sexuality + health promotion ❤
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
sexual health
is an essential element of overall health and wellbeing that healthcare providers and patients often do not discuss
while many patients have sexual history questions and want a providers insight....
they may be hesitant to start the conversation
by asking adult and adolescent patients a few essential questions you helped remove
the stigma around discussing sex and normalizing these discussions
a sexual history should be taken as part of
our routine health care as well as when there are s/s or physical exam
when assessing a pts sexual health you will look at
social history + and get a complete health picture
when obtaining a complete health picture you will ask about
sexual preferences + sexual practices + sexual identity when dealing with sexuality + also health and risk promotion!
health promotion education includes
support groups + educate about condoms and contraceptives
normal erectile function includes
nerve stimulation of blood flow into corpus cavernosum + the rapid influx of blood causes the penis to straighten and expand + the higher rate of blood flow into corpus cavernosum and a limitation in blood outflow are maintained in sexual arousal continues + balance of brain, emotions, hormones, nerves, muscles and blood vessles leads to normal male sexual arousal
erectile dysfunction (ED)
repeated inability to initiate or maintain an erection sufficient for sexual intercourse
erectile dysfunction (ED) pathophysiology
disruptions in the complex interplay between the vascular + neurological + hormonal and psychological systems
the most common biologic cause of ED is
neurological and vascular disorders such as neuropathy from diabetes mellitus and or atherosclerosis of penial arteries
ED becomes more common
as men age but simply growing older is not the primary cause of ED + men of any age can occasionally experience ED which should not cause excessive concern
the prevalence of ED increases
with age from 8% of men in 20's and 30's + 18% of men in 50's + 25% of men in 60's + 37% of men in 70's + 80% of men in 80's (true incidence of ED is higher due to under reporting of condition)
about 40% of cases of ED in men that are older than 50 are attributed to
atherosclerosis + diabetes + neuropathy + vascular disease
risk factors of ED include
chronic depression + anxiety + PTSD + intrapersonal or intimacy issues + strict upbringing + inadequate sex education + life stressors + surgeries such as prostatectomy and or radiation therapy due to prostate or colon cancer + smoking + alcohol + low energy levels
what are the 2 biggest risk factors for ED?
PTSD and STRESS
again the medical diagnoses that impact risk of ED include
diabetes + hypertension + hyperlipidemia + atherosclerosis + chronic liver failure + COPD + genetics + obesity + poor diet + chronic insomnia or sleep related disorders + low testosterone (hypogonadism) + decreased sexual energy (low libido) + mood disturbances
clinical presentation of ED should include
patient history + laboratory tests + other diagnostics
laboratory tests to assess ED include
testosterone levels + urinalysis + renal function
ED t/x includes
referral to urology or ED speciality to evaluate physiological causes + risk and benefits of non invasive t/x + pharmacological t/x
PDE-5 Inhibitors for ED
sildenafil and tadalafil (think meds ending in -fil help fill the penis with blood to get erect)
PDE-5 Inhibitors are CONTRAINDICATED when
taking nitroglycerin for heart conditions
PDE-5 Inhibitors are used with CAUTION in men using
alpha adrenergic blockers (tamsulosin (flomax) in those that had a myocardial infarction in past 6 months + resting hypotension + uncontrolled hypertension
tamsulosin (flomax) is used for
BPH to help urine flow
PDE-5 Inhibitors side effects
headache + flushed feeling + nasal congestion + mild visual disturbances + priapism
priapism
a painful erection that lasts 4 hours or more but is not accompanied by sexual excitement
testosterone (pharmacological t/x)
it is only effective if ED is caused by clinically low testosterone (hypogonadism). even then, TRT primarily improves libido (sex drive) and may only slightly enhance the effectiveness of erection
family planning is defined as
the spacing of conception of children according to wishes of the parents rather than to chance + accomplished by practicing some form of birth control
people may choose different contraceptive methods based off
safety + effectiveness + availability + side effects + user control + ease of removal or discontinuation
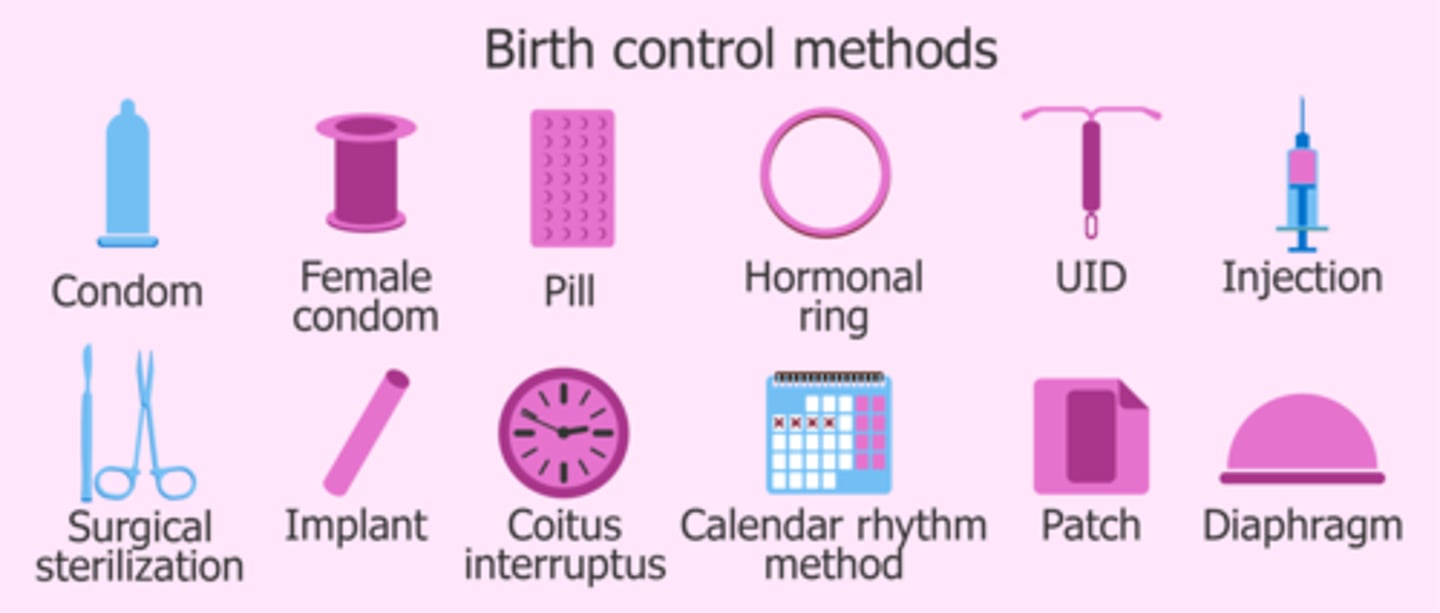
contraception (birth control) should be chosen via
voluntary and informed choices
most contraceptive methods DO NOT protect against
STI including HIV
using condoms can help protect
against HIV and other STI's
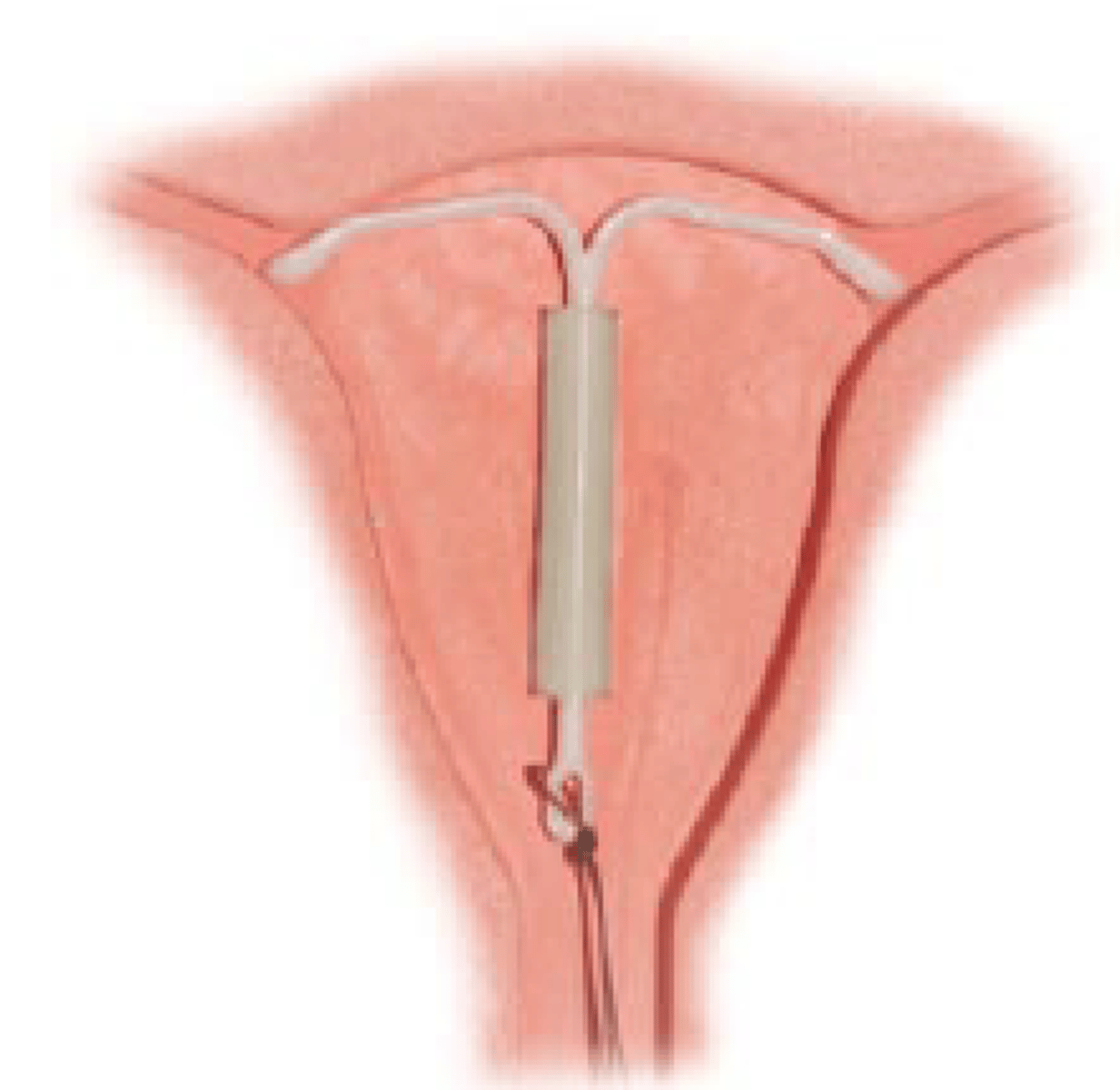
IUD (intrauterine device)
placed inside uterus by a doctor + works by releasing a small amount of progestin each day to keep you from getting pregnant + typically stays from 3 to 10 years
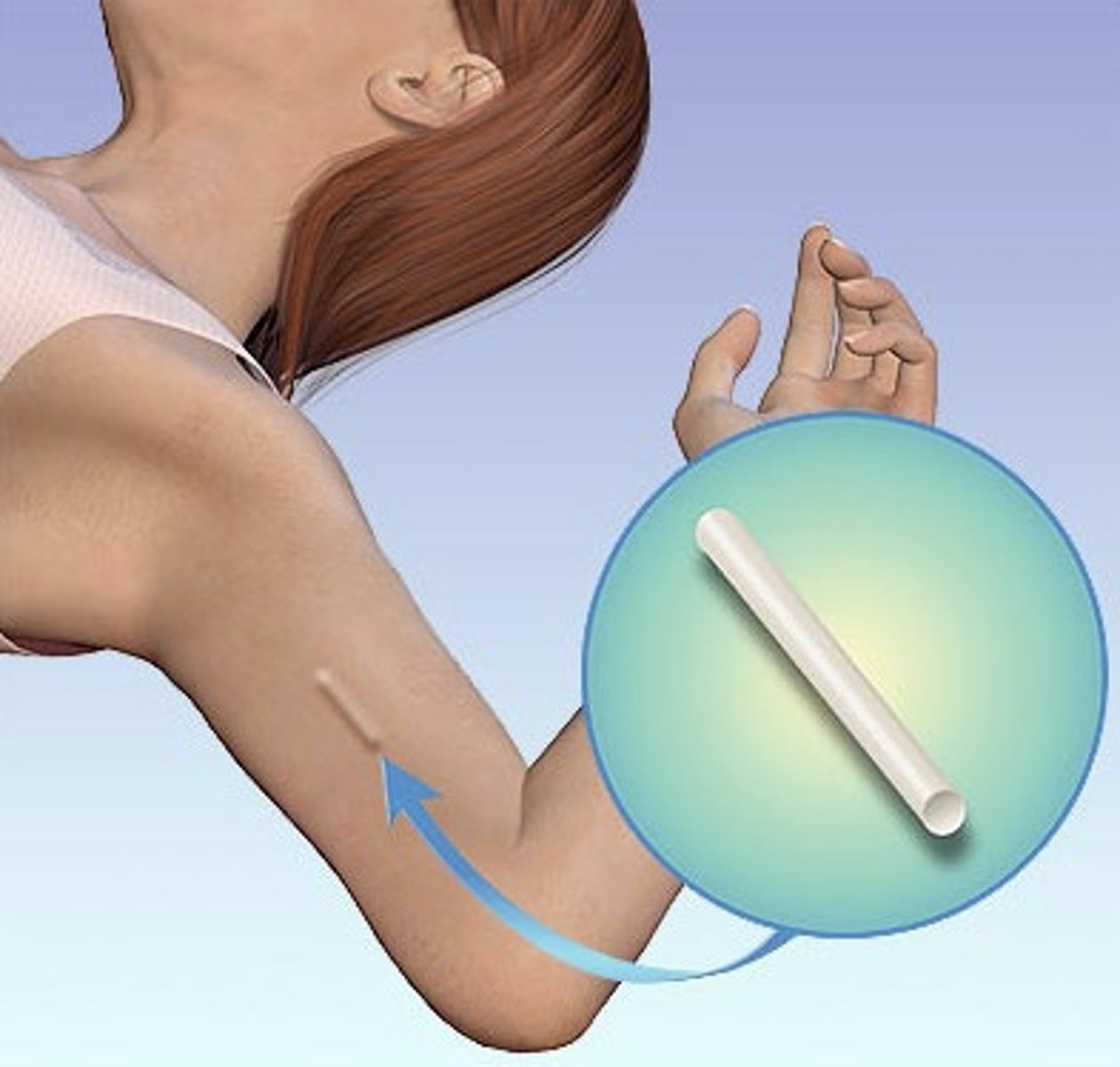
implant
single thin rod that is inserted under the skin of a women's upper arm + rod contains a progestin that is released into the body over 3 years
injection or birth control shot
women get shots of hormone progestin in buttock or arm every 3 months + can be self or provider administered

combined oral contraceptives (the pill)
combination of estrogen and progestin hormones + prescribed by doctor + taken daily at the same time + if you are older than 35 y/o and smoke, have a h/x of blood clots or breast cancer your doctor may advise you against taking it
progestin only pills (mini pill)
only contains progestin and NO estrogen + taken daily at the same time + good option for women who can not take estrogen
birth control patch
worn on the lower abdomen, buttocks, upper body but NOT breasts + prescribed by a provider + releases estrogen and progestin hormones to the blood stream via topical route + new patch 1x a week for 3 weeks and during 4th week they will NOT wear it so they can have a menstrual period

hormonal vaginal contraceptive ring
ring releases the hormones progestin and estrogen + place the ring inside your vagina + you wear the ring for three weeks, take it out for the week you have your period and then put in a new ring after cycle

diaphragm or cervical cap
before sexual intercourse the diaphragm or cervical cap is inserted in the vagina with spermicide to block or kill sperm + prescribed by provider

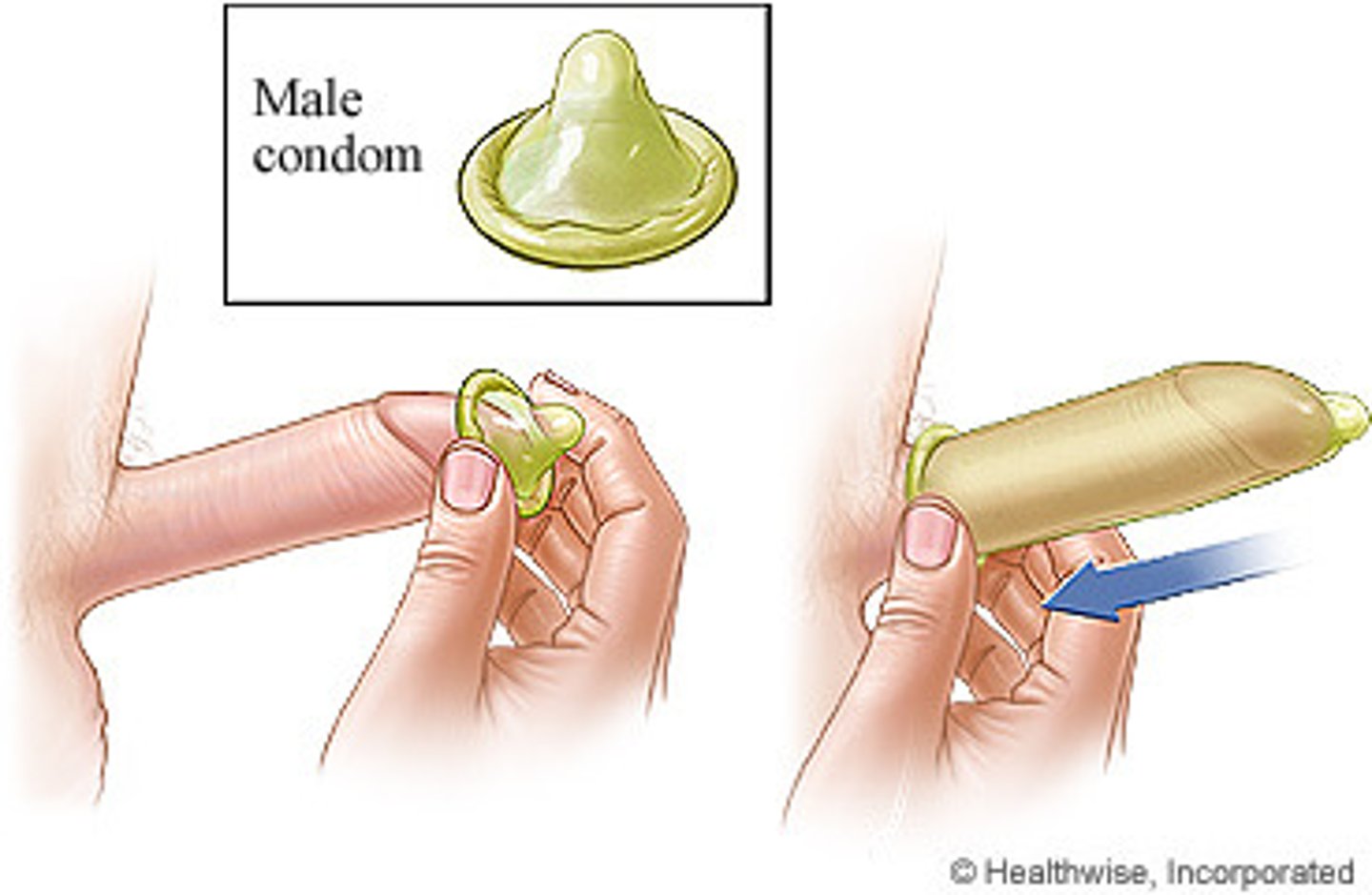
male condoms
covers the penis + keeps sperm out of the vagina + latex condoms (most common type) help protect against STI's and HIV + available OTC
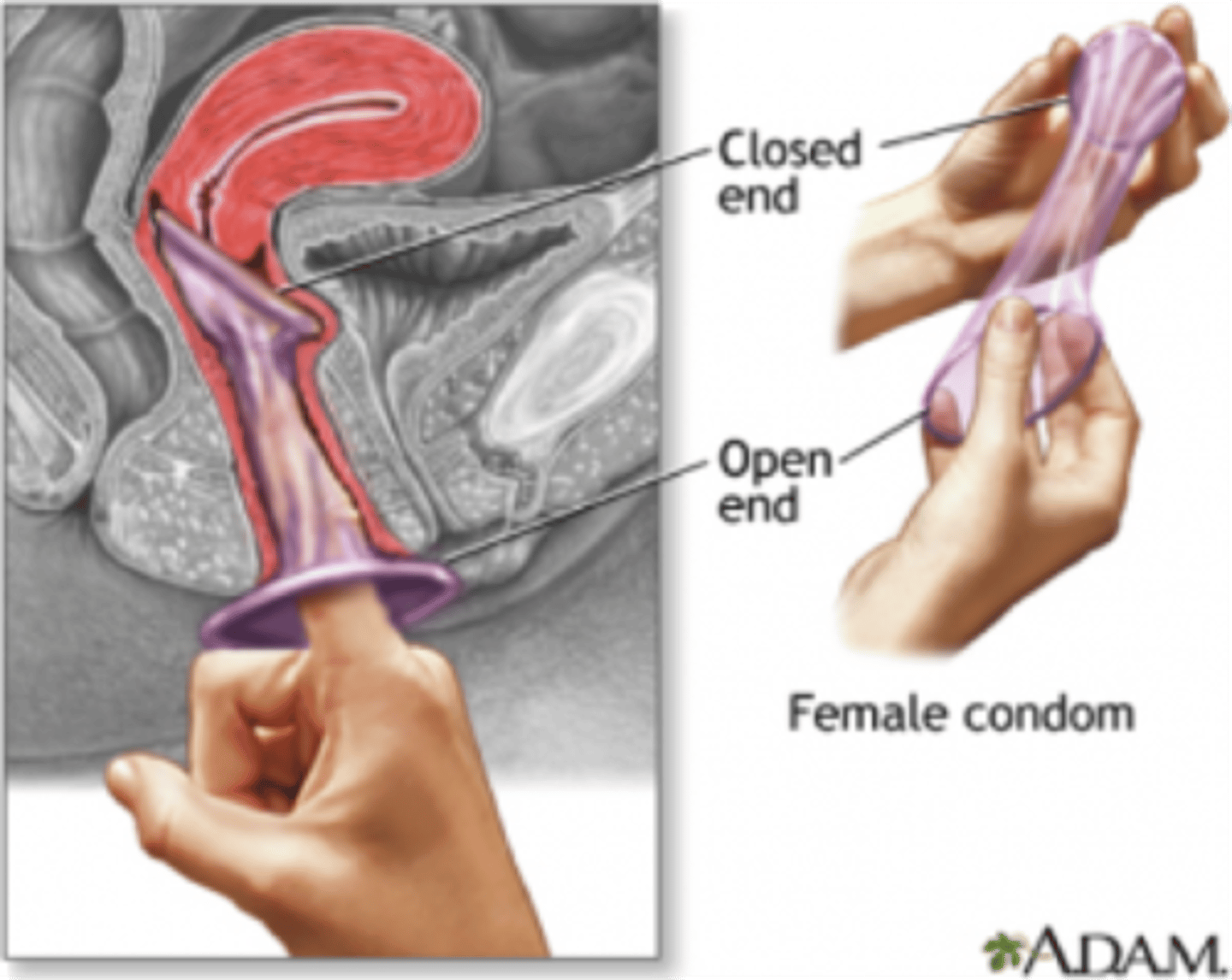
female condoms
internal and help prevent pregnancy by blocking sperm getting to the egg + packaged with lubricant + available OTC + can be inserted up to 8 hours before intercourse + might help prevent STI's
calendar rhythm method
takes account of variability in the length of a woman's menstrual cycles + can help plan to get pregnant or avoid getting pregnant

coitus interruptus
pull out method
surgical contraceptive methods
tubal ligation ("tying the tubes") fallopian tubes are tied, closed or cut so sperm and eggs can not meet for fertilization (can be same day surgery or out patient hospital) also effective immediately + vasectomy is done to keep sperm from going to the penis so ejaculate never has any sperm in it that can fertilize an egg (outpatient surgical center) follow up after 12 weeks to ensure sperm count has reached 0!
fertility pattern is
number of days of the month when you are fertile + days you are not fertile + days when in fertility is unlikely but possible + if you do not want get pregnant do not have sex on days you are most fertile or use some sort of contraceptive method
infertility
the inability to conceive a child or get pregnant after 1 year or longer after having unprotected sex
infertility statistics
in the US 1 in 5 married women ages 15-49 y/o women with no prior births are unable to get pregnant after 1 year or longer after having unprotected sex + 1 in 4 in this group have difficulty getting pregnant and or carrying it to term
conditions that can contribute to infertility include
polycystic ovary syndrome + diminished ovary reserve + impaired function of the hypothalamus and pituitary glands + premature menopause + fallopian tube obstruction + abnormalities of the uterus
what increases risk of infertility in women?
age + smoking + excessive alcohol use + obesity + underweight + EXTREME weight gain or loss + excessive emotional or physical stress that results in absent periods
infertility in men
disruption of testicular or ejaculatory function + hormone and genetic disorders
t/x options of infertility include
timed intercourse + medications + intrauterine insemination + surgery + assisted reproductive technology
menopause
when a women has not had a menstrual cycle in more than 1 year + normal part of aging + mainly occurs in women 40 to 58 y/o
before age of 40 woman can experience
perimenopause! s/s that mirror menopause
menopause occurs when
estrogen and progestin hormones become lowered + ovaries stop releasing eggs when hormones are too low
what other factors may cause menopause to occur
having surgery to remove the uterus or ovaries + cancer t/x
early menopause
when a women before 40 has not had a menstrual cycle in more than 1 year
early menopause risk factors include
smoking + cancer t/x + having surgery to remove the uterus or ovaries + use of oral bc + low body fat + having a mother who has been given DES when pregnant
DES is
diethylstilbestrol a synthetic estrogen medication
menopause s/s
may be asymptomatic + can effect every body system + irregular periods + hot flashes + night sweats + problems sleeping like insomnia + vaginal dryness + discharge + itching + pain w/sex
women who do not have many symptoms
have them leading up to menopause
menopause diagnosis includes
provider asking about symptoms + past health + physical exam + asking about periods + blood test may be done to look for follicular stimulating hormone (FSH)
high levels of FSH suggest
menopause
t/x of menopause
NONE it is apart of normal life so just manage hormones with medicine and general care
HRT's (hormone replacement therapy)
such as estrogen + progesterone or testosterone class of medications that can be used for a short time as pills and injections (used to ease s/s of menopause) + but INCREASES RISK OF BREAST CANCER!
non hormone options include
certain bp meds + antidepressant meds + antiseizure meds (used to ease s/s of menopause)
self care t/x of menopause
balanced diet (veggies + fruit + whole grains) + regular physical activity each day + relaxation methods to ease stress + good sleep habits + no smoking + moderate or no alcohol + vaginal lubricants for dryness + thin layer to help with night sweats + cool drinks or cooling towels to help heat flashes
menstrual cycle
a monthly series of changes the body goes through in preparation for the possibility of pregnancy + each month one of the ovaries releases an egg (ovulation) + hormonal changes at this time get the body ready for pregnancy + if the released egg is fertilized during ovulation then the lining of the uterus sheds through the vagina (period)
on average, the normal menstrual cycle is one in which a woman menstruates is
every 28 day (varies in length)
menstrual dysfunction includes
absent periods + heavy menstrual bleeding + irregular periods + painful periods + light periods + prolonged bleeding + bleeding between periods
causes of menstrual dysfunction include
hormonal imbalances + stress + eating disorders + excessive exercise + certain medications + uterine fibroids + endometriosis + thyroid issues + pelvic inflammatory disease
STI's have a
direct impact on sexual and reproductive health through stigmatization + infertility + cancer + pregnancy complications and can increase risk of HIV
drug resistance is a major threat to reducing
the burden of STI's worldwide
more than 1 million curable STI's are acquired
every day worldwide in people between the ages of 15 and 49 + majority is asymptomatic
prevention of STI's includes
condoms are most effective prevention method when used correctly and consistently
s/s of STI's include
mainly asymptomatic but when s/s occur they can be non specific
diagnostic for STI's includes
molecular technology that is widely used in high income countries mainly used in asymptomatic infections
t/x of bacterial STI's (chlamydia + gonorrhea + syphilis + trichomoniasis) are generally curable with
SINGlE DOSE regimen of antibiotics
trichomoniasis is actually a
parasitic STI
herpes and hiv t/x is
antivirals (-vir) medications that can modulate the course of the disease but can NOT cure
hep b t/x
antivirals can help fight the virus and slow damage to the liver