FSHN 3620 • Exam 2 SG: Ch. 12/13
1/14
Earn XP
Description and Tags
School Age Nutrition
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Growth and development in childhood and preadolescence
During early school years, growth is slow and steady preceding to pre-pubertal growth spurt
Growth spurt:
Girls: 10 years
Boys: 12 years
Limb length increases more than trunk length
Growth of brain decreases after infancy
Assess head circumference measurement only up to 3 years
Throughout childhood, percent weight as fat remains same but fat free mass (muscle, bone, soft tissue protein) increases
Shift in body fat accumulation location - leaner
Increases in skeletal muscle mass
Bone formation exceeds bone resorption
Growth hormone – where it originates, its role and purpose, etc.
Small protein that is made by the pituitary gland and secreted into the bloodstream
Pituitary puts out GH in bursts
Levels rise following exercise, trauma, and sleep
More GH is produced at night than during the day
GH is available as a prescription drug that is administered by injection
GH is indicated for children with GH deficiency and others with very short stature
HGH doping and athletic performance
Banned!
BMI Rebound
increase in body fat % in preparation for a growth spurt.
early rebound (before age 5) associated w/ increased risk of overweight & obesity
Body fat minimum
16% in girls
13% in boys
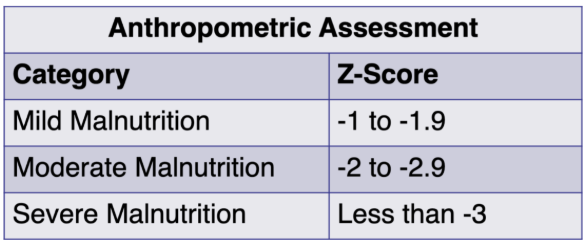
Calculating and interpreting Z scores
used to compare and individual’s anthropometric measurement (like weight, height, or BMI) to a reference population’s mean and standard deviation
The World Health Organization (WHO) provides growth standards with mean & standard deviation values for different age & sex groups, which are used to calculate
Z-scores are only meaningful when compared to a specific reference population
Formula: z-score = O – M/SD
O = observed value
M = median value of the reference population
SD = standard deviation value of reference population
Statistical measure of how many standard deviations the values lies from the mean
Negative = values below the mean
Positive = values above the mean
Understand Growth Velocity, Growth Spurts, and when they happen in boys and girls
Growth spurt
Girls: 10 years
Boys: 12 years
Limb length increases more than trunk length
Growth of brain decreases after infancy
Assess head circumference measurement only up to 3 years
Throughout childhood, percent weight as fat remains same but fat free mass (muscle, bone, soft tissue protein) increases
Shift in body fat accumulation location - leaner
Increases in skeletal muscle mass
Bone formation exceeds bone resorption
Growth velocity: the rate of change in growth over a set period of time.
If too slow, monitor closely
Midgrowth spurt – small increase in growth velocity between 4-8 years
Not all children experience this (more boys than girls)
Occurs before puberty
Somewhat dependent on the season
Children 3-8 usually grow:
At least 2 in per yr
Around 4.4 lbs per yr
Factors Influencing Growth & Development
Genetics
Hormones – GH is most important hormone involved in the growth process
Primary role: Induce growth in height by making bones grow
Pituitary Gland secretes GH
Amount of GF released changes during a person’s lifespan
Peaks during Puberty
Nutrition
Environment
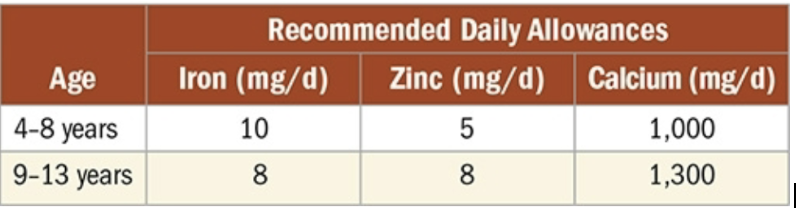
Know the protein and mineral needs for children of different ages, and why these nutrients are important
Protein
Rec. intake is 0.95 g per kg body weight/day for 4- to 13-year-old girls & boys
Children can meet this recommendation by following healthy dietary patterns
Vitamins & minerals
Children’s mean intake of most nutrients meets or exceeds recommendations
Certain subsets of children do not meet nutrient needs for iron, zinc, & calcium
Calcium & vitamin D
Adequate intake important for development of peak bone mass
Adequate vitamin D needed for calcium absorption
Vitamin D from fortified foods and sunlight
Increased skin pigmentation
Limited sunlight exposure
Supplements need to be given under guidance of physician or RDN
Iron
Add good vitamin C source for enhancing absorption
Increased needs related to rapid rate of linear growth, increase in blood volume, & menarche in females
Females → greatest need after menarche
Males → greatest need during growth spurt
Fluoride
Hydroxyfluoroapatite on the enamel — crystalline structure of bones & teeth composed of calcium carbonate & calcium phosphate with fluoride in a collagen matrix gives strength and rigidity to the bones
What children are at particular risk of vitamin deficiency?
Children of deprived families
Children with anorexia, poor eating habits and fad diets
Chronic disease
Dietary regimen to manage obesity
Pregnant teenage children
Vegan/vegetarian diet
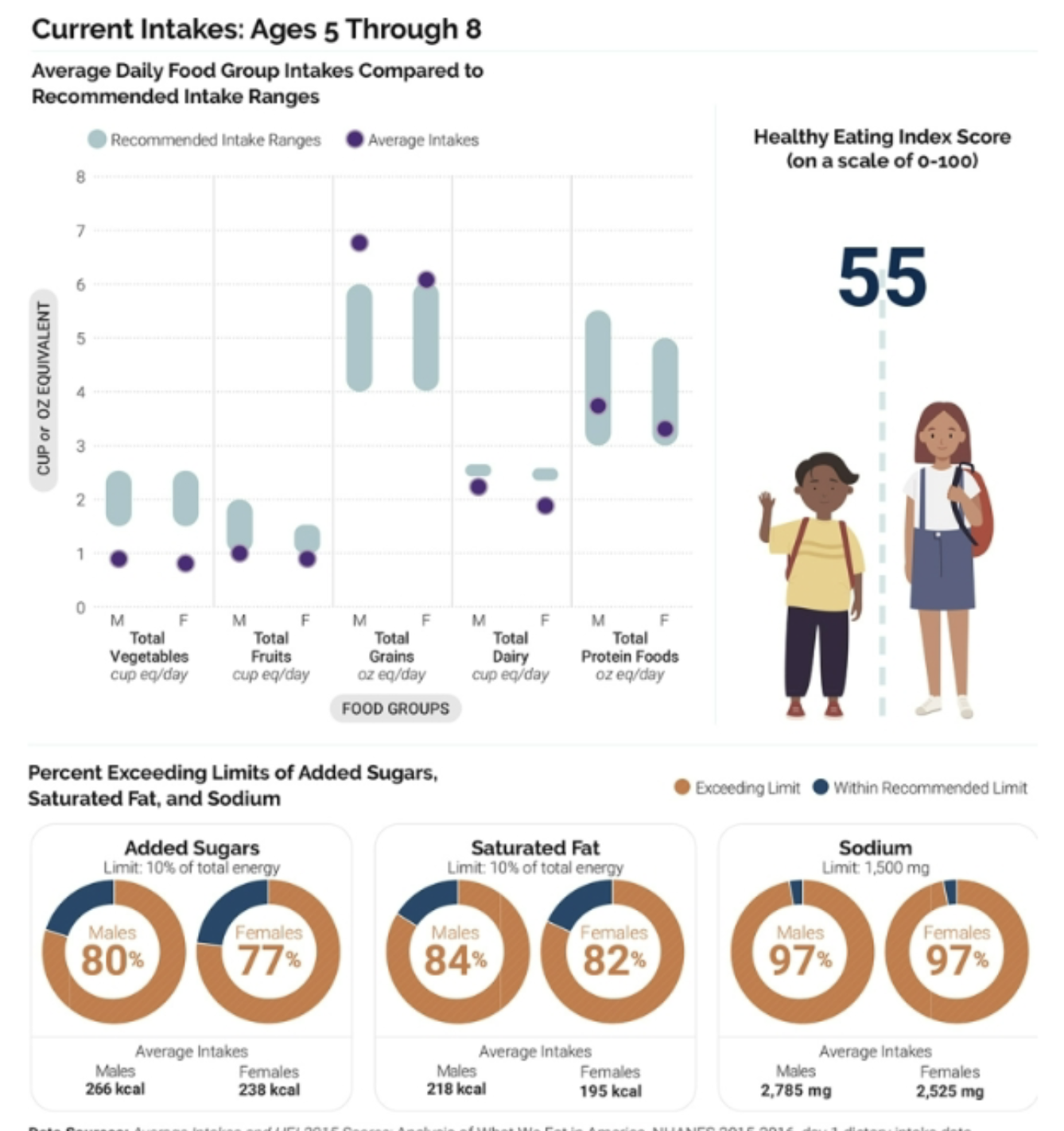
Compare the current dietary recommendations vs actual intakes of the average American child
review photo
Understand the basics of the School Lunch Program and School Breakfast Program
School Lunch Program
Child nutrition programs began in 1946
purpose: provide nutritious meals to all children
Reinforce nutrition education in the classroom
Schools should have a wellness plan
School Breakfast Program
Authorized in 1966
Must provide 25% of the DRIs for the children being served
National School Lunch Program rules apply
States may require schools that serve certain populations to provide breakfast
Cystic fibrosis
genetic mutation in cystic fibrosis transmembrane conductance regulator (CFTR) gene. Affects all exocrine organs in body with lung complications often causing death during adult yrs.
Malabsorption of fat & fat-soluble vitamins due to lack of pancreatic enzymes
Slower rate of weight & height gain
Higher energy needs due to chronic lung infections
Close monitoring to avoid malnutrition
Intensive nutrition interventions
Adequate nutrition & growth link to better pulmonary function
Req
fat-soluble vitamin supplements due to poor intestinal absorption
Cerebral palsy
damage to brain early in life (before or after birth); progression of secondary effects occurs over time.
Secondary effects → contractures, scoliosis, gastroesophageal reflux & constipation (due to coordinated muscle movements part of bowel emptying)
Most nutrition problems is spastic quadriplegia (involving all limbs)
May appear thin bc of smaller muscle size
Slow weight gain
Difficulty w/ feeding & eating
Changes in body composition
Nutrient problems w/ → bone density, calcium, & vitamin D or other nutrients bc of medication side effects
No specific vitamins or minerals to correct CP
Lower energy needs
Nutrition interventions
Stimulating oral feeding
Promoting healthy eating at school
Adjusting menus & timing of meals & snacks at home or school for meeting nutrient needs from foods that minimize fatigue during meals
Assessing & adjusting child’s dietary plan over time
Using adapted self-feeding utensils or other types of feeding equipment
Down syndrome
Low percentile heights are normal for a child w/ Down syndrome
Short stature, low muscle tone, & low weight compared to age-matched peers shouldn’t be attributed to low energy intake
Natural consequences of neuromuscular changes within Down syndrome population
Prescription of growth hormone (GH)
Children with CF, Down syndrome, Prader-Willi syndrome & other chromosomal disorders
If prescribed – time of initiation & discontinuation to be noted in growth assessment to interpret correct growth patterns
Prader-Willi syndrome
Rare genetic condition that leads to physical, mental and behavioral problems.
Short stature, overweight
Key feature: Hyperphagia = feeling hungry ALL THE TIME
As babies, have hypotonia, difficulty feeding
As children, have low growth hormone and behavior problems
80% of energy needs as child of same age/sex w/o the syndrome
At some point in childhood, begin excessive binge eating & cannot stop
Dietitians play a big role in their lives!