sagittal depth with a contact lens on the eye?
The AS-OCT does not know a contact lens is on the eye
The image is not adjusted for the lens refractive index
This can affect interpretation of the upper image / lens-related measurement
How should sagittal depth measurements be oriented on AS-OCT if you are not measuring along the first surface?
Keep measurements parallel to the scanning beam
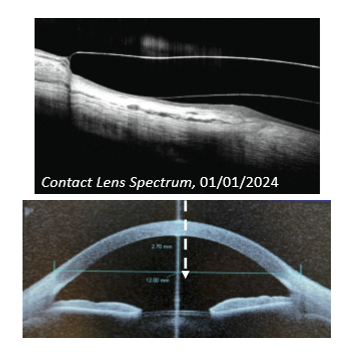
What are the two technical notes for measuring corneal sagittal depth on AS-OCT?
AS-OCT images are not corrected for the contact lens refractive index
If not measuring from the first surface, keep the measurement parallel to the scanning beam
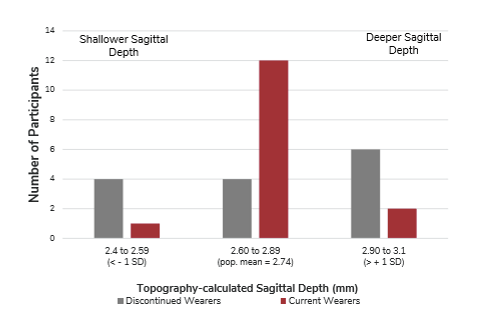
What was a common finding for patients who did not have a good fit with the contact lens?
Shallower-than-average corneal sagittal depth
How is corneal sagittal depth related to contact lens dropout?
Discontinued wearers were more often found at the extremes of corneal sagittal depth
Dropout was associated with both shallower and deeper corneal sagittal depths
Current wearers were more often found in the middle of the population distribution
Why can Ks and HVID alone fail to explain contact lens dropout?
A patient may have typical K readings and typical HVID, yet still have abnormal overall corneal shape
Asphericity/sphericity can change sagittal depth even when Ks and HVID look normal
What symptom were common in discontinued contact lens wearers?
Discomfort symptoms, especially feeling like they had dry eye while wearing contact lenses
Why might some doctors intentionally avoid prescribing small amounts of cylinder in glasses for a spherical contact lens wearer?
For low cylinder amounts (about 0.25 to 0.50 D)
Some doctors leave it out so the patient can switch more easily between glasses and spherical contact lenses
What are the main options for measuring vertex distance?
Phoroptor/phoropter vertex gauge
Gauge on trial frame
Distometer
What are the drawbacks of the phoroptor/phoropter vertex gauge?
Difficult to read
Difficult to monitor patient during refraction to make sure the distance stays consistent
Where is the gauge on a trial frame located, and what is its limitation?
Located on the side of the trial frame
Less precise than a distometer
Which method is generally more precise for measuring vertex distance: trial frame gauge or distometer?
Distometer is more precise
Trial frame gauge is less precise

What is the general procedure for measuring vertex distance with a distometer?
Place refraction in trial frame
Perform a binocular sphere check
Have the patient close their eyes
Measure vertex distance with the distometer
Add 1 mm unless that correction is already built in by the manufacturer (to account for eyelid thickness)

What major decisions must be made when selecting a contact lens disposal schedule and modality?
Choose modality: Daily Wear (DW) vs Extended Wear (EW)
Consider oxygen needs
Choose replacement schedule: daily disposable vs planned replacement
Consider tints and handling
What factors should guide the choice between daily wear vs extended wear and different replacement schedules?
Oxygen needs
Desired wear modality (DW vs EW)
Replacement frequency (daily, 1–2 week, monthly, quarterly)
Patient factors like handling and preference for tints
What is the general relationship between replacement frequency and contact lens outcomes?
More frequent replacement = better vision, comfort, and ocular health/ the more frequently a lens is replaced, the fewer complications occur
What are the advantages of daily disposable contact lenses?
Lowest overall complication rate
Lowest level of deposition
Often associated with good vision and sometimes improved comfort
Fewest unscheduled visits (less chair time)
What is the main drawback of daily disposable lenses?
Cost may be difficult for some patients
Why are daily disposables often preferred clinically?
Fewest unscheduled visits
Great vision
Sometimes improved comfort
Fewer overall complications
Less deposition
What is the main risk with extended or continuous wear CL?
They have the highest overall complication rate.
How do complication rates of disposable EW lenses compare with conventional (non-disposable) EW lenses?
The complication rates are approximately the same
Simply making the lens disposable does not eliminate the higher risk of EW
Why do many patients want extended wear, and why is this clinically important?
Many patients want EW because they are bad at insertion and removal
This is important because convenience may drive demand despite increased risk
Why do many clinics require a consent form/policy for extended wear contact lenses?
Because fitting a patient in EW involves extra risk
Most practices use a consent form to document risk discussion and patient understanding
How is sagittal depth used when selecting a soft contact lens (SCL) brand or base curve radius (BCR)?
For soft contact lenses, clinicians often estimate the patient’s sagittal depth
This helps predict which lens design/brand will fit best
How should you use K readings + HVID when choosing an initial soft contact lens?
Use central corneal curvature (K) and HVID to estimate whether the patient likely needs a shallower or deeper lens
What corneal features suggest a shallower soft lens vs a deeper soft lens?
Shallower lens: flatter K + smaller HVID
Deeper lens: steeper K + larger HVID
How is soft contact lens power determined?
Based on the vertexed manifest refraction
Use spherical or spherical equivalent for low cylinder amounts
Use a toric lens when cylinder is significant
When is a toric soft contact lens usually needed?
Typically when cylinder is ≥ 1.00 DC
Often considered starting at ≥ 0.75 DC
How should the trial lens power be chosen after calculating the predicted CL power?
Choose the trial lens closest to the predicted power
Remember that higher powers may only be available in 0.50 D steps
What are the characteristics of an ideal soft contact lens fit?
Produces good, stable vision
Is comfortable
Is wearable for practical periods of time
Causes minimal physiological response
What does an excessively tight soft contact lens fit risk causing?
Increased physiologic response
Can lead to irritation and inflammation
Why is tear exchange important in a soft contact lens fit?
Tear exchange helps remove debris/inflammatory material from under the lens
However, tear exchange is difficult to achieve with soft lenses
How much tear exchange occurs with blink in even a “good” soft contact lens fit?
Very little / almost none
Roughly ~2% with blink
High-yield implication: debris and inflammatory products can remain under the lens
What is the minimum settling time before assessing a newly applied soft contact lens?
Allow at least 10 minutes of settling time
During this time, check whether the lens is grossly too small or too tight
Record the fit assessment after the lens settles
Why may a soft contact lens fit need reassessment after 3 to 4 hours or 1 to 2 weeks?
Soft lenses dehydrate on the eye over time
Because of this, the fit may change/tighten after longer wear
Especially important if the patient has poor tear volume
How does poor tear volume affect soft contact lens fit over time?
Soft lenses can dehydrate on the eye
With poor tear volume, the lens fit may tighten over time
What are the 3 main things assessed when evaluating a soft contact lens fit?
Coverage of the cornea/limbus
Centration over the cornea
Movement with blink / eye movements