Gen Med: Lines and Monitors
1/28
Earn XP
Description and Tags
zoeolsen
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Patient monitor purpose
used for continuous monitoring of cardiovascular and pulmonary systems
(Electrocardiogram, pulse oximetry, blood pressure, respiratory rate, body temperature, advanced hemodynamics , intra-cranial pressure)
Patient monitor: therapy considerations
-look into portable devices
-PT needs to push patients BUT need to dose it appropriately
-PT needs to be able to interpret the monitor (if waveform is gone..is the machine working?)
Peripheral IV purpose
used to deliver intravenous fluids or medications
(commonly: dorsal hand, wrist; cubital fossa; dorsal foot)

Peripheral IV therapy considerations
-PT needs to ensure vein is not occluded during ROM
-PT needs to watch for redness or signs of infection
-careful not to pull on lines
-veins can collapse
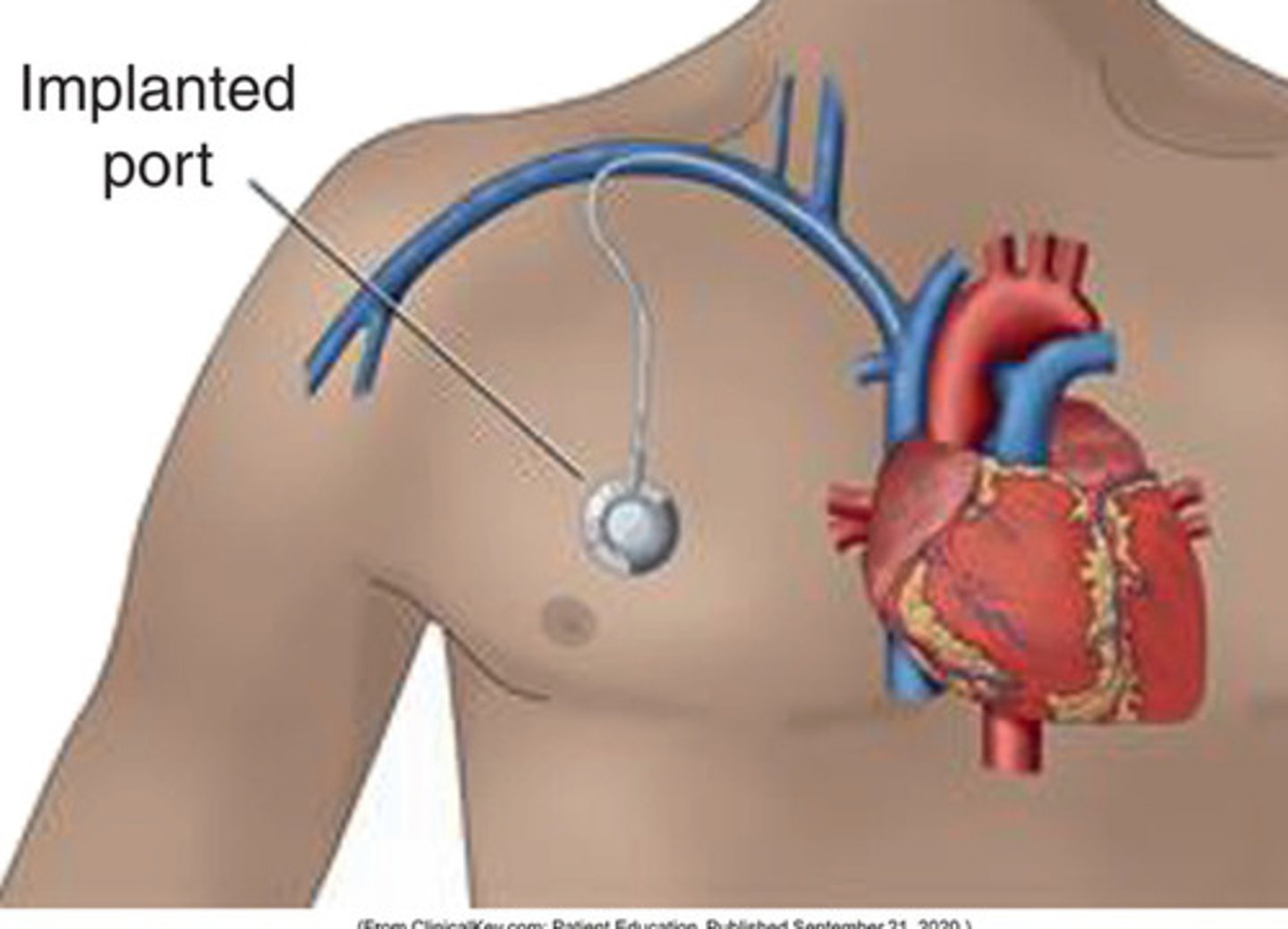
Central lines purpose
-used for central venous access (jugular, subclavian, femoral)
-allows for monitoring of central venous pressure or right atrial pressure
-route for medication delivery, fluid administration, blood sampling, TPN
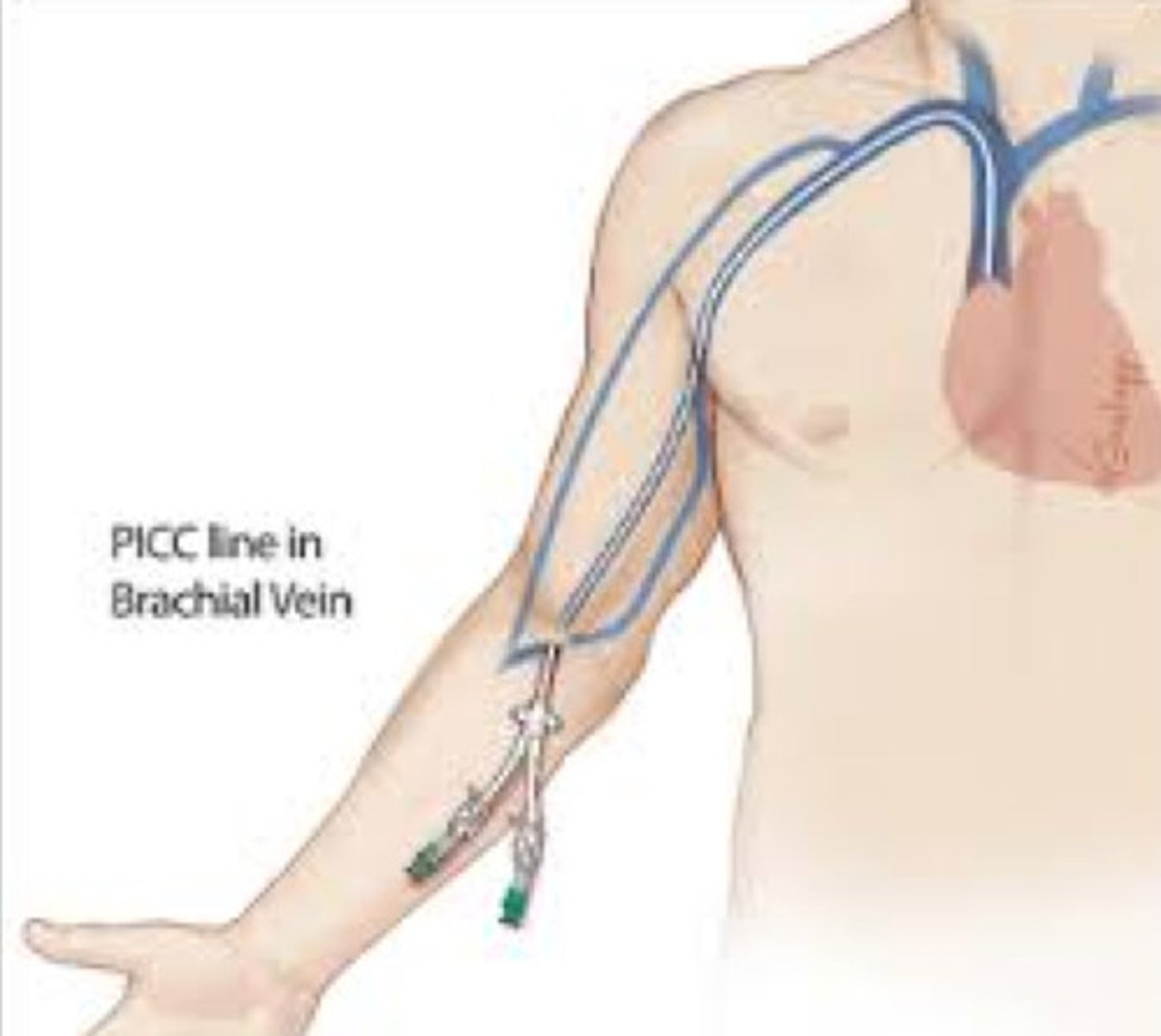
-peripherally inserted central catheter (PICC) line: typically placed in upper arm

Central venous lines: dialysis catheters
Mahurkar, permacath
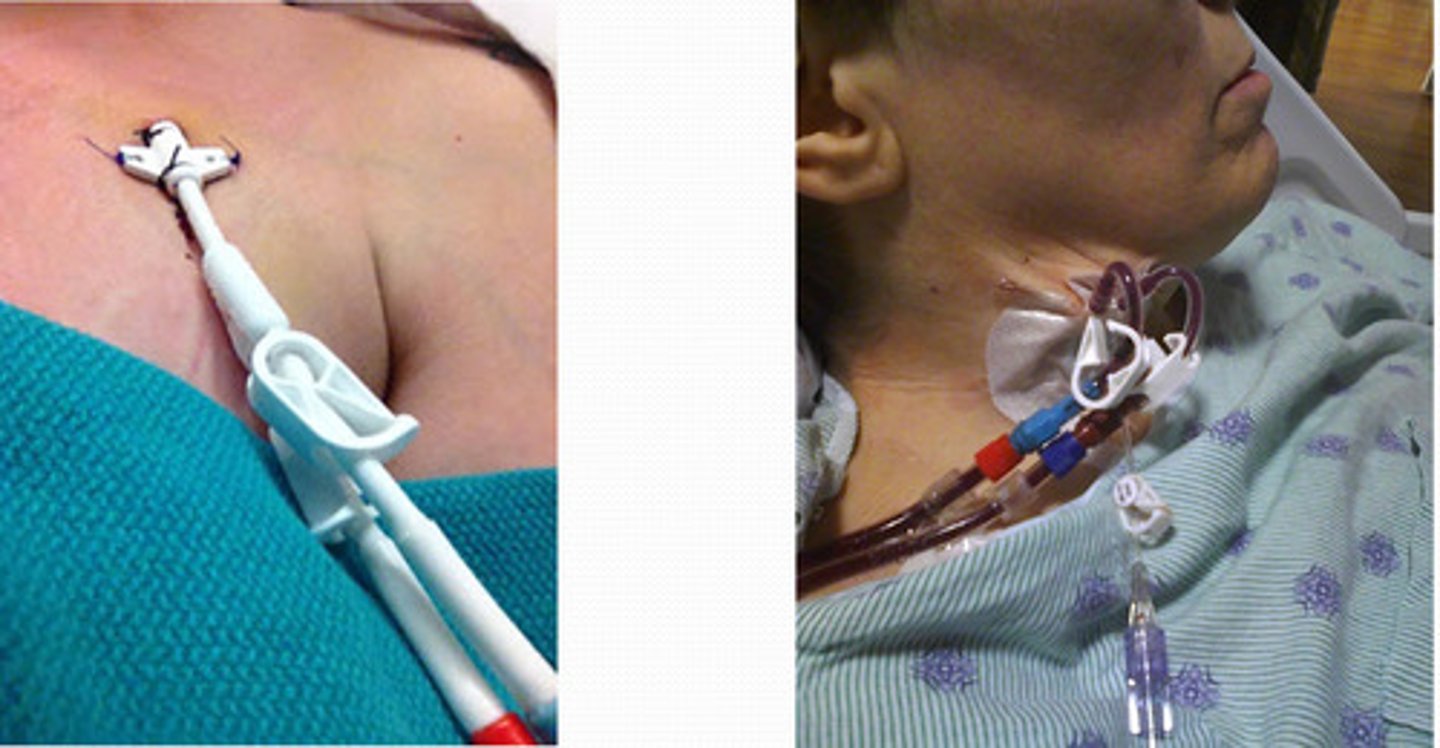
Central venous lines: tunneled
allow for long term access
Peripherally inserted central catheter line PICC
typically placed in upper arm
Central line therapy considerations
-don't pull out the line, watch it, and support
-caution with neck and arm motions
Swan-Ganz or PA catheter purpose
-placed in central vein and is most invasive to measure: CVP, right atrial pressure, pulmonary artery pressure, pulmonary wedge pressure, cardiac output and cardiac index, calculation of systemic and pulmonary vascular resistance, temporary pacing
-advanced to superior vena cava -> R atrium -> R ventricle -> pulmonary artery

Swan-Ganz or PA catheter therapy considerations
-Patient may be unstable
-avoid pulling because it can damage the heart causing: malignant arrhythmias, pulmonary artery, rupture, pulmonary valve tear or infection
**for these reasons it is recommended that mobilization, if essential, only be undertaken by an experienced clinician after it has been determined that the patient is hemodynamically stable
Arterial line purpose
-allows continuous blood pressure measurement and sampling of arterial blood (MAP - mean arterial pressure and ABGs - arterial blood gases)
-usually placed radial or femoral

Arterial line therapy considerations
-if pulled out = bad blood will go everywhere due to high arterial pressure
-transducer must be at level of right atrium to have accurate reading
-change in body position, bed position or ROM can change reading
-avoid wrist motions
ICP monitor purpose
catheter placed through skull into epidural space, subarachnoid space, or directly into ventricle to measure pressure and/or drain cerebral spinal fluid
(normal ICP < 10 mmHg)
ICP monitor therapy considerations
-elevated levels can lead to brainstem compression and reduced cerebral blood flow which can lead to brain injury
-high infection risk
-avoid resistance/isotonic exercises that would drive up pressure (no isometric or valsalva)
-gravity will influence so these patients will typically be elevated instead of head down position
-be aware of coughing during activity
Chest tube purpose
-used to drain excess air or fluid from pleural space or mediastinum
-tube connected to drainage system and collection box, usually placed on floor next to bed
-can be placed to suction or water seal
Chest tube therapy considerations
suction needs to remain below the level of insertion unless they are on suction
Chest tube contraindications
cannot move the patient if suction is connected to the wall
Drains purpose
-drain fluid from body cavity or surgical site
-consist of small collection
-may use suction or gravity; Examples: Jackson-pratt drains, hemovac, j-vac, wound vac
Drains therapy considerations
-pin to the gown when you are doing treatment to prevent drain from ripping out
-easy to lose and if gets taken out they have to go into a procedure to get back in
Foley catheter purpose
indwelling catheter, inserted in urethra, sits in bladder to drain urine and is held in place with balloon inflated in bladder
Foley catheter therapy considerations
-must be below level of insertion
-do not pull because it can damage urethra
-tripping hazard
NG tube purpose
placed in through the nose and ending in stomach or small intestines to suction to remove stomach contents (common after surgery to await return of GI function or NPO status) or for nutrition (smaller caliber than tube for drainage)
NG tube therapy considerations
-must check number prior to and after treatment to make sure tube is not coming out of the stomach
-might not use a gait belt if it will dislodge line ... do not put gait belt on top
NG tube therapy contraindications
-patients head should always be above 30 degrees of flexion because patient can aspirate (can be unelevated for a minute or two otherwise you must pause it which we don't like to do)
Oxygen delivery devices purpose
-used to provide supplemental O2 to patients that have decreased saturation levels
-can have nasal cannula (1-6 L/min), high flow nasal cannula, simple mask (5-10 L/min), aersol mask, venturi mask, reservoir masks, non invasive positive ventilation (BiPAP/CPAP, continuous/bilevel positive airway pressure, short term ventilatory support, used to prevent or wean off mechanical ventilation, delivered with fitted face/nose mask), ventilator, low flow supplemental oxygen (can be humidified for comfort), high flow nasal cannula (high amounts supplemental oxygen up to 60 L/min, oxygen is heated and humidified, larger diameter tubing, snug nasal prongs ex: optiflow, vapotherm),
Oxygen delivery devices therapy considerations
-monitor saturation levels
-look at order to see if you can increase amount of O2 during treatment
-if still not saturating high enough at 6 L then think about switching mask
Endotracheal and tracheostomy tubes purpose
artificial airway to provide ventilation and oxygenation in respiratory failure
-speaking valves can be placed over trach opening to allow patient to vocalize (patient may receive supplemental oxygen)
Endotracheal and tracheostomy tubes therapy considerations
-watch for skin deterioration around trach
-watch for vitals to make sure patient is within normal ranges especially with O2